
Mindfulness-Based Cognitive Therapy for Stress Reduction in Family Carers of People Living with Dementia: A Systematic Review

 and
and
Abstract
:1. Introduction
1.1. Psychological Factors Related to Carers of PLWD
1.2. Traditional Stress-Reduction Interventions
1.3. Mindfulness-Based Interventions
1.4. Research Gap
1.5. Aims
2. Materials and Methods
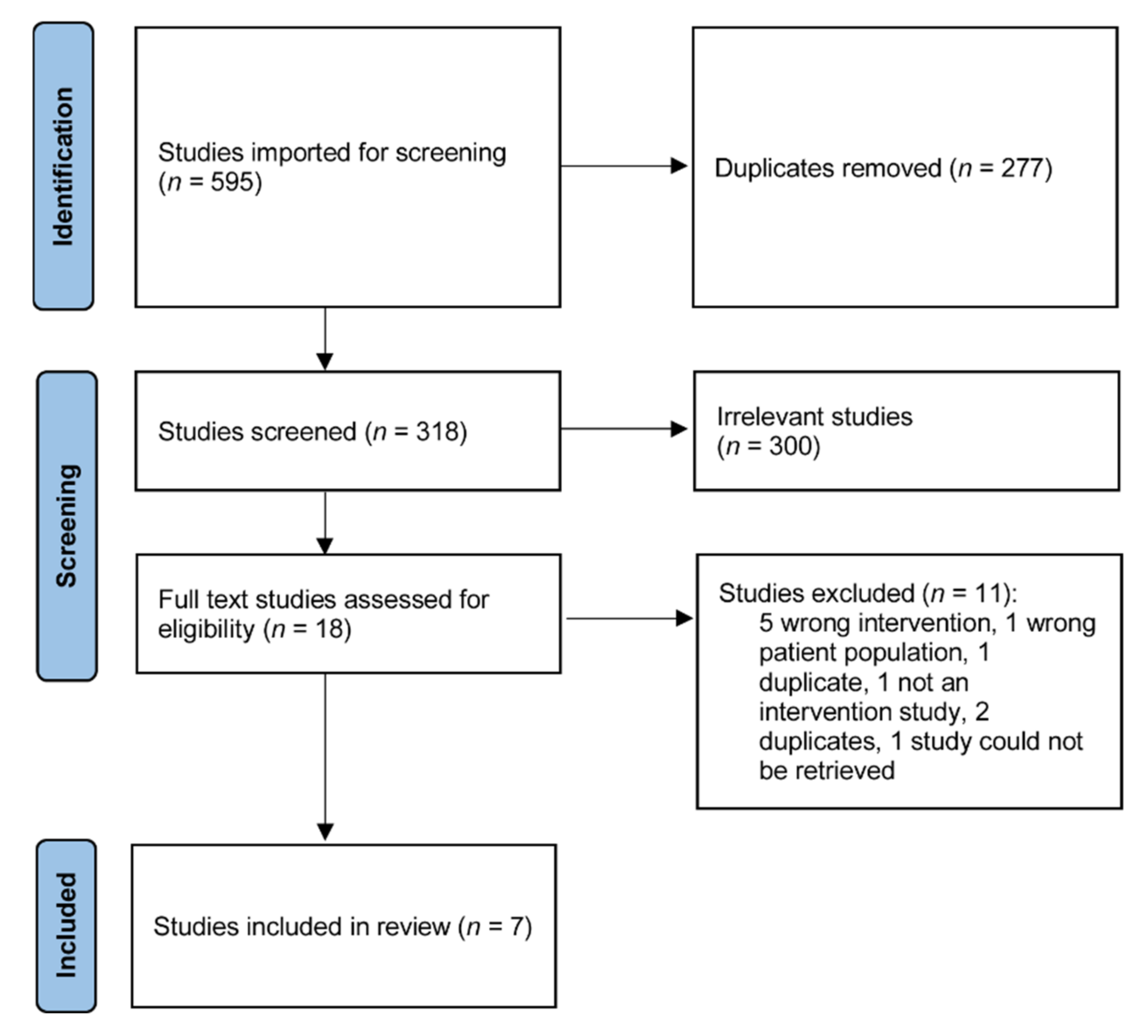
2.1. Search Strategy
2.2. Eligibility Criteria
2.2.1. Study Types
2.2.2. Participant Types
2.2.3. Intervention Types
2.2.4. Outcome Measurement Types
2.3. Data Extraction
2.4. Risk of Bias
2.5. Data Analysis
3. Results
3.1. Study Characteristics
3.1.1. Study Design and Control Group Conditions
3.1.2. Family Carer Characteristics
3.1.3. Intervention
3.1.4. Outcome Measures
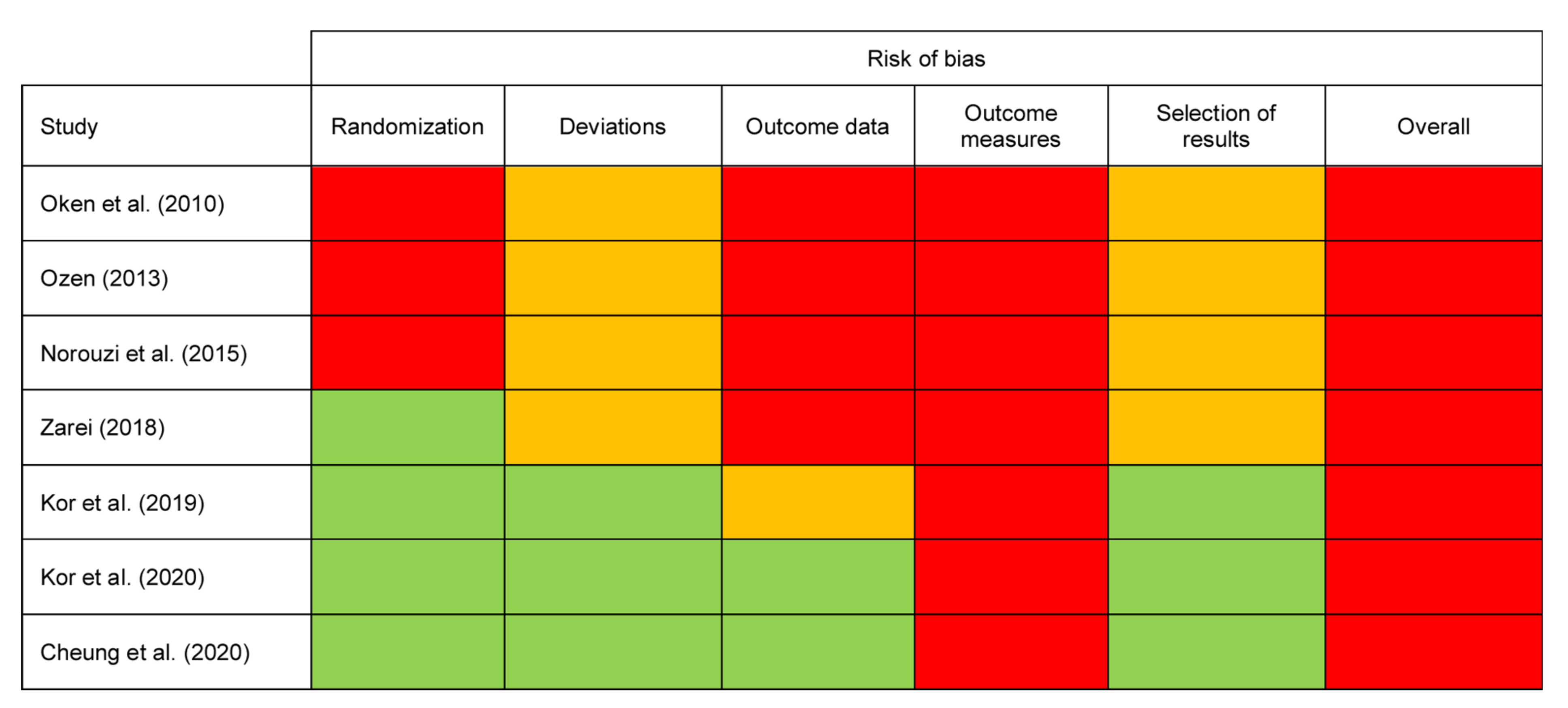
3.2. Risk of Bias Assessment of Included Studies
3.2.1. Randomization
3.2.2. Deviations
3.2.3. Outcome Data
3.2.4. Outcome Measures
3.2.5. Selection of Results
3.2.6. Overall Risk of Bias
3.3. Outcomes of MBCT Interventions
3.3.1. Carer Stress
3.3.2. Carer Burden
3.3.3. Depression
3.3.4. Resilience
3.3.5. Quality of Life
3.3.6. Trait Mindfulness
3.3.7. BPSD in PLWD
3.3.8. Adverse Effects
4. Discussion
4.1. Carer Stress
4.2. Depression and Anxiety
4.3. BPSD in PLWD
4.4. Adaptations of the MBCT Protocol
4.5. Skill Maintenance
4.6. The Superiority of MBCT over MBSR in This Context
4.7. Adverse Effect Reporting
4.8. Future Research Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015: The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015; Available online: https://www.alzint.org/u/WorldAlzheimerReport2015.pdf (accessed on 1 April 2019).
- Prince, M.; Bryce, R.; Ferri, C. World Alzheimer Report 2011: The Benefits of Early Diagnosis and Intervention; Alzheimer’s Disease International: London, UK, 2018; Available online: https://www.alz.co.uk/research/WorldAlzheimerReport2011ExecutiveSummary.pdf (accessed on 1 April 2019).
- Gilhooly, K.J.; Gilhooly, M.L.M.; Sullivan, M.P.; McIntyre, A.; Wilson, L.; Harding, E.; Woodbridge, R.; Crutch, S. A meta-review of stress, coping and interventions in dementia and dementia caregiving. BMC Geriatr. 2016, 16, 106. [Google Scholar] [CrossRef] [Green Version]
- Pinquart, M.; Sörensen, S. Correlates of physical health of informal caregivers: A meta-analysis. J. Gerontol. 2007, 62, 126–137. [Google Scholar] [CrossRef] [Green Version]
- Ory, M.; Hoffman, R.; Yee, J.; Tennstedt, S.; Schulz, R. Prevalence and impact of caregiving: A detailed comparison between dementia and nondementia caregivers. Gerontologist 1999, 39, 177–185. [Google Scholar] [CrossRef] [Green Version]
- O’Dwyer, S.T.; Moyle, W.; Zimmer-Gembeck, M.; De Leo, D. Suicidal ideation in family carers of people with dementia. Aging Ment. Health 2015, 20, 222–230. [Google Scholar] [CrossRef]
- Cooper, C.; Balamurali, T.B.S.; Livingston, G. A systematic review of the prevalence and covariates of anxiety in caregivers of people with dementia. Int. Psychogeriatr. 2007, 19, 175–195. [Google Scholar] [CrossRef]
- Mahoney, R.; Regan, C.; Katona, C.; Livingston, G. Anxiety and depression in family caregivers of people with Alzheimer disease: The LASER-AD study. Am. J. Geriatr. Psychiatry 2005, 13, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Tremont, G. Family caregiving in dementia. Med. Health Rhode Isl. 2011, 94, 36–38. [Google Scholar]
- Adelman, R.D.; Tmanova, L.L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver burden: A clinical review. J. Am. Med. Assoc. 2014, 311, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Zainuddin, J.; Arokiasamy, Z.T.; Poi, P.J. Caregiving burden is associated with short rather than long duration of care for older persons. Asia Pac. J. Public Health 2003, 15, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Spaid, W.M.; Barusch, A. Emotional closeness and caregiver burden in the marital relationship. J. Gerontol. Soc. Work 1994, 21, 197–212. [Google Scholar] [CrossRef]
- Burgener, S.; Twigg, P. Relationships among caregiver factors and quality of life in care recipients with irreversible dementia. Alzheimer Dis. Assoc. Disord. 2002, 16, 88–102. [Google Scholar] [CrossRef]
- Edwards, H.B.; Ijaz, S.; Whiting, P.F.; Leach, V.; Richards, A.; Cullum, S.J.; Cheston, R.I.; Savović, J. Quality of family relationships and outcomes of dementia: A systematic review. BMJ Open 2018, 8, e015538. [Google Scholar] [CrossRef] [Green Version]
- Gaugler, J.E.; Kane, R.L.; Newcomer, R. Resilience and transitions from dementia caregiving. J. Gerontol. 2007, 62, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.; Selwood, A.; Blanchard, M.; Walker, Z.; Blizard, R.; Livingston, G. The determinants of family carers’ abusive behaviour to people with dementia: Results of the CARD study. J. Affect. Disord. 2010, 121, 136–142. [Google Scholar] [CrossRef]
- Sörensen, S.; Pinquart, M.; Duberstein, P. How effective are interventions with caregivers? An updated meta-analysis. Gerontologist 2002, 42, 356–372. [Google Scholar] [CrossRef] [PubMed]
- Dam, A.E.H.; de Vugt, M.E.; Klinkenberg, I.P.M.; Verhey, F.R.J.; van Boxtel, M.P.J. A systematic review of social support interventions for caregivers of people with dementia: Are they doing what they promise? Maturitas 2016, 85, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Sörensen, S. Helping caregivers of persons with dementia: Which interventions work and how large are their effects? Int. Psychogeriatr. 2006, 18, 577–595. [Google Scholar] [CrossRef] [PubMed]
- Teahan, Á.; Lafferty, A.; McAuliffe, E.; Phelan, A.; O’Sullivan, L.; O’Shea, D.; Nicholson, E.; Fealy, G. Psychosocial interventions for family carers of people with dementia: A systematic review and meta-analysis. J. Aging Health 2020, 32, 1198–1213. [Google Scholar] [CrossRef]
- Hopkinson, M.D.; Reavell, J.; Lane, D.A.; Mallikarjun, P. Cognitive behavioral therapy for depression, anxiety, and stress in caregivers of dementia patients: A systematic review and meta-analysis. Gerontologist 2019, 59, e343–e362. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Asnaani, A.; Vonk, I.J.J.; Sawyer, A.T.; Fang, A. The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cogn. Ther. Res. 2012, 36, 427–440. [Google Scholar] [CrossRef] [Green Version]
- Lynch, D.; Laws, K.R.; McKenna, P.J. Cognitive behavioural therapy for major psychiatric disorder: Does it really work? A meta-analytical review of well-controlled trials. Psychol. Med. 2010, 40, 9–24. [Google Scholar] [CrossRef] [Green Version]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Delacorte Press: New York, NY, USA, 1990. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Piet, J.; Hougaard, E. The effect of mindfulness-based cognitive therapy for prevention of relapse in recurrent major depressive disorder: A systematic review and meta-analysis. Clin. Psychol. Rev. 2011, 31, 1032–1040. [Google Scholar] [CrossRef]
- Kuyken, W.; Hayes, R.; Barrett, B.; Byng, R.; Dalgleish, T.; Kessler, D.; Lewis, G.; Watkins, E.; Brejcha, C.; Cardy, J.; et al. Effectiveness and cost-effectiveness of mindfulness-based cognitive therapy compared with maintenance antidepressant treatment in the prevention of depressive relapse or recurrence (PREVENT): A randomised controlled trial. Lancet 2015, 386, 63–73. [Google Scholar] [CrossRef]
- National Institute for Clinical Excellence. Depression: Management of Depression in Primary and Secondary Care (NICE Guideline CG23); National Institute for Clinical Excellence: London, UK, 2004; Available online: https://www.nice.org.uk/guidance/CG23 (accessed on 1 April 2019).
- Malhi, G.S.; Bassett, D.; Boyce, P.; Bryant, R.; Fitzgerald, P.B.; Fritz, K.; Hopwood, M.; Lyndon, B.; Mulder, R.; Murray, G.; et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust. N. Z. J. Psychiatry 2015, 49, 1087–1206. [Google Scholar] [CrossRef]
- Metcalf, C.A.; Dimidjian, S. Extensions and mechanisms of mindfulness-based cognitive therapy: A review of the evidence. Aust. Psychol. 2014, 49, 271–279. [Google Scholar] [CrossRef]
- Birnie, K.; Garland, S.N.; Carlson, L.E. Psychological benefits for cancer patients and their partners participating in mindfulness-based stress reduction (MBSR). Psycho-Oncol. 2010, 19, 1004–1009. [Google Scholar] [CrossRef] [PubMed]
- Bazzano, A.; Wolfe, C.; Zylowska, L.; Wang, S.; Schuster, E.; Barrett, C.; Lehrer, D. Mindfulness based stress reduction (MBSR) for parents and caregivers of individuals with developmental disabilities: A community-based approach. J. Child Fam. Stud. 2015, 24, 298–308. [Google Scholar] [CrossRef]
- Kor, P.P.K.; Wai, T.C.; Liu, J.Y.W.; Lai, C.K.Y. Mindfulness-based intervention for stress reduction of family caregivers of people with dementia: A systematic review and meta-analysis. Mindfulness 2018, 9, 7–22. [Google Scholar] [CrossRef]
- Epstein-Lubow, G.; Miller, I.W.; McBee, L. Mindfulness training for caregivers. Psychiatr. Serv. 2006, 57, 421. [Google Scholar] [CrossRef]
- Oken, B.S.; Fonareva, I.; Haas, M.; Wahbeh, H.; Lane, J.B.; Zajdel, D.; Amen, A. Pilot controlled trial of mindfulness meditation and education for dementia caregivers. J. Altern. Complement. Med. 2010, 16, 1031–1038. [Google Scholar] [CrossRef] [Green Version]
- Whitebird, R.R.; Kreitzer, M.; Crain, A.L.; Lewis, B.A.; Hanson, L.R.; Enstad, C.J. Mindfulness-based stress reduction for family caregivers: A randomized controlled trial. Gerontologist 2013, 53, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, i4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, D.S.K.; Kor, P.P.K.; Jones, C.; Davies, N.; Moyle, W.; Chien, W.T.; Yip, A.L.K.; Chambers, S.; Yu, C.T.K.; Lai, C.K.Y. The use of modified mindfulness-based stress reduction and mindfulness-based cognitive therapy program for family caregivers of people living with dementia: A feasibility study. Asian Nurs. Res. 2020, 14, 221–230. [Google Scholar] [CrossRef]
- Kor, P.P.K.; Liu, J.Y.W.; Chien, W.T. Effects of a modified mindfulness-based cognitive therapy for family caregivers of people with dementia: A pilot randomized controlled trial. Int. J. Nurs. Stud. 2019, 98, 107–117. [Google Scholar] [CrossRef]
- Kor, P.P.K.; Liu, J.Y.W.; Chien, W.T. Effects of a modified mindfulness-based cognitive therapy for family caregivers of people with dementia: A randomized clinical trial. Gerontologist 2021, 61, 977–990. [Google Scholar] [CrossRef]
- Norouzi, M.; Golzari, M.; Faramarz, S. Effectiveness of mindfulness based cognitive therapy on the quality of life, depression and burden of demented women caregivers. Zahedan J. Res. Med. Sci. 2015, 16, 5–11. [Google Scholar] [CrossRef]
- Ozen, L.J. The Efficacy of Mindfulness-Based Cognitive Therapy (MBCT) to Improve Depression Symptoms and Quality of Life in Individuals with Dementia and Their Caregivers: A Pilot Study. Open Trials. 2013. Available online: https://www.openaire.eu/search/dataset?datasetId=opentrials__::10b9db3e55e93fa0bb24fb5db3ccf7dd (accessed on 7 May 2020).
- Zarei, S. Tele-Mindfulness for Dementia’s Family Caregivers: A Randomized Trial with a Usual Care Control Group. Master’s Thesis, University of Toronto, Toronto, ON, Canada, 2018. Available online: http://hdl.handle.net/1807/91463 (accessed on 7 May 2020).
- Teasdale, J.D.; Williams, J.M.G.; Segal, Z.V.; Kabat-Zinn, J. The Mindful Way Workbook; Guilford: New York, NY, USA, 2014. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Teri, L.; Truax, P.; Logsdon, R.; Uomoto, J.; Zarit, S.; Vitaliano, P.P. Assessment of behavioral problems in dementia. Psychol. Aging 1992, 7, 622–631. [Google Scholar] [CrossRef]
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist 1980, 20, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Bedard, M.; Molloy, D.; Squire, L.; Dubois, S.; Lever, J.; O’Donnell, M. The Zarit Burden Interview: A new short version and screening version. Gerontologist 2001, 42, 652–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caserta, M.S.; Lund, D.A.; Wright, S.D. Exploring the caregiver burden inventory (CBI): Further evidence for a multidimensional view of burden. Int. J. Aging Hum. Dev. 1996, 43, 21–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radloff, L.S. The CES-D scale. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation: Sydney, NSW, Australia, 1995. [Google Scholar]
- Hamilton, M. Rating depressive patients. J. Clin. Psychiatry 1980, 41, 21–24. [Google Scholar]
- Lai, J.C.L.; Yue, X. Using the brief resilience scale to assess Chinese people’s ability to bounce back from stress. SAGE Open 2014, 4, 2158244014554386. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.; Kosinski, M.; Keller, S.D. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marin, R.S.; Biedrzycki, R.C.; Firinciogullari, S. Reliability and validity of the apathy evaluation scale. Psychiatry Res. 1991, 38, 143–162. [Google Scholar] [CrossRef]
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The neuropsychiatric inventory: Comprehensive assessment of psychopathology in dementia. Neurology 1994, 44, 2308. [Google Scholar] [CrossRef] [Green Version]
- Bohlmeijer, E.; ten Klooster, P.M.; Fledderus, M.; Veehof, M.; Baer, R. Psychometric properties of the five facet mindfulness questionnaire in depressed adults and development of a short form. Assessment 2011, 18, 308–320. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present. J. Personal. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, K.W.; Coogle, C.L.; Wegelin, J. A pilot randomized controlled trial of mindfulness-based stress reduction for caregivers of family members with dementia. Aging Ment. Health 2016, 20, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Godfrin, K.A.; van Heeringen, C. The effects of mindfulness-based cognitive therapy on recurrence of depressive episodes, mental health and quality of life: A randomized controlled study. Behav. Res. Ther. 2010, 48, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G.; Gómez, A.F. Mindfulness-based interventions for anxiety and depression. Psychiatr. Clin. N. Am. 2017, 40, 739–749. [Google Scholar] [CrossRef]
- Chiesa, A.; Serretti, A. Mindfulness based cognitive therapy for psychiatric disorders: A systematic review and meta-analysis. Psychiatry Res. 2011, 187, 441–453. [Google Scholar] [CrossRef]
- Speca, M.; Carlson, L.E.; Goodey, E.; Angen, M. A randomized, wait-list controlled clinical trial: The effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. Psychosom. Med. 2000, 62, 613–622. [Google Scholar] [CrossRef] [Green Version]
- Hawley, L.L.; Schwartz, D.; Bieling, P.J.; Irving, J.; Corcoran, K.; Farb, N.A.S.; Anderson, A.K.; Segal, Z.V. Mindfulness practice, rumination and clinical outcome in mindfulness-based treatment. Cogn. Ther. Res. 2013, 38, 1–9. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Del Re, A.C.; Hoyt, W.T.; Davis, J.M. The secret ingredient in mindfulness interventions? A case for practice quality over quantity. J. Couns. Psychol. 2014, 61, 491–497. [Google Scholar] [CrossRef]
- Alsubaie, M.; Dickens, C.; Dunn, B.D.; Gibson, A.; Ukoumunne, O.C.; Evans, A.; Vicary, R.; Gandhi, M.; Kuyken, W. Feasibility and acceptability of mindfulness-based cognitive therapy compared with mindfulness-based stress reduction and treatment as usual in people with depression and cardiovascular disorders: A three-arm randomised controlled trial. Mindfulness 2020, 11, 30–50. [Google Scholar] [CrossRef] [Green Version]
- Van Dam, N.T.; van Vugt, M.K.; Vago, D.R.; Schmalzl, L.; Saron, C.D.; Olendzki, A.; Meissner, T.; Lazar, S.W.; Kerr, C.E.; Gorchov, J.; et al. Mind the hype: A critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspect. Psychol. Sci. 2018, 13, 36–61. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author (Year) Country | Design | Sample | Demographics | Intervention Protocol | InterventionSelf-Practice | Control | Measures | Main Findings | Attrition Rate (%) |
|---|---|---|---|---|---|---|---|---|---|
| Oken et al., (2010) USA | Pilot single blinded 3-arm RCT with 2 controls (active A and pragmatic B). | Family carers of PLWD providing at least 12 h per week of care (N = 31). | Female 80.6% Mean age 64.5years (SD = 9.3) Care recipient relationship: Spouse 74.2% Ethnicity: Caucasian 90.3% African American 3.2% Asian 6.5% |
Modified MBCT (n = 10) One education session on dementia weekly in-person group 90 min MBCT session for 6 weeks. Based on both MBCT and MBSR. Contents:
| Strongly encouraged to do regular daily practice with logbook records. Provided written material and audio instructions. |
| RMBPC reaction RMBPC confidence PSS CESD SF-36 Fatigue MAAS FFNJ GPSE PSQI ESS NPI CA CRI approach CRI avoidance Cortisol IL-6 TNF-alpha hsCRP Stroop interference ANT conflict ANT alerting Word list Expectancy Credibility | Both active interventions (MBCT and education) showed decreased self-rated carer stress compared to the respite only control. No significant difference between active groups. | 12.9 |
| Ozen et al., (2013) Canada | Pilot unblinded crossover RCT using dyads of spouses and PLWD, or spouses alone. Unpublished data. | Spouses of PLWD (N = 12) | Female 78% Mean Age 68.9y (SD = 11) Education 13.8y (SD = 2.2) | Modified MBCT (n = 12) Weekly 2 h sessions for 8 weeks Content:
| Daily practice assigned as homework with self-report of time and observations. Guided meditation CDs provided. | Wait list | GDS DASS AES FFMQ QOL-AD SCS ZBI (short version) Brief COPEInventory | MBCT did not have an effect on the outcome variables examined. | 25 |
| Norouzi et al. (2015) Iran | Unblinded RCT | Female carers of PLWD with depression, low quality of life (N = 20) | Female 100% | Unmodified MBCT (n = 10) Weekly 2.5 h sessions for 8 weeks Content:
| No details | Wait list | HAM-D SF-36 CBI | Reductions in depression and carer burden reported at 2 month follow up compared to their baseline within MBCT group. | 0% |
| Zarei et al. (2018) Canada | Unblinded RCT With mixed methods. Unpublished data. | Family carers of PLWD with internet access, computer literacy, and baseline stress (N = 26) | Female 88% Mean age 60y (SD = 13) Care recipient relationship spouse 30% Tertiary educated 88.5% Employed 35% Duration of care relationship 5.12y (SD = 2.88) Living with PLWD 46% PLWD having Alzheimer’s disease 46% | Modified self-help and tele-MBCT (n = 14) Weekly 2 h sessions for 8 weeks 4–6 participants per group All received additional workbook Content:
| Instructed to practice one exercise during the week with recording in practice log for 30–45 min per day. CDs and further readings provided in Mindful Way workbook. | Usual care | PSS SCS CES-D STAI-S CISS-SF NPI-Q Satisfaction questionnaire including 6 open questions for qualitative data. | High satisfaction with MBCT. Pre–post results in stress, depression, and anxiety were not significant in the intervention group. | 8 |
| Kor et al., (2019) Hong Kong | Pilot single blinded RCT | Family carers of PLWD providing care for at least 3 months (N = 36) | Female 83.3% M age 57.1 y (SD = 10.6) Care recipient spouse 16.7% Tertiary educated 44.4% Employed 50% Duration of care relationship 75.1 months (SD = 78.8) Duration of care per week 76.9 h (SD = 62.6) | Modified MBCT (n = 18) 7 sessions of 2 h each (the last 3 sessions were extended to 2 weeks apart with phone contact in between those) over 10 weeks. Single large group of 18 Content:
| Daily practice encouraged with MP3 recordings provided. Home practice duration was recorded. Weekly phone support between sessions 5 and 7 | Brief education with same number of sessions and duration as intervention group. Included group sharing in addition to didactic and skills based training | PSS CESD ZBI BRS SF12_PCS SF12_MCS FFMQ HADS | The intervention group had significantly greater improvements than control for perceived stress and depression from baseline to post intervention and 3 month follow up. They also had very statistically significant reduction in burden compared to controls at the 3 month follow up. | 11.1 |
| Kor et al., (2020) Hong Kong | Multi centre Single blinded parallel group RCT 6 month follow up | Cantonese speaking family carers of PLWD providing at least 4 h of daily contact. Baseline measures suggest higher than average stress levels and lower mental health-related quality of life compared to the Hong Kong population (N = 113) | Female 61.1% Mean age 61.7y (SD = 10.5) Care recipient spouse 34.5% Duration of care relationship 71.0 months (SD = 91.7) Living with PLWD 69.9% Assistance from non-family 39.8% Diagnosed with more than one chronic disease 28.3% | Modified MBCT (n = 56) 7 sessions of 2 h each (the last 3 sessions were extended to 2 weeks apart with phone contact in between those) over 10 weeks. 3 large groups group of 17–19. Content:
| Encouraged, documented, and monitored including during follow up by WhatsApp and emails. | Brief education and usual care with same number of sessions as intervention group. Included group sharing in addition to didactic training. Usual family care services as provided by district elderly community centres. | PSSCESD HADS (Anxiety) ZBI BRS SF12_PCS SF12_MCS NPIQ (Severity) NIPQ (Distress) FFMQ | The intervention group had greater improvement in stress, depression, anxiety, and BPSD-related caregiver distress, compared to control at both post intervention and 6 month follow up. | 7 |
| Cheung et al., (2020) Hong Kong | Single blinded RCT. | Family carers of PLWD, providing care for at least 3 months (N = 53) | Female 86.8% Care recipient spouse 7.5% Ethnicity All Chinese Mean duration of providing care to PLWD 8.71 years (SD = 10.56) | Modified MBCT (n = 26) 7 sessions of 2.5 h over 16 weeks (first 4 sessions were weekly then the last 3 were monthly with phone contact in between) Content:
| CD recording of all exercises provided. | Modified MBSR. Same number of sessions, duration, and frequency (including phone support) as MBCT group. Delivered by same therapist as MBCT. Adaptations made by same panel of expert clinicians as MBCT. Fidelity checking done. | PSS CESD ZBI FFMQ-SF | Both interventions were feasible. Both groups had positive within-group effects on perceived stress, depression and burden, while the MBCT group had a larger effect on stress reduction than the MBSR group. | 3.8 |
| Study | Outcome Measure | Effect Size (d) | ||
|---|---|---|---|---|
| Post Intervention | 3 Months Post Intervention | 6 Months Post Intervention | ||
| Oken et al., (2010) | PSS | 0.0 | ||
| CES-D | 0.3 | |||
| Kor et al., (2020) | PSS | 0.4 | 0.7 | |
| CES-D | 0.9 | 1.4 | ||
| HADS (Anxiety) | 0.7 | 1.0 | ||
| ZBI | 0.7 | 0.6 | ||
| BRS | 0.1 | 0.3 | ||
| SF12-PCS | 0.5 | 0.04 | ||
| SF12-MCS | 0.1 | 0.6 | ||
| NPIQ (Severity) | 0.2 | 0.3 | ||
| NPIQ (Distress) | 0.4 | 0.8 | ||
| Kor et al., (2019) | PSS | 0.4 | 0.2 | |
| CES-D | 0.04 | 0.77 | ||
| HADS (Anxiety) | 0.35 | 0.08 | ||
| ZBI | 0.71 | 0.13 | ||
| BRS | 0.64 | 0.16 | ||
| SF12-PCS | 0.24 | 0.24 | ||
| SF12-MCS | 0.17 | 0.17 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chacko, E.; Ling, B.; Avny, N.; Barak, Y.; Cullum, S.; Sundram, F.; Cheung, G. Mindfulness-Based Cognitive Therapy for Stress Reduction in Family Carers of People Living with Dementia: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 614. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010614
Chacko E, Ling B, Avny N, Barak Y, Cullum S, Sundram F, Cheung G. Mindfulness-Based Cognitive Therapy for Stress Reduction in Family Carers of People Living with Dementia: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(1):614. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010614
Chicago/Turabian StyleChacko, Emme, Benjamin Ling, Nadav Avny, Yoram Barak, Sarah Cullum, Fred Sundram, and Gary Cheung. 2022. "Mindfulness-Based Cognitive Therapy for Stress Reduction in Family Carers of People Living with Dementia: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 1: 614. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010614