
The Operationalisation of Sex and Gender in Quantitative Health–Related Research: A Scoping Review

 and
and
Abstract
:1. Introduction
- (1)
- To identify and characterise instruments used in current quantitative health–related research to measure sex and/or gender;
- (2)
- To provide an overview of whether and how sex and/or gender is conceptualised within the identified instruments.
2. Materials and Methods
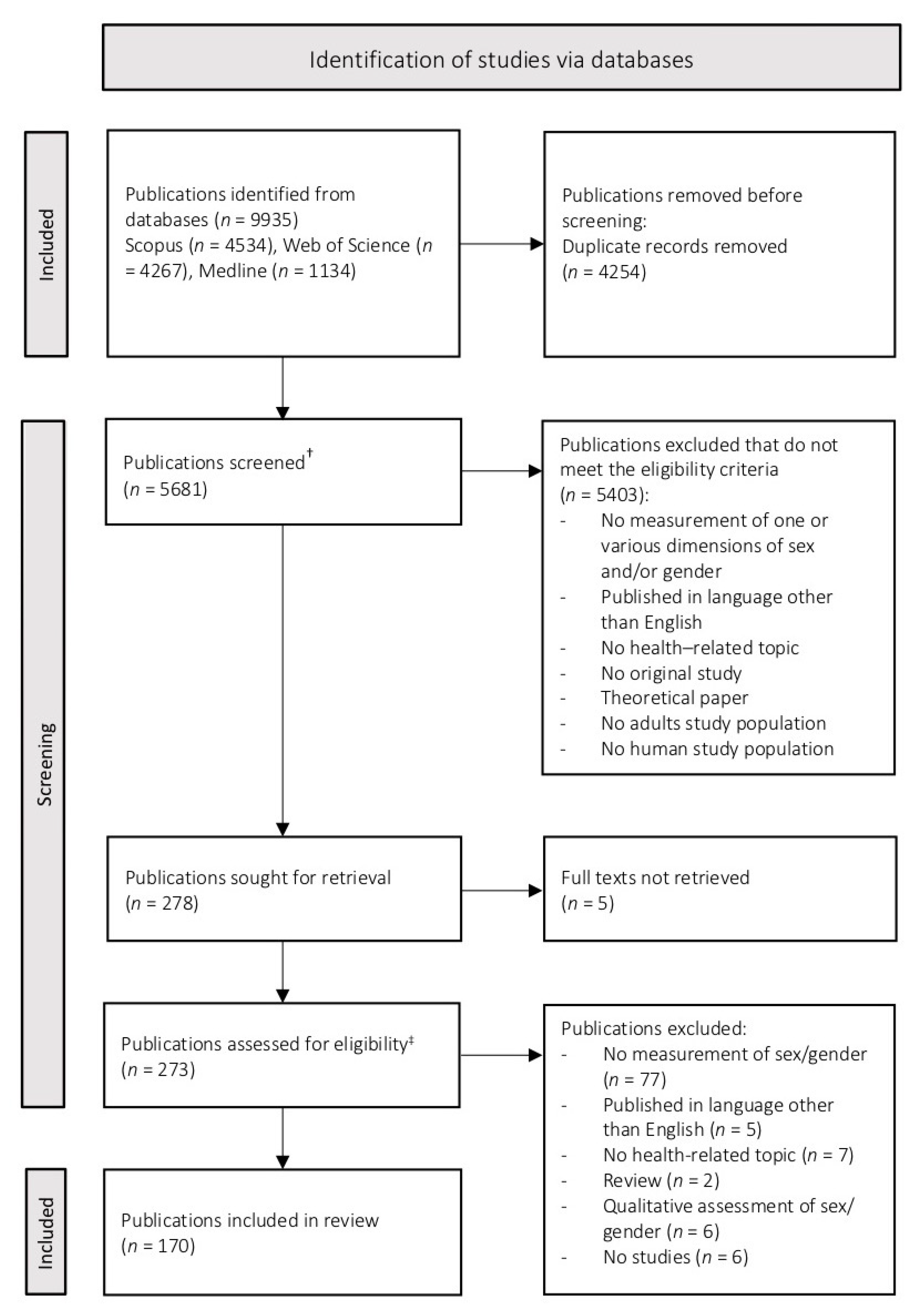
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Selection Process
2.4. Data Extraction and Further Characterisation of the Instruments
2.5. Analysis
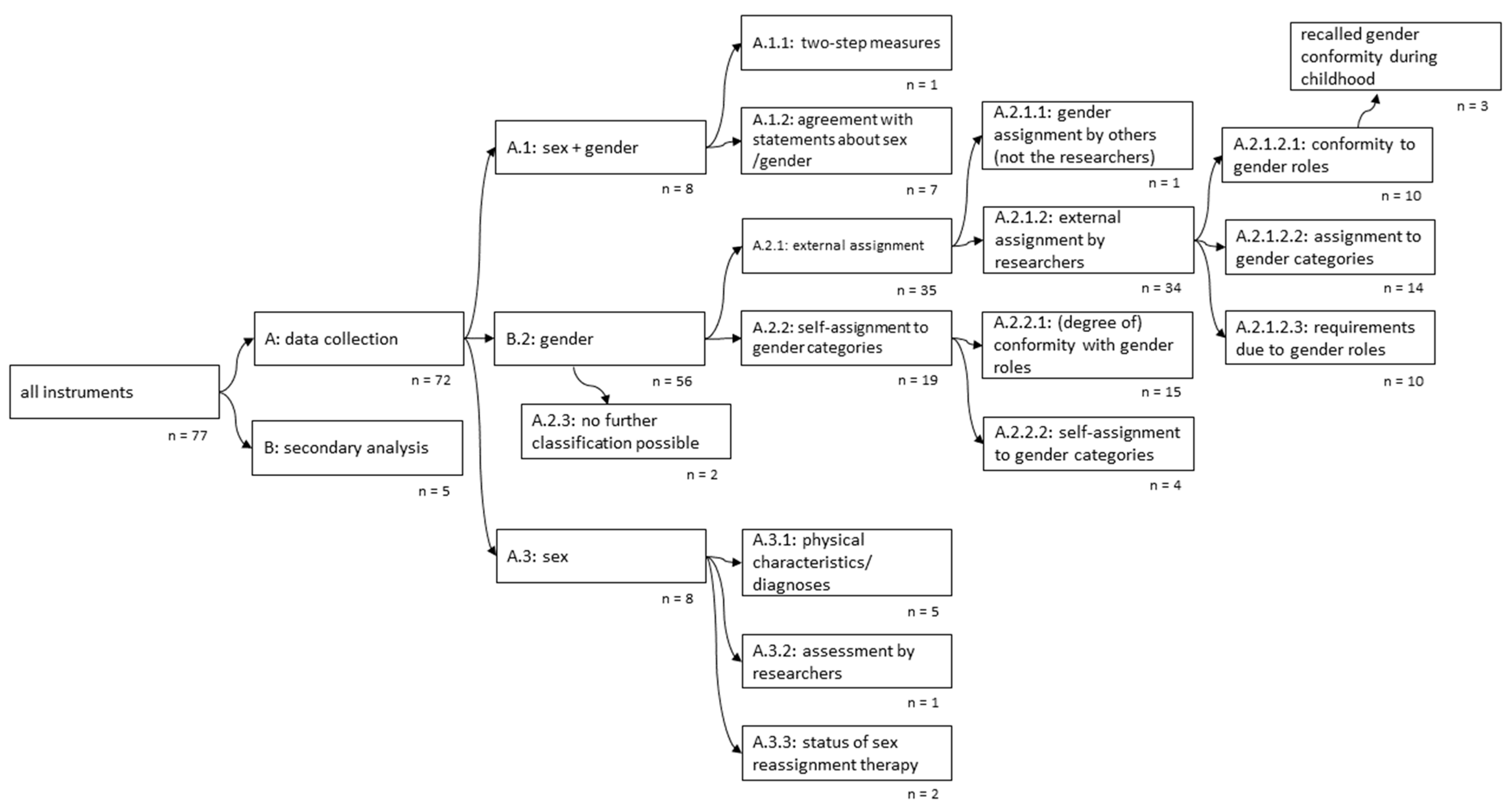
- (a)
- We distinguished between those instruments that have to be employed during data collection and those applied for secondary analysis using already existing data.
- (b)
- We categorised the instruments based on measured dimensions of sex and/or gender and their approach. Since the terms ‘sex’ and ‘gender’ are often confused with each other [11,17,34] and we wanted to achieve comparability, we did not rely on the terminology used in the included publications. Instead, we grouped the instruments according to their captured content. All instruments assessing biological dimensions (e.g., hormonal transition) were categorised as measuring sex, while those focusing on social dimensions (e.g., gender identity) were considered as ‘gender instruments’. Measurements assessing both social and biological dimensions were categorised as ‘sex+gender instruments’.
- (c)
- We additionally classified the instruments into external and self-assessment instruments. Within the external assessment instruments, the participants agree with certain behaviours or traits, and an external person (e.g., the researcher) then assigns the participants to a sex and/or gender category based on these answers. In contrast to this, within the self-assessment instruments, the participants classify themselves into one or multiple sex and/or gender categories.
- (d)
- We distinguished between instruments that are used to assign participants to one or multiple sex and/or gender categories or those that measure the participants’ conformity, degree of belonging to a sex and/or gender category or the expectations and stress participants experience connected to a determined sex and/or gender role.
- (e)
- We differentiated whether the instruments work only with the categories male/female respectively masculinity/femininity (while also allowing different approaches, e.g., various grades of femininity/masculinity) or whether they propose other sex and/or gender categories (e.g., developing the category ‘androgyny’ based on certain grades of masculinity and femininity). All information used for these categorisations was taken from the information provided by the authors who developed the instruments. The categorisation was performed by two independent researchers, and any disagreements were solved by discussion.
3. Results
3.1. Characteristics of Publications and Instruments
3.2. Classification of Instruments
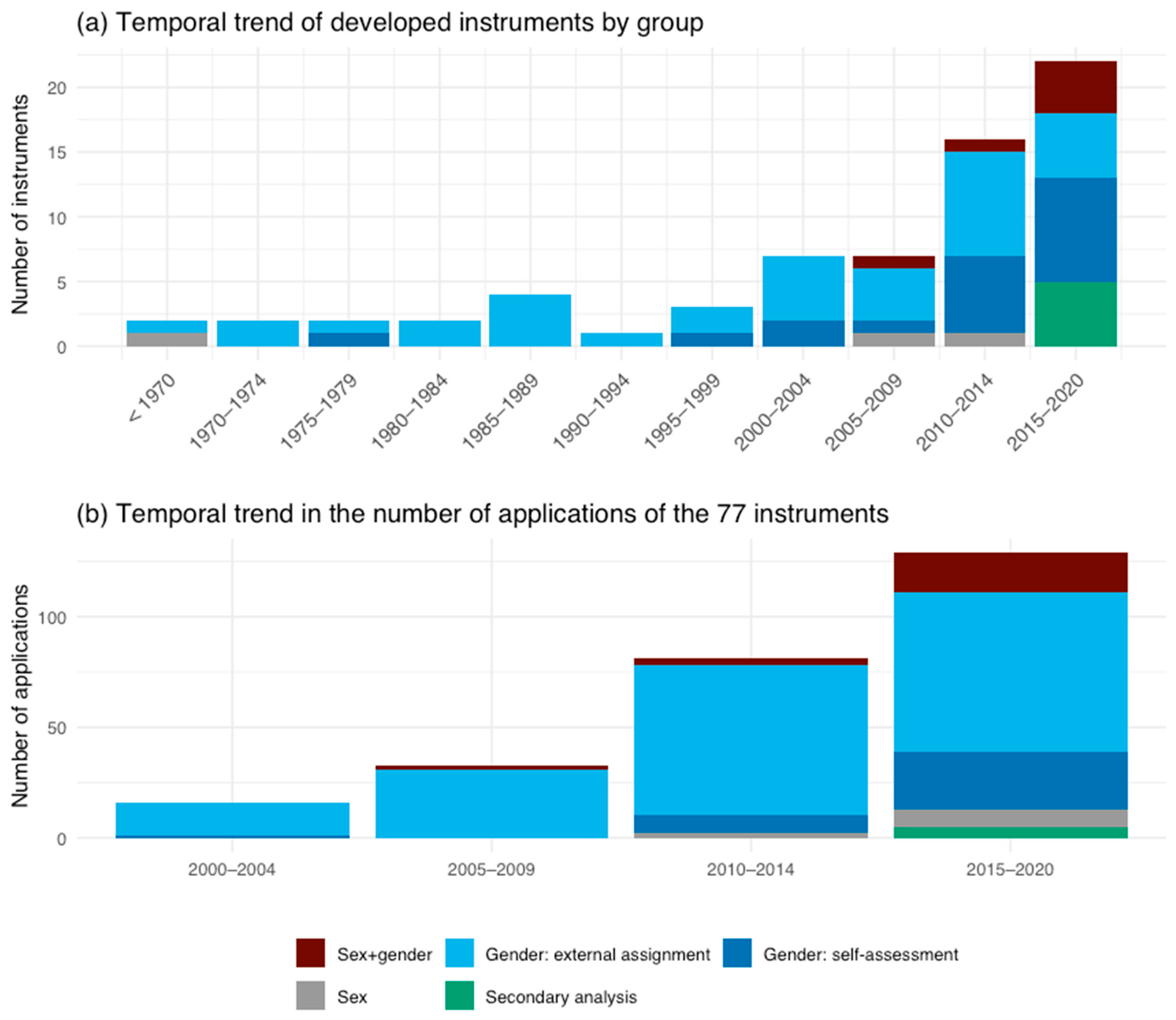
3.3. Temporal Trends
3.4. Classification of Instruments by Concepts of Sex/Gender
3.5. Consideration of Other Social Categories
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bekker, M.H.J. Investigating Gender within Health Research Is More than Sex Disaggregation of Data: A Multi-Facet Gender and Health Model. Psychol. Health Med. 2003, 8, 231–243. [Google Scholar] [CrossRef]
- Bolte, G.; Jacke, K.; Groth, K.; Kraus, U.; Dandolo, L.; Fiedel, L.; Debiak, M.; Kolossa-Gehring, M.; Schneider, A.; Palm, K. Integrating Sex/Gender into Environmental Health Research: Development of a Conceptual Framework. IJERPH 2021, 18, 12118. [Google Scholar] [CrossRef] [PubMed]
- Bottorff, J.L.; Oliffe, J.L.; Robinson, C.A.; Carey, J. Gender Relations and Health Research: A Review of Current Practices. Int J. Equity Health 2011, 10, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regitz-Zagrosek, V.; Seeland, U. Sex and Gender Aspects in Clinical Medicine; Oertelt-Prigione, S., Regitz-Zagrosek, V., Eds.; Springer: London, UK; New York, NY, USA, 2012; ISBN 978-0-85729-831-7. [Google Scholar]
- Palm, K. Verkörperte Sozialität. Zum Interventionspotential Gendertheoretisch Angeleiteter Embodimentforschung in Biologie Und Medizin. In Erkenntnis, Wissen, Intervention. Geschlechterwissenschaftliche Perspektiven; Mahs, C., Riegraf, B., Schröttle, M., Rendtorff, B., Eds.; Beltz Juventa: Weinheim, Germany, 2015. [Google Scholar]
- Mazure, C.M.; Jones, D.P. Twenty Years and Still Counting: Including Women as Participants and Studying Sex and Gender in Biomedical Research. BMC Women’s Health 2015, 15, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieuwenhoven, L.; Klinge, I. Scientific Excellence in Applying Sex- and Gender-Sensitive Methods in Biomedical and Health Research. J. Women’s Health 2010, 19, 313–321. [Google Scholar] [CrossRef]
- European Commission. Directorate General for Research and Innovation. In Horizon Europe Guidance on Gender Equality Plans; Publications Office: Luxembourg, 2021. [Google Scholar]
- Johnson, J.L.; Repta, R. Sex and Gender: Beyond the Binaries. In Designing and Conducting Gender, Sex, & Health Research; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2012; pp. 17–38. ISBN 978-1-4129-8243-6. [Google Scholar]
- Heise, L.; Greene, M.E.; Opper, N.; Stavropoulou, M.; Harper, C.; Nascimento, M.; Zewdie, D.; Darmstadt, G.L.; Greene, M.E.; Hawkes, S.; et al. Gender Inequality and Restrictive Gender Norms: Framing the Challenges to Health. Lancet 2019, 393, 2440–2454. [Google Scholar] [CrossRef]
- Krieger, N. Genders, Sexes, and Health: What Are the Connections—and Why Does It Matter? Int. J. Epidemiol. 2003, 32, 652–657. [Google Scholar] [CrossRef]
- Tannenbaum, C.; Greaves, L.; Graham, I.D. Why Sex and Gender Matter in Implementation Research. BMC Med. Res. Methodol. 2016, 16, 145. [Google Scholar] [CrossRef] [Green Version]
- Hyde, J.S.; Bigler, R.S.; Joel, D.; Tate, C.C.; van Anders, S.M. The Future of Sex and Gender in Psychology: Five Challenges to the Gender Binary. Am. Psychol. 2019, 74, 171–193. [Google Scholar] [CrossRef]
- Springer, K.W.; Mager Stellman, J.; Jordan-Young, R.M. Beyond a Catalogue of Differences: A Theoretical Frame and Good Practice Guidelines for Researching Sex/Gender in Human Health. Soc. Sci. Med. 2012, 74, 1817–1824. [Google Scholar] [CrossRef]
- Hammarström, A.; Johansson, K.; Annandale, E.; Ahlgren, C.; Aléx, L.; Christianson, M.; Elwér, S.; Eriksson, C.; Fjellman-Wiklund, A.; Gilenstam, K.; et al. Central Gender Theoretical Concepts in Health Research: The State of the Art. J. Epidemiol. Community Health 2014, 68, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Schiebinger, L.; Klinge, I. Gendered Innovation in Health and Medicine. Gender 2015, 7, 29–50. [Google Scholar] [CrossRef] [Green Version]
- Heidari, S.; Babor, T.F.; De Castro, P.; Tort, S.; Curno, M. Sex and Gender Equity in Research: Rationale for the SAGER Guidelines and Recommended Use. Res. Integr. Peer Rev. 2016, 1, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, G.R.; Braimoh, J.; Scheim, A.I.; Dharma, C. Transgender-Inclusive Measures of Sex/Gender for Population Surveys: Mixed-Methods Evaluation and Recommendations. PLoS ONE 2017, 12, e0178043. [Google Scholar] [CrossRef] [Green Version]
- Hart, C.G.; Saperstein, A.; Magliozzi, D.; Westbrook, L. Gender and Health: Beyond Binary Categorical Measurement. J. Health Soc. Behav. 2019, 60, 101–118. [Google Scholar] [CrossRef]
- Pelletier, R.; Ditto, B.; Pilote, L. A Composite Measure of Gender and Its Association With Risk Factors in Patients With Premature Acute Coronary Syndrome. Psychosom. Med. 2015, 77, 517–526. [Google Scholar] [CrossRef]
- Lombardi, E.; Banik, S. The Utility of the Two-Step Gender Measure Within Trans and Cis Populations. Sex. Res. Soc. Policy 2016, 13, 288–296. [Google Scholar] [CrossRef]
- Reisner, S.L.; Biello, K.; Rosenberger, J.G.; Austin, S.B.; Haneuse, S.; Perez-Brumer, A.; Novak, D.S.; Mimiaga, M.J. Using a Two-Step Method to Measure Transgender Identity in Latin America/the Caribbean, Portugal, and Spain. Arch. Sex Behav. 2014, 43, 1503–1514. [Google Scholar] [CrossRef] [Green Version]
- The GenIUSS Group. Best Practices for Asking Questions to Identify Transgender and Other Gender Minority Respondents on Population-Based Surveys; The Williams Institute: Los Angeles, CA, USA, 2014. [Google Scholar]
- Ballering, A.V.; Bonvanie, I.J.; Olde Hartman, T.C.; Monden, R.; Rosmalen, J.G.M. Gender and Sex Independently Associate with Common Somatic Symptoms and Lifetime Prevalence of Chronic Disease. Soc. Sci. Med. 2020, 253, 112968. [Google Scholar] [CrossRef]
- Norris, C.M.; Johnson, N.L.; Hardwicke-Brown, E.; McEwan, M.; Pelletier, R.; Pilote, L. The Contribution of Gender to Apparent Sex Differences in Health Status Among Patients with Coronary Artery Disease. J. Women’s Health 2017, 26, 50–57. [Google Scholar] [CrossRef]
- Smith, P.M.; Koehoorn, M. Measuring Gender When You Don’t Have a Gender Measure: Constructing a Gender Index Using Survey Data. Int J. Equity Health 2016, 15, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Döring, N. Zur Operationalisierung von Geschlecht Im Fragebogen: Probleme Und Lösungsansätze Aus Sicht von Mess-, Umfrage-, Gender- Und Queer-Theorie. GENDER-Z. Geschlecht Kult. Ges. 2013, 2, 94–113. [Google Scholar]
- Gómez-Gil, E.; Gómez, A.; Cañizares, S.; Guillamón, A.; Rametti, G.; Esteva, I.; Vázquez, A.; Salamero-Baró, M. Clinical Utility of the Bem Sex Role Inventory (BSRI) in the Spanish Transsexual and Nontranssexual Population. J. Personal. Assess. 2012, 94, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Bem, S.L. The Measurement of Psychological Androgyny. J. Consult. Clin. Psychol. 1974, 42, 155–162. [Google Scholar] [CrossRef]
- Miani, C.; Wandschneider, L.; Niemann, J.; Batram-Zantvoort, S.; Razum, O. Measurement of Gender as a Social Determinant of Health in Epidemiology—A Scoping Review. PLoS ONE 2021, 16, e0259223. [Google Scholar] [CrossRef]
- Nielsen, M.W.; Stefanick, M.L.; Peragine, D.; Neilands, T.B.; Ioannidis, J.P.A.; Pilote, L.; Prochaska, J.J.; Cullen, M.R.; Einstein, G.; Klinge, I.; et al. Gender-Related Variables for Health Research. Biol. Sex. Differ. 2021, 12, 23. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Basic Documents, 49th ed.; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-000051-3. [Google Scholar]
- Hammarström, A.; Annandale, E. A Conceptual Muddle: An Empirical Analysis of the Use of ‘Sex’ and ‘Gender’ in ‘Gender-Specific Medicine’ Journals. PLoS ONE 2012, 7, e34193. [Google Scholar] [CrossRef] [Green Version]
- McCall, L. The Complexity of Intersectionality. Signs J. Women Cult. Soc. 2005, 30, 1771–1800. [Google Scholar] [CrossRef] [Green Version]
- Hepp, U.; Spindler, A.; Milos, G. Eating Disorder Symptomatology and Gender Role Orientation. Int. J. Eat. Disord. 2005, 37, 227–233. [Google Scholar] [CrossRef]
- Raparelli, V.; Romiti, G.; Spugnardi, V.; Borgi, M.; Cangemi, R.; Basili, S.; Proietti, M.; the EVA Collaborative Group. Gender-Related Determinants of Adherence to the Mediterranean Diet in Adults with Ischemic Heart Disease. Nutrients 2020, 12, 759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, C.J.; Keel, P.K. Homosexuality as a Specific Risk Factor for Eating Disorders in Men. Int. J. Eat. Disord. 2002, 31, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Arcand, M.; Juster, R.-P.; Lupien, S.J.; Marin, M.-F. Gender Roles in Relation to Symptoms of Anxiety and Depression among Students and Workers. Anxiety Stress Coping 2020, 33, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Rice, S.M.; Fallon, B.J.; Aucote, H.M.; Möller-Leimkühler, A.M. Development and Preliminary Validation of the Male Depression Risk Scale: Furthering the Assessment of Depression in Men. J. Affect. Disord. 2013, 151, 950–958. [Google Scholar] [CrossRef]
- Mahalik, J.R.; Morray, E.B.; Coonerty-Femiano, A.; Ludlow, L.H.; Slattery, S.M.; Smiler, A. Development of the Conformity to Feminine Norms Inventory. Sex. Roles 2005, 52, 417–435. [Google Scholar] [CrossRef] [Green Version]
- Orlofsky, J.L. Relationship between Sex Role Attitudes and Personality Traits and the Sex Role Behavior Scale-1: A New Measure of Masculine and Feminine Role Behaviors and Interests. J. Personal. Soc. Psychol. 1981, 40, 927–940. [Google Scholar] [CrossRef]
- Donnelly, K.; Twenge, J.M. Masculine and Feminine Traits on the Bem Sex-Role Inventory, 1993–2012: A Cross-Temporal Meta-Analysis. Sex. Roles 2017, 76, 556–565. [Google Scholar] [CrossRef]
- Carver, L.F.; Vafaei, A.; Guerra, R.; Freire, A.; Phillips, S.P. Gender Differences: Examination of the 12-Item Bem Sex Role Inventory (BSRI-12) in an Older Brazilian Population. PLoS ONE 2013, 8, e76356. [Google Scholar] [CrossRef] [Green Version]
- Choi, N.; Fuqua, D.R.; Newman, J.L. The Bem Sex-Role Inventory: Continuing Theoretical Problems. Educ. Psychol. Meas. 2008, 68, 881–900. [Google Scholar] [CrossRef]
- Agbayani, P.; Min, J.W. Examining the Validity of the Bem Sex Role Inventory for Use with Filipino Americans Using Confirmatory Factor Analysis. J. Ethn. Cult. Divers. Soc. Work 2006, 15, 55–80. [Google Scholar] [CrossRef]
- Ferrer-Pérez, V.A.; Bosch-Fiol, E. The Measure of the Masculinity–Femininity Construct Today: Some Reflections on the Case of the Bem Sex Role Inventory/La Medida Del Constructo Masculinidad–Feminidad En La Actualidad: Algunas Reflexiones Sobre El Caso Del Bem Sex Role Inventory. Rev. Psicol. Soc. 2014, 29, 180–207. [Google Scholar] [CrossRef]
- Carothers, B.J.; Reis, H.T. Men and Women Are from Earth: Examining the Latent Structure of Gender. J. Personal. Soc. Psychol. 2013, 104, 385–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rippon, G.; Jordan-Young, R.; Kaiser, A.; Fine, C. Recommendations for Sex/Gender Neuroimaging Research: Key Principles and Implications for Research Design, Analysis, and Interpretation. Front. Hum. Neurosci. 2014, 8, 650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fausto-Sterling, A. Sexing the Body: Gender Politics and the Construction of Sexuality, 1st ed.; Basic Books: New York, NY, USA, 2000; ISBN 978-0-465-07713-7. [Google Scholar]
- Oyěwùmí, O. The Invention of Women: Making an African Sense of Western Gender Discourses; University of Minnesota Press: Minneapolis, MN, USA, 1997; ISBN 978-0-8166-2440-9. [Google Scholar]
- Bockting, W.O.; Miner, M.H.; Swinburne Romine, R.E.; Dolezal, C.; Robinson, B.E.; Rosser, B.R.S.; Coleman, E. The Transgender Identity Survey: A Measure of Internalized Transphobia. LGBT Health 2020, 7, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Tate, C.C.; Ledbetter, J.N.; Youssef, C.P. A Two-Question Method for Assessing Gender Categories in the Social and Medical Sciences. J. Sex Res. 2013, 50, 767–776. [Google Scholar] [CrossRef]
- Day, S.; Mason, R.; Tannenbaum, C.; Rochon, P.A. Essential Metrics for Assessing Sex & Gender Integration in Health Research Proposals Involving Human Participants. PLoS ONE 2017, 12, e0182812. [Google Scholar] [CrossRef]
- Day, S.; Mason, R.; Lagosky, S.; Rochon, P.A. Integrating and Evaluating Sex and Gender in Health Research. Health Res. Policy Sys 2016, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Sexual Minority Assessment Research Team (SMART) Best Practices for Asking Questions about Sexual Orientation on Surveys. 2009. Available online: https://williamsinstitute.law.ucla.edu/publications/smart-so-survey/ (accessed on 14 March 2022).
- Mahalik, J.R.; Locke, B.D.; Ludlow, L.H.; Diemer, M.A.; Scott, R.P.J.; Gottfried, M.; Freitas, G. Development of the Conformity to Masculine Norms Inventory. Psychol. Men Masc. 2003, 4, 3–25. [Google Scholar] [CrossRef]
- Bowleg, L. The Problem with the Phrase, Women and Minorities: Intersectionality—an Important Theoretical Framework for Public Health. Am. J. Public Health 2012, 102, 1267–1273. [Google Scholar] [CrossRef]
- Mena, E.; Bolte, G. On behalf of the ADVANCE GENDER Study Group Intersectionality-Based Quantitative Health Research and Sex/Gender Sensitivity: A Scoping Review. Int J. Equity Health 2019, 18, 199. [Google Scholar] [CrossRef] [Green Version]
- Weaver, J.; Sargent, S.L. Gender Role Inventory: In Handbook of Research on Electronic Surveys and Measurements; Reynolds, R.A., Woods, R., Baker, J.D., Eds.; IGI Global: Hershey, PA, USA, 2007; pp. 367–370. ISBN 978-1-59140-792-8. [Google Scholar]
- Schellenberg, D.; Kaiser, A. The Sex/Gender Distinction: Beyond f and m. In APA Handbook of the Psychology of Women: History, Theory, and Battlegrounds; Travis, C.B., White, J.W., Rutherford, A., Williams, W.S., Cook, S.L., Wyche, K.F., Eds.; American Psychological Association: Washington, DC, USA, 2018; Volume 1, pp. 165–187. ISBN 978-1-4338-2800-3. [Google Scholar]
- Lofters, A.; O’Campo, P. Differences That Matter. In Rethinking Social Epidemiology: Towards a Science of Change; O’Campo, P., Dunn, J.R., Eds.; Springer Netherlands: Dordrecht, The Netherlands, 2012; pp. 93–109. [Google Scholar]
- Cella, S.; Iannaccone, M.; Cotrufo, P. Influence of gender role orientation (masculinity versus femininity) on body satisfaction and eating attitudes in homosexuals, heterosexuals and transsexuals. Eat. Weight Disord. - Stud. Anorexia, Bulim. Obes. 2013, 18, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.A.; Bouman, W.P.; Haycraft, E.; Arcelus, J. The Gender Congruence and Life Satisfaction Scale (GCLS): Development and validation of a scale to measure outcomes from transgender health services. Int. J. Transgenderism 2018, 20, 63–80. [Google Scholar] [CrossRef] [PubMed]
- McGuire, J.K.; Beek, T.F.; Catalpa, J.M.; Steensma, T. The Genderqueer Identity (GQI) Scale: Measurement and validation of four distinct subscales with trans and LGBQ clinical and community samples in two countries. Int. J. Transgenderism 2018, 20, 289–304. [Google Scholar] [CrossRef] [PubMed]
- Michaels, S.; Milesi, C.; Stern, M.; Viox, M.H.; Morrison, H.; Guerino, P.; Dragon, C.N.; Haffer, S.C. Improving Measures of Sexual and Gender Identity in English and Spanish to Identify LGBT Older Adults in Surveys. LGBT Health 2017, 4, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagata, J.M.; Murray, S.B.; Compte, E.J.; Pak, E.H.; Schauer, R.; Flentje, A.; Capriotti, M.R.; Lubensky, M.E.; Lunn, M.R.; Obedin-Maliver, J. Community norms for the Eating Disorder Examination Questionnaire (EDE-Q) among transgender men and women. Eat. Behav. 2020, 37, 101381. [Google Scholar] [CrossRef]
- Pickett, A.C.; Valdez, D.; Barry, A.E. Measurement implications associated with refinement of sexual and gender identity survey items: A case study of the National College Health Assessment. J. Am. Coll. Health 2019, 68, 720–726. [Google Scholar] [CrossRef]
- Reisner, S.L.; Conron, K.J.; Tardiff, L.A.; Jarvi, S.; Gordon, A.R.; Austin, S.B. Monitoring the health of transgender and other gender minority populations: Validity of natal sex and gender identity survey items in a U.S. national cohort of young adults. BMC Public Health 2014, 14, 1224. [Google Scholar] [CrossRef] [Green Version]
- Tamar-Mattis, S.; Gamarel, K.; Kantor, A.; Baratz, A.; Tamar-Mattis, A.; Operario, D. Identifying and Counting Individuals with Differences of Sex Development Conditions in Population Health Research. LGBT Health 2018, 5, 320–324. [Google Scholar] [CrossRef]
- Tate, C.C.; Bettergarcia, J.; Brent, L.M. Re-assessing the Role of Gender-Related Cognitions for Self-Esteem: The Importance of Gender Typicality for Cisgender Adults. Sex Roles 2015, 72, 221–236. [Google Scholar] [CrossRef]
- Taube, L.N.; Mussap, A.J. Evaluating the transgender positive identity measure (T-PIM) across intersecting identities. J. Gay Lesbian Ment. Health 2020, 25, 20–53. [Google Scholar] [CrossRef]
- Walls, N.E.; Kattari, S.K.; Speer, S.R.; Kinney, M.K. Transfeminine Spectrum Parenting: Evidence from the National Transgender Discrimination Survey. Soc. Work Res. 2019, 43, 133–144. [Google Scholar] [CrossRef]
- Chesebro, J.W.; Fuse, K. The development of a perceived masculinity scale. Commun. Q. 2001, 49, 203–278. [Google Scholar] [CrossRef]
- Bauer, G. Making Sure Everyone Counts: Considerations for Inclusion, Identification and Analysis of Transgender and Transsexual Participants in Health Surveys/Pour s’assurer que tout le monde compte: Facteurs pouvant justifier l’inclusion, l’identification et l’analyse de participants transgenres et transsexuels dans les enquêtes sur la santé. Open Collect. 2012. [Google Scholar] [CrossRef]
- Hakeem, A.; Črnčec, R.; Asghari-Fard, M.; Harte, F.; Eapen, V. Development and validation of a measure for assessing gender dysphoria in adults: The Gender Preoccupation and Stability Questionnaire. Int. J. Transgenderism 2016, 17, 131–140. [Google Scholar] [CrossRef]
- Scheim, A.I.; Bauer, G.R. Sex and Gender Diversity Among Transgender Persons in Ontario, Canada: Results From a Respondent-Driven Sampling Survey. J. Sex Res. 2014, 52, 1–14. [Google Scholar] [CrossRef]
- Dharma, C.; Scheim, A.I.; Bauer, G.R. Exploratory Factor Analysis of Two Sexual Health Scales for Transgender People: Trans-Specific Condom/Barrier Negotiation Self-Efficacy (T-Barrier) and Trans-Specific Sexual Body Image Worries (T-Worries). Arch. Sex. Behav. 2019, 48, 1563–1572. [Google Scholar] [CrossRef]
- Ho, F.; Mussap, A.J. The Gender Identity Scale: Adapting the Gender Unicorn to measure gender identity. Psychol. Sex. Orientat. Gend. Divers. 2019, 6, 217–231. [Google Scholar] [CrossRef]
- Ho, F.; Mussap, A.J. Development of the Trans and Gender Diverse Social Anxiety Scale. Anxiety, Stress Coping 2020, 33, 675–697. [Google Scholar] [CrossRef]
- Epletzer, B.; Epetasis, O.; Ortner, T.M.; Ecahill, L. Interactive effects of culture and sex hormones on the sex role self-concept. Front. Neurosci. 2015, 9, 240. [Google Scholar] [CrossRef] [Green Version]
- Gruber, F.M.; Distlberger, E.; Scherndl, T.; Ortner, T.M.; Pletzer, B. Psychometric Properties of the Multifaceted Gender-Related Attributes Survey (GERAS). Eur. J. Psychol. Assess. 2020, 36, 612–623. [Google Scholar] [CrossRef]
- Zucker, K.J.; Mitchell, J.N.; Bradley, S.J.; Tkachuk, J.; Cantor, J.M.; Allin, S.M. The Recalled Childhood Gender Identity/Gender Role Questionnaire: Psychometric Properties. Sex Roles 2006, 54, 469–483. [Google Scholar] [CrossRef]
- Green, L.; Rimes, K.A.; Rahman, Q. Beliefs About Others’ Perceptions—Gender Typicality: Scale Development and Relationships to Gender Nonconformity, Sexual Orientation, and Well-Being. J. Sex Res. 2017, 55, 837–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, D.; Deogracias, J.J.; Johnson, L.L.; Bradley, S.J.; Kibblewhite, S.J.; Owen-Anderson, A.; Peterson-Badali, M.; Meyer-Bahlburg, H.F.L.; Zucker, K.J. The Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults: Further Validity Evidence. J. Sex Res. 2010, 47, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Veale, J.F. Factorial Validity and Invariance Assessment of a Short Version of the Recalled Childhood Gender Identity/Role Questionnaire. Arch. Sex. Behav. 2016, 45, 537–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, J.M.; Oberschneider, M. Sexual orientation and professional dance. Arch. Sex. Behav. 1997, 26, 433–444. [Google Scholar] [CrossRef]
- Skidmore, W.C.; Linsenmeier, J.A.W.; Bailey, M. Gender Nonconformity and Psychological Distress in Lesbians and Gay Men. Arch. Sex. Behav. 2006, 35, 685–697. [Google Scholar] [CrossRef]
- Kachel, S.; Steffens, M.C.; Niedlich, C. Traditional Masculinity and Femininity: Validation of a New Scale Assessing Gender Roles. Front. Psychol. 2016, 7, 956. [Google Scholar] [CrossRef] [Green Version]
- Burk, L.R.; Burkhart, B.R.; Sikorski, J.F. Construction and Preliminary Validation of the Auburn Differential Masculinity Inventory. Psychol. Men Masculinities 2004, 5, 4–17. [Google Scholar] [CrossRef] [Green Version]
- Blanchard, R.; Freund, K. Measuring masculine gender identity in females. J. Consult. Clin. Psychol. 1983, 51, 205–214. [Google Scholar] [CrossRef]
- Lehavot, K.; King, K.M.; Simoni, J.M. Development and Validation of a Gender Expression Measure Among Sexual Minority Women. Psychol. Women Q. 2011, 35, 381–400. [Google Scholar] [CrossRef]
- Alt, M.; Lewis, A.M.; Liu, W.M.; Vilain, E.; Sánchez, F.J. On the Validity of Popular Masculinity Rating Scales with Gay Men. Arch. Sex. Behav. 2014, 43, 1547–1557. [Google Scholar] [CrossRef] [PubMed]
- Brabete, A.C.; Sánchez-López, M.D.P. How does the gender influence people’s health? Data of a sample of Romanian people living in Spain. Procedia -Soc. Behav. Sci. 2012, 33, 148–152. [Google Scholar] [CrossRef] [Green Version]
- Brabete, A.C.; Sánchez-López, M.D.P.; Cuéllar-Flores, I.; Rivas-Diez, R. The Impact of Gender Norms on Alcohol and Tobacco Use at Romanians. Procedia -Soc. Behav. Sci. 2013, 78, 230–234. [Google Scholar] [CrossRef] [Green Version]
- Burn, S.M.; Ward, A.Z. Men’s Conformity to Traditional Masculinity and Relationship Satisfaction. Psychol. Men Masculinities 2005, 6, 254–263. [Google Scholar] [CrossRef] [Green Version]
- Easton, S.D. Masculine norms, disclosure, and childhood adversities predict long-term mental distress among men with histories of child sexual abuse. Child Abus. Negl. 2014, 38, 243–251. [Google Scholar] [CrossRef]
- Esteban-Gonzalo, L.; Manso-Martínez, M.E.; Botín-González, P.; Manchado-Simal, B.; Rodrigo-De-Frutos, R.M.; González-Pascual, J.L. The relationship between conformity to male and female gender norms and depression during pregnancy. Arch. Women’s Ment. Health 2019, 22, 809–815. [Google Scholar] [CrossRef]
- Hammer, J.H.; Heath, P.J.; Vogel, D.L. Fate of the total score: Dimensionality of the Conformity to Masculine Norms Inventory-46 (CMNI-46). Psychol. Men Masculinities 2018, 19, 645–651. [Google Scholar] [CrossRef]
- Hayley, A.; Cox, E.; Zinkiewicz, L.; Graham, K.; Wells, S.; Zhou, J.; Miller, P.G. Barroom aggression perpetration by Australian women: Associations with heavy episodic drinking, trait aggression, and conformity to gender norms. J. Subst. Use 2017, 22, 597–604. [Google Scholar] [CrossRef]
- Levant, R.F.; Hall, R.J.; Weigold, I.K.; McCurdy, E.R. Construct distinctiveness and variance composition of multi-dimensional instruments: Three short-form masculinity measures. J. Couns. Psychol. 2015, 62, 488–502. [Google Scholar] [CrossRef]
- Levant, R.F.; McDermott, R.; Parent, M.C.; Alshabani, N.; Mahalik, J.R.; Hammer, J.H. Development and evaluation of a new short form of the Conformity to Masculine Norms Inventory (CMNI-30). J. Couns. Psychol. 2020, 67, 622–636. [Google Scholar] [CrossRef]
- Ludlow, L.H.; Mahalik, J.R. Congruence between a theoretical continuum of masculinity and the Rasch model: Examining the Conformity to Masculine Norms Inventory. J. Appl. Meas. 2001, 2, 205–226. [Google Scholar] [PubMed]
- Magovcevic, M.; Addis, M.E. The Masculine Depression Scale: Development and psychometric evaluation. Psychol. Men Masculinities 2008, 9, 117–132. [Google Scholar] [CrossRef] [Green Version]
- Murray, S.B.; Rieger, E.; Karlov, L.; Touyz, S.W. Masculinity and femininity in the divergence of male body image concerns. J. Eat. Disord. 2013, 1, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owen, J. Assessing the Factor Structures of the 55- and 22-Item Versions of the Conformity to Masculine Norms Inventory. Am. J. Men’s Health 2010, 5, 118–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parent, M.C.; Moradi, B. Confirmatory factor analysis of the Conformity to Masculine Norms Inventory and development of the Conformity to Masculine Norms Inventory-46. Psychol. Men Masculinities 2009, 10, 175–189. [Google Scholar] [CrossRef]
- Parent, M.C.; Davis-Delano, L.R.; Morgan, E.M.; Woznicki, N.W.; Denson, A. An Inductive Analysis of Young Adults’ Conceptions of Femininity and Masculinity and Comparison to Established Gender Inventories. Gend. Issues 2019, 37, 1–24. [Google Scholar] [CrossRef]
- Parent, M.C.; Smiler, A.P. Metric invariance of the Conformity to Masculine Norms Inventory-46 among women and men. Psychol. Men Masculinities 2013, 14, 324–328. [Google Scholar] [CrossRef]
- Rochelle, T.L.; Yim, K.H. Assessing the Factor Structure of the Chinese Conformity to Masculine Norms Inventory. J. Psychol. 2014, 149, 29–41. [Google Scholar] [CrossRef]
- Steinfeldt, J.A.; Gilchrist, G.A.; Halterman, A.W.; Gomory, A.; Steinfeldt, M.C. Drive for muscularity and conformity to masculine norms among college football players. Psychol. Men Masculinities 2011, 12, 324–338. [Google Scholar] [CrossRef] [Green Version]
- Wide, J.; Mok, H.; McKenna, M.; Ogrodniczuk, J.S. Effect of gender socialization on the presentation of depression among men: A pilot study. Can. Fam. Physician 2011, 57, e74–e78. [Google Scholar]
- Wong, Y.J.; Shea, M.; Hickman, S.J.; LaFollette, J.R.; Cruz, N.; Boghokian, T. The Subjective Masculinity Stress Scale: Scale development and psychometric properties. Psychol. Men Masculinities 2013, 14, 148–155. [Google Scholar] [CrossRef]
- Aparicio-García, M.E.; Alvarado-Izquierdo, J.M. Is there a “Conformity to Feminine Norms” Construct? A Bifactor Analysis of two Short Versions of Conformity to Feminine Norms Inventory. Curr. Psychol. 2018, 38, 1110–1120. [Google Scholar] [CrossRef]
- Brown, E.L.; Ovrebo, E.; Emery, H.E.; Stenersen, M. The Validity of the Conformity to Feminine Norms Inventory with Sexual and Gender Minority Women. J. LGBTQ Issues Couns. 2020, 14, 56–68. [Google Scholar] [CrossRef]
- Green, M.A.; Davids, C.M.; Skaggs, A.K.; Riopel, C.M.; Hallengren, J.J. Femininity and Eating Disorders. Eat. Disord. 2008, 16, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Kling, J.; Gattario, K.H.; Frisén, A. Swedish women’s perceptions of and conformity to feminine norms. Scand. J. Psychol. 2017, 58, 238–248. [Google Scholar] [CrossRef] [Green Version]
- Lyócsa, I.; Lyocsa, S. Confirmatory Factor Analysis of the Abbreviated Conformity to Feminine Norms Inventory. Soc. Work Res. 2013, 37, 414–422. [Google Scholar] [CrossRef]
- Parent, M.C.; Moradi, B. Confirmatory Factor Analysis of the Conformity to Feminine Norms Inventory and Development of an Abbreviated Version: The CFNI-45. Psychol. Women Q. 2010, 34, 97–109. [Google Scholar] [CrossRef]
- Parent, M.C.; Moradi, B. An abbreviated tool for assessing feminine norm conformity: Psychometric properties of the Conformity to Feminine Norms Inventory–45. Psychol. Assess. 2011, 23, 958–969. [Google Scholar] [CrossRef]
- Deogracias, J.J.; Johnson, L.L.; Meyer-Bahlburg, H.F.L.; Kessler, S.J.; Schober, J.M.; Zucker, K.J. The Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults. J. Sex Res. 2007, 44, 370–379. [Google Scholar] [CrossRef]
- Fisher, A.D.; Castellini, G.; Ristori, J.; Casale, H.; Giovanardi, G.; Carone, N.; Fanni, E.; Mosconi, M.; Ciocca, G.; Jannini, E.A.; et al. Who has the worst attitudes toward sexual minorities? Comparison of transphobia and homophobia levels in gender dysphoric individuals, the general population and health care providers. J. Endocrinol. Investig. 2016, 40, 263–273. [Google Scholar] [CrossRef]
- Galupo, M.P.; Pulice-Farrow, L. Subjective Ratings of Gender Dysphoria Scales by Transgender Individuals. Arch. Sex. Behav. 2019, 49, 479–488. [Google Scholar] [CrossRef] [PubMed]
- George, R.; A Stokes, M. Gender identity and sexual orientation in autism spectrum disorder. Autism 2017, 22, 970–982. [Google Scholar] [CrossRef] [PubMed]
- Haghighat, F.; Shirazi, E.; Ardebili, M.E.; Alavi, K. Psychometric Assessment of the Persian Version of a Dimensional Instrument to Measure Gender Identity Disorder. Latinoamericana de Hipertensión 2019, 14, 346–353. [Google Scholar]
- Schneider, C.; Cerwenka, S.; Nieder, T.; Briken, P.; Cohen-Kettenis, P.T.; De Cuypere, G.; Haraldsen, I.R.; Kreukels, B.P.C.; Richter-Appelt, H. Measuring Gender Dysphoria: A Multicenter Examination and Comparison of the Utrecht Gender Dysphoria Scale and the Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults. Arch. Sex. Behav. 2016, 45, 551–558. [Google Scholar] [CrossRef]
- Taskinen, S.; Suominen, J.S.; Mattila, A.K. Gender Identity and Sex Role of Patients Operated on for Bladder Exstrophy-Epispadias. J. Urol. 2016, 196, 531–535. [Google Scholar] [CrossRef]
- Cohen-Kettenis, P.T.; VAN Goozen, S.H. Sex Reassignment of Adolescent Transsexuals: A Follow-up Study. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 263–271. [Google Scholar] [CrossRef]
- Jürgensen, M.; Kleinemeier, E.; Lux, A.; Steensma, T.D.; Cohen-Kettenis, P.T.; Hiort, O.; Thyen, U.; Köhler, B. Psychosexual Development in Adolescents and Adults with Disorders of Sex Development—Results from the German Clinical Evaluation Study. J. Sex. Med. 2013, 10, 2703–2714. [Google Scholar] [CrossRef]
- Kreukels, B.P.; Köhler, B.; Nordenström, A.; Roehle, R.; Thyen, U.; Bouvattier, C.; de Vries, A.L.; Cohen-Kettenis, P.T.; Arlt, W.; Wiesemann, C.; et al. Gender Dysphoria and Gender Change in Disorders of Sex Development/Intersex Conditions: Results From the dsd-LIFE Study. J. Sex. Med. 2018, 15, 777–785. [Google Scholar] [CrossRef]
- van de Grift, T.C.; Elaut, E.; Cerwenka, S.C.; Cohen-Kettenis, P.T.; De Cuypere, G.; Richter-Appelt, H.; Kreukels, B.P. Effects of Medical Interventions on Gender Dysphoria and Body Image: A Follow-Up Study. Psychosom. Med. 2017, 79, 815–823. [Google Scholar] [CrossRef] [Green Version]
- Wylie, S.A.; Corliss, H.; Boulanger, V.; Prokop, L.A.; Austin, S.B. Socially Assigned Gender Nonconformity: A Brief Measure for Use in Surveillance and Investigation of Health Disparities. Sex Roles 2010, 63, 264–276. [Google Scholar] [CrossRef]
- Choi, N.; Fuqua, D.R.; Newman, J.L. Hierarchical Confirmatory Factor Analysis of the Bem Sex Role Inventory. Educ. Psychol. Meas. 2007, 67, 818–832. [Google Scholar] [CrossRef]
- Choi, N.; Fuqua, D.R.; Newman, J.L. Exploratory and Confirmatory Studies of the Structure of the Bem Sex Role Inventory Short Form With Two Divergent Samples. Educ. Psychol. Meas. 2009, 69, 696–705. [Google Scholar] [CrossRef]
- Costa, P.A.; Garcia, I.Q.; Pimenta, F.; Marôco, J.; Leal, I. Late-onset hypogonadism (LOH), masculinity and relationship and sexual satisfaction: Are sexual symptoms of LOH mediators of traditional masculinity on relationship and sexual satisfaction? Sex. Health 2019, 16, 389. [Google Scholar] [CrossRef]
- Crosby, J.P.; Sprock, J. Effect of patient sex, clinician sex, and sex role on the diagnosis of Antisocial Personality Disorder: Models of underpathologizing and overpathologizing biases. J. Clin. Psychol. 2004, 60, 583–604. [Google Scholar] [CrossRef] [PubMed]
- Endut, N.; Bagheri, R.; Azman, A.; Hashim, I.H.M.; Selamat, N.H.; Mohajer, L. The Effect of Gender Role on Attitudes Towards Inequitable Gender Norms Among Malaysian Men. Sex. Cult. 2020, 24, 2113–2136. [Google Scholar] [CrossRef]
- Factor, R.J.; Rothblum, E.D. A Comparison of Trans Women, Trans Men, Genderqueer Individuals, and Cisgender Brothers and Sisters on the Bem Sex-Role Inventory: Ratings by Self and Siblings. J. Homosex. 2017, 64, 1872–1889. [Google Scholar] [CrossRef] [PubMed]
- Fisher, A.D.; Bandini, E.; Ricca, V.; Ferruccio, N.; Corona, G.; Meriggiola, M.C.; Jannini, E.A.; Manieri, C.; Ristori, J.; Forti, G.; et al. Dimensional Profiles of Male to Female Gender Identity Disorder: An Exploratory Research. J. Sex. Med. 2010, 7, 2487–2498. [Google Scholar] [CrossRef]
- Geldenhuys, M.; Bosch, A. A Rasch Adapted Version of the 30-Item Bem Sex Role Inventory (BSRI). J. Pers. Assess. 2019, 102, 428–439. [Google Scholar] [CrossRef]
- Ghiasi, A. The effect of gender-role orientation on attitudes towards menstruation in a sample of female university students. J. Turk. Gynecol. Assoc. 2019, 20, 138–141. [Google Scholar] [CrossRef]
- Hoffmann, W.; Latza, U.; Baumeister, S.E.; Brünger, M.; Buttmann-Schweiger, N.; Hardt, J.; Hoffmann, V.; Karch, A.; Richter, A.; Schmidt, C.O.; et al. Guidelines and recommendations for ensuring Good Epidemiological Practice (GEP): A guideline developed by the German Society for Epidemiology. Eur. J. Epidemiology 2019, 34, 301–317. [Google Scholar] [CrossRef] [Green Version]
- Hunt, K.; Lewars, H.; Emslie, C.; Batty, G.D. Decreased risk of death from coronary heart disease amongst men with higher ’femininity’ scores: A general population cohort study. Int. J. Epidemiology 2007, 36, 612–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, H.D.; McNair, R.; Vojick, A.; Congdon, D.; Monacelli, J.; Lamont, J. Categorical and continuous measurement of sex-role orientation: Differences in associations with young adults’reports of well-being. Soc. Behav. Pers. Int. J. 2006, 34, 59–76. [Google Scholar] [CrossRef]
- Juster, R.-P.; Lupien, S. A Sex- and Gender-Based Analysis of Allostatic Load and Physical Complaints. Gend. Med. 2012, 9, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Kamboj, S.K.; Oldfield, L.; Loewenberger, A.; Das, R.K.; Bisby, J.; Brewin, C.R. Voluntary and involuntary emotional memory following an analogue traumatic stressor: The differential effects of communality in men and women. J. Behav. Ther. Exp. Psychiatry 2014, 45, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Karim, H.; Shirazi, E.; Nohesara, S.; Sadeghi, H.M.; Saeb, A.; Alavi, K. Comparison of Gender Roles in Male and Female in Patients with Borderline Personality Disorder (BPD) with Control Group and It’s Correlation with Severity of Clinical Symptoms. Rev. Latinoam. Hipertens. 2019, 14, 1–7. [Google Scholar]
- Klingemann, H.; Gomez, V. Masculinity issues in addiction treatment in Swiss inpatient alcohol programs: Bringing men’s treatment needs back to the research agenda. J. Men’s Health 2010, 7, 211–220. [Google Scholar] [CrossRef]
- Kurpisz, J.; Mak, M.; Lew-Starowicz, M.; Nowosielski, K.; Bieńkowski, P.; Kowalczyk, R.; Misiak, B.; Frydecka, D.; Samochowiec, J. Personality traits, gender roles and sexual behaviours of young adult males. Ann. Gen. Psychiatry 2016, 15, 28. [Google Scholar] [CrossRef] [Green Version]
- March, E.; Grieve, R.; Marx, E.; Witteveen, K. More of a (wo)man offline? Gender roles measured in online and offline environments. Pers. Individ. Differ. 2013, 55, 887–891. [Google Scholar] [CrossRef]
- Nielsen, K.J.; Hansen, C.D.; Bloksgaard, L.; Christensen, A.-D.; Jensen, S.Q.; Kyed, M. The impact of masculinity on safety oversights, safety priority and safety violations in two male-dominated occupations. Saf. Sci. 2015, 76, 82–89. [Google Scholar] [CrossRef]
- O’Kelly, M. Psychometric Properties of the O’Kelly Women’s Belief Scales. J. Ration. Cogn. Ther. 2010, 29, 145–157. [Google Scholar] [CrossRef]
- Oswald, P.A. An Examination of the Current Usefulness of the Bem Sex-Role Inventory. Psychol. Rep. 2004, 94, 1331–1336. [Google Scholar] [CrossRef] [PubMed]
- Lajunen, T. Masculinity, Femininity, and the Bem Sex Role Inventory in Turkey. Sex Roles 2005, 52, 103–110. [Google Scholar] [CrossRef]
- Peng, T.K. Construct Validation of the Bem Sex Role Inventory in Taiwan. Sex Roles 2006, 55, 843–851. [Google Scholar] [CrossRef]
- Peralta, R.; Steele, J.L.; Nofziger, S.; Rickles, M. The Impact of Gender on Binge Drinking Behavior Among U.S. College Students Attending a Midwestern University: An Analysis of Two Gender Measures. Fem. Criminol. 2010, 5, 355–379. [Google Scholar] [CrossRef]
- Reynolds, G.L.; Fisher, D.G.; Dyo, M.; Huckabay, L.M. Using the Bem and Klein Grid Scores to Predict Health Services Usage by Men. Behav. Med. 2016, 42, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Ritter, D. Gender Role Orientation and Performance on Stereotypically Feminine and Masculine Cognitive Tasks. Sex Roles 2004, 50, 583–591. [Google Scholar] [CrossRef]
- Sajatovic, M.; Micula-Gondek, W.; Tatsuoka, C.; Bialko, C. The Relationship of Gender and Gender Identity to Treatment Adherence Among Individuals With Bipolar Disorder. Gend. Med. 2011, 8, 261–268. [Google Scholar] [CrossRef] [Green Version]
- Stafford, L.; Dainton, M.; Haas, S. Measuring routine and strategic relational maintenance: Scale revision, sex versus gender roles, and the prediction of relational characteristics. Commun. Monogr. 2000, 67, 306–323. [Google Scholar] [CrossRef]
- Tardif, M.; Van Gijseghem, H. The Gender Identity of Pedophiles: What Does the Outcome Data Tell Us? J. Child Sex. Abus. 2005, 14, 57–74. [Google Scholar] [CrossRef]
- Tate, C. The “Problem of Number” Revisited: The Relative Contributions of Psychosocial, Experiential, and Evolutionary Factors to the Desired Number of Sexual Partners. Sex Roles 2010, 64, 644–657. [Google Scholar] [CrossRef]
- Vafaei, A.; Alvarado, B.; Tomás, C.; Muro, C.; Martinez, B.; Zunzunegui, M.V. The validity of the 12-item Bem Sex Role Inventory in older Spanish population: An examination of the androgyny model. Arch. Gerontol. Geriatr. 2014, 59, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Vafaei, A.; Ahmed, T.; Freire, A.D.N.F.; Zunzunegui, M.-V.; Guerra, R. Depression, Sex and Gender Roles in Older Adult Populations: The International Mobility in Aging Study (IMIAS). PLoS ONE 2016, 11, e0146867. [Google Scholar] [CrossRef] [PubMed]
- Van Well, S.; Kolk, A.M.; Arrindell, W.A. Cross-Cultural Validity of the Masculine and Feminine Gender Role Stress Scales. J. Pers. Assess. 2005, 84, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Norvilitis, J.M.; Jin, S. Measuring Gender Orientation with the Bem Sex Role Inventory in Chinese Culture. Sex Roles 2001, 44, 237–251. [Google Scholar] [CrossRef]
- Taher, N.S. Self-concept and masculinity/femininity among normal male individuals and males with gender identity disorder. Soc. Behav. Pers. Int. J. 2007, 35, 469–478. [Google Scholar] [CrossRef]
- Alavi, K.; Eftekhar, M.; Nadoushan, A.H.J. Comparison of Masculine and Feminine Gender Roles in Iranian Patients with Gender Identity Disorder. Sex. Med. 2015, 3, 261–268. [Google Scholar] [CrossRef] [Green Version]
- Park, H.Y.; Jang, Y.E.; Oh, S.; Lee, P.B. Psychological Characteristics in Patients with Chronic Complex Regional Pain Syndrome: Comparisons with Patients with Major Depressive Disorder and Other Types of Chronic Pain. J. Pain Res. 2020, ume 13, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Woo, M.; Oei, T.P.S. The MMPI-2 Gender-Masculine and Gender-Feminine scales: Gender roles as predictors of psychological health in clinical patients. Int. J. Psychol. 2006, 41, 413–422. [Google Scholar] [CrossRef]
- Woo, M.; Oei, T.P. Empirical Investigations of the MMPI-2 Gender-Masculine and Gender-Feminine Scales 1Dr Matthew Woo, Principal Psychologist, is now at the Department of Psychology, Institute of Mental Health, 10 Buangkok View, Singapore 539 747. J. Individ. Differ. 2008, 29, 1–10. [Google Scholar] [CrossRef]
- Langelier, D.M.; Cormie, P.; Bridel, W.; Grant, C.; Albinati, N.; Shank, J.; Daun, J.T.; Fung, T.S.; Davey, C.; Culos-Reed, S.N. Perceptions of masculinity and body image in men with prostate cancer: The role of exercise. Support. Care Cancer 2018, 26, 3379–3388. [Google Scholar] [CrossRef]
- Luyt, R. Masculinities Representations Inventory (MRI, English Version): A Measure of Gender (Re)Presentation. J. Men’s Stud. 2017, 26, 157–183. [Google Scholar] [CrossRef]
- Kowalczyk, R.; Skrzypulec, V.; Lew-Starowicz, Z.; Nowosielski, K.; Grabski, B.; Merk, W. Psychological gender of patients with polycystic ovary syndrome. Acta Obstet. et Gynecol. Scand. 2012, 91, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Mandal, E.; Kocur, D. Psychological Masculinity, Femininity and Tactics of Manipulation in Patients with Borderline Personality Disorder. Arch. Psychiatry Psychother. 2013, 15, 45–53. [Google Scholar]
- McCreary, D.R.; Rhodes, N.D.; Saucier, D.M. A Confirmatory Factor Analysis of the Short Form Sex Role Behavior Scale. Sex Roles 2002, 47, 169–177. [Google Scholar] [CrossRef]
- Sterner, T.R.; Gudmundsson, P.; Seidu, N.; Bäckman, K.; Skoog, I.; Falk, H. A Psychometric Evaluation of a Swedish Version of the Positive–Negative Sex-Role Inventory (PN-SRI). Societies 2018, 8, 13. [Google Scholar] [CrossRef] [Green Version]
- Hirokawa, K.; Yamada, F.; Dohi, I.; Miyata, Y. Effect of gender-types on interpersonal stress measured by blink rate and questionnaires: Focusing on stereotypically sex-typed and androgynous types. Soc. Behav. Pers. Int. J. 2001, 29, 375–384. [Google Scholar] [CrossRef]
- Ward, C.A. Models and Measurements of Psychological Androgyny: A Cross-Cultural Extension of Theory and Research. Sex Roles 2000, 43, 529–552. [Google Scholar] [CrossRef]
- Basu, J. Development of the Indian Gender Role Identity Scale. J. Indian Acad. Appl. Psychol. 2010, 36, 25–34. [Google Scholar]
- Basu, J.; Dasgupta, S.; Chakraborty, U.; Basu, S. Variants of the Indian Gender Role Identity Scale (IGRIS) for Different Age Groups in Bengali Population. J. Indian Acad. Appl. Psychol. 2012, 38, 305–310. [Google Scholar]
- Eisler, R.M.; Skidmore, J.R. Masculine Gender Role Stress: Scale Development and Component Factors in the Appraisal of Stressful Situations. Behav. Modif. 1987, 11, 123–136. [Google Scholar] [CrossRef]
- Arrindell, W.A.; Kolk, A.M.; Martín, K.; Kwee, M.; Booms, E.O.; Martín, K. Masculine Gender Role Stress: A potential predictor of phobic and obsessive–compulsive behaviour. J. Behav. Ther. Exp. Psychiatry 2003, 34, 251–267. [Google Scholar] [CrossRef] [PubMed]
- Kaźmierczak, M.; Pastwa-Wojciechowska, B.; Błażek, M. A Multidimensional Model of Empathy, and the Occurrence of Personality Disorders and Stress in Social Settings. Acta Neuropsychol. 2013, 11, 113–125. [Google Scholar]
- Mussap, A.J. Masculine Gender Role Stress and the Pursuit of Muscularity. Int. J. Men’s Health 2008, 7, 72–89. [Google Scholar] [CrossRef] [Green Version]
- Susánszky, A.; Döbrössy, B. The Correlation Between Body Mass Index and Gender Role Stress Among Young Hungarian Males. Eur. J. Ment. Health 2019, 14, 190–202. [Google Scholar] [CrossRef] [Green Version]
- Swartout, K.M.; Parrott, D.J.; Cohn, A.M.; Hagman, B.T.; Gallagher, K.E. Development of the Abbreviated Masculine Gender Role Stress Scale. Psychol. Assess. 2015, 27, 489–500. [Google Scholar] [CrossRef] [Green Version]
- Gillespie, B.L.; Eisler, R.M. Development of the Feminine Gender Role Stress Scale: A Cognitive-Behavioral Measure of Stress, Appraisal, and Coping for Women. Behav. Modif. 1992, 16, 426–438. [Google Scholar] [CrossRef]
- Richmond, K.; Levant, R.; Smalley, B.; Cook, S. The Femininity Ideology Scale (FIS): Dimensions and Its Relationship to Anxiety and Feminine Gender Role Stress. Women Health 2015, 55, 263–279. [Google Scholar] [CrossRef]
- Shea, M.; Wong, Y.J.; Wang, S.; Wang, S.; Jimenez, V.; Hickman, S.J.; LaFollette, J.R. Toward a Constructionist Perspective of Examining Femininity Experience: The Development and Psychometric Properties of the Subjective Femininity Stress Scale. Psychol. Women Q. 2013, 38, 275–291. [Google Scholar] [CrossRef]
- O’Neil, J.M.; Helms, B.J.; Gable, R.K.; David, L.; Wrightsman, L.S. Gender-role conflict scale: College men’s fear of femininity. Sex Roles 1986, 14, 335–350. [Google Scholar] [CrossRef]
- Hammer, J.H.; McDermott, R.C.; Levant, R.F.; McKelvey, D.K. Dimensionality, reliability, and validity of the Gender-Role Conflict Scale–Short Form (GRCS-SF). Psychol. Men Masculinities 2018, 19, 570–583. [Google Scholar] [CrossRef]
- Herdman, K.J.; Fuqua, D.R.; Choi, N.; Newman, J.L. Gender Role Conflict Scale: Validation for a Sample of Gay Men and Lesbian Women. Psychol. Rep. 2012, 110, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.D.; Heesacker, M. Addressing the situation: Some evidence for the significance of microcontexts with the gender role conflict construct. Psychol. Men Masculinities 2012, 13, 294–307. [Google Scholar] [CrossRef]
- Komlenac, N.; Siller, H.; Bliem, H.R.; Hochleitner, M. Validation of the Internal Structure of a German-Language Version of the Gender Role Conflict Scale – Short Form. Front. Psychol. 2018, 9, 1161. [Google Scholar] [CrossRef]
- Lease, S.H.; Çiftçi, A.; Demir, A.; Boyraz, G. Structural validity of Turkish versions of the Gender Role Conflict Scale and Male Role Norms Scale. Psychol. Men Masculinities 2009, 10, 273–287. [Google Scholar] [CrossRef]
- Moradi, B.; Tokar, D.M.; Schaub, M.; Jome, L.M.; Serna, G.S. Revisiting the structural validity of the Gender Role Conflict Scale. Psychol. Men Masculinities 2000, 1, 62–69. [Google Scholar] [CrossRef]
- Norwalk, K.E.; Vandiver, B.J.; White, A.M.; Englar-Carlson, M. Factor structure of the gender role conflict scale in African American and European American men. Psychol. Men Masculinities 2011, 12, 128–143. [Google Scholar] [CrossRef]
- Wester, S.R.; Vogel, D.L.; O’Neil, J.M.; Danforth, L. Development and evaluation of the Gender Role Conflict Scale Short Form (GRCS-SF). Psychol. Men Masculinities 2012, 13, 199–210. [Google Scholar] [CrossRef]
- Zhang, C.; Blashill, A.J.; Wester, S.R.; O’Neil, J.M.; Vogel, D.L.; Wei, J.; Zhang, J. Factor structure of the Gender Role Conflict Scale-Short Form in Chinese heterosexual and gay samples. Psychol. Men Masculinities 2015, 16, 229–233. [Google Scholar] [CrossRef] [Green Version]
- Mincey, K.; Alfonso, M.; Hackney, A.; Luque, J. Being a Black Man: Development of the Masculinity Inventory Scale (MIS) for Black Men. J. Men’s Stud. 2014, 22, 167–179. [Google Scholar] [CrossRef]
- Brown, D.L.; Blackmon, S.; Rosnick, C.B.; Griffin-Fennell, F.D.; White-Johnson, R.L. Initial Development of a Gendered-Racial Socialization Scale for African American College Women. Sex Roles 2016, 77, 178–193. [Google Scholar] [CrossRef]
- Clark, J.A.; Inui, T.S.; Silliman, R.A.; Bokhour, B.G.; Krasnow, S.H.; Robinson, R.A.; Spaulding, M.; Talcott, J.A. Patients’ Perceptions of Quality of Life After Treatment for Early Prostate Cancer. J. Clin. Oncol. 2003, 21, 3777–3784. [Google Scholar] [CrossRef] [PubMed]
- Kozee, H.B.; Tylka, T.L.; Bauerband, L. Measuring Transgender Individuals’ Comfort With Gender Identity and Appearance. Psychol. Women Q. 2012, 36, 179–196. [Google Scholar] [CrossRef]
- Barr, S.M.; Budge, S.L.; Adelson, J.L. Transgender community belongingness as a mediator between strength of transgender identity and well-being. J. Couns. Psychol. 2016, 63, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Egan, S.K.; Perry, D.G. Gender identity: A multidimensional analysis with implications for psychosocial adjustment. Dev. Psychol. 2001, 37, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Reisen, C.A.; Brooks, K.D.; Zea, M.C.; Poppen, P.J.; Bianchi, F.T. Can additive measures add to an intersectional understanding? Experiences of gay and ethnic discrimination among HIV-positive Latino gay men. Cult. Divers. Ethn. Minor. Psychol. 2013, 19, 208–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Docter, R.F.; Fleming, J.S. Measures of transgender behavior. Arch. Sex. Behav. 2001, 30, 255–271. [Google Scholar] [CrossRef] [PubMed]
- Storms, M.D. Sex role identity and its relationships to sex role attributes and sex role stereotypes. J. Pers. Soc. Psychol. 1979, 37, 1779–1789. [Google Scholar] [CrossRef]
- Bejerot, S.; Eriksson, J. Sexuality and Gender Role in Autism Spectrum Disorder: A Case Control Study. PLoS ONE 2014, 9, e87961. [Google Scholar] [CrossRef]
- Wade, J.C.; Gelso, C.J. Reference Group Identity Dependence Scale. Couns. Psychol. 1998, 26, 384–412. [Google Scholar] [CrossRef]
- Cicero, E.C.; Reisner, S.L.; Merwin, E.I.; Humphreys, J.C.; Silva, S.G. Application of Behavioral Risk Factor Surveillance System Sampling Weights to Transgender Health Measurement. Nurs. Res. 2020, 69, 307–315. [Google Scholar] [CrossRef]
- Bauerband, L.A.; Teti, M.; Velicer, W.F. Measuring minority stress: Invariance of a discrimination and vigilance scale across transgender and cisgender LGBQ individuals. Psychol. Sex. 2018, 10, 17–30. [Google Scholar] [CrossRef]
- Bazzi, A.R.; Whorms, D.S.; King, D.S.; Potter, J. Adherence to Mammography Screening Guidelines Among Transgender Persons and Sexual Minority Women. Am. J. Public Health 2015, 105, 2356–2358. [Google Scholar] [CrossRef] [PubMed]
- Christian, R.; Mellies, A.A.; Bui, A.G.; Lee, R.; Kattari, L.; Gray, C. Measuring the Health of an Invisible Population: Lessons from the Colorado Transgender Health Survey. J. Gen. Intern. Med. 2018, 33, 1654–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraser, G.; Bulbulia, J.; Greaves, L.M.; Wilson, M.S.; Sibley, C.G. Coding Responses to an Open-ended Gender Measure in a New Zealand National Sample. J. Sex Res. 2019, 57, 979–986. [Google Scholar] [CrossRef]
- Ewalds-Kvist, S.B.M.; Rantala, M.; Nikkanen, V.; Selander, R.K.; Lertola, K. The response of the Finnish man to vasectomy. Psychol. Health Med. 2003, 8, 355–369. [Google Scholar] [CrossRef]
- Tanner, J. Current advances in the study of physique: Photogrammetric anthropometry and an androgyny scale. Lancet 1951, 257, 574–579. [Google Scholar] [CrossRef]
- Dubey, A. Importance of androgyny score in differentiation between sexes and as a diagnostic tool in schizophrenic females. J. Evol. Med Dent. Sci. 2015, 4, 1765–1768. [Google Scholar] [CrossRef]
- Mishra, V.; Sharma, S.; Kulsreshtha, V.; Kumar, V.; Singh, D. Anthropometric Study Revealed: Androgyny Score as an Important Tool in Early Diagnosis of Schizophrenia. J. Anat. Soc. India 2011, 60, 207–209. [Google Scholar] [CrossRef]
- Smith, Y.L.; van Goozen, S.H.; Kuiper, A.; Cohen-Kettenis, P.T. Transsexual subtypes: Clinical and theoretical significance. Psychiatry Res. 2005, 137, 151–160. [Google Scholar] [CrossRef]
- Suppakitjanusant, P.; Ji, Y.; Stevenson, M.O.; Chantrapanichkul, P.; Sineath, R.C.; Goodman, M.; Alvarez, J.A.; Tangpricha, V. Effects of gender affirming hormone therapy on body mass index in transgender individuals: A longitudinal cohort study. J. Clin. Transl. Endocrinol. 2020, 21, 100230. [Google Scholar] [CrossRef]
- Lacasse, A.; Pagé, M.G.; Choinière, M.; Dorais, M.; Vissandjée, B.; Nguefack, H.L.N.; Katz, J.; Samb, O.M.; Vanasse, A. Conducting gender-based analysis of existing databases when self-reported gender data are unavailable: The GENDER Index in a working population. Can. J. Public Health 2020, 111, 155–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | % | |
|---|---|---|---|
| Country of corresponding author † | USA | 34 | 53.1 |
| Canada | 9 | 14.1 | |
| Australia | 3 | 4.7 | |
| Germany | 3 | 4.7 | |
| Netherlands | 3 | 4.7 | |
| Austria | 2 | 3.1 | |
| United Kingdom | 2 | 3.1 | |
| Finland | 1 | 1.6 | |
| India | 1 | 1.6 | |
| Italy | 1 | 1.6 | |
| Japan | 1 | 1.6 | |
| New Zealand | 1 | 1.6 | |
| Poland | 1 | 1.6 | |
| Sweden | 1 | 1.6 | |
| Switzerland | 1 | 1.6 | |
| Not specified | 13 | ||
| Discipline of corresponding author † | Psychology | 38 | 61.3 |
| Public health | 9 | 14.5 | |
| Medicine | 8 | 12.9 | |
| Sociology | 2 | 3.2 | |
| Interdisciplinary network | 2 | 3.2 | |
| Communication science | 1 | 1.6 | |
| Neuroscience | 1 | 1.6 | |
| Nursing | 1 | 1.6 | |
| Not specified | 15 | ||
| Characteristics of study population of instrument development |
Students General population |
17 13 |
28.3 21.7 |
| Trans* people | 10 | 16.7 | |
| Patients with certain mental or physical health conditions (and controls) | 8 | 13. | |
| Women only | 6 | 10.0 | |
| Men only | 3 | 5. | |
| Young adult | 2 | 3.3 | |
| Children | 1 | 1.7 | |
| Not specified | 17 | ||
| Country of study population of instrument development | USA | 34 | 55.7 |
| Canada | 6 | 9.8 | |
| Several countries | 5 | 8.2 | |
| United Kingdom | 3 | 4.9 | |
| Netherlands | 3 | 4.9 | |
| Australia | 2 | 3.3 | |
| Finland | 1 | 1.6 | |
| Germany | 1 | 1.6 | |
| India | 1 | 1.6 | |
| Italy | 1 | 1.6 | |
| Japan | 1 | 1.6 | |
| Singapore | 1 | 1.6 | |
| Sweden | 1 | 1.6 | |
| Switzerland | 1 | 1.6 | |
| Not specified | 16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horstmann, S.; Schmechel, C.; Palm, K.; Oertelt-Prigione, S.; Bolte, G. The Operationalisation of Sex and Gender in Quantitative Health–Related Research: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 7493. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127493
Horstmann S, Schmechel C, Palm K, Oertelt-Prigione S, Bolte G. The Operationalisation of Sex and Gender in Quantitative Health–Related Research: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(12):7493. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127493
Chicago/Turabian StyleHorstmann, Sophie, Corinna Schmechel, Kerstin Palm, Sabine Oertelt-Prigione, and Gabriele Bolte. 2022. "The Operationalisation of Sex and Gender in Quantitative Health–Related Research: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 12: 7493. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127493