
Association between Parenthood and Health Behaviour in Later Life—Results from the Population-Based CARLA Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Parental Status
2.3. Health Behaviour
2.4. Confounders
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Physical Activity in Sports
4.2. Physical Activity in Leisure-Time Other Than Sports
4.3. Diet
4.4. Tobacco and Alcohol Consumption
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chudasama, Y.V.; Khunti, K.; Gillies, C.L.; Dhalwani, N.N.; Davies, M.J.; Yates, T.; Zaccardi, F. Healthy lifestyle and life expectancy in people with multimorbidity in the UK Biobank: A longitudinal cohort study. PLoS Med. 2020, 17, e1003332. [Google Scholar] [CrossRef]
- Khaw, K.T.; Wareham, N.; Bingham, S.; Welch, A.; Luben, R.; Day, N. Combined impact of health behaviours and mortality in men and women: The EPIC-Norfolk prospective population study. PLoS Med. 2008, 5, e12. [Google Scholar] [CrossRef] [Green Version]
- Fransen, H.P.; May, A.M.; Beulens, J.W.; Struijk, E.A.; de Wit, G.A.; Boer, J.M.; Onland-Moret, N.C.; Hoekstra, J.; van der Schouw, Y.T.; Bueno-de-Mesquita, H.B.; et al. Association between lifestyle factors and quality-adjusted life years in the EPIC-NL cohort. PLoS ONE 2014, 9, e111480. [Google Scholar] [CrossRef]
- Myint, P.K.; Smith, R.D.; Luben, R.N.; Surtees, P.G.; Wainwright, N.W.J.; Wareham, N.J.; Khaw, K.-T. Lifestyle behaviours and quality-adjusted life years in middle and older age. Age Ageing 2011, 40, 589–595. [Google Scholar] [CrossRef] [Green Version]
- Saxbe, D.; Rossin-Slater, M.; Goldenberg, D. The transition to parenthood as a critical window for adult health. Am. Psychol. 2018, 73, 1190–1200. [Google Scholar] [CrossRef] [PubMed]
- Umberson, D.; Crosnoe, R.; Reczek, C. Social Relationships and Health Behavior Across the Life Course. Annu. Rev. Sociol. 2010, 36, 139–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendig, H.; Dykstra, P.A.; van Gaalen, R.I.; Melkas, T. Health of aging parents and childless individuals. J. Fam. Issues 2007, 28, 1457–1486. [Google Scholar] [CrossRef] [Green Version]
- Abell, L.P.; Tanase, K.A.; Gilmore, M.L.; Winnicki, A.E.; Holmes, V.L.; Hartos, J.L. Do physical activity levels differ by number of children at home in women aged 25–44 in the general population? Women’s Health 2019, 15, 1745506519871186. [Google Scholar] [CrossRef] [Green Version]
- Bellows-Riecken, K.H.; Rhodes, R.E. A birth of inactivity? A review of physical activity and parenthood. Prev. Med. 2008, 46, 99–110. [Google Scholar] [CrossRef]
- Carson, V.; Adamo, K.; Rhodes, R.E. Associations of Parenthood with Physical Activity, Sedentary Behavior, and Sleep. Am. J. Health Behav. 2018, 42, 80–89. [Google Scholar] [CrossRef]
- Corder, K.; Winpenny, E.M.; Foubister, C.; Guagliano, J.M.; Hartwig, X.M.; Love, R.; Clifford Astbury, C.; van Sluijs, E.M.F. Becoming a parent: A systematic review and meta-analysis of changes in BMI, diet, and physical activity. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2020, 21, e12959. [Google Scholar] [CrossRef] [Green Version]
- Perales, F.; del Pozo-Cruz, J.; del Pozo-Cruz, B. Long-term dynamics in physical activity behaviour across the transition to parenthood. Int. J. Public Health 2015, 60, 301–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pot, N.; Keizer, R. Physical activity and sport participation: A systematic review of the impact of fatherhood. Prev. Med. Rep. 2016, 4, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Rattay, P.; von der Lippe, E. Association between Living with Children and the Health and Health Behavior of Women and Men. Are There Differences by Age? Results of the “German Health Update” (GEDA) Study. Int. J. Env. Res. Public Health 2020, 17, 3180. [Google Scholar] [CrossRef]
- Werneck, A.O.; Winpenny, E.M.; van Sluijs, E.M.F.; Corder, K. Cohabiting and becoming a parent: Associations with changes in physical activity in the 1970 British cohort study. BMC Public Health 2020, 20, 1085. [Google Scholar] [CrossRef]
- Berge, J.M.; Larson, N.; Bauer, K.W.; Neumark-Sztainer, D. Are parents of young children practicing healthy nutrition and physical activity behaviors? Pediatrics 2011, 127, 881–887. [Google Scholar] [CrossRef] [Green Version]
- Laroche, H.H.; Wallace, R.B.; Snetselaar, L.; Hillis, S.L.; Steffen, L.M. Changes in diet behavior when adults become parents. J. Acad. Nutr. Diet. 2012, 112, 832–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.J.; McNaughton, S.A.; Gall, S.L.; Otahal, P.; Dwyer, T.; Venn, A.J. Associations between Partnering and Parenting Transitions and Dietary Habits in Young Adults. J. Acad. Nutr. Diet. 2017, 117, 1210–1221. [Google Scholar] [CrossRef]
- Bricard, D.; Legleye, S.; Khlat, M. Changes in Smoking Behavior over Family Transitions: Evidence for Anticipation and Adaptation Effects. Int. J. Environ. Res. Public Health 2017, 14, 610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomeer, M.B.; Hernandez, E.; Umberson, D.; Thomas, P.A. Influence of Social Connections on Smoking Behavior across the Life Course. Adv. Life Course Res. 2019, 42, 100294. [Google Scholar] [CrossRef] [Green Version]
- McDermott, L.J.; Dobson, A.; Owen, N. From partying to parenthood: Young women’s perceptions of cigarette smoking across life transitions. Health Educ. Res. 2006, 21, 428–439. [Google Scholar] [CrossRef] [Green Version]
- Borschmann, R.; Becker, D.; Spry, E.; Youssef, G.J.; Olsson, C.A.; Hutchinson, D.M.; Silins, E.; Boden, J.M.; Moreno-Betancur, M.; Najman, J.M.; et al. Alcohol and parenthood: An integrative analysis of the effects of transition to parenthood in three Australasian cohorts. Drug Alcohol Depend. 2019, 197, 326–334. [Google Scholar] [CrossRef]
- Levy, F.; Le Strat, Y.; Hoertel, N.; Ancelet, C.; Dubertret, C. Childbirth and alcohol consumption impact of recent childbirth on alcohol consumption. J. Child Fam. Stud. 2018, 27, 2245–2253. [Google Scholar] [CrossRef]
- Patrick, M.E.; Evans-Polce, R.; Wagner, A.C.; Mehus, C.J. High-intensity drinking by parental status: Differences by age and sex. Addict. Behav. 2020, 102, 106180. [Google Scholar] [CrossRef] [PubMed]
- Chilcoat, H.D.; Breslau, N. Alcohol Disorders in Young Adulthood: Effects of Transitions into Adult Roles. J. Health Soc. Behav. 1996, 37, 339–349. [Google Scholar] [CrossRef]
- Nelson, S.K.; Kushlev, K.; Lyubomirsky, S. The pains and pleasures of parenting: When, why, and how is parenthood associated with more or less well-being? Psychol. Bull. 2014, 140, 846–895. [Google Scholar] [CrossRef]
- Nomaguchi, K.; Milkie, M.A. Parenthood and well-being: A decade in review. J. Marriage Fam. 2020, 82, 198–223. [Google Scholar] [CrossRef] [PubMed]
- Grundy, E.; van den Broek, T.; Keenan, K. Number of Children, Partnership Status, and Later-life Depression in Eastern and Western Europe. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2019, 74, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Lee, S.G.; Shin, J.; Choi, Y.; Park, E.C. The effect of offspring on depressive disorder among old adults: Evidence from the Korean Longitudinal Study of Aging from 2006 to 2012. Arch. Gerontol. Geriatr. 2015, 61, 351–362. [Google Scholar] [CrossRef]
- Eisenberg, M.L.; Park, Y.; Hollenbeck, A.R.; Lipshultz, L.I.; Schatzkin, A.; Pletcher, M.J. Fatherhood and the risk of cardiovascular mortality in the NIH-AARP Diet and Health Study. Hum. Reprod. 2011, 26, 3479–3485. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, D.A.; Emberson, J.R.; Ebrahim, S.; Whincup, P.H.; Wannamethee, S.G.; Walker, M.; Smith, G.D. Is the association between parity and coronary heart disease due to biological effects of pregnancy or adverse lifestyle risk factors associated with child-rearing? Findings from the British Women’s Heart and Health Study and the British Regional Heart Study. Circulation 2003, 107, 1260–1264. [Google Scholar] [CrossRef] [Green Version]
- Elenkov, A.; Giwercman, A.; Søgaard Tøttenborg, S.; Bonde, J.P.E.; Glazer, C.H.; Haervig, K.K.; Bungum, A.B.; Nilsson, P.M. Male childlessness as independent predictor of risk of cardiovascular and all-cause mortality: A population-based cohort study with more than 30 years follow-up. PLoS ONE 2020, 15, e0237422. [Google Scholar] [CrossRef] [PubMed]
- Bungum, A.B.; Glazer, C.H.; Bonde, J.P.; Nilsson, P.M.; Giwercman, A.; Søgaard Tøttenborg, S. Risk of metabolic disorders in childless men: A population-based cohort study. BMJ Open 2018, 8, e020293. [Google Scholar] [CrossRef] [Green Version]
- Högnäs, R.S.; Roelfs, D.J.; Shor, E.; Moore, C.; Reece, T. J-Curve? A Meta-Analysis and Meta-Regression of Parity and Parental Mortality. Popul. Res. Policy Rev. 2017, 36, 273–308. [Google Scholar] [CrossRef]
- Modig, K.; Talbäck, M.; Torssander, J.; Ahlbom, A. Payback time? Influence of having children on mortality in old age. J. Epidemiol. Community Health 2017, 71, 424–430. [Google Scholar] [CrossRef]
- Barclay, K.; Keenan, K.; Grundy, E.; Kolk, M.; Myrskylä, M. Reproductive history and post-reproductive mortality: A sibling comparison analysis using Swedish register data. Soc. Sci. Med. 2016, 155, 82–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundy, E.; Kravdal, Ø. Fertility history and cause-specific mortality: A register-based analysis of complete cohorts of Norwegian women and men. Soc. Sci. Med. 2010, 70, 1847–1857. [Google Scholar] [CrossRef]
- Sironi, M.; Ploubidis, G.B.; Grundy, E.M. Fertility History and Biomarkers Using Prospective Data: Evidence From the 1958 National Child Development Study. Demography 2020, 57, 529–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barclay, K.; Kolk, M. Parity and Mortality: An Examination of Different Explanatory Mechanisms Using Data on Biological and Adoptive Parents. Eur. J. Popul. Rev. Eur. De Demogr. 2018, 35, 63–85. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO): Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 18 July 2021).
- Alwan, A. Global Status Report on Noncommunicable Diseases 2010; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- World Health Organization (WHO). Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organizatio: Geneva, Switzerland, 2019. [Google Scholar]
- Greiser, K.H.; Kluttig, A.; Schumann, B.; Kors, J.A.; Swenne, C.A.; Kuss, O.; Werdan, K.; Haerting, J. Cardiovascular disease, risk factors and heart rate variability in the elderly general population: Design and objectives of the CARdiovascular disease, Living and Ageing in Halle (CARLA) Study. BMC Cardiovasc. Disord. 2005, 5, 33. [Google Scholar] [CrossRef] [Green Version]
- Greiser, K.H.; Kluttig, A.; Schumann, B.; Swenne, C.A.; Kors, J.A.; Kuss, O.; Haerting, J.; Schmidt, H.; Thiery, J.; Werdan, K. Cardiovascular diseases, risk factors and short-term heart rate variability in an elderly general population: The CARLA study 2002–2006. Eur. J. Epidemiol. 2009, 24, 123–142. [Google Scholar] [CrossRef] [PubMed]
- Baecke, J.A.; Burema, J.; Frijters, J.E. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am. J. Clin. Nutr. 1982, 36, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Philippaerts, R.M.; Westerterp, K.R.; Lefevre, J. Doubly labelled water validation of three physical activity questionnaires. Int. J. Sports Med. 1999, 20, 284–289. [Google Scholar] [CrossRef]
- Winkler, G.; Döring, A. Validation of a short qualitative food frequency list used in several German large scale surveys. Z. Für Ernahr. 1998, 37, 234–241. [Google Scholar] [CrossRef]
- Winkler, G.; Döring, A. Kurzmethoden zur Charakterisierung des Ernährungsmusters: Einsatz und Auswertung eines Food-Frequency-Fragebogens. Ernahr. Umsch. 1995, 42, 289–291. [Google Scholar]
- Bühringer, G.; Augustin, R.; Bergmann, E.; Bloomfield, K.; Funk, W.; Junge, B.; Kraus, L.; Merfert-Diete, C.; Rumpf, H.J.; Simon, R. Alkoholkonsum und Alkoholbezogene Störungen in Deutschland; Das Bundesministerium für Gesundheit: Berlin, Germany, 2000. [Google Scholar]
- Schumann, B.; Kluttig, A.; Tiller, D.; Werdan, K.; Haerting, J.; Greiser, K.H. Association of childhood and adult socioeconomic indicators with cardiovascular risk factors and its modification by age: The CARLA Study 2002–2006. BMC Public Health 2011, 11, 289. [Google Scholar] [CrossRef] [Green Version]
- Engelman, M.; Agree, E.M.; Yount, K.M.; Bishai, D. Parity and parents’ health in later life: The gendered case of Ismailia, Egypt. Popul. Stud. 2010, 64, 165–178. [Google Scholar] [CrossRef]
- Halland, F.; Morken, N.-H.; DeRoo, L.A.; Klungsøyr, K.; Wilcox, A.J.; Skjærven, R. Association of Women’s Reproductive History With Long-term Mortality and Effect of Socioeconomic Factors. Obstet. Gynecol. 2015, 126, 1181–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrovic, D.; de Mestral, C.; Bochud, M.; Bartley, M.; Kivimäki, M.; Vineis, P.; Mackenbach, J.; Stringhini, S. The contribution of health behaviors to socioeconomic inequalities in health: A systematic review. Prev. Med. 2018, 113, 15–31. [Google Scholar] [CrossRef] [Green Version]
- Gierc, M.; Locke, S.; Jung, M.; Brawley, L. Attempting to be active: Self-efficacy and barrier limitation differentiate activity levels of working mothers. J. Health Psychol. 2016, 21, 1351–1360. [Google Scholar] [CrossRef]
- Mailey, E.L.; Huberty, J.; Dinkel, D.; McAuley, E. Physical activity barriers and facilitators among working mothers and fathers. BMC Public Health 2014, 14, 657. [Google Scholar] [CrossRef] [Green Version]
- Saligheh, M.; McNamara, B.; Rooney, R. Perceived barriers and enablers of physical activity in postpartum women: A qualitative approach. BMC Pregnancy Childbirth 2016, 16, 131. [Google Scholar] [CrossRef] [Green Version]
- Schluter, P.; Oliver, M.; Paterson, J. Perceived barriers and incentives to increased physical activity for Pacific mothers in New Zealand: Findings from the Pacific Islands Families Study. Aust. N. Z. J. Public Health 2011, 35, 151–158. [Google Scholar] [CrossRef]
- Nomaguchi, K.M.; Bianchi, S.M. Exercise Time: Gender Differences in the Effects of Marriage, Parenthood, and Employment. J. Marriage Fam. 2004, 66, 413–430. [Google Scholar] [CrossRef]
- Baranowska-Rataj, A.; Abramowska-Kmon, A. Number of children and social contacts among older people: The moderating role of filial norms and social policies. Eur. J. Ageing 2018, 16, 95–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundy, E.; Read, S. Social contacts and receipt of help among older people in England: Are there benefits of having more children? J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2012, 67, 742–754. [Google Scholar] [CrossRef] [Green Version]
- Becker, C.; Kirchmaier, I.; Trautmann, S.T. Marriage, parenthood and social network: Subjective well-being and mental health in old age. PLoS ONE 2019, 14, e0218704. [Google Scholar] [CrossRef] [Green Version]
- Vikström, J.; Bladh, M.; Hammar, M.; Marcusson, J.; Wressle, E.; Sydsjö, G. The influences of childlessness on the psychological well-being and social network of the oldest old. BMC Geriatr. 2011, 11, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsay Smith, G.; Banting, L.; Eime, R.; O’Sullivan, G.; van Uffelen, J.G.Z. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 56. [Google Scholar] [CrossRef] [PubMed]
- Deindl, C.; Brandt, M. Support networks of childless older people: Informal and formal support in Europe. Ageing Soc. 2017, 37, 1543–1567. [Google Scholar] [CrossRef] [Green Version]
- Klaus, D.; Schnettler, S. Social networks and support for parents and childless adults in the second half of life: Convergence, divergence, or stability? Adv. Life Course Res. 2016, 29, 95–105. [Google Scholar] [CrossRef]
- Umberson, D. Gender, marital status and the social control of health behavior. Soc. Sci. Med. 1992, 34, 907–917. [Google Scholar] [CrossRef]
- Ainsworth, B.E. Issues in the Assessment of Physical Activity in Women. Res. Q. Exerc. Sport 2000, 71, 37–42. [Google Scholar] [CrossRef]
- Reczek, C.; Beth Thomeer, M.; Lodge, A.C.; Umberson, D.; Underhill, M. Diet and Exercise in Parenthood: A Social Control Perspective. J. Marriage Fam. 2014, 76, 1047–1062. [Google Scholar] [CrossRef] [Green Version]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Wendel-Vos, W.; Droomers, M.; Kremers, S.; Brug, J.; Van Lenthe, F. Potential environmental determinants of physical activity in adults: A systematic review. Obes. Rev. 2007, 8, 425–440. [Google Scholar] [CrossRef]
- McMunn, A.; Bartley, M.; Hardy, R.; Kuh, D. Life course social roles and women’s health in mid-life: Causation or selection? J. Epidemiol. Community Health 2006, 60, 484–489. [Google Scholar] [CrossRef] [Green Version]
- Lacey, R.E.; Sacker, A.; Bell, S.; Kumari, M.; Worts, D.; McDonough, P.; Kuh, D.; McMunn, A. Work-family life courses and BMI trajectories in three British birth cohorts. Int. J. Obes. 2017, 41, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Grundy, E.; Read, S. Pathways from fertility history to later life health. Results from analyses of the English Longitudinal Study of Ageing. Demogr. Res. 2015, 32, 107–146. [Google Scholar] [CrossRef] [Green Version]
- Hardy, R.; Lawlor, D.A.; Black, S.; Wadsworth, M.E.; Kuh, D. Number of children and coronary heart disease risk factors in men and women from a British birth cohort. BJOG Int. J. Obstet. Gynaecol. 2007, 114, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Raley, R.K.; Sweeney, M.M. Divorce, Repartnering, and Stepfamilies: A Decade in Review. J. Marriage Fam. 2020, 82, 81–99. [Google Scholar] [CrossRef] [Green Version]
- Pollmann-Schult, M. Single motherhood and life satisfaction in comparative perspective: Do institutional and cultural contexts explain the life satisfaction penalty for single mothers? J. Fam. Issues 2018, 39, 2061–2084. [Google Scholar] [CrossRef]
- Reczek, C. Sexual-and gender-minority families: A 2010 to 2020 decade in review. J. Marriage Fam. 2020, 82, 300–325. [Google Scholar] [CrossRef]
- Hansen, T. Parenthood and Happiness: A Review of Folk Theories Versus Empirical Evidence. Soc. Indic. Res. 2012, 108, 29–64. [Google Scholar] [CrossRef] [Green Version]
- Quashie, N.T.; Arpino, B.; Antczak, R.; Mair, C.A. Childlessness and Health Among Older Adults: Variation Across Five Outcomes and 20 Countries. J. Gerontol. Ser. B 2019, 76, 348–359. [Google Scholar] [CrossRef]
- Hank, K. Childbearing history, later-life health, and mortality in Germany. Popul. Stud. 2010, 64, 275–291. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Women | N | Missing (%) | Men | N | Missing (%) |
|---|---|---|---|---|---|---|
| 45.6% | 812 | 0 | 54.4% | 967 | 0 | |
| Parents | 88.3% | 717 | 0 | 89.8% | 868 | 0 |
| Number of children | 2.0 (1.0) | 717 | 11.7 | 2.1 (1.1) | 868 | 10.2 |
| Age | 63.8 (9.9) | 0 | 64.9 (10.2) | 0 | ||
| Living with a partner | 61.1% | 496 | 0 | 86.5% | 836 | 0 |
| Education years | 13.93 (2.5) | 0 | 15.21 (2.5) | 0 | ||
| Occupational position | 0.7 | 0.3 | ||||
| Unskilled-simple | 37.7% | 304 | 38.2% | 368 | ||
| Qualified | 47.4% | 382 | 25.9% | 250 | ||
| High qualified | 14.9% | 120 | 35.9% | 346 | ||
| Net equivalent income per person | 1.6 | 0.9 | ||||
| <EUR 750 | 14.6% | 117 | 9.9% | 95 | ||
| EUR 750– <EUR 1500 | 57.3% | 458 | 53.3% | 511 | ||
| ≥EUR 1500 | 28.0% | 224 | 36.7% | 352 | ||
| Socioeconomic status in childhood | 1.6 | 1.8 | ||||
| Low | 57.2% | 457 | 55.1% | 523 | ||
| Middle | 37.4% | 299 | 39.5% | 375 | ||
| High | 5.4% | 43 | 5.5% | 52 | ||
| Number of chronic conditions | 0 | 0 | ||||
| 0 | 40.8% | 331 | 44.9% | 434 | ||
| 1 | 33.3% | 270 | 30.0% | 290 | ||
| 2 | 15.5% | 126 | 16.4% | 159 | ||
| 3+ | 10.5% | 85 | 8.7% | 84 |
| Variable | Mothers | N | Non-Mothers | N | Fathers | N | Non-Fathers | N |
|---|---|---|---|---|---|---|---|---|
| Physical activity | ||||||||
| Active in sports | 43.2% | 310 | 39.4% | 37 | 31.9% | 277 | 19.2% | 19 |
| Sport index | 2.37 (2.32; 2.42) | 715 | 2.33 (2.18; 2.47) | 93 | 2.41 (2.36; 2.46) | 864 | 2.09 (1.96; 2.21) | 98 |
| Leisure-time index | 3.16 (3.11; 3.20) | 717 | 3.11 (2.99; 3.23) | 93 | 3.13 (3.08; 3.17) | 867 | 3.10 (2.97; 3.23) | 99 |
| Dietary pattern | ||||||||
| Dietary pattern index | 16.44 (16.08; 16.79) | 717 | 16.49 (15.40; 17.58) | 95 | 14.58 (14.34; 14.82) | 866 | 14.44 (13.72; 15.15) | 99 |
| Alcohol | ||||||||
| 0 g Alcohol per day | 55.1% | 395 | 54.7% | 52 | 21.4% | 185 | 21.2% | 21 |
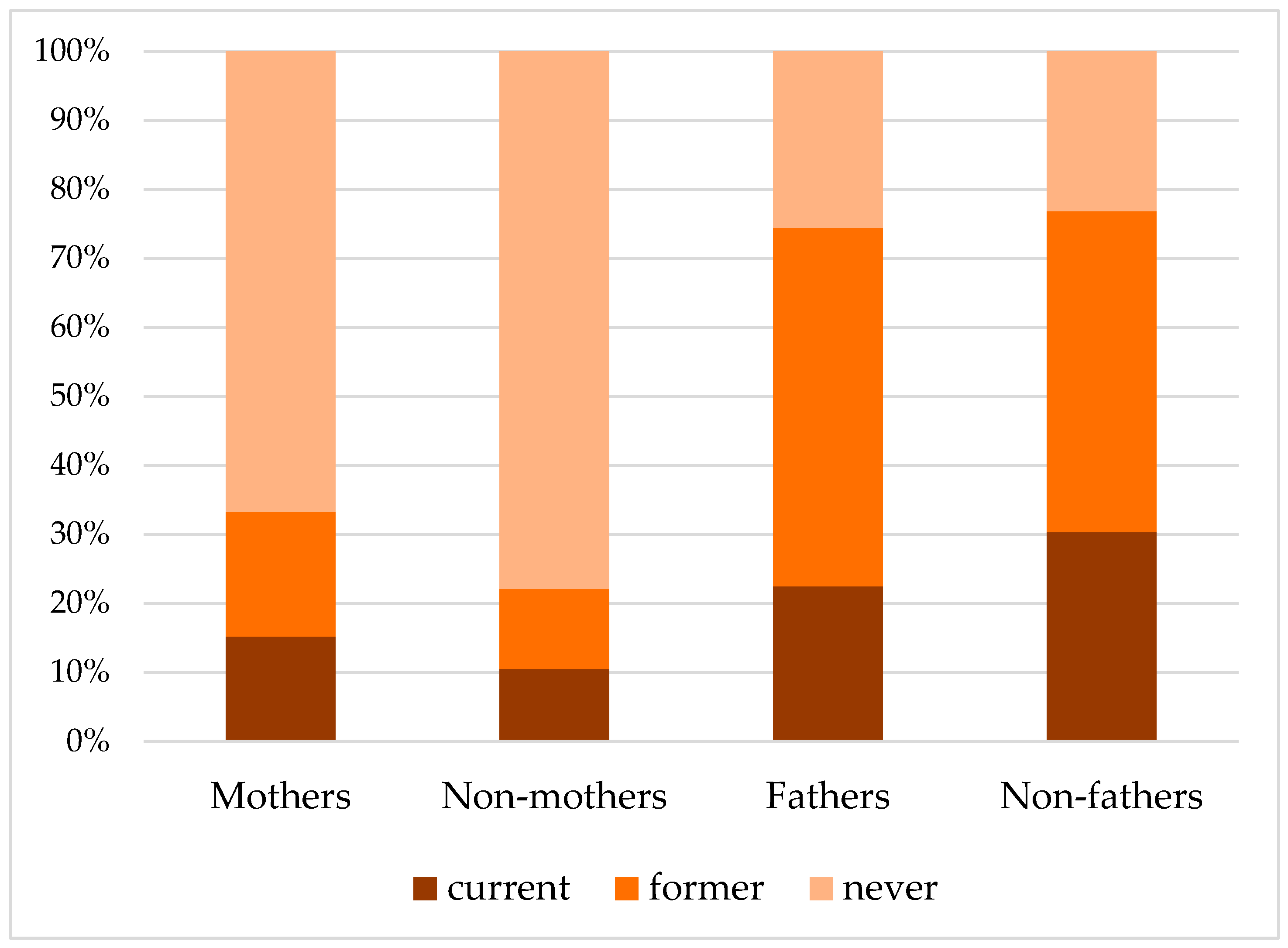
| Smoking | ||||||||
| Current | 15.2% | 109 | 10.5% | 10 | 22.5% | 195 | 30.3% | 30 |
| Former | 18.0% | 129 | 11.6% | 11 | 51.9% | 450 | 46.5% | 46 |
| Never | 66.8% | 479 | 77.9% | 74 | 25.6% | 222 | 23.2% | 23 |
| Outcome Variable | Unadjusted | Adjusted * |
|---|---|---|
| β (95%CI) | β (95%CI) | |
| Women | ||
| Sport index | 0.05 (−0.11; 0.20) | 0.10 (−0.06; 0.25) |
| Leisure-time index | 0.05 (−0.08; 0.18) | 0.06 (−0.07; 0.20) |
| Dietary pattern index | −0.28 (−0.95; 0.40) | −0.05 (−0.76; 0.66) |
| Men | ||
| Sport index | 0.33 (0.18; 0.48) | 0.29 (0.14; 0.44) |
| Leisure-time index | 0.03 (−0.11; 0.16) | 0.03 (−0.11; 0.16) |
| Dietary pattern index | −0.08 (−0.75; 0.58) | −0.04 (−0.71; 0.62) |
| Outcome Variable | Unadjusted | Adjusted * |
|---|---|---|
| OR (95%CI) | OR (95%CI) | |
| Women | ||
| Active in sports | 1.17 (0.76; 1.82) | 1.32 (0.82; 2.14) |
| Consumption of alcohol | 0.99 (0.64; 1.52) | 0.84 (0.52; 1.36) |
| Smoking status | ||
| Former vs. current smoker | 1.08 (0.44; 2.63) | 1.60 (0.61; 4.21) |
| Never vs. current smoker | 0.59 (0.30; 1.19) | 0.99 (0.46; 2.12) |
| Men | ||
| Active in sports | 1.98 (1.18; 3.33) | 2.06 (1.17; 3.61) |
| Consumption of alcohol | 0.99 (0.60; 1.65) | 0.89 (0.52; 1.53) |
| Smoking status | ||
| Former vs. current smoker | 1.51 (0.92; 2.46) | 1.35 (0.77; 2.38) |
| Never vs. current smoker | 1.49 (0.84; 2.64) | 1.45 (0.76; 2.78) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becker, L.; Negash, S.; Kartschmit, N.; Kluttig, A.; Mikolajczyk, R. Association between Parenthood and Health Behaviour in Later Life—Results from the Population-Based CARLA Study. Int. J. Environ. Res. Public Health 2022, 19, 82. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010082
Becker L, Negash S, Kartschmit N, Kluttig A, Mikolajczyk R. Association between Parenthood and Health Behaviour in Later Life—Results from the Population-Based CARLA Study. International Journal of Environmental Research and Public Health. 2022; 19(1):82. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010082
Chicago/Turabian StyleBecker, Lisa, Sarah Negash, Nadja Kartschmit, Alexander Kluttig, and Rafael Mikolajczyk. 2022. "Association between Parenthood and Health Behaviour in Later Life—Results from the Population-Based CARLA Study" International Journal of Environmental Research and Public Health 19, no. 1: 82. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010082