
The Effect of Outdoor Environmental Exposure on Readmission Rates for Children and Adolescents with Asthma—A Systematic Review

Abstract
:1. Introduction
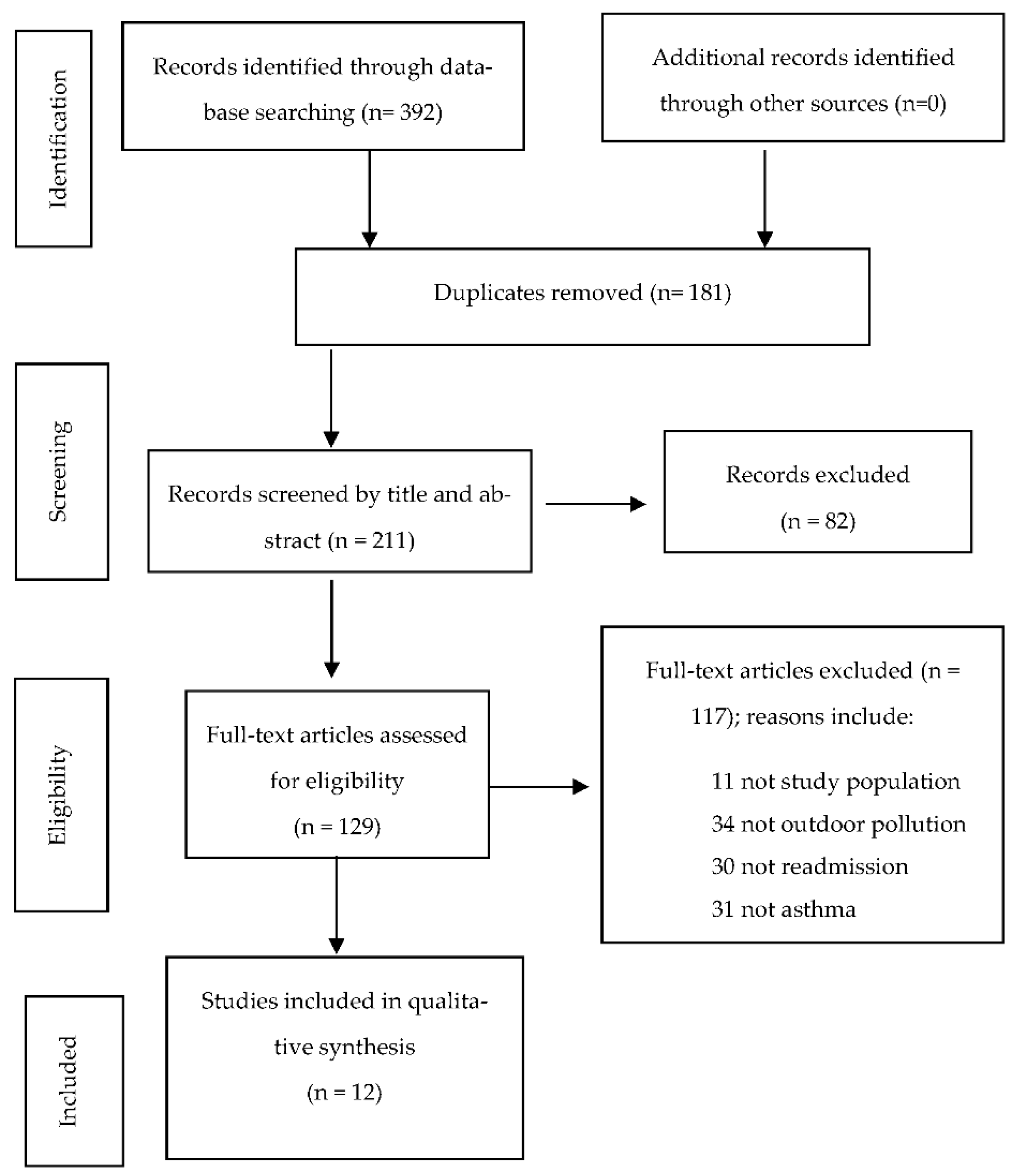
2. Materials and Methods
2.1. Data Extraction
2.2. Assessment of Quality and Risk of Bias
2.3. Assessment for Meta-Analysis
3. Results
3.1. Odds Ratio
3.2. General Additive Models (GAMs)
3.3. Hazards Ratio
3.4. Descriptive Analysis
3.5. Quality Assessment and Risk of Bias
4. Discussion
4.1. Main Findings
4.1.1. Readmission within 28 Days
4.1.2. Readmission within 6 Months
4.1.3. Readmission Greater Than 6 Months
4.2. Strengths
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Author (Year) | Score | Possible Limitations and Biases | Strengths |
|---|---|---|---|
| Rushworth et al. 1995 [9] | 11.5/17 |
|
|
| Chang et al. 2008 [20] | 13.25/17 |
|
|
| Delfino et al. 2009 [21] | 13.5/17 |
|
|
| Vicendese et al. 2013 [18] | 13.25/17 |
|
|
| Vicendese et al. 2014 [15] | 13.25/17 |
|
|
| Newman et al. 2014 [11] | 13/17 |
|
|
| Beck et al. 2016 [22] | 12.75/17 |
|
|
| Brittan et al. 2016 [10] | 12.25/17 |
|
|
| Beck et al. 2017 [17] | 11.5/17 |
|
|
| Lam et al. 2019 [19] | 11/17 |
|
|
| Baek et al. 2020 [12] | 13/17 |
|
|
| Baek et al. 2020 [13] | 11.5/17 |
|
|
| Total Average | 12.54/17 |
References
- Henderson, A.J. Aetiology of asthma. Paediatr. Child Health 2013, 23, 287–290. [Google Scholar] [CrossRef]
- World Health Organization. Asthma. Available online: http://www.who.int/news-room/fact-sheets/detail/asthma (accessed on 16 June 2021).
- 2022 GINA Report, Global Strategy for Asthma Management and Prevention. Available online: https://ginasthma.org/gina-reports/ (accessed on 16 June 2021).
- Forno, E.; Saglani, S. Severe Asthma in Children and Adolescents Mechanisms and Management, 1st ed.; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Garcia, C.A.; Stolbrink, M.; Zaidi, S.; Cooper, P.J.; Blakey, J.D. Predictors of repeated acute hospital attendance for asthma in children: A systematic review and meta-analysis. Pediatr. Pulmonol. 2018, 53, 1179–1192. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.S.; Poletti, G.; Kebadze, T.; Morris, J.; Woodcock, A.; Johnston, S.L.; Custovic, A. Study of modifiable risk factors for asthma exacerbations: Virus infection and allergen exposure increase the risk of asthma hospital admissions in children. Thorax 2006, 61, 376–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saglani, S.; Bush, A. Asthma attacks in children: Does blocking IgE reduce rhinovirus infections? Am. J. Respir. Crit. Care Med. 2017, 196, 941–942. [Google Scholar] [CrossRef]
- Ellwood, P.; Asher, M.I.; Billo, N.E.; Bissell, K.; Chiang, C.Y.; Ellwood, E.M.; El-Sony, A.; García-Marcos, L.; Mallol, J.; Marks, G.B.; et al. The global asthma network rationale and methods for phase I global surveillance: Prevalence, severity, management and risk factors. Eur. Clin. Respir. J. 2017, 49, 1601605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rushworth, R.L.; Rob, M.I. Readmissions to hospital: The contribution of morbidity data to the evaluation of asthma management. Aust. J. Public Health 1995, 19, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Brittan, M.; Richardson, T.; Kenyon, C.; Sills, M.R.; Fieldston, E.; Hall, M.; Fox, D.; Shah, S.; Berry, J. Association between postdischarge oral corticosteroid prescription fills and readmission in children with asthma. J. Pediatr. 2017, 180, 163–169.e1. [Google Scholar] [CrossRef] [PubMed]
- Newman, N.C.; Ryan, P.H.; Huang, B.; Beck, A.F.; Sauers, H.S.; Kahn, R.S. Traffic-related air pollution and asthma hospital readmission in children: A longitudinal cohort study. J. Pediatr. 2014, 164, 1396–1402.e1. [Google Scholar] [CrossRef] [Green Version]
- Baek, J.; Kash, B.A.; Xu, X.; Benden, M.; Roberts, J.; Carrillo, G. Effect of ambient air pollution on hospital readmissions among the pediatric asthma patient population in South Texas: A case-crossover study. Int. J. Environ. Res. Public Health 2020, 17, 4846. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.; Kash, B.A.; Xu, X.; Benden, M.; Roberts, J.; Carrillo, G. Pediatric asthma hospitalization: Individual and environmental characteristics of high utilizers in South Texas. J. Asthma 2020, 59, 94–104. [Google Scholar] [CrossRef] [PubMed]
- McCaul, K.A.; Wakefield, M.A.; Roder, D.M.; Ruffin, R.E.; Heard, A.R.; Alpers, J.H.; Staugas, R.E. Trends in hospital readmission for asthma: Has the Australian National Asthma Campaign had an effect? Med. J. Aust. 2000, 172, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Vicendese, D.; Abramson, M.J.; Dharmage, S.C.; Tang, M.L.; Allen, K.J.; Erbas, B. Trends in asthma readmissions among children and adolescents over time by age, gender and season. J. Asthma 2014, 51, 1055–1060. [Google Scholar] [CrossRef]
- The Endnote Team. EndNote; Clarivate: Philadelphia, PA, USA, 2016. [Google Scholar]
- Beck, A.F.; Huang, B.; Wheeler, K.; Lawson, N.R.; Kahn, K.S.; Riley, C.L. The child opportunity index and disparities in pediatric asthma hospitalizations across one Ohio metropolitan area, 2011–2013. J. Pediatr. 2017, 190, 200–206.e1. [Google Scholar] [CrossRef] [PubMed]
- Vicendese, D.; Olenko, A.; Dharmage, S.C.; Tang, M.L.; Abramson, M.J.; Erbas, B. Modelling and predicting low count child asthma hospital readmissions using General Additive Models. Open J. Epidemiol. 2013, 3, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Lam, H.C.Y.; Hajat, S.; Chan, E.Y.Y.; Goggins, W.B. Different sensitivities to ambient temperature between first- and re-admission childhood asthma cases in Hong Kong—A time series study. Environ. Res. 2019, 170, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Delfino, R.J.; Gillen, D.; Tjoa, T.; Nickerson, B.; Cooper, D. Repeated respiratory hospital encounters among children with asthma and residential proximity to traffic. Occup. Environ. Med. 2008, 66, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Delfino, R.J.; Chang, J.; Wu, J.; Ren, C.; Tjoa, T.; Nickerson, B.; Cooper, D.; Gillen, D.L. Repeated hospital encounters for asthma in children and exposure to traffic-related air pollution near the home. Ann. Allergy Asthma Immunol. 2009, 102, 138–144. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.F.; Huang, B.; Auger, K.A.; Ryan, P.H.; Chen, C.; Kahn, R.S. Explaining racial disparities in child asthma readmission using a causal inference approach. JAMA Pediatr. 2016, 170, 695–703. [Google Scholar] [CrossRef]
- Zaza, S.; Agüero, L.K.W.; Briss, P.A.; Truman, B.I.; Hopkins, D.P.; Hennessy, M.H.; Sosin, D.M.; Anderson, L.; Carande-Kulis, V.G.; Teutsch, S.M.; et al. Data collection instrument and procedure for systematic reviews in the Guide to Community Preventive Services. Task Force on Community Preventive Services. Am. J. Prev. Med. 2000, 18, 44–74. [Google Scholar] [CrossRef]
- Erbas, B.; Jazayeri, M.; Lambert, K.A.; Katelaris, C.H.; Prendergast, L.A.; Tham, R.; Parrodi, M.J.; Davies, J.; Newbigin, E.; Abramson, M.J.; et al. Outdoor pollen is a trigger of child and adolescent asthma emergency department presentations: A systematic review and meta-analysis. Allergy 2018, 73, 1632–1641. [Google Scholar] [CrossRef]
- Gantt, B.; McDonald, K.; Henderson, B.; Mannshardt, E. Incorporation of remote PM(2.5) concentrations into the downscaler model for spatially fused air quality surfaces. Atmosphere 2020, 11, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acevedo-Garcia, D.; McArdle, N.; Hardy, E.F.; Crisan, U.I.; Romano, B.; Norris, D.; Baek, M.; Reece, J. The child opportunity index: Improving collaboration between community development and public health. Health Aff. 2014, 33, 1948–1957. [Google Scholar] [CrossRef] [PubMed]
- English, P.; Neutra, R.; Scalf, R.; Sullivan, M.; Waller, L.; Zhu, L. Examining associations between childhood asthma and traffic flow using a geographic information system. Environ. Health Perspect. 1999, 107, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Caline 4-a Dispersion Model for Predicting Air Pollutant Concentrations Near Roadways. Available online: https://trid.trb.org/view/285625#:~:text=A%20description%20of%20the%20California,nitrogen%20dioxide%20and%20suspended%20particles (accessed on 16 June 2021).
- National Asthma Council Australia. Australian Asthma Handbook, Version 2.2; National Asthma Council Australia Ltd.: Melbourne, Australia, 2022. [Google Scholar]
- Melsom, R. Rising Admission of Children with Asthma. Tidsskr. Nor. Laegeforen. 1990, 110, 3219–3221. [Google Scholar] [PubMed]

| Search Terms | |
|---|---|
| Environment* | 1 |
| Aeroallergen | 2 |
| “traffic related air pollution” | 3 |
| “air pollut*” | 4 |
| “Nitrous oxide” | 5 |
| “Nitrogen dioxide” | 6 |
| “Carbon Monoxide” | 7 |
| “Volatile organic compounds” | 8 |
| “Particulate Matter*” | 9 |
| Ozone | 10 |
| Pollen | 11 |
| Grass | 12 |
| Tree* | 13 |
| Weed* | 14 |
| “PM2.5” | 15 |
| “PM10” 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10 OR 11 OR 12 OR 13 OR 14 OR 15 OR 16 | 16 17 |
| Child* | 18 |
| Infant | 19 |
| Youth | 20 |
| Adoles* | 21 |
| P?ediatric | 22 |
| “young people” | 23 |
| Teen* | 24 |
| 18 OR 19 OR 20 OR 21 OR 22 OR 23 OR 24 | 25 |
| Readmi* | 26 |
| “repeat admi*” | 27 |
| Re-hospitali?ation | 28 |
| “repeat hospital encounters” | 29 |
| 26 OR 27 OR 28 OR 29 | 30 |
| Asthma* | 31 |
| 17 AND 25 AND 30 AND 31 | 32 |
| Author(s) (Year) | Study Population /Setting/Duration/Age of the Participants/Sample Size/Design of the Study | Exposure Variable/ Exposure Measurement | Readmission timeframe/ Outcome Definition/ Statistical Analysis | Confounders/Covariates/ Interactions | Results | Findings |
|---|---|---|---|---|---|---|
| Rushworth et al. (1995) [9] | Patients (1–14 years) admitted for asthma (ICD9-CM code 493) to all New South Wales (NSW) hospitals including NSW residents who attended hospital interstate for the financial year 1989–1990 and first 2 weeks for 1990/1991. Readmitted included n = 782. Descriptive study. | Months of the year were used to assess the seasonal effect. Season is a crude marker of environmental effects of pollen and viruses. Winter months (July to August are used as the reference point for the results analysis). | Readmission within 6 months of index admission. Only the first readmission from the index admission was counted. Descriptive analysis. |
| The effect of month of readmission was statistically significant during October and November: OR 1.70 (95% CI 1.10–2.64) and 1.78 (95% CI 1.21–2.62), respectively. The OR in spring–summer (September–December) was 1.53 (95% CI 1.30–1.80) when compared to winter. |
|
| Newman et al. (2014) [11] | Patients (1–16 years) admitted for asthma or bronchodilator-responsive wheezing (ICD-9 (493.XX or 786.07)) to the Cincinnati Children’s Hospital Medical Centre (CCHMC), an urban tertiary care hospital, between August 2010 and October 2011; also included nearby satellite inpatient facility from November 2010. The readmission sample size, n = 774 Descriptive study. | Traffic related air pollution (TRAP) measured as elemental carbon attributed to traffic (ECAT). They used modelling of a validated Land use regression model (LUR) (to reported residence) as a substitute to measure TRAP. ECAT was measured at the median level of 0.37 microgram/m3 and either classified as above or below this result. | Readmission within 12 months of index admission. Logistic regression analysis and cox proportional hazards models. |
| Patients with high TRAP exposure were readmitted at a higher rate: OR 1.5 (95%CI 1.0–2.1), p = 0.05 aOR 1.4 (95%CI 0.9–2.2) TRAP and race interaction: OR 1.5 (95% CI 0.9–2.5), p = 0.07. When broken into individual race: white-OR 3.0 (95%CI 1.1–8.1) p = 0.03 African American-OR 1.1 (95% CI 0.6–1.8) p = 0.7. |
|
| Beck et al. (2017) [17] | Patients (1–16 years) living within Hamilton County, Ohio, with a hospitalisation or visited Emergency Department for asthma or wheezing (ICD-9, (code 493.xx)) at the Cincinnati Children’s Hospital Medical Center (CCHMC) between January 2011 and December 2013. Sample size n = 1845 Descriptive study. | The subcategory variables to the health and environmental opportunity index (HEOI) used as exposure variables are proximity from their home to parks and green space, volume of nearby toxic release, and proximity to toxic waste release sites. For patient level analyses, each opportunity index was measured in categories, i.e., very low, low, medium, high, or very high, to represent quintiles of the census tract z-scores. | Hospital readmission within 12 months of the index admission for the study period and the patients’ address was geocoded and mapped to the in-county census tract. |
| At a patient level analysis for HEOI, the very low–low category: OR 1.16 95%CI (0.90–1.50), aOR 0.98 (0.75–1.29); At the moderate level: OR 1.03 (0.72–1.46) aOR 1.1 (0.71–1.44), p = 0.20 |
|
| Brittan et al. (2017) [10] | Patients (2–18 years) hospitalised for asthma (ICD-9 (493.xx)) between 1 July 2009, and 30 June 2011, and continuously enrolled in Medicaid from 1 of 12 states for 6 months before and 3 months after the hospitalization with health claims contained in the Truven Health MarketScan Database (Ann Arbor, Michigan). The readmitted sample size was 259. Descriptive study. | The effect of seasonal trends. This study defined each season as the inclusive dates below: summer (21 June to 20 September), autumn (fall) (21 September to 20 December), winter (21 December to 20 March), and spring (21 March to 20 June). | Hospital readmission from 15 to 90 days after discharge from the index admission within the study period. For those children with greater than 1 readmission, 1 hospital admission was randomly chosen. Multivariable logistic regression models. |
| Of the children who were readmitted, 35.5% were aged 2–4, 45.6% 5–11 years old, and 18.5% aged 12–18 years. The median number of days between discharge from index admission and readmission was 50 days with inter quartile range of 32–70. Summer discharge compared to fall (autumn) discharge had a greater likelihood of readmission OR 1.5 95% CI (1.1–2). Greater percentage of children with index admission in summer had readmission (p ≤ 0.001). |
|
| Baek et al. (2020) [13] | Patients (5–18 years) readmitted to Driscoll Children’s Hospital, South Texas, for Asthma (ICD-9 or ICD-10) between 2010 to 2016. Total readmissions were 143. (2–3 admissions n = 121 4 admissions n = 22). Ecological time series study. | The air pollutants (PM2.5 and ozone) were both measured by using the daily average prediction using the Downscaler model of the U.S. EPA at census tract level, then divided into four categories as quartiles. Seasons were defined as warm, from May until October, or cold, from November until April. | Readmission timeframes were split into 1–30 days, 31–90 days, 91–365 days, and 366 days or longer. This study utilised bivariate and multivariate logistic regression (3 models created (unadjusted, adjusted model with only individual-level factors, and adjusted model with individual-level and environmental factors)). |
| Most of the total readmissions were after 90 or more days. None of the environmental factors showed significant differences between the different readmission groups; however, quartile 4 of the ozone group waslarger in high utilisation groups (p = 0.052). In the multivariate analysis, when only individual characteristic was considered, season (warm, p = 0.034) was associated with readmission. When environmental factors were considered, very similar associations were seen. Children living in areas with an ozone level of quartile 2 were more likely to be readmitted than those in the lowest ozone level (p = 0.045). |
|
| Baek et al. (2020) [12] | Patients (5–18 years) readmitted to Driscoll Children’s Hospital, South Texas, for Asthma (ICD-9) between 2010 to 2014. Sample size = 111 Ecological time series study. | The daily mean concentration of PM2.5 was measured in micrograms per cubic metre (μg/m3) and ozone was measured by the mean 8-h average concentration in parts per billion (ppb). Temperature data was collected from the air monitoring stations that were closest to the patients’ home address. Seasons were defined as warm, from May until October, or cold, from November until April. | Readmission within the study period. |
| Only 8.1% of patients were readmitted within 30 days, and almost 37% of all readmissions were over a year (366 days). There were a greater percentage of readmissions in the cold season (52.3%) compared to the warm season (47.7%). Both PM2.5 and ozone had a significant association on readmission only in the warm season. Increased risk of readmission with elevated PM2.5 concentration. |
|
| Author(s) (Year) | Study Population /Setting/Duration/Age of the Participants/Sample Size/Design of the Study | Exposure Variable/ Exposure Measurement | Readmission Timeframe/Outcome Definition/Statistical Analysis | Confounder/Covariates/ Interactions | Results | Findings |
|---|---|---|---|---|---|---|
| GAM studies | ||||||
| Vicendese et al. (2013) [18] | Daily childhood asthma hospital admissions (2–18 years) with a principal diagnosis of asthma, ICD-9 codes (493) up to 1998 and ICD-10 codes (J45 or J46) in Victoria, Australia, between 1997 and 2009 from the VAED Department of Human Services. n = 2401 Study length—13 years Ecological time series study. | Seasonal trends. The hospital records were divided into day of week, month of year, and day of year. The month variable was used to measure the seasonal trend. | Patients were included if their readmission was within 28 days from their index admission. Hospital readmission with a principal diagnosis of asthma, ICD-9 codes (493) up to 1998 and ICD-10 codes (J45 or J46) for remaining data to 2009 for the study period. GAM analysis. |
| The chi square test conducted for readmission rate and season showed a very strong association with a p value of <0.0005. Readmissions peaked in winter (30.5%), then autumn (28.6%), spring (24.6%), and lastly summer (16.2%). Regarding months, the highest readmission rates were seen in June (11.75%), August (10.41%), May (10.16%), and March (10.12%). Both semi parametric and non-parametric models showed that both month and day of the week had significance to the overall daily readmission rates. |
|
| Lam et al. (2019) [19] | Patients (0–5 years) admitted for asthma (ICD-9 code 493.xx) in all public hospitals in Hong Kong between 2002 and 2011 from the Hospital Authority in Hong Kong. Ecological time series study. There were 2185 readmissions. | Seasonal trends. The seasons were defined as hot season (May to October) and cold season (November to April). The other meteorological measures included daily mean temp (°C), daily mean relative humidity (%), daily mean wind speed (km/h), daily total solar radiation (J/m2), and daily rainfall (mm). | Readmission within the study period. A general additive models (GAMs) analysis and Distributed Lagged Nonlinear models (DLNMs) were used for lagged effects and other nonlinear associations. |
| Significant GAMS were observed for temperature and readmission. The hot season analysis showed a relative risk (RR) of 3.4 (1.26–9.18) and a relative risk ratio of (RRR) 4.59 (1.23–17.21). The cold season analysis with 10 °C vs. 15 °C showed RR 1.43 (1.00–2.04) and RRR 1.15 (0.74–1.81), and with 21 vs. 15 °C, RR 0.88 (0.61–1.26) and RRR 0.69 (0.46–1.04). |
|
| Hazard Ratio studies | ||||||
| Chang et al. (2008) [20] | Patients (0–18 years) admitted for asthma as primary or secondary diagnosis to the Children’s Hospital of Orange County (CHOC) and the University Children’s Hospital of the University of California Irvine Medical Center (UCIMC), between 1 January 2000 and 31 December 2003. Repeat admissions were defined as 2 or more encounters. n = 817. Ecological time series study. | TRAP was represented by 3 traffic proxies calculated by measuring traffic density by measuring distance to major roads surrounding the participants’ house. No specific pollutant was measured. | All readmissions for asthma after 8 days from index admission during study period. |
| The time to first readmission included within 1–2 months (26.5%), 3–6 months (26.9%), 7–12 months (21.6%), and after 1 year (22.1%). Traffic-related air pollution metrics on repeat admissions to hospital showed, for 150–300 m compared to greater than 300 m, HR 1.21 95% CI 1.00–1.45, p = 0.05. Additionally, “total arterial road and freeway length within 300 m of residence” and whole study population with greater than or equal to 750 m was associated with an 18% higher rate of repeated hospital admission than children without any major roads nearby, HR 1.18 95% CI 0.99–1.41. p = 0.06. When stratified by insurance, within that index the total length of less than 750 m of major roads calculated a HR 1.43, 95% CI (1.11–1.84), and for the total major road length greater than or equal to 750 m HR 1.48, 95%CI (1.15–1.90). Girls who had greater than 750 m of total arterial road length within 300 m of their house had a 39% higher rate of readmission compared to none, HR 1.39, 95% CI (1.04–1.87). |
|
| Delfino et al. (2009) [21] | Patients (0–18 years) admitted for asthma (ICD-9 493) to the Children’s Hospital of Orange County (CHOC) and the University Children’s Hospital of the University of California Irvine Medical Center (UCIMC), between 1 January 2000 and 31 December 2003. The sample size was defined as 2 or more admissions, n = 697. | Nitrogen dioxide (NO2), Nox (Nitric oxide and Nitrogen dioxide), and carbon monoxide (CO) concentrations were estimated as the local traffic emissions for both trucks and vehicles within a 5 km radius of each residence. The exposure was stratified by either warm season (May–October) or cool season (November–April). TRAP was measured using CALINE4 model estimates. | Readmission within study timeframe of 4 years or by the patient’s 19th birthday. Only 10 readmissions or less per patient were included. Time to event. Regression analysis using Hazards ratio to estimate effects of environmental factors. |
| The hazards ratio analysis for TRAP and repeat admission (NOx HR 1.094 (1.035–1.156) p = 0.002, aHR 1.097 (1.034–1.164) p = 0.002, CO HR 1.072 (1.016–1.131) p = 0.01, aHR 1.073 (1.013–1.137) p = 0.02). However, there was no association seen for NO2: HR 1.044 (0.992–1.098) p = 0.10 and aHR 1.042 (0.987–1.101). When the models were stratified for sex and TRAP association, for NOx and females HR was 1.136 (1.043–1.238) p = 0.003 and an association was seen between CO and females with HR 1.1 (1.011–1.197) p = 0.02. The point estimates for CO and NOx are also stronger for infants compared to older children: NOx HR 1.197 95% CI (1.075–1.333) p value = 0.02 and CO HR 1.158 95% CI (1.041–1.289) p = 0.007. |
|
| Beck et al. (2016) [22] | Patients (1–16 years) admitted for asthma or bronchodilator-responsive wheezing ICD-9 (493.xx) at the Cincinnati Children’s Hospital Medical Center (CCHMC), an urban, academic, pediatric hospital, between August 2010 and October 2011. n = 774 total population n = 695 readmission population. Descriptive study. | Traffic related air pollutants (TRAP) (Elemental carbon attributed to traffic). TRAP was estimated using land use regression (LUR) models. TRAP was measured as the average daily elemental carbon attributed to traffic (ECAT). When the measure was developed, it was further classified as above or below the median level of 0.37 microgram/m3. | Readmission within the study period of 14 months. Weighted cox proportional hazard regression and Kaplan–Meier curves. |
| The inverse probability of treatment weighting (IPTW) between “White” and African American” for TRAP above sample mean had a standardised mean difference before IPTW was 0.390 and after IPTW was 0.038. For any outdoor allergen sensitisation, the standardised mean difference before IPTW was 0.313 and after was 0.009. |
|
| Descriptive analysis | ||||||
| Vicendese et al. 2014 [15] | Daily childhood (2–18 years) asthma hospital admissions ICD-9 (493) up to 1998 and ICD-10 (J45 or J46) for remaining data until 2009 in Victoria, Australia, between 1997 and 2009 from the Department of Human Services. Readmissions within 28 days were 2401, and readmissions within 1 year were 10263. Ecological time series. | Seasonal trends and the effect of grass pollen season between October and January. The hospital records were divided into autumn, winter, spring, and summer based on the month of admission. The grass pollen season was defined as between October and January, as per Burkhart TRAP. | Readmission within 28 days and 1 year from index admission. Logistic regression. |
| For readmission within 28 days, season (p < 0.001) and age (p = 0.01) were associated for boys in the autumn and summer seasons and age were significant (p = 0.03), and in winter for girls. Once age stratification was applied, differences were observed for autumn and spring in the 6–12-year-old age group between boys and girls (p = 0.02 and p = 0.01, respectively). In the oldest age group, 13–18 years old, differences were observed for boys in autumn (p = 0.03) and girls in summer (p < 0.001). Grass pollen season and age group were only associated for boys (p = 0.01). Whereas readmission within 1 year and summer were associated with boys p = 0.04 and winter p = 0.03 and summer p = 0.004 for girls. However, readmission within 1 year and the grass pollen season for both girls and boys (p = 0.94 and p = 0.31, respectively) were not associated. |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smaller, L.; Batra, M.; Erbas, B. The Effect of Outdoor Environmental Exposure on Readmission Rates for Children and Adolescents with Asthma—A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 7457. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127457
Smaller L, Batra M, Erbas B. The Effect of Outdoor Environmental Exposure on Readmission Rates for Children and Adolescents with Asthma—A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(12):7457. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127457
Chicago/Turabian StyleSmaller, Lisa, Mehak Batra, and Bircan Erbas. 2022. "The Effect of Outdoor Environmental Exposure on Readmission Rates for Children and Adolescents with Asthma—A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 12: 7457. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127457