
Reflexive Practice as an Approach to Improve Healthcare Delivery for Indigenous Peoples: A Systematic Critical Synthesis and Exploration of the Cultural Safety Education Literature


Abstract
:1. Introduction
Reflexivity and Cultural Safety
- How is reflexivity conceptualised within cultural safety educational interventions?
- Where and how is reflexivity included as part of learning outcomes in educational interventions?
- What types of pedagogical approaches are used in cultural safety educational interventions to help students develop reflexive skills?
- How is the development of reflexivity as a skill assessed?
2. Materials and Methods
2.1. Data Sources and Search Strategies
2.2. Eligibility Criteria
2.3. Article Review
2.4. Data Extraction
3. Results
3.1. Summary of Educational Interventions
3.2. Definitions of Cultural Safety
3.3. Definition of Reflexivity
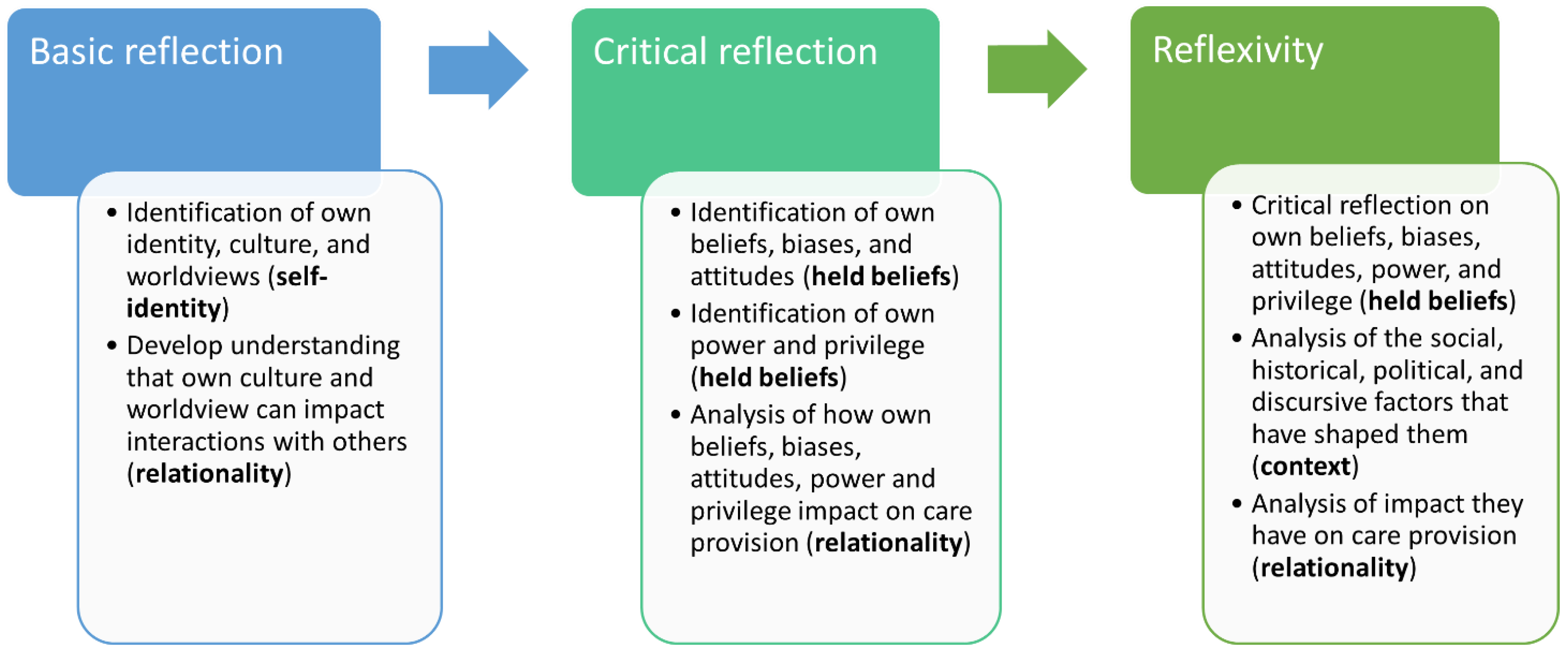
3.4. Conceptualisations of Reflexivity
3.4.1. Sub-Theme 1: Self-Identity
“Participants were therefore encouraged to…explore their own culture, values, and beliefs [and] acknowledge difference”[17] (p. 248)
“[Cultural safety] requires registered nurses to reflect on their own cultural identity and practice in a way that affirms the culture of clients and co-workers”[21] (p. 3)
“This includes understanding your own worldview and how your values and beliefs influence the way you perceive other people”[57] (p. 88)
“[Students will] reflect on their own cultural background and their life experiences including the development of values and attitudes that have shaped their thinking and behaviours”[23] (p. 120)
3.4.2. Sub-Theme 2: Held Beliefs
“…highlighted the importance of health providers reflecting on and questioning their own assumptions about Aboriginal people that can impact on the care they provide”.[90] (p. 3, emphasis added)
“…learners were encouraged to reflect on their own cultural values or emotional responses to diverse histories, cultures, worldviews, values, and contemporary events related to Indigenous people”[32] (p. e2, emphasis added)
3.4.3. Sub-Theme 3: Relationality
“…students reflected on their own place-based identity (i.e., who they were, where they came from) and recognized how their own personal biases were unintentionally but significantly brought into practice and how those biases influenced their work and social interactions”[31] (p. 187)
“…notice our own cultural practices and individual behaviours and the impact these may have on Aboriginal and Torres Strait Islander people”[87] (p. 23)
3.4.4. Sub-Theme 4: Context
“Become aware of their own social conditioning, their (often privileged) status, and how their conditioning and status can affect their interactions with clients”[59] (p.179)
3.5. Where and How Reflexivity Is Included as a Learning Outcome
Specific aims of the day were to facilitate students in:
“Our goal was to study whether expanding the clinic beyond the classroom and into a Métis community would make the students more aware of their own identity and worldviews, how they may be different from those in that community, and how they shape their stereotypes and misperceptions of peoples from other cultures”.[58] (p. 147)
3.6. Pedagogical Approaches to Facilitate Reflexivity
3.6.1. Objects
“… the session includes a semi-formal lecture in a quieter space of the gallery … student literature reviews, gallery exploration, and a group reflective discussion”.[30] (p. 37)
“The tutorial format was tightly structured and included the viewing of a vodcast (prepared specifically for the unit and featuring Aboriginal speakers), discussion of issues arising, case studies, and periodic presentations by students. … Guidelines [were] developed by students [to facilitate classroom discussions, to ensure] that consideration be given to experiences and background that may influence attitudes expressed”.[23] (pp. 115–116)
3.6.2. People
“Cultural immersion is an experiential approach to learning about culture and social situations. In medical education this type of approach is beginning to be recognized for its potential to raise consciousness among students; expose tacit inappropriate biases, including racism; help students learn about themselves and other cultures; and assist students in their preparation for work in culturally diverse settings”.[26] (p. 3)
“Having the opportunity to be taught by and interact with an Indigenous academic is thought to have a major role in reducing stereotypes and negative attitudes about Indigenous Australians … Our objective was to present an Indigenous informed perspective filling in the gaps of knowledge that have resulted from silencing Indigenous peoples, their stories and experiences. We wanted to provide students with some positive and affirming images of the strength and resilience of Australian Indigenous peoples”.[55] (pp. 105–107)
3.6.3. Indigenous Pedagogical Practices
“field experiences can provide students with a first-hand account of the ‘ways of knowing, being, and doing’ …that is, communicating with and listening to Aboriginal Elders, practitioners and community members provides a deeper analysis of social work practice through assessing the cultural context, yarning and storying”[54] (p. 199)
“A yarning circle approach was used to privilege First Peoples’ culture and voice. First Peoples have recognised yarning as a method of sharing stories, information and knowledge for generations”.[17] (pp. 247–248)
3.7. Assessment of Reflexivity
“Students subsequently submitted a critical self-reflection exploring their personal learnings, including reflections on assumptions, discomfort and realisations”.[38] (p. 6)
“The idea that students would be given a ‘real world’ experience, be required to reflect on what they had observed and what they had learnt, with supporting literature, was vital to identifying elements of changing attitudes and effectiveness of learning. Furthermore, students then had to plan how they would use their new knowledge in future practice contexts”.[54] (p. 201)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Awofeso, N. Racism: A major impediment to optimal Indigenous health and health care in Australia. Aust. Indig. Healthbull. 2011, 11, 14. [Google Scholar]
- Jennings, W.; Bond, C.; Hill, P.S. The power of talk and power in talk: A systematic review of Indigenous narratives of culturally safe healthcare communication. Aust. J. Prim. Health 2018, 24, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Power, T.; Geia, L.; Adams, K.; Drummond, A.; Saunders, V.; Stuart, L.; Deravin, L.; Tuala, M.; Roe, Y.; Sherwood, J.; et al. Beyond 2020: Addressing racism through transformative Indigenous health and cultural safety education. J. Clin. Nurs. 2021, 30, e32–e35. [Google Scholar] [CrossRef] [PubMed]
- Kairuz, C.A.; Casanelia, L.M.; Bennett-Brook, K.; Coombes, J.; Yadav, U.N. Impact of racism and discrimination on physical and mental health among Aboriginal and Torres Strait islander peoples living in Australia: A systematic scoping review. BMC Public Health 2021, 21, 1302. [Google Scholar] [CrossRef]
- Temple, J.B.; Kelaher, M.; Paradies, Y. Prevalence and context of racism experienced by older Aboriginal and Torres Strait Islanders. Aust. J. Ageing 2019, 38, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Ziersch, A.M.; Gallaher, G.; Baum, F.; Bentley, M. Responding to racism: Insights on how racism can damage health from an urban study of Australian Aboriginal people. Soc. Sci. Med. 2011, 73, 1045–1053. [Google Scholar] [CrossRef]
- Findling, M.G.; Casey, L.S.; Fryberg, S.A.; Hafner, S.; Blendon, R.J.; Benson, J.M.; Sayde, J.M.; Miller, C. Discrimination in the United States: Experiences of Native Americans. Health Serv. Res. 2019, 54, 1431–1441. [Google Scholar] [CrossRef] [Green Version]
- Phillips-Beck, W.; Eni, R.; Lavoie, J.G.; Kinew, K.A.; Achan, G.K.; Katz, A. Confronting racism within the canadian healthcare system: Systemic exclusion of first nations from quality and consistent care. Int. J. Environ. Res. Public Health 2020, 17, 8343. [Google Scholar] [CrossRef]
- Reid, P.; Cormack, D.; Paine, S.J. Colonial histories, racism and health—The experience of Māori and Indigenous peoples. Public Health 2019, 172, 119–124. [Google Scholar] [CrossRef]
- Papps, E.; Ramsden, I. Cultural Safety in Nursing: The New Zealand Experience. Int. J. Qual. Health Care 1996, 8, 491–497. [Google Scholar] [CrossRef] [Green Version]
- Ramsden, I. Kawa Whakaruruhau: Cultural Safety in Nursing Education in Aotearoa; I. M. Ramsden: Aotearoa, New Zealand, 1990. [Google Scholar]
- Australian Health Practitioner Regulation Agency. The National Scheme’s Aboriginal and Torres Strait Islander Health and Cultural Safety Strategy 2020–2025; Australian Health Practitioner Regulation Agency: Sydney, Australia, 2020; pp. 1–28.
- Curtis, E.; Jones, R.; Tipene-Leach, D.; Walker, C.; Loring, B.; Paine, S.-J.; Reid, P. Why cultural safety rather than cultural competency is required to achieve health equity: A literature review and recommended definition. Int. J. Equity Health 2019, 18, 174. [Google Scholar] [CrossRef] [PubMed]
- Laverty, M.; McDermott, D.R.; Calma, T. Embedding cultural safety in Australia’s main health care standards. Med. J. Aust. 2017, 207, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Withall, L.; Ryder, C.; Mackean, T.; Edmondson, W.; Sjoberg, D.; McDermott, D.R.; Wilson, A. Assessing cultural safety in Aboriginal and Torres Strait Islander Health. Aust. J. Rural Health 2021, 29, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Arnold, O.; Appleby, L.; Heaton, L. Incorporating cultural safety in nursing education. Nurs. BC 2008, 40, 14–17. [Google Scholar]
- Fleming, T.; Creedy, D.K.; West, R. Impact of a continuing professional development intervention on midwifery academics’ awareness of cultural safety. Women Birth 2017, 30, 245–252. [Google Scholar] [CrossRef]
- Hart, B.; Cavanagh, M.; Douglas, D. The “Strengthening Nursing Culture Project”—An exploratory evaluation study of nursing students’ placements within Aboriginal Medical Services. Contemp Nurse 2015, 51, 245–256. [Google Scholar] [CrossRef]
- Hulko, W.; Mahara, M.S.; Wilson, D.; Campbell-McArthur, G. Culturally safe dementia care: Building nursing capacity to care for First Nation Elders with memory loss. Int. J. Older People Nurs. 2021, 16, e12395–e12410. [Google Scholar] [CrossRef]
- Kelly, J.; Wilden, C.; Chamney, M.; Martin, G.; Herman, K.; Russell, C. Improving cultural and clinical competency and safety of renal nurse education. Ren. Soc. Australas. J. 2016, 12, 106–112. [Google Scholar]
- Mahara, M.S.; Duncan, S.M.; Whyte, N.; Brown, J. It Takes a Community to Raise a Nurse: Educating for Culturally Safe Practice with Aboriginal Peoples. Int. J. Nurs. Educ. Sch. 2011, 8, 1–13. [Google Scholar] [CrossRef]
- Power, T.; Lucas, C.; Hayes, C.; Jackson, D. ‘With my heart and eyes open’: Nursing students′ reflections on placements in Australian, urban Aboriginal organisations. Nurse Educ. Pract. 2020, 49, 1–6. [Google Scholar] [CrossRef]
- Thackrah, R.D.; Thompson, S.C. Confronting uncomfortable truths: Receptivity and resistance to Aboriginal content in midwifery education. Contemp Nurse 2013, 46, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Carriage, C.; Akers, J.; Payne, K. An Immersive Model of Learning in Aboriginal Community Controlled Services for MBBS Students. In LIME Good Practice Case Studies Volume Four; Leaders in Indigenous Medical Education Network; Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne: Melbourne, Australia, 2017; pp. 32–37. Available online: https://limenetwork.net.au/resources-hub/good-practice-case-studies/ (accessed on 14 September 2020).
- Crampton, P.; Dowell, A.; Parkin, C.; Thompson, C. Combating effects of racism through a cultural immersion medical education program. Acad. Med. 2003, 78, 595–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hudson, G.L.; Maar, M. Faculty analysis of distributed medical education in Northern Canadian Aboriginal communities. Rural Remote Health 2014, 14, 2664. [Google Scholar] [CrossRef]
- Paul, D.; Austen, L.; Groves, D.; Isaacs, K.; Walley, C. Important business: Community Engagement and learning on Country. In LIME Good Practice Case Studies Volume Five; Leaders in Indigenous Medical Education Network; Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne: Melbourne, Australia, 2019; pp. 35–48. [Google Scholar]
- Ryder, C.; Yarnold, D.; Hayes, C.; MacKean, L.; Sjoberg, D.; Porter, M. Demonstrating cultural safety in communication through standardised role play. In LIME Good Practice Case Studies Volume Two; Onmeda VicHealth Koori Health Unit, University of Melbourne: Melbourne, Australia, 2013; pp. 19–23. [Google Scholar]
- Chiodo, L.N.; Sonn, C.C.; Morda, R. Implementing an Intercultural Psychology Undergraduate Unit: Approach, Strategies, and Outcomes. Aust. Psychol. 2014, 49, 181–192. [Google Scholar] [CrossRef]
- Bolton, J.; Andrews, S. ‘I learned more than from any lecture’—Indigenous place and space for teaching Indigenous health to physiotherapy students. Phys. Ther. Rev. 2018, 23, 35–39. [Google Scholar] [CrossRef]
- Demers, M.; Phenix, A.; Schmitz, C.; Storr, C. Socially Accountable Canadian Occupational Therapy Fieldwork with Indigenous Peoples: Where Are We At? Occup. Ther. Health Care 2021, 35, 182–197. [Google Scholar] [CrossRef]
- Jamieson, M.; Chen, S.-P.; Murphy, S.; Maracle, L.; Mofina, A.; Hill, J. Pilot testing an intervention on cultural safety and indigenous health in a canadian occupational therapy curriculum. J. Allied Health 2017, 46, e1–e7. [Google Scholar]
- McCartan, J.; Dart, J.; Adams, K.; Davidson, Z.; Brimblecombe, J. Can integrating Aboriginal health content in undergraduate nutrition curricula foster student cultural capabilities? High. Educ. Res. Dev. 2021, 40, 325–340. [Google Scholar] [CrossRef]
- Kurtz, D.L.M.; Janke, R.; Vinek, J.; Wells, T.; Hutchinson, P.; Froste, A. Health Sciences cultural safety education in Australia, Canada, New Zealand, and the United States: A literature review. Int. J. Med. Educ 2018, 9, 271–285. [Google Scholar] [CrossRef] [Green Version]
- Australian Indigenous Doctors’ Association. AIDA’s Cultural Safety Training. Available online: https://aida.org.au/cultural-safety-program/what-is-cultural-safety/ (accessed on 20 February 2022).
- Royal Australian College of General Practitioners. Cultural Awareness and Cultural Safety Training; RACGP: Melbourne, Australia, 2011; Available online: https://www.racgp.org.au/the-racgp/faculties/atsi/education-and-training/cpd-activities-for-gps-and-health-professionals/cultural-awareness-and-cultural-safety-training (accessed on 14 May 2020).
- San’yas. San’yas Anti-Racism Indigenous Cultural Safety Training Program. Available online: https://sanyas.ca/ (accessed on 20 February 2022).
- Delbridge, R.; Garvey, L.; Mackelprang, J.L.; Cassar, N.; Ward-Pahl, E.; Egan, M.; Williams, A. Working at a cultural interface: Co-creating Aboriginal health curriculum for health professions. High. Educ. Res. Dev. 2021, 1–16. [Google Scholar] [CrossRef]
- Lumsden, K.; Bradford, J.; Goode, J. Reflexivity: Theory, Method, and Practice, 1st ed.; Routledge: Florence, Italy, 2019; Volume 1. [Google Scholar]
- Pillow, W. Confession, catharsis, or cure? Rethinking the uses of reflexivity as methodological power in qualitative research. Int. J. Qual. Stud. Educ. 2003, 16, 175–196. [Google Scholar] [CrossRef]
- May, T.; Perry, B. Reflexivity: The Essential Guide; SAGE Publications: London, UK, 2017. [Google Scholar] [CrossRef]
- Wilson, A. Addressing Uncomfortable Issues: Reflexivity as a Tool for Culturally Safe Practice in Aboriginal and Torres Strait Islander Health. Aust. J. Indig. Educ. 2014, 43, 218–230. [Google Scholar] [CrossRef] [Green Version]
- McGough, S.; Wynaden, D.; Gower, S.; Duggan, R.; Wilson, R. There is no health without cultural safety: Why cultural safety matters. Contemp Nurse 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ramsden, I. Cutural Safety and Nursing Education in Aotearoa and Te Waipounamu. Ph.D. Thesis, Victoria University, Wellington, New Zealand, 2002. [Google Scholar]
- Beagan, B.L. Approaches to culture and diversity: A critical synthesis of occupational therapy literature: Des approches en matière de culture et de diversité: Une synthèse critique de la littérature en ergothérapie. Can. J. Occup. Ther. 2015, 82, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Cromb, N. Why Heritage Does Not Ascibe Cultural Authenticity or Authority. IndigenousX, 2021. Available online: https://indigenousx.com.au/why-heritage-does-not-ascribe-cultural-authenticity-or-authority/ (accessed on 20 March 2022).
- Heckenberg, S. Cultural safety: A model and method that reflects us, respects us and represents us. J. Aust. Indig. Issues 2020, 23, 48–66. [Google Scholar]
- McDermott, D.R.; Sjoberg, D. Managing a Diverse Student Discomfort with an Indigenous Health Curriculum. In LIME Good Practice Case Studies Volume One; Onmeda VicHealth Koori Health Unit, University of Melbourne: Melbourne, Australia, 2012; pp. 26–28. [Google Scholar]
- Mills, K.; Creedy, D.K. The ’Pedagogy of discomfort’: A qualitative exploration of non-indigenous student learning in a First Peoples health course. Aust. J. Indig. Educ. 2019, 50, 29–37. [Google Scholar] [CrossRef]
- Mills, K.; Creedy, D.K.; West, R. Experiences and outcomes of health professional students undertaking education on Indigenous health: A systematic integrative literature review. Nurse Educ. Today 2018, 69, 149–158. [Google Scholar] [CrossRef]
- Castell, E.; Bullen, J.; Garvey, D.; Jones, N. Critical Reflexivity in Indigenous and Cross-cultural Psychology: A Decolonial Approach to Curriculum? Am. J. Community Psychol. 2018, 62, 261–271. [Google Scholar] [CrossRef]
- Drummond, A. Embodied Indigenous knowledges protecting and privileging Indigenous peoples’ ways of knowing, being and doing in undergraduate nursing education. Aust. J. Indig. Educ. 2020, 49, 127–134. [Google Scholar] [CrossRef]
- Faulkner, J.; Crowhurst, M. ‘So far multicultural that she is racist to Australians’: Discomfort as a pedagogy for change. Pedagog. Cult. Soc. 2014, 22, 389–403. [Google Scholar] [CrossRef]
- Duthie, D.; King, J.; Mays, J. Raising awareness of Australian Aboriginal peoples reality: Ambedding Aboriginal knowledge in social work education through the use of field experiences. Int. Educ. J. Comp. Perspect. 2013, 12, 197–212. [Google Scholar]
- Jackson, D.; Power, T.; Sherwood, J.; Geia, L. Amazingly resilient Indigenous people! Using transformative learning to facilitate positive student engagement with sensitive material. Contemp Nurse 2013, 46, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Kickett, M.; Hoffman, J.; Flavell, H. A Model for Large-Scale, Interprofessional, Compulsory Cross-Cultural Education with an Indigenous Focus. J. Allied Health 2014, 43, 38–44. [Google Scholar] [PubMed]
- Lucas, C.; Aly, M.; Power, T. Pharmacy students’ learnings and reflections to inform the development of the ’Working Respectfully with Aboriginal Peoples’ (WRAP) Toolkit. Reflective Pract. 2021, 22, 86–100. [Google Scholar] [CrossRef]
- Oosman, S.; Durocher, L.; Roy, T.; Nazarali, J.; Potter, J.; Schroeder, L.; Sehn, M.; Stout, K.; Abonyi, S. Essential elements for advancing cultural humility through a community-based physical therapy practicum in a metis community. Physiother. Can. 2019, 71, 146–157. [Google Scholar] [CrossRef]
- Bernhardt, B.M.; Green, E.; Khurana, A.; Laporte, T.; Osmond, S.; Panchyk, H.; Shahnaz, N.; Campbell Wood, H. Course Development at The University of British Columbia Concerning Audiology and Speech-Language Pathology for People of First Nations, Metis and Inuit Heritage. Can. J. Speech-Lang. Pathol. Audiol. 2011, 35, 178–189. [Google Scholar]
- Dowell, A.; Crampton, P.; Parkin, C. The first sunrise: An experience of cultural immersion and community health needs assessment by undergraduate medical students in New Zealand. Med. Educ. 2001, 35, 242–249. [Google Scholar] [CrossRef]
- Fleming, T.; Creedy, D.K.; West, R. The influence of yarning circles: A cultural safety professional development program for midwives. Women Birth 2020, 33, 175–185. [Google Scholar] [CrossRef]
- Gray, M.; Thomas, Y.; Bonassi, M.; Elston, J.; Tapia, G. Cultural safety training for allied health students in Australia. Aust. J. Indig. Educ. 2020, 50, 274–283. [Google Scholar] [CrossRef]
- Min, J.; Albon, S.; Leung, L.; Clarke, A. Creating a pharmacy elective course in Indigenous health. Curr. Pharm. Teach. Learn. 2020, 12, 1004–1013. [Google Scholar] [CrossRef]
- Nash, R.; Meiklejohn, B.; Sacre, S. The Yapunyah project: Embedding Aboriginal and Torres Strait Islander perspectives in the nursing curriculum. Contemp Nurse 2006, 22, 296–316. [Google Scholar] [CrossRef] [PubMed]
- Thackrah, R.D.; Thompson, S.C. Applying a Midwifery Lens to Indigenous Health Care Delivery: The Contribution of Campus Learning and Rural Placements to Effecting Systemic Change. Can. J. Nurs. Res. 2018, 50, 179–188. [Google Scholar] [CrossRef]
- Thorpe, K.; Burgess, C. Pedagogical approaches in a mandatory Indigenous education subject. Int. J. Learn. 2012, 18, 177–190. [Google Scholar] [CrossRef]
- Hardcastle, L.; Bradford, V. Aboriginal and Torres Strait Islander Cultural Respect Program. Aborig. Isl. Health Work. J. 2007, 31, 21–23. [Google Scholar]
- Herzog, L.S.; Wright, S.R.; Pennington, J.J.; Richardson, L. The KAIROS Blanket Exercise: Engaging Indigenous ways of knowing to foster critical consciousness in medical education. Med. Teach. 2021, 43, 1437–1443. [Google Scholar] [CrossRef] [PubMed]
- Joyce, M. Cultural safety in Aotearoa New Zealand—An overview. Whitireia Nurs. J. 1996, 3, 7–16. [Google Scholar]
- Ramsden, I. Teaching cultural safety. N. Z. Nurs. J. 1992, 85, 21–23. [Google Scholar]
- Richardson, C.; Carriere, J.; Boldo, V. Invitations to dignity and well-being: Cultural safety through indigenous pedagogy, witnessing and giving back. AlterNative Int. J. Indig. Peop. 2017, 13, 190–195. [Google Scholar] [CrossRef]
- Richardson, F.; Carryer, J. Teaching cultural safety in a New Zealand nursing education program. J. Nurs. Educ. 2005, 44, 201–208. [Google Scholar] [CrossRef]
- Sjoberg, D.; McDermott, D.R. The deconstruction exercise: An assessment tool for enhancing critical thinking in cultural safety education. Int. J. Crit. Indig. Stud. 2016, 9, 28–48. [Google Scholar] [CrossRef] [Green Version]
- The EndNote Team. EndNote X9; Clarivate: Philadelphia, PA, USA, 2013. [Google Scholar]
- Braun, V.; Clark, V. Successful Qualitative Research: A Practical Guide for Beginnners; SAGE Publications Ltd.: London, UK, 2013. [Google Scholar]
- Potter, J. Representing Reality: Discourse, Rhetoric and Social Construction; Sage: London, UK; Thousand Oaks, CA, USA, 1996. [Google Scholar]
- Gaunt, H. Friday Essay: Can Looking At art Make for Better Doctors? The Conversation: Melbourne, Australia, 2016. [Google Scholar]
- Salmon, F.; Wurm, J. The Power of Things: Enhancing Employability in Higher Education through Object-Based Learning; Australian Government Department of Education and Training: Sydney, Australia, 2019.
- Nakata, M. The Cultural Interface. Aust. J. Indig. Educ. 2007, 36, 7–14. [Google Scholar] [CrossRef]
- Maar, M.; Bessette, N.; McGregor, L.; Lovelace, A.; Reade, M. Co-creating Simulated Cultural Communication Scenarios with Indigenous Animators: An Evaluation of Innovative Clinical Cultural Safety Curriculum. J. Med. Educ. Curric. Dev. 2020, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- West, M.; Sadler, S.; Hawke, F.; Munteanu, S.E.; Chuter, V. Effect of a culturally safe student placement on students’ understanding of, and confidence with, providing culturally safe podiatry care. J. Foot Ankle Res. 2021, 14, 9. [Google Scholar] [CrossRef]
- QSR International Pty Ltd. NVivo; Version 12; QSR International Pty Ltd.: Doncaster, Australia, 2018. [Google Scholar]
- Herzog, L.S. The need for narrative reflection and experiential learning in medical education: A lesson learned through an urban indigenous health elective. Med. Teach. 2017, 39, 995–996. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.; Creedy, D.K.; Sunderland, N.; Allen, J.; Carter, A.; Corporal, S. Evaluation of a First Peoples-led, emotion-based pedagogical intervention to promote cultural safety in undergraduate non-Indigenous health professional students. Nurse Educ. Today 2022, 109, 105219. [Google Scholar] [CrossRef] [PubMed]
- NSW Government Family & Community Services. Assessment Guide: Dementia Learning Resource for Aboriginal and Torres Strait Islander Communities; NSW Government Family & Community Services: Sydney, Australia, 2007.
- NSW Government Family & Community Services. Facilitators Guide: Dementia Learning Resource for Aboriginal and Torres Strait Islander Communities; NSW Government Family & Community Services: Sydney, Australia, 2007.
- NSW Government Family & Community Services. Student Guide: Dementia Learning Resource for Aboriginal and Torres Strait Islaner Communities; NSW Government Family & Community Services: Sydney, Australia, 2007.
- Crameri, P.; Barrett, C.; Latham, J.R.; Whyte, C. It is more than sex and clothes: Culturally safe services for older lesbian, gay, bisexual, transgender and intersex people. Australas. J. Ageing 2015, 34, 21–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, M.D.J.; Ramsey, I.; Kennedy, K.; Sharplin, G.; Eckert, M. Culturally safe, high-quality breast cancer screening for transgender people: A scoping review protocol. J. Adv. Nurs. 2022, 78, 276–281. [Google Scholar] [CrossRef]
- Durey, A.; Halkett, G.; Berg, M.; Lester, L.; Kickett, M. Does one workshop on respecting cultural differences increase health professionals’ confidence to improve the care of Australian Aboriginal patients with cancer? An evaluation. BMC Health Serv Res. 2017, 17, 660. [Google Scholar] [CrossRef] [Green Version]
- The Royal New Zealand College of General Practitioners. Health Equity and Cultural Safety. Available online: https://www.rnzcgp.org.nz/RNZCGP/Dashboard/Resources/CPD_Resources/Health_equity_and_cultural_safety_?WebsiteKey=4105e6d5-9ad4-4cbf-b3d4-8a1df183be9d (accessed on 30 September 2021).
- Bond, C. When the Object Teaches: Indigenous Academics in Australian Universities. Right Now, 14 November 2014. [Google Scholar]
- Dune, T.; Crnek-Georgeson, K.; Bidewell, J.; Firdaus, R.; John, J.R. Undergraduate health science students’ development of reflective practice on communication skills via e-Portfolios. J. Univ. Teach. Learn. Pract. 2018, 15, 5. [Google Scholar] [CrossRef]
- Gopal, D.P.; Douglass, C.; Wong, S.; Khan, I.; Lokugamage, A.U. Reflexivity, Cultural Safety, and improving the health of racially minoritised communities. Lancet 2022, 399, 1581–1582. [Google Scholar] [CrossRef]
- Plaza Del Pino, F.J.; Arrogante, O.; Gallego-Gómez, J.I.; Simonelli-Muñoz, A.J.; Castro-Luna, G.; Jiménez-Rodríguez, D. Romani Women and Health: The Need for a Cultural Safety-Based Approach. Healthcare 2022, 10, 271. [Google Scholar] [CrossRef] [PubMed]
- Engnes, J.I.; Sivertsen, N.; Bongo, B.A.; Mehus, G. Sámi and Norwegian nurses’ perspectives on nursing care of Sámi patients: A focus group study on culturally safe nursing. Int. J. Circumpolar Health 2021, 80, 1948246. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference Country | Learner Level and Field of Study | Site and Type of Educational Intervention | Duration. Delivery Method | Level of Indigenous Involvement |
|---|---|---|---|---|
| Arnold et al. (2008) [16] Canada | Undergraduate nursing students. | University. Reciprocal partnership, including community placements. | Not specified. Face-to-face. | Initiated, co-designed, and co-delivered. |
| Bernhardt et al. (2011) [59] Canada | Undergraduate speech-language pathology and audiology students. | University. Unit of study, including community placement. | 8-month teaching period. 26 h in-class teaching time. 26 h out of class time. Face-to-face with some online components. | Advisory Group established. Co-designed and co-delivered. |
| Bolton and Andrews (2018) [30] Australia | Doctor of physiotherapy students. | University. Field trip within a unit of study. | Not specified. Face-to-face. | Co-designed and co-delivered. |
| Carriage et al. (2017) [24] Australia | Fifth-year medical students. | University. Rural and remote placements. | Half-day lecture followed by 5-week placement. Face-to-face. | Aboriginal Medical Service host organisations, including cultural mentoring. |
| Chiodo et al. (2014) [29] Australia | Undergraduate psychology students. | University. Unit of study. | 6-week teaching period. 2 h weekly lectures. 1 h weekly tutorials. Face-to-face. | Includes a ‘diverse teaching group’ and involvement of ‘Indigenous guest speakers.’ |
| Crampton et al. (2003) [25] Aotearoa New Zealand | Third-year medical students. | University. Cultural immersion placement. | 1 week Face-to-face. | Consultation and collaboration with local community. |
| Delbridge et al. (2021) [38] Australia | Undergraduate and postgraduate health professions students. | University. 2 discipline specific PBL modules. 1 inter-professional simulation session. | PBL modules: Pre-workshop online learning, 1 h seminar, and 3 h workshop. Simulation: Pre-session online learning, length of session not specified. Face-to-face with some online components | Co-designed involving expert knowledge holders. |
| Demers et al. (2021) [31] Canada | Undergraduate occupational therapy students. | University. Fieldwork placement. | Pre-placement self-paced learning. 8-week placement. Face-to-face with some online components. | Partnership was initiated by a community-based Indigenous OT. |
| Dowell et al. (2001) [60] Aotearoa New Zealand | Third-year medical students. | University. Cultural immersion placement; part of a unit of study. | 1 week Face-to-face. | Consultation and collaboration with local community. |
| Durey et al. (2017) [90] Australia | Health professionals (radiation oncology). | CPE. Workshop. | 2 h workshop. Face-to-face. | Co-presentation. |
| Duthie et al. (2013) [54] Australia | Master of social work students. | University. Field experience; part of a unit of study. | 1 day. Face-to-face. | Co-designed and co-delivered. |
| Fleming et al. (2017) [17] Australia | Midwifery academic educators. | CPE. Workshops and yarning circles. | 2 half-day workshops and 5 yarning circles; held over a 12-week semester. Face-to-face. | Co-designed and co-delivered. |
| Gray et al. (2020) [62] Australia | Undergraduate allied health students. | University. Workshop. | 1 day. Face-to-face. | Co-designed and co-delivered. |
| Hardcastle and Bradford (2007) [67] Australia | Nurses and other health professionals. | CPE. Online module. | 6 self-paced learning modules. Online (web-based training programme). | Initiated, co-designed, and co-delivered. |
| Hart et al. (2015) [18] Australia | Undergraduate nursing students. | University. Pre-placement unit. Placement (urban, rural, and remote locations). | Pre-placement semester unit of study. Placement (5 weeks). Face-to-face. | Collaboration and consultation with Aboriginal Medical Services to set up placements. |
| Herzog (2017) [83] Canada | Fourth-year medical students. | University. Elective unit of study. | 4 weeks. Face-to-face. | Development and delivery of learning. |
| Herzog et al. (2021) [68] Canada | Second-year medical students. | University. Class activity. | Not specified. Face-to-face | Not specified. |
| Hudson and Maar (2014) [26] Canada | First-year medical students. | University. Pre-placement preparation. Placement in community. | 4 weeks (total) 2-week placement in Aboriginal community. 2-week follow-up on campus. Face-to-face with some online components. | Co-designed, co-delivered, and co-evaluation. |
| Hulko et al. (2021) [19] Canada | Health professionals (nurses working with dementia patients). | CPE. Module. | Self-paced, equivalent to 8–10 h completed over 8 weeks. Online and face-to-face components. | Co-designed and co-delivered. |
| Jackson et al. (2013) [55] Australia | Masters-level postgraduate health professions students. | University. Workshop within a compulsory subject. | 1 day; 7 discrete sessions. Face-to-face. | Co-designed and co-delivered. |
| Jamieson et al. (2017) [32] Canada | First-year occupational therapy students. | University. Modules included in a first year OT course. | 3 × 1 h modules. Face-to-face. | Co-designed and co-delivered. |
| Joyce (1996) [69] Aotearoa New Zealand | Undergraduate nursing students. | University. Scaffolded and integrated curriculum across undergraduate programme. | 3-year curriculum. Approximately 252 h total across 3600 h of teaching. Face-to-face. | Co-delivery of teaching. |
| Kelly et al. (2016) [20] Australia | Renal health training for new and current nursing staff. | CPE. Workshop (pilot and evaluation). | Aim is to offer a 1-day workshop. Face-to-face. | Not specified. |
| Kickett et al. (2014) [56] Australia | First-year health sciences students. | University. Integrated curricula. | 12-week semester. 2 h weekly tutorials. Offered in two formats: fully online; and face-to-face with some online components. | Co-coordination. Delivery of teaching. |
| Lucas et al. (2021) [57] Australia | Master of pharmacy students. | University. Immersive workshop. | 8 h. Face-to-face. | Co-designed and co-delivered. |
| Maar et al. (2020) [80] Canada | Pre-clerkship medical students. | University. Simulated clinical scenarios. | 15-min interview and 20-min debrief interview. Face-to-face. | Co-designed and co-delivered. |
| Mahara et al. (2011) [21] Canada | Baccalaureate nursing students. | University. Proposed curriculum. Scaffolded and integrated curriculum across the programme; includes a community placement. | 4-year curriculum. Total amount of time not specified. Proposed activities would be face-to-face. | Conceptualisation, planning, and development. |
| McCartan et al. (2021) [33] Australia | First-year nutrition science students. | University. Integrated curriculum across first year. | Integrated across 4 semester-long first-year subjects. Face-to-face. | Co-designed. |
| Mills et al. (2022) [84] Australia | Undergraduate health sciences students. | University. Semester-long unit of study. | Four 3 h workshops across a 12-week unit. 1 face-to-face workshop; 3 online workshops (due to COVID-19). | Co-designed and co-delivered. |
| Min et al. (2020) [63] Canada | Third- and fourth-year pharmacy students. | University. One-semester unit of study; includes experiential learning activities. | 3 h per week; 36 h total. Face-to-face. | Co-designed and co-delivered. |
| Nash et al. (2006) [64] Australia | Undergraduate nursing students. | University. Scaffolded and integrated curricula across the programme of study. | Seven units across the programme had content embedded; five were practical placements. Face-to-face with online components. | Consultation and collaboration in the development. |
| NSW Government Family and Community Services (2007) [85,86,87] Australia | Not specified. | Vocational training. Units of study within a Certificate III in Aged Care. | 5-day workshop. Face-to-face. | Contributed to resource development. Required as assessor(s). |
| Oosman et al. (2019) [58] Canada | Master of physical therapy students. | University. Pre-placement orientation session. Placement in community. | Varied length, 2–4-week placements. 2 days per week in a health facility, 3 days per week in community. Face-to-face. | Design and delivery of community practicum. |
| Paul et al. (2019) [27] Australia | Medical students, first to fourth year. | University. Vertically and horizontally integrated curriculum. | Activities included in the curriculum vary between 1 h (smoking ceremony and welcome to country) and 8-weeks (rural GP and psychiatry rotation). Face-to-face. | Aboriginal health team responsible for coordination, development, implementation, and evaluation. |
| Power et al. (2020) [22] Australia | Third-year nursing students. | University. Elective clinical placement. | Not specified. Face-to-face. | Written and facilitated. |
| Ramsden (1992) [70] Aotearoa New Zealand | Undergraduate nursing and midwifery students. | University. Proposed curriculum framework. | Not specified, but curricula to be scaffolded and embedded throughout the programmes. Not specified. | Conceptualisation of framework. |
| Richardson et al. (2017) [71] Canada | Child and youth mental health workers. | CPE. Short course. | 5-day training programme. Face-to-face. | Co-designed and co-delivered. |
| Royal Australian College of General Practitioners (2011) [36] Australia | Medical practitioners. | CPE. Framework for delivery; to be developed and delivered on a case-by-case basis by accredited trainers. | Minimum 6 h, up to 10 h of structured learning. Must also include preparatory activities. Mandatory 6 h face-to-face; can also include online components. | Planning, delivery, and evaluation of the programme. |
| Ryder et al. (2013) [28] Australia | Second- and third-year medical students. | University. Structured clinical simulations. | 3 h session. Face-to-face. | Co-designed and co-delivered. |
| Sjoberg and McDermott (2016) [73] Australia | Health professions students (undergraduate and postgraduate). | University. Assessment included within a semester-long unit of study. | Not specified. Face-to-face. | Development. |
| Thackrah and Thomson (2013) [23] Australia | First-year midwifery students. | University. Semester-long unit of study. | 12-week semester. 2 contact hours per week. Face-to-face. | Co-designed and co-delivered. |
| The Royal New Zealand College of General Practitioners (n.d.) [91] Aotearoa New Zealand | Practicing general practitioners. | CPE. Online training module. | Self-paced training module. Online. | Development and presentation. |
| Thorpe and Burgess (2012) [66] Australia | Undergraduate preservice teachers. | University. Semester-long unit of study. | 12-week semester. Weekly contact time not specified. Face-to-face. | Co-designed and co-delivered. |
| West et al. (2021) [81] Australia | Final year undergraduate podiatry students. | University. Immersive clinical placement. | Minimum of four 1-day placements over the final year of study. Face-to-face | Clinic is staffed by Aboriginal health professionals. |
| Self-Identity | Held Beliefs | Relationality | Context |
|---|---|---|---|
| Identity Culture and ethnicity Worldview Values | Assumptions Biases and stereotypes Internalised racism Power and privilege | Impact of self-identity and held beliefs on relationships with others | Impact of context on self-identity, held beliefs, and relationality |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dawson, J.; Laccos-Barrett, K.; Hammond, C.; Rumbold, A. Reflexive Practice as an Approach to Improve Healthcare Delivery for Indigenous Peoples: A Systematic Critical Synthesis and Exploration of the Cultural Safety Education Literature. Int. J. Environ. Res. Public Health 2022, 19, 6691. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116691
Dawson J, Laccos-Barrett K, Hammond C, Rumbold A. Reflexive Practice as an Approach to Improve Healthcare Delivery for Indigenous Peoples: A Systematic Critical Synthesis and Exploration of the Cultural Safety Education Literature. International Journal of Environmental Research and Public Health. 2022; 19(11):6691. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116691
Chicago/Turabian StyleDawson, Jessica, Keera Laccos-Barrett, Courtney Hammond, and Alice Rumbold. 2022. "Reflexive Practice as an Approach to Improve Healthcare Delivery for Indigenous Peoples: A Systematic Critical Synthesis and Exploration of the Cultural Safety Education Literature" International Journal of Environmental Research and Public Health 19, no. 11: 6691. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116691