
The Synergetic Impact of Physical Activity and Fruit and Vegetable Consumption on the Risk of Depression in Taiwanese Adults

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
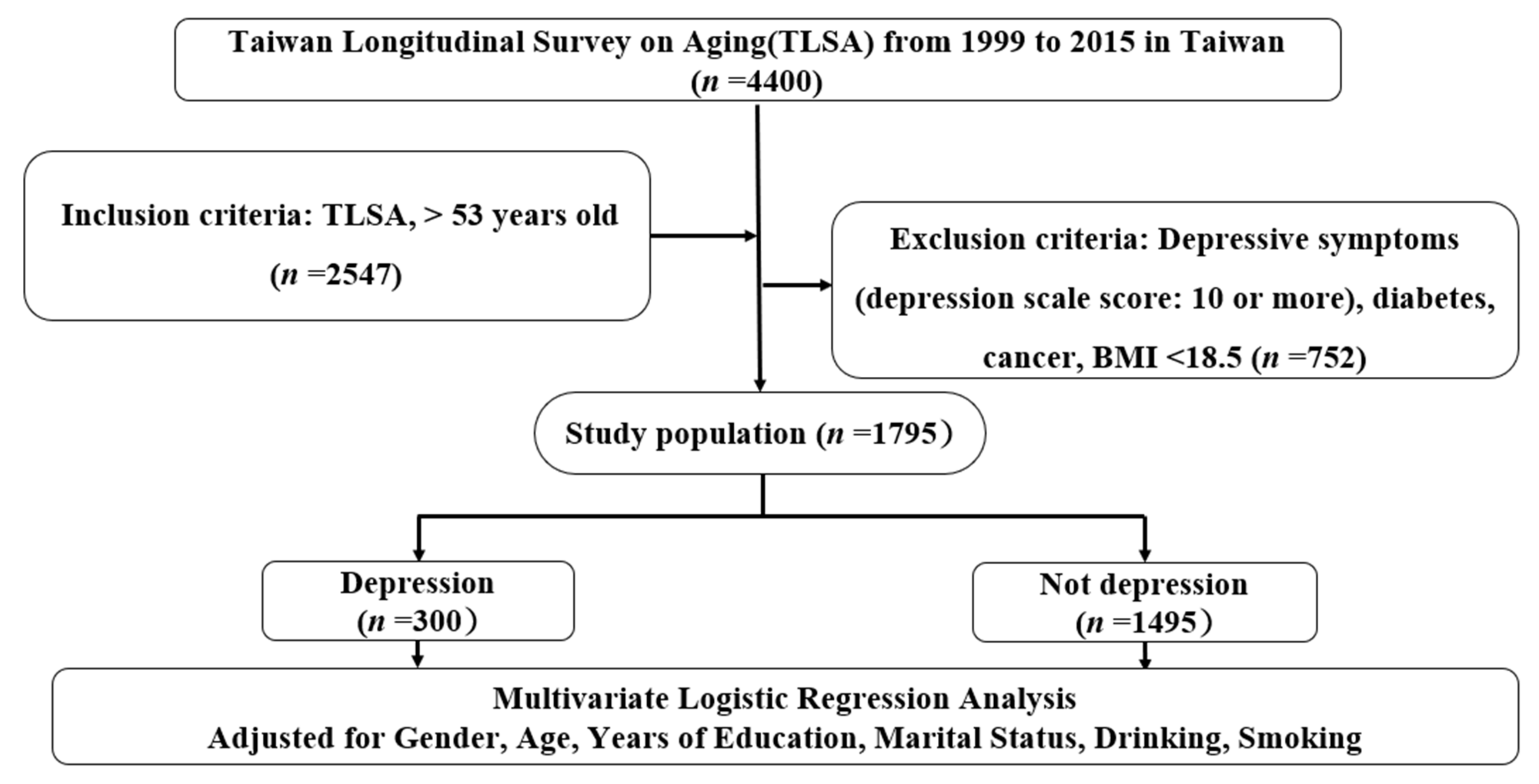
2.1. Data Sources
2.2. Research Steps and Content
2.3. Data Processing and Statistical Analysis
3. Results
4. Discussion
4.1. The Association between Physical Activity and Depression Risk
4.2. Association of Fruit and Vegetable Intake with Depression Risk
4.3. Association between Nutrition, Physical Activity, and Depression Risk
4.4. Other Findings
4.5. Research Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Development Council. Timeline of Aging in Taiwan. 2022. Available online: https://www.ndc.gov.tw/Content_List.aspx?n=695E69E28C6AC7F3 (accessed on 15 January 2022).
- World Health Organization. Depression. 2022. Available online: https://www.who.int/health-topics/depression#tab=tab_1 (accessed on 15 January 2022).
- Kumar, S.; Joseph, S.; Abraham, A. Prevalence of depression amongst the Elderly population in old age homes of Mangalore city. J. Fam. Med. Prim. Care 2021, 10, 1868–1872. [Google Scholar] [CrossRef]
- Pei-Xin, G. The Prevalence of Depression among the Elderly in Taiwan. 2022. Available online: http://www.chimei.org.tw/ePhotoAlbum/files/FD3ECB69597B533AD79945D191126234.pdf (accessed on 15 January 2022).
- Remes, O.; Mendes, J.F.; Templeton, P. Biological, Psychological, and Social Determinants of Depression: A Review of Recent Literature. Brain Sci. 2021, 11, 1633. [Google Scholar] [CrossRef] [PubMed]
- Kandola, A.; Lewis, G.; Osborn, D.; Stubbs, B.; Hayes, J.F. Depressive symptoms and objectively measured physical activity and sedentary behaviour throughout adolescence: A prospective cohort study. Lancet Psychiatry 2020, 7, 262–271. [Google Scholar] [CrossRef] [Green Version]
- Fleg, J.L. Aerobic Exercise in the Elderly: A Key to Successful Aging. Discov. Med. 2012, 13, 223–228. [Google Scholar] [PubMed]
- Qikun, W. The effect of regular exercise on anxiety and depression. J. Cult. Sports 2006, 4, 21–32. [Google Scholar]
- Dharmayani, P.; Juergens, M.; Allman-Farinelli, M.; Mihrshahi, S. Association between Fruit and Vegetable Consumption and Depression Symptoms in Young People and Adults Aged 15–45: A Systematic Review of Cohort Studies. Int. J. Environ. Res. Public Health 2021, 18, 780. [Google Scholar] [CrossRef] [PubMed]
- Saghafian, F.; Malmir, H.; Saneei, P.; Keshteli, A.H.; Hosseinzadeh-Attar, M.J.; Afshar, H.; Siassi, F.; Esmaillzadeh, A.; Adibi, P. Consumption of fruit and vegetables in relation with psychological disorders in Iranian adults. Eur. J. Nutr. 2018, 57, 2295–2306. [Google Scholar] [CrossRef]
- Ju, S.Y.; Park, Y.K. Low fruit and vegetable intake is associated with depression among Korean adults in data from the 2014 Korea National Health and Nutrition Examination Survey. J. Health Popul. Nutr. 2019, 38, 39. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. Dietary consumption and happiness and depression among university students: A cross-national survey. J. Psychol. Afr. 2017, 27, 372–377. [Google Scholar] [CrossRef]
- Brenner, M.H.; Bhugra, D. Acceleration of Anxiety, Depression, and Suicide: Secondary Effects of Economic Disruption Related to COVID-19. Front. Psychiatry 2020, 11, 592467. [Google Scholar] [CrossRef]
- Harmer, B.; Lee, S.; Duong, T.V.H.; Saadabadi, A. Suicidal Ideation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Sapranaviciute-Zabazlajeva, L.; Sileikiene, L.; Luksiene, D.; Tamosiunas, A.; Radisauskas, R.; Milvidaite, I.; Bobak, M. Lifestyle factors and psychological well-being: 10-year follow-up study in Lithuanian urban population. BMC Public Health 2022, 22, 1011. [Google Scholar] [CrossRef] [PubMed]
- National Health Administration of the Ministry of Health and Welfare. Long-Term Follow-Up Survey on Physical and Mental and Social Living Conditions of Middle-Aged and Elderly People in Taiwan in 1988. 2014. Available online: http://www.hpa.gov.tw/BHPNet/Web/HealthTopic/TopicArticle.aspx?No=201106080002&parentid=200712270002 (accessed on 26 May 2014).
- National Health Administration of the Ministry of Health and Welfare. Introduction to a Series of Long-Term Follow-Up Surveys on Physical and Mental and Social Living Conditions of Middle-Aged and Elderly People. 2014. Available online: http://www.hpa.gov.tw/Bhpnet/web/HealthTopic/Topic.aspx?id=200712270002 (accessed on 26 May 2014).
- Ruifeng, Y.; Zhonghong, C. A study on the correlation between food intake frequency and depression risk among elderly people in Taiwan. Taiwan Wei Zhi 2011, 30, 123–134. [Google Scholar]
- Yiru, C.; Zhonghong, C.; Junyi, W. Combined effect of exercise and fruit and vegetable intake on prevention of new-onset diabetes in middle-aged and elderly people in Taiwan. Taiwan J. Public Health 2013, 32, 551–561. [Google Scholar]
- Aihara, Y.; Minai, J.; Aoyama, A.; Shimanouchi, S. Depressive symptoms and past lifestyle among Japanese elderly people. Community Ment. Health J. 2011, 47, 186–193. [Google Scholar] [CrossRef]
- Zhicheng, X.; Yunzuo, L.; Yingchun, X.; Yating, X.; Qinghui, L. Regional differences in population distribution and perceived health of the elderly in Taiwan. Taiwan J. Fam. Med. 2007, 17, 59–72. [Google Scholar]
- APA (American Psychological Association). Effect of Exercise on Depression. 2014. Available online: http://www.apa.org/reserach/action/fit.aspx (accessed on 15 January 2022).
- U.S. Department of Health and Human Services. Physical activity and health: A report of the surgeon general Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion. Int. Med. Publ. 1996, 22–23, 149–150. [Google Scholar]
- Yuren, P.; Shuling, Z. The effects of aerobic and anaerobic exercise on anxiety and depression. Coll. Phys. Educ. 1997, 34, s46–s50. [Google Scholar]
- Jiabi, W.; Zhaoda, L. Exercise therapy for depression. Coll. Phys. Educ. 2007, 90, 170–176. [Google Scholar]
- Chunhua, S.; Shuying, H.; Mingren, Y.; Lizhen, Z.; Ziqiang, Z.; Junren, H. The epidemiology of depressive symptoms in the elderly in the community and the effect of participation in activities. Empir. Nurs. 2005, 1, 29–34. [Google Scholar]
- Sherril, D.L.; Kotchou, K.; Quan, S.F. Association of physical activity and human sleep disorders. Arch. Intern. Med. 2005, 158, 1894–1898. [Google Scholar] [CrossRef] [Green Version]
- Sports Department of the Ministry of Education. Talking about Sports and Life from the Perspective of the National Health Bureau. 2014. Available online: http://www1.sa.gov.tw/resource/annualreport/Quarterly169/ppag15.htm (accessed on 12 April 2022).
- Tsai, A.C.; Chang, T.L.; Chi, S.H. Frequent consumption of vegetables predicts lower risk of depression in older Taiwanese—Results of a prospective population-based study. Public Health Nutr. 2012, 15, 1087–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akbaraly, T.N.; Brunner, E.J.; Ferrie, J.E.; Marmot, M.G.; Kivimaki, M.; Singh-Manoux, A. Dietary pattern and depressive symptoms in middle age. Br. J. Psychiatry 2009, 195, 408–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanri, A.; Kimura, Y.; Matsushita, Y.; Ohta, M.; Sato, M.; Mishima, N.; Sasaki, S.; Mizoue, T. Dietary patterns and depressive symptoms among Japanese men and women. Eur. J. Clin. Nutr. 2010, 64, 832–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Villegas, A.; Delgado-Rodriguez, M.; Alonso, A.; Schlatter, J.; Lahortiga, F.; Majem, L.S.; Martínez-González, M.A. Association of the Mediterranean dietary pattern with the incidence of depression: The Seguimiento Universidad de Navarra/University of Navarra follow-up (SUN) cohort. Arch. Gen. Psychiatry 2009, 66, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.; Lynn, H.; Lau, W.Y.; Leung, J.; Lau, E.; Wong, S.Y.; Kwok, T. Nutrient intake and psychological health in an elderly Chinese population. Int. J. Geriatr. Psychiatry 2006, 21, 1036–1043. [Google Scholar] [CrossRef]
- Oishi, J.; Doi, H.; Kawakami, N. Nutrition and depressive symptoms in community-dwelling elderly persons in Japan. Acta. Med. Okayama. 2009, 63, 9–17. [Google Scholar] [CrossRef]
- Karakula, H.; Opolska, A.; Kowal, A.; Domanski, M.; Poltka, A.; Perzynski, J. Does diet affect our mood? The significance of folic acid and homocysteine. Pol. Merkur Lekarski. 2009, 26, 136–141. [Google Scholar]
- Benton, D.; Donohoe, R.T. The effects of nutrients on mood. Public Health Nutr. 1999, 2, 403–409. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.L. The methylation, neurotransmitter, and antioxidant connections between folate and depression. Altern. Med. Rev. 2008, 13, 216–226. [Google Scholar]
- Alghadir, A.H.; Gabr, S.A.; Iqbal, Z.A. Effect of Gender, Physical Activity and Stress-Related Hormones on Adolescent’s Academic Achievements. Int. J. Environ. Res. Public Health 2020, 17, 4143. [Google Scholar] [CrossRef]
- Ivarsson, T.; Spetz, A.C.; Hammar, M. Physical exercise and vasomotor symptoms in postmenopausal women. Maturitas 1998, 29, 139–146. [Google Scholar] [CrossRef]
- Jóźków, P.; Mędraś, M. Psychological stress and the function of male gonads. Endokrynol. Pol. 2012, 63, 44–49. [Google Scholar] [PubMed]
- Wright, A.; Cattan, M. Physical activity and the management of depression. Work. Older People 2009, 13, 15–18. [Google Scholar] [CrossRef]
- Hedlund, E.R.; Ljungberg, H.; Söderström, L.; Lundell, B.; Sjöberg, G. Physical exercise may improve sleep quality in children and adolescents with Fontan circulation. Cardiol. Young 2019, 29, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Vigil, P.; Orellana, R.F.; Cortés, M.; Molina, C.T.; Switzer, B.E.; Klaus, H. Endocrine Modulation of the Adolescent Brain: A Review. J. Pediatr. Adolesc. Gynecol. 2011, 24, 330–337. [Google Scholar] [CrossRef]
- Farooqui, A.A. Effect of Exercise on Neurodegeneration in Neurological Disorders. In Inflammation and Oxidative Stress in Neurological Disorders: Effect of Lifestyle, Genes, and Age; Farooqui, A.A., Ed.; Springer: Cham, Switzerland, 2014; pp. 143–173. [Google Scholar]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Jianian, L. The relationship between socioeconomic status, general health status, health behaviors and depression among adults in the community. Taiwan Wei Zhi 2009, 28, 300–311. [Google Scholar]
- Shuyu, L.; Zongyi, L. A study on the prevalence of depressive symptoms and related factors in the elderly in southern communities. Taiwan J. Public Health 2000, 19, 50–60. [Google Scholar]
- Wang, P. The Influence of Work and Depression in Middle-Aged and Elderly People in Taiwan. Master′s Thesis, Institute of Health Management, Asia University, Taichung City, Taiwan, 2010. Unpublished. [Google Scholar]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in older adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef]


{kind=link}
| Item | Overall, n (%) | Depression, n (%) | Not Depression, n (%) | p-Value |
|---|---|---|---|---|
| Sex | 0.789 | |||
| Male | 933 (52.0) | 165/933 (17.6) | 768/933 (82.4) | |
| Female | 862 (48.0) | 135/862 (15.6) | 727/862 (84.4) | |
| Age (mean ± SD, year) | 0.876 | |||
| 53–64 | 996 (55.5) | 145/996 (14.5) | 851/996 (85.5) | |
| 65–74 | 549 (30.6) | 107/549 (19.5) | 442/549 (80.5) | |
| ≥75 | 118 (6.6) | 50/118 (42.4) | 68/118 (57.6) | |
| Years of education | 0.687 | |||
| ≤6 | 1252 (69.7) | 205/1252 (16.3) | 1047/1252 (83.7) | |
| 7–12 | 299 (16.7) | 65/299 (21.7) | 234/299 (78.3) | |
| ≥13 | 112 (6.2) | 39/112 (34.8) | 73/112 (65.2) | |
| Marital status | * 0.039 | |||
| Married | 1299 (72.4) | 215/1299 (16.5) | 1084/1299(83.5) | |
| Unmarried | 364 (20.3) | 85/364 (23.3) | 279/364(76.6) | |
| Smoking status | 0.078 | |||
| Yes | 355 (19.8) | 63/355 (17.7) | 292/355 (82.3) | |
| No | 1308 (72.9) | 229/1308 (17.5) | 1079/1308 (82.5) | |
| Alcohol consumption | ** 0.001 | |||
| Yes | 463 (25.8) | 67/463 (14.5) | 396/463 (85.5) | |
| No | 1200 (66.9) | 235/1200 (19.5) | 965/1200 (80.5) | |
| Amount of physical activity | ** <0.001 | |||
| Low | 1029 (573) | 135/1029 (13.2) | 894/1029 (86.8) | |
| Moderate | 445 (24.8) | 80/445 (17.9) | 355/445 (82.1) | |
| High | 186 (10.4) | 85/186 (45.6) | 101/186 (54.4) | |
| Fruit and vegetable intake frequency (times/week) a | * 0.025 | |||
| <7 | 166 (9.2) | 35/166 (21.1) | 146/185 (78.9) | |
| 7–9 | 176 (9.8) | 32/176 (18.1) | 144/176 (81.9) | |
| ≥10 | 1321 (73.6) | 214/1321 (16.1) | 1107/1321 (83.8) | |
| Physical activity and fruit and vegetable intake | * 0.043 | |||
| Both low | 77 (4.3) | 11/77 (14.2) | 66/77 (85.7) | |
| Both high | 246 (13.7) | 72/246 (29.2) | 174/246 (70.7) | |
| High Transport, Low fruit-vegetable intake | 40 (2.2) | 8/40 (20.0) | 32/40 (80.0) | |
| Low Shipping, High fruit-vegetable intake | 1075 (59.9) | 152/1075 (14.2) | 923/1075 (85.8) | |
| Other | 225 (12.5) | 56/225 (24.8) | 169/225 (75.2) | |
| BMI (kg/m2) | 23.96 + 3.03 | 23.95 + 3.02 | 23.97 + 3.03 | 0.882 |
| CES-D overall Score b | 5.26 + 2.42 | 13.30 + 3.49 | 5.37 + 2.57 | ** <0.001 |
| Depression Risk from 1999 to 2015 | ||||
|---|---|---|---|---|
| Variable a | Total (%) | Depression Risk (%) | OR (95%CI) | p-Value |
| Amount of physical activity | ||||
| complicate | 37.5 | 19.2 | 1 | |
| Moderate | 27.7 | 15.7 | 0.65 (0.23–0.78) | 0.257 |
| high | 34.8 | 11.6 | 0.60 (0.42–0.78) | ** 0.001 |
| Fruit and vegetable intake (times/week) | ||||
| <7 | 9.2 | 20.0 | 1 | |
| 7–9 | 10.8 | 15.3 | 0.75 (0.54–1.06) | 0.242 |
| ≥10 | 80.0 | 14.0 | 0.60 (0.40–0.78) | * 0.025 |
| Depression Risk from 1999 to 2015 | ||||
|---|---|---|---|---|
| Variable a | Total (%) | Depression Risk (%) | OR (95%CI) | p-Value |
| Physical Activity and Fruit and Vegetable Intake b | ||||
| Both are low | 1.5 | 35.7 | 1 | |
| Both high | 30.8 | 10.5 | 0.20 (0.10–0.45) | ** 0.001 |
| High physical activity, Low fruit-vegetable Intake | 3.2 | 12.5 | 0.30 (0.15–0.63) | ** 0.005 |
| Low physical activity, High fruit-vegetable Intake | 40.4 | 17.5 | 0.35 (0.10–1.05) | * 0.038 |
| Other | 15.0 | 18.0 | 0.33 (0.15–0.78) | * 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fann, L.-Y.; Huang, S.-H.; Huang, Y.-C.; Chen, C.-F.; Sun, C.-A.; Wang, B.-L.; Chien, W.-C.; Lu, C.-H. The Synergetic Impact of Physical Activity and Fruit and Vegetable Consumption on the Risk of Depression in Taiwanese Adults. Int. J. Environ. Res. Public Health 2022, 19, 7300. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127300
Fann L-Y, Huang S-H, Huang Y-C, Chen C-F, Sun C-A, Wang B-L, Chien W-C, Lu C-H. The Synergetic Impact of Physical Activity and Fruit and Vegetable Consumption on the Risk of Depression in Taiwanese Adults. International Journal of Environmental Research and Public Health. 2022; 19(12):7300. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127300
Chicago/Turabian StyleFann, Li-Yun, Shi-Hao Huang, Yao-Ching Huang, Chin-Fu Chen, Chien-An Sun, Bing-Long Wang, Wu-Chien Chien, and Chieh-Hua Lu. 2022. "The Synergetic Impact of Physical Activity and Fruit and Vegetable Consumption on the Risk of Depression in Taiwanese Adults" International Journal of Environmental Research and Public Health 19, no. 12: 7300. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127300