
Appraising Evidence-Based Mental Health and Psychosocial Support (MHPSS) Guidelines—PART II: A Content Analysis with Implications for Disaster Risk Reduction


Abstract
:1. Introduction
1.1. Challenges in Integrating MHPSS with DRR Programming
- The material points at a lack of “consensus or overarching framework”. No “definition or consensus-based model for discussing MHPSS components of DRR” could be identified. MHPSS and DRR are typically discussed in isolation, without combined narrative (likewise for the findings of a literature review exploring the cross-section of MHPSS principles and crisis management [10]).
- There is limited consensus or understanding of “what activities constitute the integration of MHPSS and DRR”. Similarly, there is no clear consensus on “MHPSS placement in DRR policy or guidance on best practices for working with various stakeholders to integrate MHPSS with existing DRR programming”.
- Evidence-based or consensus-driven definitions and guidelines for integrating MHPSS into DRR programming are necessary for an effective widespread implementation [20].
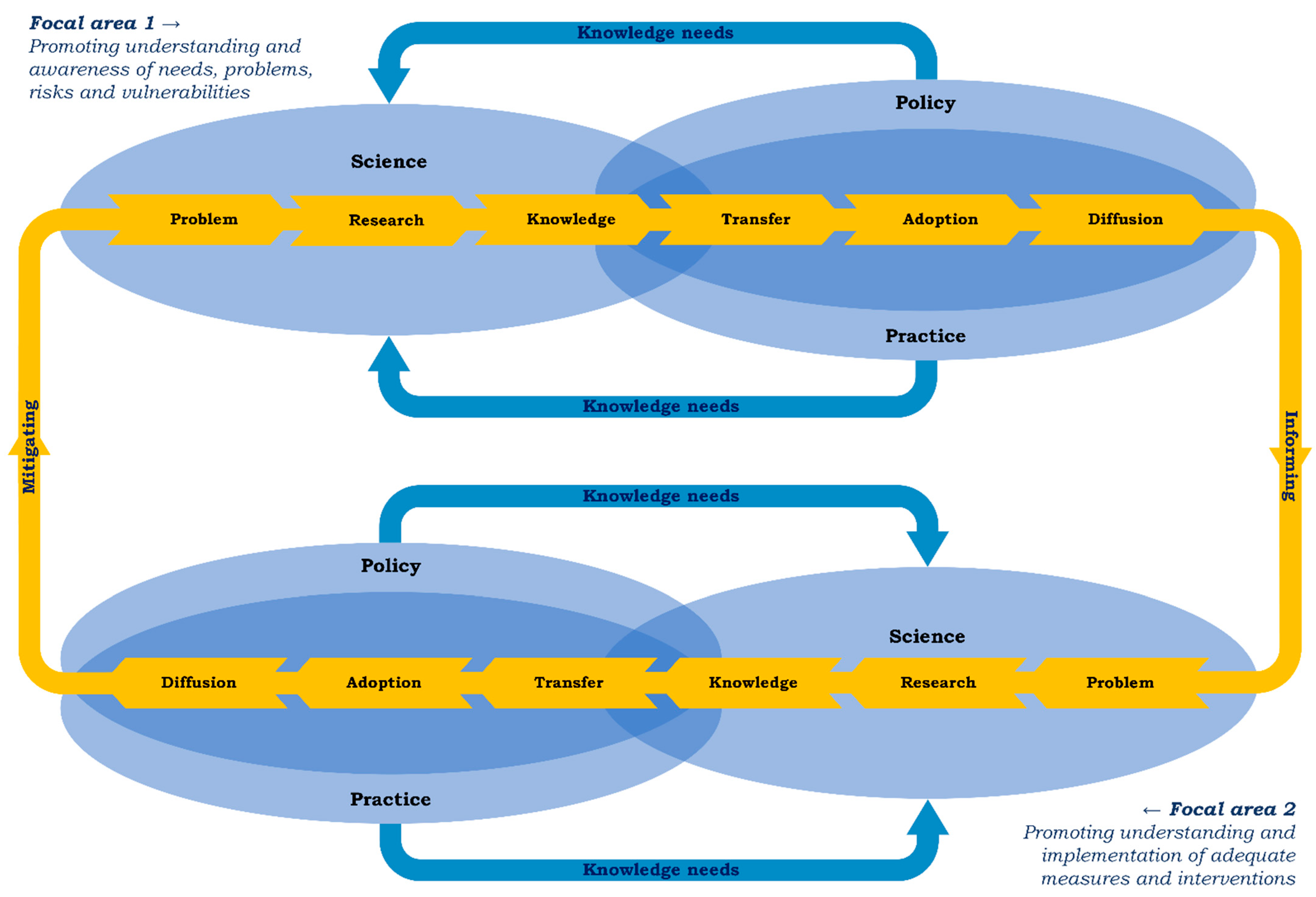
1.2. MHPSS Knowledge Development and Uptake on Behalf of Disaster Risk Reduction
1.2.1. Disaster Risk Reduction: Two Focal Areas
1.2.2. Zooming in on the Second Focal Area: MHPSS Knowledge Captured in Guidelines
1.3. Study Focus
2. Materials and Methods
2.1. Selection of Guidelines
- Inter-Agency Standing Committee (IASC guidelines; 2007; 63.6) [18].
- Dutch multi-disciplinary guidelines (Dutch or Impact guidelines; 2014; 67.6) [45].
- Operationalising Psychosocial Support in Crises (OPSIC guidelines; 2016; 56.8) [38].
- International Committee of the Red Cross (Red Cross guidelines; 2018; 60.8) [46].
2.2. Data Extraction
2.3. Analysis
3. Results
3.1. Characteristics of the Guidelines
3.1.1. Context
3.1.2. Definitions, Purpose, User Groups, and Target Groups
3.2. Nature of the Guidance
3.2.1. Emphasis in Terminology
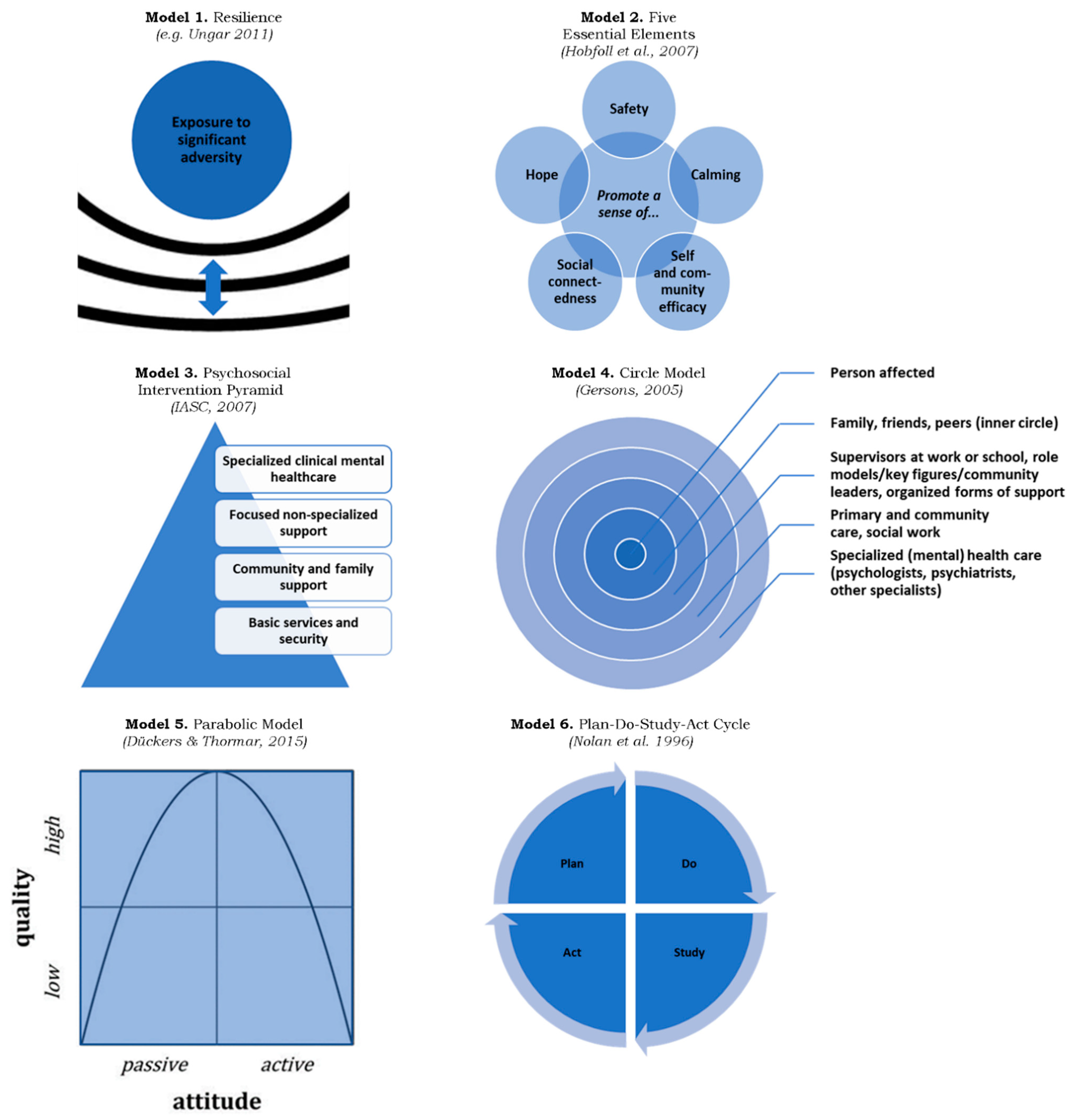
3.2.2. Models

3.2.3. Measures and Interventions
3.2.4. Monitoring and Evaluation
3.2.5. Implementation and Preparedness
3.3. Conditions for Implementation and Preparedness
4. Discussion
4.1. Main Findings
4.1.1. Characteristics of the Guidelines
4.1.2. Nature of the Guidance: The Common Ground in the MHPSS Knowledge Base
4.1.3. Conditions for Implementation and Preparedness
4.2. Implications for Disaster Risk Reduction
4.2.1. Using the Guidance to Overcome Integration Challenges
4.2.2. Cross-Level Integration: Translating Universal Guidance to Specific Contexts
4.2.3. Closing the Cycle: Disaster Risk Reduction through Learning
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Focal area 1 | Veerkracht (17) Zelfredzaamheid (18) |
| Kwetsbaar/Kwetsbaarheid/Kwetsbaarheden/Kwetsbare (11) | |
| Risico/Risico’s (17) Risicofactoren (30) | |
| Behoeften (66) | |
| Probleem/Problemen (84) | |
| Stoornis/Stoornissen (13) | |
| Trauma/Traumatisch (21) | |
| PTSS (14) | |
| Focal area 2 | Preventie/Preventief/Preventieve (17) |
| [no translation for Assessment/Assessments] (-) | |
| Behoeftepeilingen (1) | |
| Screening (10) Screeningonderzoek (1) | |
| Monitor/Monitoring (3) | |
| Evaluatie/Evaluaties (28) | |
| Monitoring and evaluatie (0) | |
| Coördinatie/Coördinatietaak/Coördinatietaken (4) | |
| Preparatie (9) Voorbereiden/Voorbereiding (20) | |
| Implementatie (12) | |
| Training (3) | |
| Middelen (7) | |
| Condities (1) Randvoorwaarden (4) | |
| Focal areas 1 and 2 | Omstandigheden (11) |
| Context (25) | |
| Fase/Fasen (66) | |
| Cultuurspecifiek/Cultuurspecifieke (4) | |
| Ethiek/Ethisch (0) | |
| (Mensen)rechten (0) |
References
- Bonde, J.P.; Utzon-Frank, N.; Bertelsen, M.; Borritz, M.; Eller, N.H.; Nordentoft, M.; Olesen, K.; Rod, N.H.; Rugulies, R. Risk of Depressive Disorder following Disasters and Military Deployment: Systematic Review with Meta-Analysis. Br. J. Psychiatry 2016, 208, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Brewin, C.R.; Kaniasty, K.; Greca, A.M.L. Weighing the Costs of Disaster: Consequences, Risks, and Resilience in Individuals, Families, and Communities. Psychol. Sci. Public Interest 2010, 11, 1–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazel, M.; Reed, R.V.; Panter-Brick, C.; Stein, A. Mental Health of Displaced and Refugee Children Resettled in High-Income Countries: Risk and Protective Factors. Lancet 2012, 379, 266–282. [Google Scholar] [CrossRef]
- Galea, S.; Nandi, A.; Vlahov, D. The Epidemiology of Post-Traumatic Stress Disorder after Disasters. Epidemiol. Rev. 2005, 27, 78–91. [Google Scholar] [PubMed] [Green Version]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniast, K. 60,000 Disaster Victims Speak: Part I. An Empirical Review of the Empirical Literature, 1981–2001. Psychiatry 2002, 65, 207–239. [Google Scholar] [CrossRef] [Green Version]
- Ripoll Gallardo, A.; Pacelli, B.; Alesina, M.; Serrone, D.; Iacutone, G.; Faggiano, F.; Della Corte, F.; Allara, E. Medium- and Long-Term Health Effects of Earthquakes in High-Income Countries: A Systematic Review and Meta-Analysis. Int. J. Epidemiol. 2018, 47, 1317–1332. [Google Scholar] [CrossRef] [Green Version]
- Safarpour, H.; Sohrabizadeh, S.; Malekyan, L.; Safi-Keykaleh, M.; Pirani, D.U.; Daliri, S.; Bazyar, J. Suicide Death Rate after Disasters: A Meta-Analysis Study. Arch. Suicide Res. 2020, 26, 14–27. [Google Scholar] [CrossRef]
- Lowell, A.; Suarez-Jimenez, B.; Helpman, L.; Zhu, X.; Durosky, A.; Hilburn, A.; Schneier, F.; Gross, R.; Neria, Y. 9/11-Related PTSD among Highly Exposed Populations: A Systematic Review 15 Years after the Attack. Psychol. Med. 2018, 4, 537–553. [Google Scholar] [CrossRef] [Green Version]
- Reifels, L.; Pietrantoni, L.; Prati, G.; Kim, Y.; Kilpatrick, D.G.; Dyb, G.; Halpern, J.; Olff, M.; Brewin, C.R.; O’donnell, M. Lessons Learned about Psychosocial Responses to Disaster and Mass Trauma: An International Perspective. Eur. J. Psychotraumatol. 2013, 4, 22897. [Google Scholar] [CrossRef]
- Dückers, M.L.A.; Yzermans, C.J.; Jong, W.; Boin, A. Psychosocial Crisis Management: The Unexplored Intersection of Crisis Leadership and Psychosocial Support. Risk Hazards Crisis Public Policy 2017, 8, 94–112. [Google Scholar] [CrossRef] [Green Version]
- Dickson, K.; Bangpan, M. What are the Barriers to, and Facilitators of, Implementing and Receiving MHPSS Programmes Delivered to Populations Affected by Humanitarian Emergencies? A Qualitative Evidence Synthesis. Glob. Ment. Health 2018, 5, e21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dückers, M.L.A.; Thormar, S.B.; Juen, B.; Ajdukovic, D.; Newlove-Eriksson, L.; Olff, M. Measuring and Modelling the Quality of 40 Post-Disaster Mental Health and Psychosocial Support Programmes. PLoS ONE 2018, 13, e0193285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, J.; Oosterbeek, M.; Tummers, L.G.; Noordegraaf, M.; Yzermans, C.J.; Dückers, M.L. The Organization of Post-Disaster Psychosocial Support in The Netherlands: A Meta-Synthesis. Eur. J. Psychotraumatol. 2019, 10, 1544024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seto, M.; Nemoto, H.; Kobayashi, N.; Kikuchi, S.; Honda, N.; Kim, Y.; Kelman, I.; Tomita, H. Post-disaster Mental Health and Psychosocial Support in the Areas Affected by the Great East Japan Earthquake: A Qualitative Study. BMC Psychiatry 2019, 19, 261. [Google Scholar] [CrossRef] [Green Version]
- Cénat, J.M.; Mukunzi, J.N.; Noorishad, P.G.; Rousseau, C.; Derivois, D.; Bukaka, J. A Systematic Review of Mental Health Programs among Populations Affected by the Ebola Virus Disease. J. Psychosom. Res. 2020, 131, 109966. [Google Scholar] [CrossRef]
- Leppold, C.; Gibbs, L.; Block, K.; Reifels, L.; Quinn, P. Public Health Implications of Multiple Disaster Exposures. Lancet Public Health 2022, 7, e274–e286. [Google Scholar] [CrossRef]
- Stene, L.E.; Vuillermoz, C.; Van Overmeire, R.; Bilsen, J.; Dückers, M.L.A.; Govasli Nilsen, L.; Vandentorren, S. Psychosocial Care Responses to Terrorist Attacks: A Country Case Study of Norway, France and Belgium. BMC Health Serv. Res. 2022, 22, 390. [Google Scholar] [CrossRef]
- Inter-Agency Standing Committee (IASC). IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings; IASC: Geneva, Switzerland, 2007. [Google Scholar]
- Galappatti, A.; Richardson, S. Linking Mental Health and Psychosocial Support and Disaster Risk Reduction: Applying a WellBeing Lens to Disaster Risk Reduction. Intervention 2016, 14, 223–231. [Google Scholar] [CrossRef] [Green Version]
- Gray, B.; Hanna, F.; Reifels, L. The Integration of Mental Health and Psychosocial Support and Disaster Risk Reduction: A Mapping and Review. Int. J. Environ. Res. Public. Health 2020, 17, 1900. [Google Scholar] [CrossRef] [Green Version]
- United Nations Office for Disaster Risk Reduction (UNDRR). Disaster Risk Reduction. Available online: https://www.undrr.org/terminology/disaster-risk-reduction (accessed on 4 May 2022).
- Généreux, M.; Lafontaine, M.; Eykelbosh, A. From Science to Policy and Practice: A Critical Assessment of Knowledge Management before, during, and after Environmental Public Health Disasters. Int. J. Environ. Res. Public Health 2019, 16, 587. [Google Scholar] [CrossRef] [Green Version]
- Norris, F.H. (Ed.) Methods for Disaster Mental Health Research; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Wong, D.F.; Spencer, C.; Boyd, L.; Burkle, F.M.; Archer, F. Disaster Metrics: A Comprehensive Framework for Disaster Evaluation Typologies. Prehosp. Disaster Med. 2017, 32, 501–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korteweg, H.A.; van Bokhoven, I.; Yzermans, C.J.; Grievink, L. Rapid Health and Needs Assessments after Disasters: A Systematic Review. BMC Public Health 2010, 10, 295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosmans, M.W.G.; Baliatsas, C.; Yzermans, C.J.; Dückers, M.L.A. A Systematic Review of Rapid Needs Assessments and Their Usefulness for Disaster Decision Making: Methods, Strengths and Weaknesses and Value for Disaster Relief Policy. Int. J. Disaster Risk Reduct. 2022, 71, 102807. [Google Scholar] [CrossRef]
- Jeleff, M.; Lehner, L.; Giles-Vernick, T.; Dückers, M.L.A.; Napier, A.D.; Jirovsky-Platter, E.; Kutalek, R. Vulnerability and One Health Assessment Approaches for Infectious Threats from a Social Science Perspective: A Systematic Scoping Review. Lancet Planet. Health, 2022; in press. [Google Scholar]
- Van der Ven, L.G.L.; Duinhof, E.L.; Dückers, M.L.A.; Jambroes, M.; Van Bon-Martens, M.J.H. Conceptualizing Vulnerability for Health Effects of the COVID-19 Pandemic and the Associated Measures in Utrecht and Zeist: A Concept Map. Int. J. Environ. Res. Public Health 2021, 18, 2163. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Guidance on Research Methods for Health Emergency and Disaster Risk Management; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Osborne, J.; Paget, J.; Giles-Vernick, T.; Kutalek, R.; Napier, D.; Baliatsas, C.; Dückers, M.L.A. Community Engagement and Vulnerability in Infectious Diseases: A Systematic Review and Qualitative Analysis of the Literature. Soc. Sci. Med. 2021, 284, 114246. [Google Scholar] [CrossRef]
- UNICEF; Obregon, R.; Elessawi, R.; Chitnis, K.; Bedsen, J.; Abramowitz, S. Minimum Quality Standards and Indicators for Community Engagement; UNICEF C4D: New York, NY, USA, 2020. [Google Scholar]
- Wessells, M.; van Ommeren, M. Developing Inter-Agency Guidelines on Mental Health and Psychosocial Support in Emergency Settings. Intervention 2008, 6, 199–218. [Google Scholar] [CrossRef] [Green Version]
- Williams, R.; Mikus Kos, A.; Ajdukovic, D.; van der Veer, G.; Feldman, M. Recommendations on Evaluating Community Based Psychosocial Programmes. Intervention 2008, 6, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Te Brake, H.; Dückers, M.L.A.; De Vries, M.; Van Duin, D.; Rooze, M.; Spreeuwenberg, C. Early Psychosocial Interventions after Disasters, Terrorism, and Other Shocking Events: Guideline Development. Nurs. Health Sci. 2009, 11, 336–343. [Google Scholar] [CrossRef]
- Bisson, J.I.; Tavakoly, B.; Witteveen, A.B.; Ajdukovic, D.; Jehel, L.; Johansen, V.J.; Nordanger, D.; Garcia, F.O.; Punamaki, R.-L.; Schnyder, U.; et al. TENTS Guidelines: Development of Post-Disaster Psychosocial Care Guidelines through a Delphi Process. Br. J. Psychiatry 2010, 196, 69–74. [Google Scholar] [CrossRef]
- Suzuki, Y.; Fukasawa, M.; Nakajima, S.; Narisawa, T.; Kim, Y. Development of Disaster Mental Health Guidelines through the Delphi Process in Japan. Int. J. Ment. Health Syst. 2012, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Te Brake, H.; Dückers, M.L.A. Early Psychosocial Interventions after Disasters, Terrorism and Other Shocking Events: Is There a Gap between Norms and Practice in Europe? Eur. J. Psychotraumatol. 2013, 4, 19093. [Google Scholar] [CrossRef] [PubMed]
- Juen, B.; Warger, R.; Nindl, S.; Siller, H.; Lindenthal, M.J.; Huttner, E.; Thormar, S. The Comprehensive Guideline on Mental Health and Psychosocial Support (MHPSS) in Disaster Settings; OPSIC: Innsbruck, Austria, 2016. [Google Scholar]
- Lee, S.M.; Lee, H.Y.; Lee, M.K.; Kim, S.; Lee, S.; Lee, H.-W.; Park, E.J.; Sim, M.; Paik, J.-W. Development of Korean Disaster Mental Health Support Guidelines: Results of a Scoping Review and a Delphi Survey. Psychiatry Investig. 2019, 16, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Te Brake, H.; Willems, A.; Steen, C.; Dückers, M.L.A. Appraising Evidence-Based Mental Health and Psychosocial Support (MHPSS) Guidelines—PART I: A Systematic Review on Methodological Quality Using AGREE-HS. Int. J. Environ. Res. Public Health 2022, 19, 3107. [Google Scholar] [CrossRef]
- Reliefweb about ReliefWeb. Available online: https://reliefweb.int/about (accessed on 28 September 2021).
- The MHPSS Network What We, Do. Available online: https://www.mhpss.net (accessed on 28 September 2021).
- AGREE Collaboration AGREE Enterprise Website. Available online: https://www.agreetrust.org/resource-centre/agree-ii/ (accessed on 28 September 2021).
- AGREE-HS Research Team. AGREE-Health Systems (AGREE-HS) Reporting Checklist. Available online: http://www.agreetrust.org (accessed on 28 September 2021).
- Werkgroep Multidisciplinaire Richtlijnontwikkeling Psychosociale Hulp bij Rampen en Crises. Multidisciplinaire Richtlijn Psychosociale Hulp bij Rampen en Crises [Multidiscplinary Guidelines for Psychosocial Aid during Disasters and Crises]; Impact: Diemen, The Netherlands, 2014. [Google Scholar]
- International Committee of the Red Cross (ICRC). Guidelines on Mental Health and Psychosocial Support; ICRC: Geneva, Switzerland, 2018. [Google Scholar]
- Dückers, M.L.A.; Thormar, S.B. Post-Disaster Psychosocial Support and Quality Improvement: A Conceptual Framework for Understanding and Improving the Quality of Psychosocial Support Programs. Nurs. Health Sci. 2015, 17, 159–165. [Google Scholar] [CrossRef]
- Inter-Agency Standing Committee (IASC) Reference Group for Mental Health and Psychosocial Support in Emergency Settings. A Common Monitoring and Evaluation Framework for Mental Health and Psychosocial Support in Emergency Settings; IASC: Geneva, Switzerland, 2017. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- United Nations Office for Disaster Risk Reduction (UNDRR) Resilience. Available online: https://www.undrr.org/terminology/resilience (accessed on 4 May 2022).
- Ungar, M. Counseling in Challenging Contexts: Working with Individuals and Families across Clinical and Community Settings; Brooks/Cole: Belmont, CA, USA, 2011. [Google Scholar]
- Hobfoll, S.E.; Watson, P.; Bell, C.C.; Bryant, R.A.; Brymer, M.J.; Friedman, M.J.; Friedman, M.; Gersons, B.P.; De Jong, J.T.; Layne, C.; et al. Five Essential Elements of Immediate and Mid–Term Mass Trauma Intervention: Empirical Evidence. Psychiatry 2007, 70, 283–315. [Google Scholar] [CrossRef]
- West, J.C.; Morganstein, J.C.; Benedek, D.M. Fourteen Years Later: Hobfoll and Colleagues Five Principles of Psychological First Aid through the Lens of the COVID-19 Global Pandemic. Psychiatry 2021, 84, 373–377. [Google Scholar] [CrossRef]
- Bryant, R.A. The Relevance of the Five Elements of Resilience during the COVID-19 Pandemic. Psychiatry 2021, 84, 351–357. [Google Scholar] [CrossRef]
- Gersons, B.P.R. Bijzondere Missie: Geestelijke Gezondheidszorg voor Militairen en Veteranen [Special Mission: Mental Health Care for Military Staff and Veterans]; Ministerie van Defensie: Den Haag, The Netherlands, 2005. [Google Scholar]
- Langley, G.L.; Nolan, K.M.; Nolan, T.W.; Norman, C.L.; Provost, L.P. The Improvement Guide: A Practical Approach to Enhancing Organisational Performance; Jossey-Bass Publishers: San Francisco, CA, USA, 1996. [Google Scholar]
- Berwick, D.M. Developing and Testing Changes in Delivery of Care. Ann. Intern. Med. 1998, 128, 651–656. [Google Scholar] [CrossRef]
- Taylor, M.J.; McNicholas, C.; Nicolay, C.; Darzi, A.; Bell, D.; Reed, J.E. Systematic Review of the Application of the Plan–Do–Study–Act Method to Improve Quality in Healthcare. BMJ Qual. Saf. 2014, 23, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Rose, S.; Bisson, J.; Churchill, R.; Wessely, S. Psychological Debriefing for Preventing Post Traumatic Stress Disorder (PTSD). Cochrane Libr. 2007, 2, CD000560. [Google Scholar] [CrossRef] [PubMed]
- Tamrakar, T.; Murphy, J.; Elklit, A. Was Psychological Debriefing Dismissed Too Quickly? An Assessment of the 2002 Cochrane Review. Crisis Stress Human Resil. 2019, 1, 146–155. [Google Scholar]
- Michie, S.; van Stralen, M.M.; West, R. The Behaviour Change Wheel: A New Method for Characterising and Designing Behaviour Change Interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Herpen, M.M.; Dückers, M.L.A.; Schaap, R.; Olff, M.; Te Brake, H. Online One-Stop Shop for Disaster Response Services after the MH17 Airplane Crash: An Evaluation Study. Front. Publ. Health 2022, 10, 832840. [Google Scholar] [CrossRef]
- Dückers, M.; Bosmans, M.; de Zwart, F. COVID-19: De Psychosociale Impact van een Crisis in Slow Motion [COVID-19: The Psychosocial Impact of a Crisis in Slow Motion]; Boom Bestuurskunde: Den Haag, The Netherlands, 2021. [Google Scholar]
- IASC Reference Groups MHPSS. IASC Guidance on Operational Considerations for Multisectoral Mental Health and Psychosocial Support Programmes during the COVID-19 Pandemic; IASC: Geneva, Switzerland, 2020; Available online: https://interagencystandingcommittee.org/iasc-reference-group-mental-health-and-psychosocial-support-emergency-settings/iasc-guidance-operational-considerations-multisectoral-mental-health-and-psychosocial-support (accessed on 6 May 2022)(In Multiple Languages).
- Kola, L.; Kohrt, B.A.; Hanlon, C.; Naslund, J.A.; Sikander, S.; Balaji, M.; Benjet, C.; Cheung, E.Y.L.; Eaton, J.; Gonsalves, P.; et al. COVID-19 Mental Health Impact and Responses in Low-Income and Middle-Income Countries: Reimagining Global Mental Health. Lancet Psychiatry 2021, 8, 535–550. [Google Scholar] [CrossRef]
- Stuijfzand, S.; Deforges, C.; Sandoz, V.; Sajin, C.T.; Jaques, C.; Elmers, J.; Horsch, A. Psychological Impact of an Epidemic/Pandemic on the Mental Health of Healthcare Professionals: A Rapid Review. BMC Public Health 2020, 20, 1230. [Google Scholar] [CrossRef]
- Dückers, M. Capturing Intervention in Its Context: The Next Frontier in Disaster Response Evaluation and Scale-Up Planning. Intervention 2021, 19, 4. [Google Scholar] [CrossRef]
- Ruscio, A.M.; Hallion, L.S.; Lim, C.C.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Andrade, L.H.; Borges, G.; Bromet, E.J.; Bunting, B.; et al. Cross-Sectional Comparison of the Epidemiology of DSM-5 Generalized Anxiety Disorder across the Globe. JAMA Psychiatry 2017, 74, 465–475. [Google Scholar] [CrossRef] [Green Version]
- Dückers, M.L.A.; Reifels, L.; De Beurs, D.P.; Brewin, C.R. The Vulnerability Paradox in Global Mental Health and Its Applicability to Suicide. Br. J. Psychiatry 2019, 215, 588–593. [Google Scholar] [CrossRef] [Green Version]
- Enticott, J.; Dawadi, S.; Shawyer, F.; Inder, B.; Fossey, E.; Teede, H.; Rosenberg, S.; Ozols, I.; Meadows, G. Mental Health in Australia: Psychological Distress Reported in Six Consecutive Cross-Sectional National Surveys from 2001 to 2018. Front. Psychiatry 2022, 13, 815904. [Google Scholar] [CrossRef] [PubMed]
- Burri, A.; Maercker, A. Differences in Prevalence Rates of PTSD in Various European Countries Explained by War Exposure, Other Trauma and Cultural Value Orientation. BMC Res. Notes 2014, 7, 407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dückers, M.L.A.; Alisic, E.; Brewin, C.R. A Vulnerability Paradox in the Cross-National Prevalence of Post-Traumatic Stress Disorder. Br. J. Psychiatry 2016, 209, 300–305. [Google Scholar] [CrossRef]
- Haroz, E.E.; Nguyen, A.J.; Lee, C.I.; Tol, W.A.; Fine, S.L.; Bolton, P. What Works in Psychosocial Programming in Hu-manitarian Contexts in Low-and Middle-Income Countries: A Systematic Review of the Evidence. Intervention 2020, 18, 3. [Google Scholar]
- Nemiro, A.; Jones, T.; Tulloch, O.; Snider, L. Advancing and Translating Knowledge: A Systematic Inquiry into the 2010–2020 Mental Health and Psychosocial Support Intervention Research Evidence Base. Glob. Ment. Health 2022, 1–13. [Google Scholar] [CrossRef]

| Guidelines | MHPSS Definition | Purpose | User Groups | Target Groups |
|---|---|---|---|---|
| IASC, 2007 | A composite term to describe any type of local or outside support that aims to protect or promote psychosocial well-being and/or prevent or treat mental disorder. | Enable humanitarian actors and communities to plan, establish, and coordinate a set of minimum multi-sectoral responses to protect and improve people’s mental health and psychosocial well-being in the midst of an emergency. Additionally, list concrete strategies for mental health and psychosocial support to be considered, mainly before and after the acute emergency phase. | Humanitarian actors including community-based organizations, government authorities, United Nations organizations, NGOs, and donors operating in emergency settings at the local, national, and international levels. | Young children and care givers; people with severe physical, neurological, or mental disabilities or disorders; women (e.g., pregnant women, (single) mothers, widows, and, in some cultures, unmarried adult women and teenage girls); men (e.g., ex-combatants, young men at risk of detention, abduction, or being targets of violence); people exposed to extremely stressful events/trauma; people experiencing severe social stigma; people at specific risk of human rights violations (e.g., political activists, ethnic or linguistic minorities); helpers and staff; refugees; internally displaced persons; migrants in irregular situations; elderly; people in institutions (e.g., orphans, elderly, people with neurological/mental disabilities or disorders); extremely poor people. |
| Impact, 2014 | All support and care focused on the psychological well-being and the health of people affected, provided by the user group of the guideline, in the acute and recovery phase, for the individual as well as groups. | Offer a frame of reference and a tool for providing MHPSS. Facilitate quality improvement, optimize MHPSS, and professionalize the user group of the guidelines. | Governments and public services, aid workers (professionals and volunteers), and their organizations. | All relevant groups within the affected population including people with (a history of) psychiatric problems; adolescents; children; mothers with young children; ethnic minorities; migrants; refugees; people who previously experienced potentially shocking events; people affected with limited access to social support and resources; affected staff members. |
| OPSIC, 2016 | Providing a humanitarian response in ways that are beneficial to the mental health and psychosocial well-being of the beneficiaries. | Point users to relevant guidelines, resources, and tools for planning and implementing MHPSS programs at all phases of response and in all types of disasters, and with all possible target groups. | Decision-makers, crisis managers (including incident command and psychosocial crisis managers), mental health professionals in multi-agency coordination groups, and practitioners. | All relevant groups within the affected population; children and adolescents; elderly; disabled persons; refugees; helpers (staff and volunteers); people with severe mental disorders; marginalized people; women and girls. |
| Red Cross, 2018 | Mental health: used to denote psychological well-being. Mental health interventions aim to improve psychological well-being by reducing levels of psychological distress, improving daily functioning, and ensuring effective coping strategies. Psychosocial: used to describe the interconnection between the individual (i.e., a person’s ‘psyche’) and their environment, interpersonal relationships, community, and/or culture (i.e., their social context). Psychosocial support: essential for maintaining good physical and mental health and provides an important coping mechanism for people during difficult times. | Encompass internationally recognized, evidence-based MHPSS standards and practices, combined with the expertise, experience, and views of mental health professionals who have worked in armed conflict and other violence. They are designed to be adapted and developed over time, and set out a framework of ethical principles, common definitions, and recommended procedures to be applied to the ICRC’s MHPSS activities. | Local, national, and international Red Cross organizations. | People affected by emergencies; victims of (sexual) violence; hospitalized weapon-wounded patients; families of victims/missing persons; helpers; people deprived of their liberty and former detainees; people with a physical or mental disability; children (e.g., separated from their families, associated with armed groups); elderly; marginalized social groups within the community. |
| Term | IASC | Impact | OPSIC | Red Cross | |
|---|---|---|---|---|---|
| Focal area 1 | Resilience | 9 | 35 | 197 | 5 |
| Vulnerable/Vulnerability/Vulnerabilities | 26 | 11 | 71 | 35 | |
| Risk/Risks (Risk factors) | 133 (2) | 17 (30) | 209 (15) | 19 (5) | |
| Needs | 56 | 66 | 271 | 376 | |
| Problem/Problems | 102 | 84 | 80 | 57 | |
| Disorder/Disorders | 111 | 13 | 82 | 69 | |
| Trauma/Traumatic | 12 (20) | 11 (10) | 145 (138) | 34 (20) | |
| PTSD * | 11 | 14 | 211 | 2 | |
| Focal area 2 | Prevent/Preventive/Prevention | 75 | 17 | 194 | 28 |
| Assessment/Assessments | 153 | 1 | 270 | 80 | |
| Needs assessment/assessments | 2 | 1 | 28 | 34 | |
| Screening/Screened | 4 | 11 | 50 | 5 | |
| Monitoring | 52 | 3 | 93 | 37 | |
| Evaluation/Evaluations | 36 | 28 | 115 | 19 | |
| Monitoring and evaluation/evaluating | 27 | 0 | 14 | 28 | |
| Coordination | 100 | 4 | 74 | 4 | |
| Preparation/Prepare/Prepared/Preparedness | 35 | 29 | 278 | 8 | |
| Implementation | 24 | 12 | 31 | 32 | |
| Training | 121 | 3 | 211 | 78 | |
| Resources | 147 | 7 | 268 | 57 | |
| Conditions ** | 32 | 5 | 29 | 21 | |
| Focal areas 1 and 2 | Circumstances | 2 | 11 | 20 | 12 |
| Context/Contexts | 40 | 25 | 84 | 18 | |
| Phase/Phases | 47 | 66 | 182 | 2 | |
| Culturally appropriate/sensitive/specific | 52 | 4 | 24 | 4 | |
| Ethics/Ethical | 29 | 0 | 63 | 15 | |
| Human rights | 91 | 0 | 38 | 3 |
| Basic Aid | Information | Emotional and Social Support | Practical Support | Health Care |
|---|---|---|---|---|
| Content:
Methods:
| Individual:
Community:
Collective:
|
|
Therapy, treatment:
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dückers, M.; van Hoof, W.; Willems, A.; te Brake, H. Appraising Evidence-Based Mental Health and Psychosocial Support (MHPSS) Guidelines—PART II: A Content Analysis with Implications for Disaster Risk Reduction. Int. J. Environ. Res. Public Health 2022, 19, 7798. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19137798
Dückers M, van Hoof W, Willems A, te Brake H. Appraising Evidence-Based Mental Health and Psychosocial Support (MHPSS) Guidelines—PART II: A Content Analysis with Implications for Disaster Risk Reduction. International Journal of Environmental Research and Public Health. 2022; 19(13):7798. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19137798
Chicago/Turabian StyleDückers, Michel, Wera van Hoof, Andrea Willems, and Hans te Brake. 2022. "Appraising Evidence-Based Mental Health and Psychosocial Support (MHPSS) Guidelines—PART II: A Content Analysis with Implications for Disaster Risk Reduction" International Journal of Environmental Research and Public Health 19, no. 13: 7798. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19137798