
Association of Rural Hospital Admissions with Access, Treatment, and Mortality for Patients with Acute Myocardial Infarction in Shanxi, China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Transparency
2.2. Data Sources
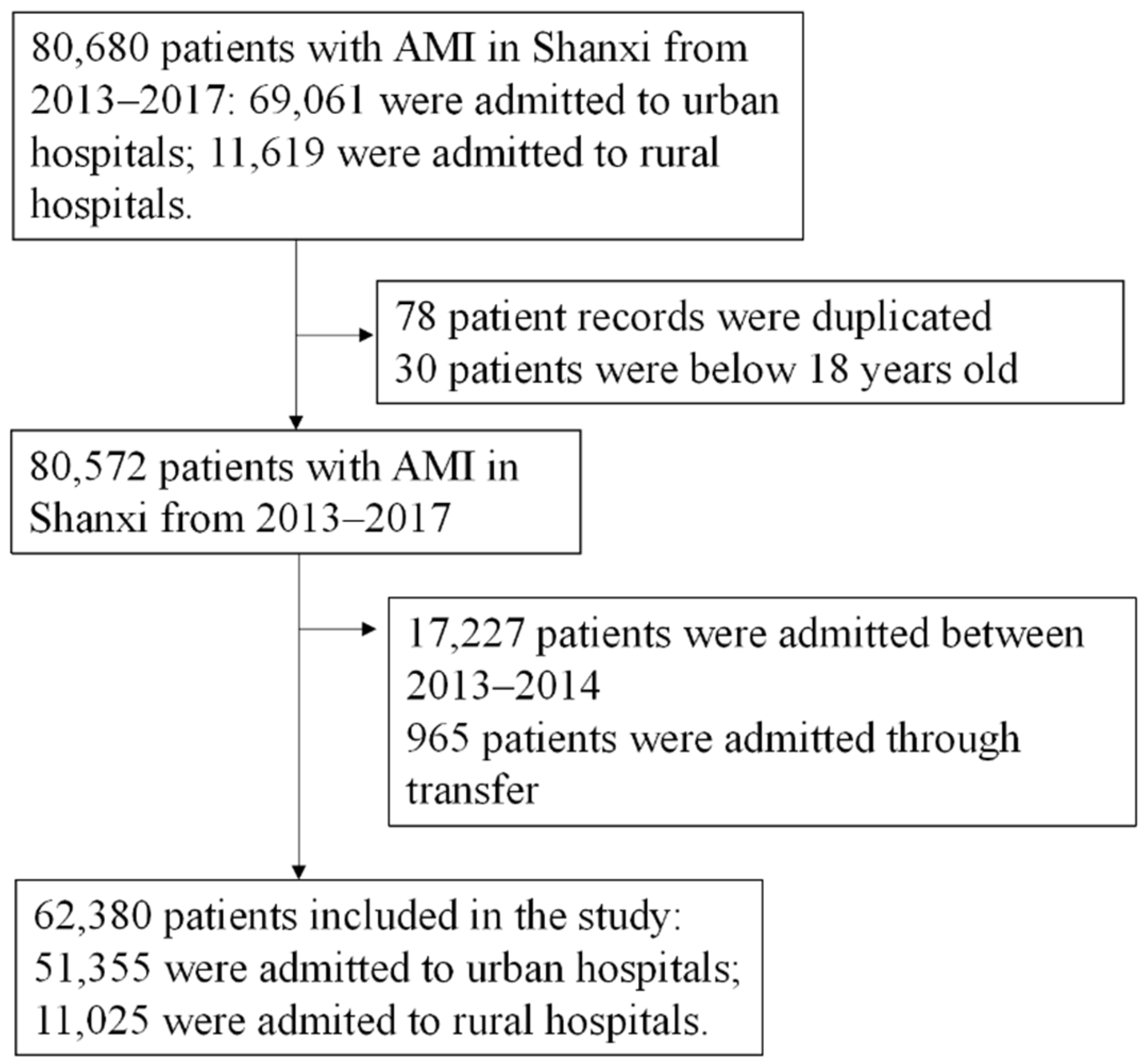
2.3. Patient Selection
2.4. Patient and Public Involvement
2.5. Outcomes
2.6. Rural and Urban Classifications
2.7. Statistical Analysis
2.8. Evaluation of IV Assumptions
3. Results
3.1. Patient Characteristics
3.2. OLS Comparison
3.3. IV Comparison
3.4. Evaluation of the Instrument
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Loccoh, E.C.; Joynt Maddox, K.E.; Wang, Y.; Kazi, D.S.; Yeh, R.W.; Wadhera, R.K. Rural-Urban Disparities in Outcomes of Myocardial Infarction, Heart Failure, and Stroke in the United States. J. Am. Coll. Cardiol. 2022, 79, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Bhuyan, S.S.; Wang, Y.; Opoku, S.; Lin, G. Rural-urban differences in acute myocardial infarction mortality: Evidence from Nebraska. J. Cardiovasc. Dis. Res. 2013, 4, 209–213. [Google Scholar] [CrossRef] [PubMed]
- James, P.A.; Li, P.; Ward, M.M. Myocardial infarction mortality in rural and urban hospitals: Rethinking measures of quality of care. Ann. Fam. Med. 2007, 5, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kang, D.R.; Kim, I.; Lee, K.; Jo, H.; Koh, S.B. Comparison between urban and rural mortality in patients with acute myocardial infarction: A nationwide longitudinal cohort study in South Korea. BMJ Open 2020, 10, e035501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alghanem, F.; Clements, J.M. Narrowing performance gap between rural and urban hospitals for acute myocardial infarction care. Am. J. Emerg. Med. 2020, 38, 89–94. [Google Scholar] [CrossRef] [PubMed]
- GDP per Capita. Available online: https://data.worldbank.org/indicator/NY.GDP.MKTP.CD (accessed on 1 August 2021).
- Cai, M.; Liu, E.; Li, W. Rural versus urban patients: Benchmarking the outcomes of patients with acute myocardial infarction in Shanxi, China from 2013 to 2017. Int. J. Environ. Res. Public Health 2018, 15, 1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Yang, Y.; Wang, C.; Yang, J.; Li, W.; Zhang, X.; Ye, Y.; Dong, Q.; Fu, R.; Sun, H.; et al. China Acute Myocardial Infarction Registry Investigators. Association of hospital-level differences in care with outcomes among patients with acute ST-segment elevation myocardial infarction in China. JAMA Netw. Open 2020, 3, e2021677. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Murugiah, K.; Li, J.; Masoudi, F.A.; Chan, P.S.; Hu, S.; Spertus, J.A.; Wang, Y.; Downing, N.S.; Krumholz, H.M.; et al. Urban–rural comparisons in hospital admission, treatments, and outcomes for ST-segment-elevation myocardial infarction in China from 2001 to 2011: A retrospective analysis from the China PEACE study (Patient-Centered Evaluative Assessment of Cardiac Events). Circulation 2017, 10, e003905. [Google Scholar] [CrossRef] [PubMed]
- Henry, T.D.; Jollis, J.G. Lessons learned from acute myocardial infarction care in China. JAMA Netw. Open 2020, 3, e2021768. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.; Kreif, N.; Grieve, R.; Sutton, M.; Sekhon, J.S. Estimating causal effects: Considering three alternatives to difference-in-differences estimation. Health Serv. Outcomes Res. Methodol. 2016, 16, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Sanwald, A.; Schober, T. Follow your heart: Survival chances and costs after heart attacks-An instrumental variable approach. Health Serv. Res. 2017, 52, 16–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keele, L.; Small, D. Instrumental variables: Don’t throw the baby out with the bathwater. Health Serv. Res. 2019, 54, 543–546. [Google Scholar] [CrossRef] [PubMed]
- McClellan, M.; McNeil, B.J.; Newhouse, J.P. Does more intensive treatment of acute myocardial infarction in the elderly reduce mortality? Analysis using instrumental variables. JAMA 1994, 272, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Newhouse, J.P.; McClellan, M. Econometrics in outcomes research: The use of instrumental variables. Ann. Rev. Public Health 1998, 19, 17–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Shi, L.; Xue, M.; Wang, N.; Dong, X.; Cai, Y.; Chen, J.; Zhu, W.; Xu, H.; Meng, Q. Geographic variations in-hospital mortality and use of percutaneous coronary intervention following acute myocardial infarction in China: A nationwide cross-sectional analysis. J. Am. Heart Assoc. 2018, 7, e008131. [Google Scholar] [CrossRef]
- Keeley, E.C.; Boura, J.A.; Grines, C.L. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: A quantitative review of 23 randomised trials. Lancet 2003, 361, 13–20. [Google Scholar] [CrossRef]
- Cutler, D.M. The lifetime costs and benefits of medical technology. J. Health Econ. 2007, 26, 1081–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coscia, T.; Nestelberger, T.; Boeddinghaus, J.; Lopez-Ayala, P.; Koechlin, L.; Miró, Ò.; Keller, D.I.; Strebel, I.; Sanchez, A.Y.; Okamura, B.; et al. Characteristics and Outcomes of Type 2 Myocardial Infarction. JAMA Cardiol. 2022, 7, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Furie, N.; Israel, A.; Gilad, L.; Neuman, G.; Assad, F.; Ben-Zvi, I.; Grossman, C. Type 2 myocardial infarction in general medical wards. Medicine 2019, 98, e17404. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Admitted to Urban Hospitals (n = 51,355) | Admitted to Rural Hospitals (n = 11,025) | p Value |
|---|---|---|---|
| Age, y (SD) | 61.82 (12.76) | 63.08 (12.62) | <0.0001 |
| Female, no. (%) | 12,869 (25.1) | 3037 (27.93) | <0.0001 |
| Farmers, no. (%) | 26,013 (50.65) | 8924 (80.94) | <0.0001 |
| Insurance, no. (%) | |||
| UEBMI | 17,631 (34.33) | 1542 (13.99) | <0.0001 |
| URBMI | 3561 (6.93) | 456 (4.14) | <0.0001 |
| NCMS | 22,700 (44.20) | 7662 (69.50) | <0.0001 |
| Other insurance | 1445 (2.81) | 71 (0.64) | 0.0002 |
| No insurance | 5034 (9.80) | 954 (8.65) | <0.0001 |
| Diabetes, no. (%) | 11,641 (22.67) | 1775 (16.10) | <0.0001 |
| Hypertension, no. (%) | 25,332 (49.33) | 4789 (43.44) | <0.0001 |
| Stroke, no (%) | 6115 (11.91) | 869 (7.88) | <0.0001 |
| STEMI | 8308 (16.18) | 648 (5.88) | <0.0001 |
| NSTEMI | 43,047 (83.82) | 10,377 (94.12) | <0.0001 |
| Primary Outcomes | |||
| Mortality rate (SD) | 0.021 (0.14) | 0.021 (0.14) | 0.541 |
| Length of stay (SD) | 11.10 (6.35) | 8.95 (7.38) | <0.0001 |
| 30-day readmission rate (SD) | 0.005 (0.07) | 0.005 (0.07) | 0.865 |
| Inpatient spending (SD) | <0.0001 | ||
| Total expenditure | 32,397.12 (26,093.17) | 13,365.53 (16,056.45) | <0.0001 |
| Out-of-pocket expenditure | 7628.12 (17,536.25) | 575.62 (2454.21) | <0.0001 |
| Secondary Outcomes, no. (%) | |||
| PCI rate | 23,275 (45.32) | 1203 (10.91) | <0.0001 |
| Fibrinolysis | 1099 (2.14) | 23 (0.21) | <0.0001 |
| Coronary angiography | 25,306 (49.28) | 1348 (12.23) | <0.0001 |
| Medication only | 19,694 (38.35) | 9364 (84.93) | <0.0001 |
| OLS | IV | |||||
|---|---|---|---|---|---|---|
| Primary Outcomes | Being Admitted to Rural Hospitals | SE | p Value | Being Admitted to Rural Hospitals | SE | p Value |
| Mortality | 0.002 | 0.002 | 0.346 | 0.053 | 0.021 | 0.011 |
| Length of stay | −1.606 | 0.074 | <0.0001 | −6.436 | 0.994 | <0.0001 |
| 30-day cardiac readmission | −0.001 | 0.001 | 0.107 | 0.003 | 0.01 | 0.79 |
| Total inpatient spending | −15,985.7 | 272.6 | <0.0001 | −44,846 | 3870 | <0.0001 |
| Out-of-pocket spending | −6882.6 | 175.7 | <0.0001 | −46,839 | 3115 | <0.0001 |
| Secondary Outcomes | ||||||
| PCI rate | −0.316 | 0.005 | <0.0001 | −0.598 | 0.069 | <0.0001 |
| Fibrinolysis | −0.018 | 0.002 | <0.0001 | −0.188 | 0.022 | <0.0001 |
| Coronary Angiography | −0.344 | 0.005 | <0.0001 | −0.357 | 0.067 | <0.0001 |
| Medication only | 0.43 | 0.005 | <0.0001 | 0.718 | 0.067 | <0.0001 |
| Characteristics | Admitted to Hospitals Below Median Distance (n = 31,191) | Admitted to Hospitals Above Median Distance (n = 31,189) | p Value |
|---|---|---|---|
| Age, y (SD) | 62.02 (12.8) | 62.07 (12.6) | 0.059 |
| Female, no. (%) | 7761 (24.9) | 8145 (26.2) | 0.0003 |
| Farmers, no. (%) | 14,510 (46.5) | 20,427 (65.5) | <0.0001 |
| Insurance, no. (%) | |||
| UREMI | 11,021 (35.33) | 8152 (26.1) | <0.0001 |
| URBMI | 2434 (7.8) | 1583 (5.1) | <0.0001 |
| NCMS | 12,124 (38.9) | 18,238 (58.5) | <0.0001 |
| Other insurance | 1081 (3.47) | 435 (1.39) | <0.0001 |
| No insurance | 3767 (12.08) | 2221 (7.12) | <0.0001 |
| Diabetes, no. (%) | 7208 (23.1) | 6208 (19.9) | <0.0001 |
| Hypertension, no. (%) | 15,168 (48.6) | 14,953 (47.9) | 0.09 |
| Stroke, no (%) | 3541 (11.4) | 3443 (11.0) | 0.21 |
| STEMI | 5444 (17.45) | 3512 (11.26) | <0.0001 |
| NSTEMI | 25,747 (82.55) | 27,677 (88.74) | <0.0001 |
| Primary Outcomes | |||
| Mortality rate (SD) | 0.019 (0.14) | 0.022 (0.15) | 0.032 |
| Length of stay (SD) | 10.9 (6.77) | 10.47 (6.41) | <0.0001 |
| 30-day readmission rate (SD) | 0.005 (0.07) | 0.005 (0.07) | 0.57 |
| Inpatient spending (SD) | |||
| Total expenditure | 30,771.6 (26,924.9) | 27,285.3 (24,219.5) | <0.0001 |
| Out-of-pocket expenditure | 7849.4 (18,027.6) | 4913.8 (13,915.5) | <0.0001 |
| Secondary Outcomes, no. (%) | |||
| PCI rate | 12,704 (0.40) | 11,774 (0.38) | <0.0001 |
| Fibrinolysis | 736 (2.36) | 386 (1.24) | <0.0001 |
| Coronary angiography | 13,548 (43.44) | 13,106 (42.02) | <0.0001 |
| Medication only | 13,902 (44.57) | 15,156 (48.59) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tao, D.; Sun, Y. Association of Rural Hospital Admissions with Access, Treatment, and Mortality for Patients with Acute Myocardial Infarction in Shanxi, China. Int. J. Environ. Res. Public Health 2022, 19, 6382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116382
Tao D, Sun Y. Association of Rural Hospital Admissions with Access, Treatment, and Mortality for Patients with Acute Myocardial Infarction in Shanxi, China. International Journal of Environmental Research and Public Health. 2022; 19(11):6382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116382
Chicago/Turabian StyleTao, Ding, and Ya Sun. 2022. "Association of Rural Hospital Admissions with Access, Treatment, and Mortality for Patients with Acute Myocardial Infarction in Shanxi, China" International Journal of Environmental Research and Public Health 19, no. 11: 6382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116382