
A Randomized Controlled Trial Evaluating the Levels of the Biomarkers hs-CRP, IL-6, and IL-8 in Patients with Temporomandibular Disorder Treated with LLLT, Traditional Conservative Treatment, and a Combination of Both

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
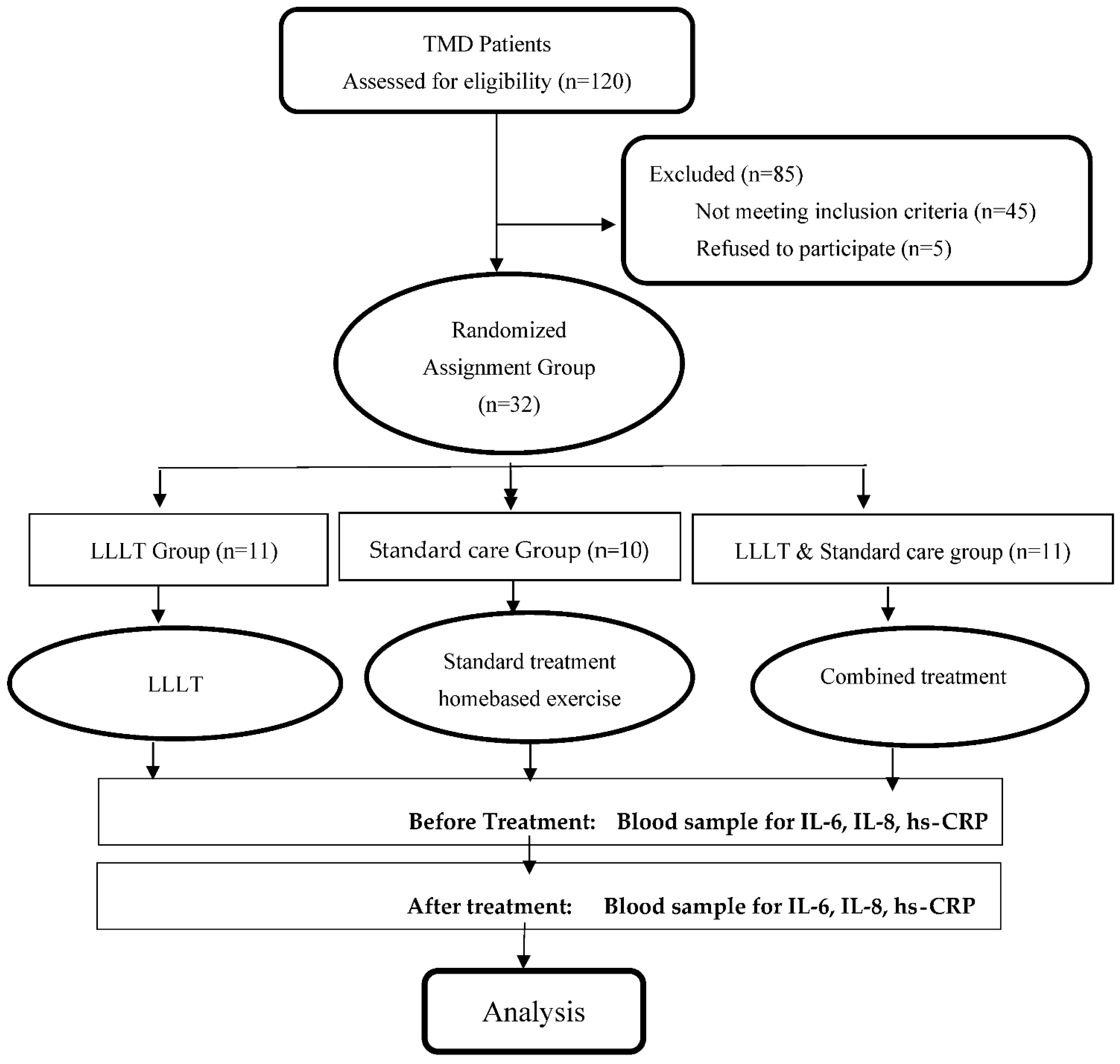
2.1. Study Design
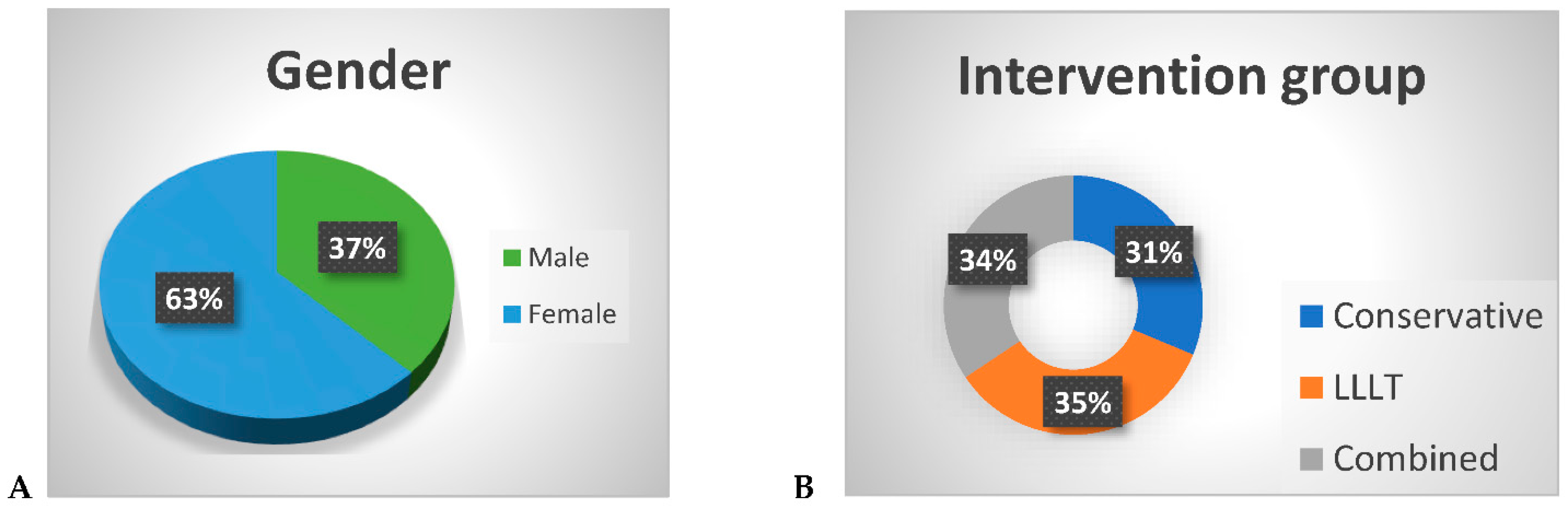
2.2. Patient Selection
2.3. Data Collection Procedure
2.3.1. Intervention
2.3.2. Biomarker’s Assay, Serum Interleukins IL-6, IL-8, and hs-CRP
2.4. Statistical Analysis
3. Results
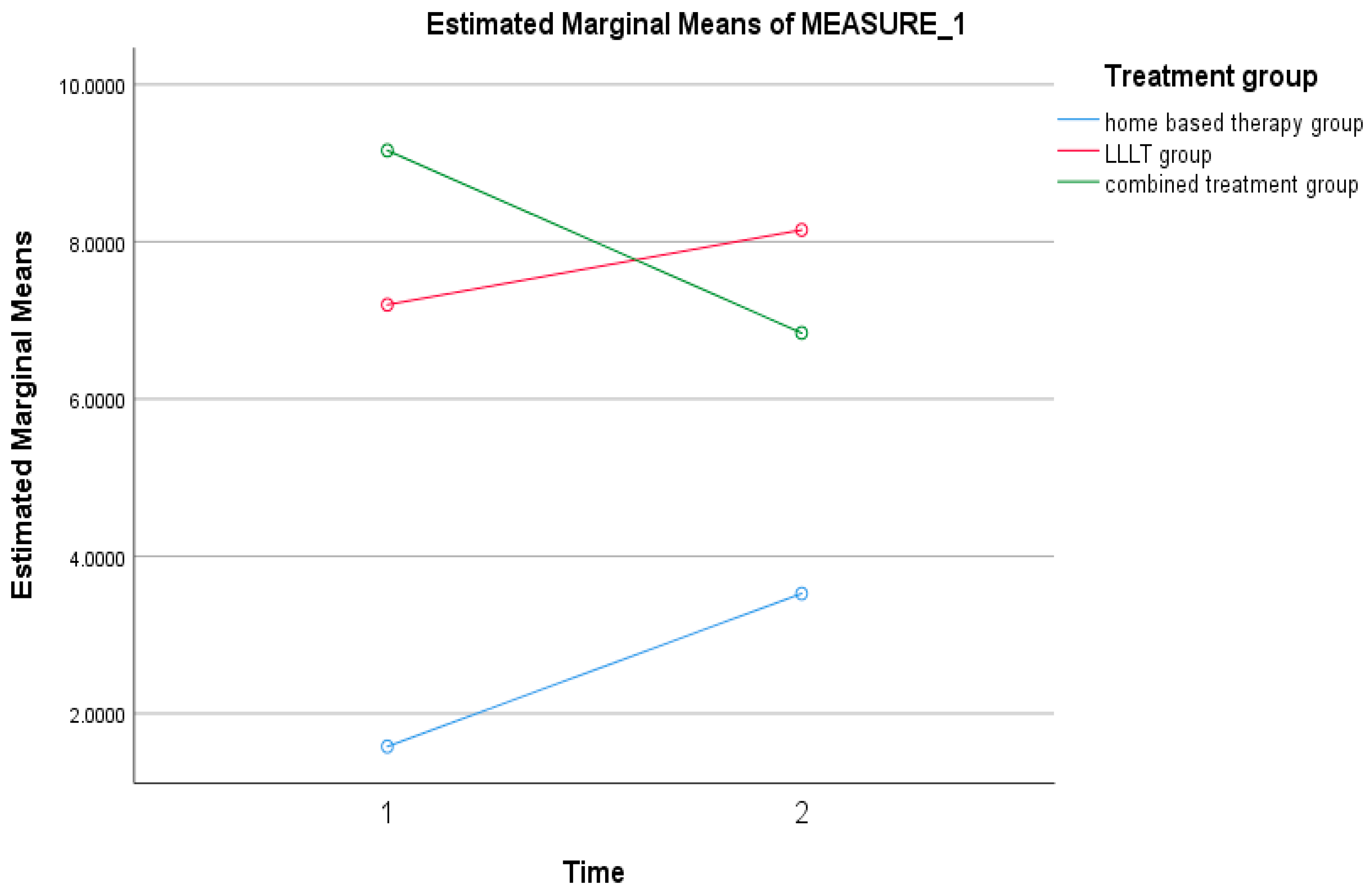
3.1. Effect of the Treatments (LLLT, Standard Treatment, and Combined Treatment) on Interleukin 6 (IL-6) Biomarkers
3.1.1. Within-Group Measures’ Analysis (Time Effect Regardless of Group)
3.1.2. Between-Group Analysis (Group Effect Regardless of Time)
3.1.3. Interaction Effect (Time Effect × Group Effect)
3.2. Effect of the Treatments (LLLT, Standard Treatment, and Combined Treatment) on Interleukin 8 (IL-8) Biomarkers
3.2.1. Within-Group Measures’ Analysis (Time Effect Regardless of Group)
3.2.2. Between-Group Analysis (Group Effect Regardless of Time)
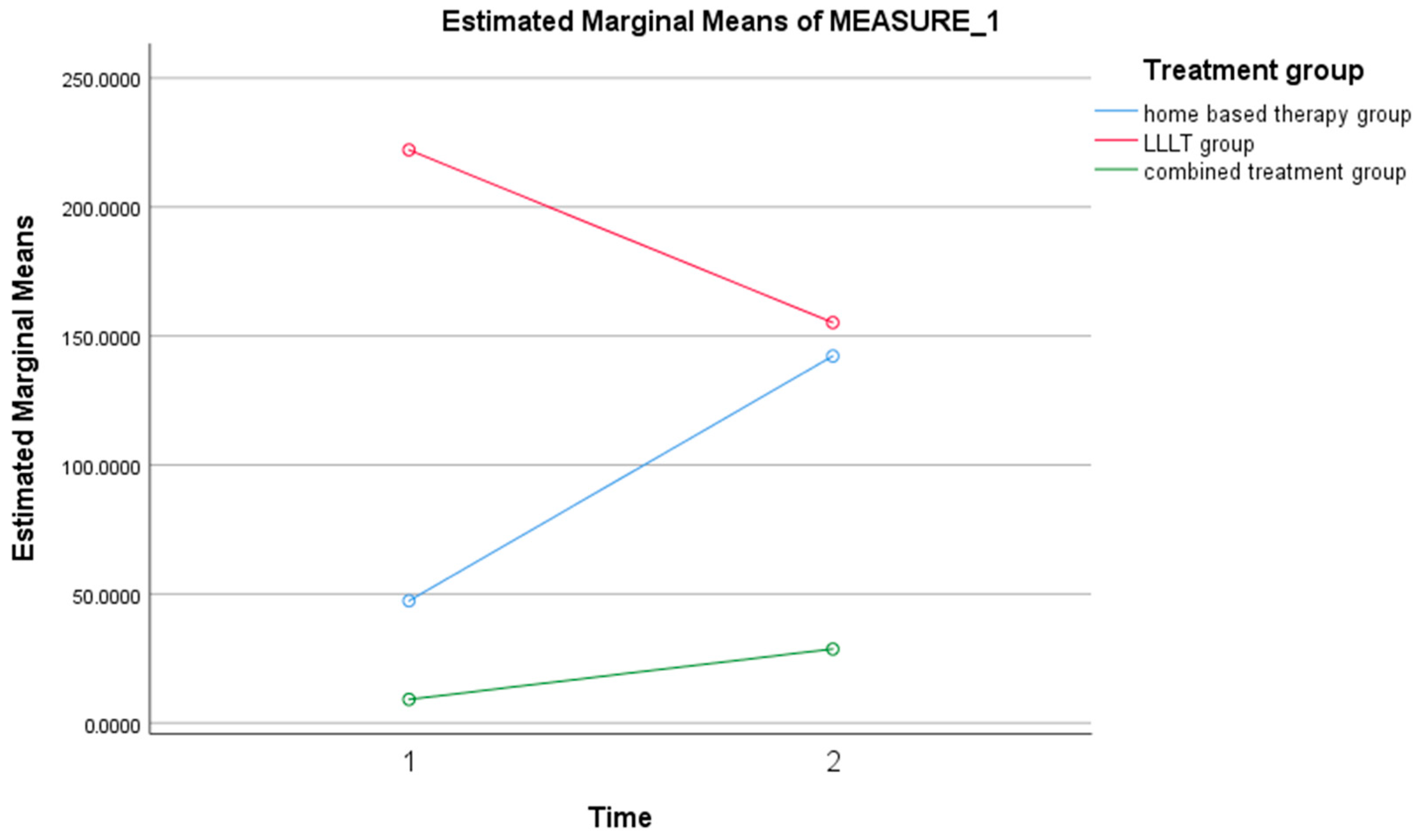
3.2.3. Interaction Effect (Time Effect × Group Effect)
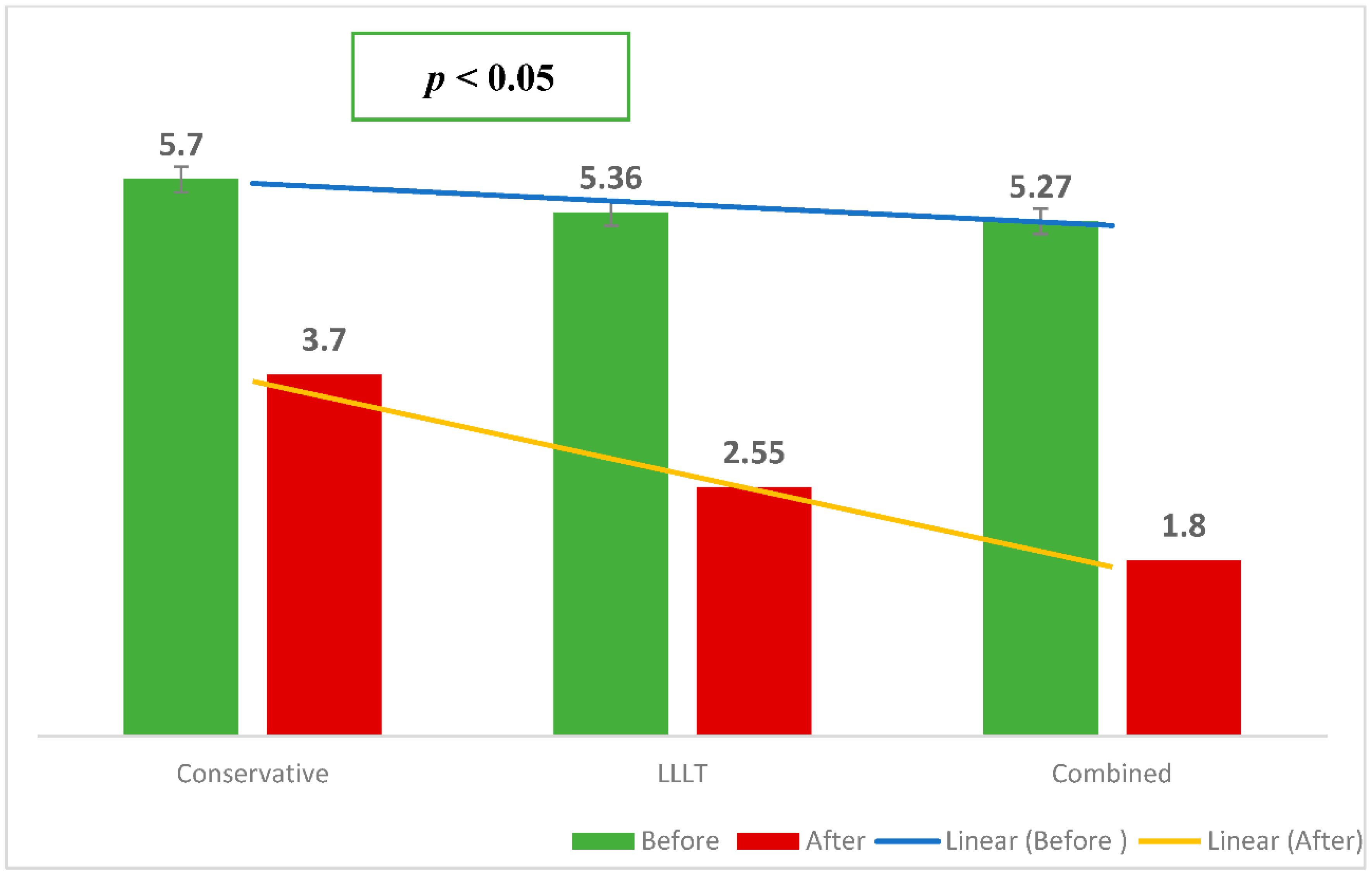
3.3. Effect of the Treatments (LLLT, Standard Treatment, and Combined Treatment) on High-Sensitivity C-Reactive Protein (hs-CRP) Biomarkers
3.3.1. Within-Group Measures Analysis (Time Effect Regardless of Group)
3.3.2. Between-Group Analysis (Group Effect Regardless of Time)
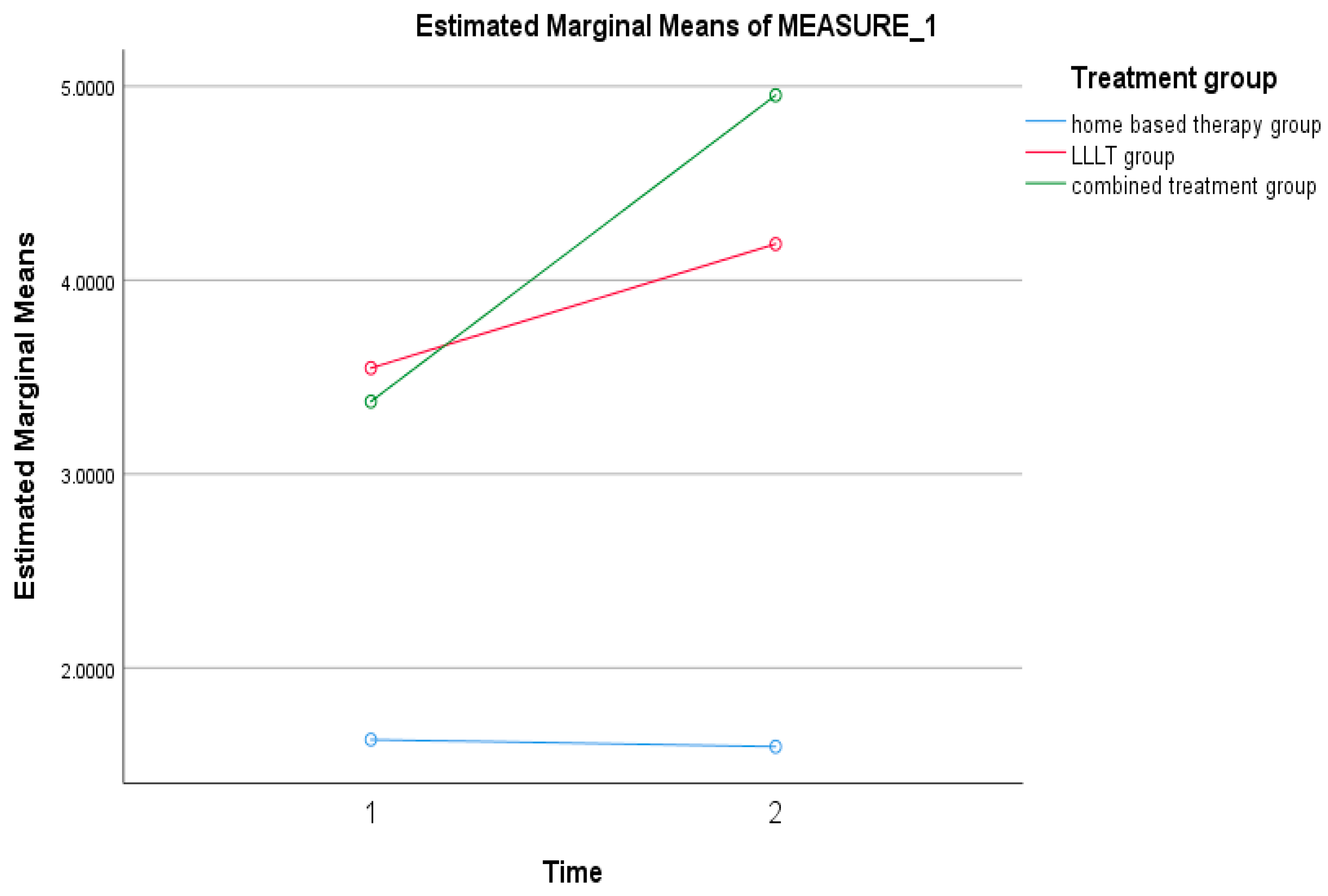
3.3.3. Interaction Effect (Time Effect × Group Effect)
3.4. Correlation between the Clinical Biomarkers and Pain Outcomes
4. Discussion
4.1. Effects of the Treatment Groups (LLLT, Standard Treatment, and Combined Treatment) on Interleukin 6 (IL-6)
4.2. Effects of the Treatment Groups (LLLT, Standard Treatment, and Combined Treatment) on Interleukin 8 (IL-8)
4.3. Effect of the Treatment Groups (LLLT, Standard Treatment, and Combined Treatment) on High-Sensitivity C-Reactive Protein (hs-CRP)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shrivastava, M.; Battaglino, R.; Ye, L. A comprehensive review on biomarkers associated with painful temporomandibular disorders. Int. J. Oral Sci. 2021, 13, 23. [Google Scholar] [CrossRef] [PubMed]
- Chisnoiu, A.M.; Picos, A.M.; Popa, S.; Chisnoiu, P.D.; Lascu, L.; Picos, A.; Chisnoiu, R. Factors involved in the etiology of temporomandibular disorders—A literature review. Clujul Med. 2015, 88, 473. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.R.; Kumar, N.R.; Shruthi, H.; Kalavathi, S.D. Temporomandibular pain. J. Oral Maxillofac. Pathol. JOMFP 2016, 20, 272. [Google Scholar] [CrossRef] [PubMed]
- Herr, M.M.; Fries, K.M.; Upton, L.G.; Edsberg, L.E. Potential biomarkers of temporomandibular joint disorders. J. Oral Maxillofac. Surg. 2011, 69, 41–47. [Google Scholar] [CrossRef]
- Davis, K.D.; Aghaeepour, N.; Ahn, A.H.; Angst, M.S.; Borsook, D.; Brenton, A.; Burczynski, M.E.; Crean, C.; Edwards, R.; Gaudilliere, B.; et al. Discovery and validation of biomarkers to aid the development of safe and effective pain therapeutics: Challenges and opportunities. Nat. Rev. Neurol. 2020, 16, 381–400. [Google Scholar] [CrossRef]
- Zwiri, A.; Alrawashdeh, M.A.; Khan, M.; Ahmad, W.M.A.W.; Kassim, N.K.; Ahmed Asif, J.; Suan Phaik, K.; Husein, A.; Ab-Ghani, Z. Effectiveness of the Laser Application in Temporomandibular Joint Disorder: A Systematic Review of 1172 Patients. Pain Res. Manag. 2020, 2020, 5971032. [Google Scholar] [CrossRef]
- Muñoz-Carrillo, J.L.; Contreras-Cordero, J.F.; Gutiérrez-Coronado, O.; Villalobos-Gutiérrez, P.T.; Ramos-Gracia, L.G.; Hernández-Reyes, V.E. Cytokine profiling plays a crucial role in activating immune system to clear infectious pathogens. In Immune Response Activation and Immunomodulation; IntechOpen: London, UK, 2018. [Google Scholar]
- Poluha, R.L.; Grossmann, E. Inflammatory mediators related to arthrogenic temporomandibular dysfunctions. BrJP 2018, 1, 60–65. [Google Scholar] [CrossRef]
- Ahmad, M.; Schiffman, E.L. Temporomandibular joint disorders and orofacial pain. Dent. Clin. 2016, 60, 105–124. [Google Scholar] [CrossRef]
- Randhawa, K.; Bohay, R.; Côté, P.; van der Velde, G.; Sutton, D.; Wong, J.J.; Yu, H.; Southerst, D.; Varatharajan, S.; Mior, S. The effectiveness of noninvasive interventions for temporomandibular disorders. Clin. J. Pain 2016, 32, 260–278. [Google Scholar] [CrossRef]
- Gil-Martínez, A.; Paris-Alemany, A.; López-de-Uralde-Villanueva, I.; La Touche, R. Management of pain in patients with temporomandibular disorder (TMD): Challenges and solutions. J. Pain Res. 2018, 11, 571. [Google Scholar] [CrossRef] [Green Version]
- Al-Moraissi, E.; Farea, R.; Qasem, K.; Al-Wadeai, M.; Al-Sabahi, M.; Al-Iryani, G. Effectiveness of occlusal splint therapy in the management of temporomandibular disorders: Network meta-analysis of randomized controlled trials. Int. J. Oral Maxillofac. Surg. 2020, 49, 1042–1056. [Google Scholar] [CrossRef] [PubMed]
- Häggman-Henrikson, B.; Alstergren, P.; Davidson, T.; Högestätt, E.; Östlund, P.; Tranæus, S.; Vitols, S.; List, T. Pharmacological treatment of oro-facial pain–health technology assessment including a systematic review with network meta-analysis. J. Oral Rehabil. 2017, 44, 800–826. [Google Scholar] [CrossRef]
- Dimitroulis, G. Management of temporomandibular joint disorders: A surgeon’s perspective. Aust. Dent. J. 2018, 63, S79–S90. [Google Scholar] [CrossRef]
- Calixtre, L.; Moreira, R.; Franchini, G.; Alburquerque-Sendín, F.; Oliveira, A. Manual therapy for the management of pain and limited range of motion in subjects with signs and symptoms of temporomandibular disorder: A systematic review of randomised controlled trials. J. Oral Rehabil. 2015, 42, 847–861. [Google Scholar] [CrossRef] [PubMed]
- Paço, M.; Peleteiro, B.; Duarte, J.; Pinho, T. The effectiveness of physiotherapy in the management of temporomandibular disorders: A systematic review and meta-analysis. J. Oral Facial Pain Headache 2016, 30, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Kapos, F.P.; Exposto, F.G.; Oyarzo, J.F.; Durham, J. Temporomandibular disorders: A review of current concepts in aetiology, diagnosis, and management. Oral Surg. 2020, 13, 321–334. [Google Scholar] [CrossRef]
- Chen, J.; Huang, Z.; Ge, M.; Gao, M. Efficacy of low-level laser therapy in the treatment of TMDs: A meta-analysis of 14 randomised controlled trials. J. Oral Rehabil. 2015, 42, 291–299. [Google Scholar] [CrossRef]
- Xu, G.-Z.; Jia, J.; Jin, L.; Li, J.-H.; Wang, Z.-Y.; Cao, D.-Y. Low-Level Laser Therapy for Temporomandibular Disorders: A Systematic Review with Meta-Analysis. Pain Res. Manag. 2018, 2018, 4230583. [Google Scholar] [CrossRef] [Green Version]
- Zokaee, H.; Zahmati, A.H.A.; Mojrian, N.; Boostani, A.; Vaghari, M. Efficacy of low-level laser therapy on orofacial pain: A literature review. Adv. Hum. Biol. 2018, 8, 70. [Google Scholar] [CrossRef]
- Manfredini, D. Occlusal equilibration for the management of temporomandibular disorders. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 257–264. [Google Scholar] [CrossRef]
- Manfredini, D.; Lombardo, L.; Siciliani, G. Temporomandibular disorders and dental occlusion. A systematic review of association studies: End of an era? J. Oral Rehabil. 2017, 44, 908–923. [Google Scholar] [CrossRef] [PubMed]
- Durham, J.; Aggarwal, V.; Davies, S.J.; Harrison, S.D.; Jagger, R.G. Temporomandibular Disorders (TMDs): An Update and Management Guidance for Primary Care from the UK Specialist Interest Group in Orofacial Pain and TMDs (USOT); Royal College of Surgeons of England: London, UK, 2013. [Google Scholar]
- Durham, J.; Al-Baghdadi, M.; Baad-Hansen, L.; Breckons, M.; Goulet, J.-P.; Lobbezoo, F.; List, T.; Michelotti, A.; Nixdorf, D.R.; Peck, C. Self-management programmes in temporomandibular disorders: Results from an international D elphi process. J. Oral Rehabil. 2016, 43, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, G.; Bonotto, D.; Hilgenberg-Sydney, P.B. Self-care, education, and awareness of the patient with temporomandibular disorder: A systematic review. BrJP 2018, 1, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Story, W.; Durham, J.; Al-Baghdadi, M.; Steele, J.; Araujo-Soares, V. Self-management in temporomandibular disorders: A systematic review of behavioural components. J. Oral Rehabil. 2016, 43, 759–770. [Google Scholar] [CrossRef]
- Michelotti, A.; Steenks, M.H.; Farella, M.; Parisini, F.; Cimino, R.; Martina, R. The additional value of a home physical therapy regimen versus patient education only for the treatment of myofascial pain of the jaw muscles: Short-term results of a randomized clinical trial. J. Orofac. Pain 2004, 18, 114–125. [Google Scholar]
- Brochado, F.T.; Jesus, L.H.; Carrard, V.C.; Freddo, A.L.; Chaves, K.D.; Martins, M.D. Comparative effectiveness of photobiomodulation and manual therapy alone or combined in TMD patients: A randomized clinical trial. Braz. Oral Res. 2018, 32, e50. [Google Scholar] [CrossRef] [Green Version]
- Graciele Carrasco, T.; Oliveira Mazzetto, M.; Galli Mazzetto, R.; Mestriner, W. Low intensity laser therapy in temporomandibular disorder: A phase II double-blind study. CRANIO® 2008, 26, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Nadershah, M.; Abdel-Alim, H.M.; Bayoumi, A.M.; Jan, A.M.; Elatrouni, A.; Jadu, F.M. Photobiomodulation therapy for myofascial pain in temporomandibular joint dysfunction: A double-blinded randomized clinical trial. J. Maxillofac. Oral Surg. 2020, 19, 93–97. [Google Scholar] [CrossRef]
- Cotler, H.B.; Chow, R.T.; Hamblin, M.R.; Carroll, J. The Use of Low Level Laser Therapy (LLLT) For Musculoskeletal Pain. MOJ Orthop. Rheumatol. 2015, 2, 00068. [Google Scholar] [CrossRef]
- Kuroda, S.; Tanimoto, K.; Izawa, T.; Fujihara, S.; Koolstra, J.H.; Tanaka, E. Biomechanical and biochemical characteristics of the mandibular condylar cartilage. Osteoarthr. Cartil. 2009, 17, 1408–1415. [Google Scholar] [CrossRef] [Green Version]
- Tosato, G.; Jones, K.D. Interleukin-1 induces interleukin-6 production in peripheral blood monocytes. Blood 1990, 75, 1305–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bas, B.; Yılmaz, N.; Gökce, E.; Akan, H. Diagnostic value of ultrasonography in temporomandibular disorders. J. Oral Maxillofac. Surg. 2011, 69, 1304–1310. [Google Scholar] [CrossRef] [PubMed]
- Shinoda, C.; Takaku, S. Interleukin-1 beta, interleukin-6, and tissue inhibitor of metalloproteinase-1 in the synovial fluid of the temporomandibular joint with respect to cartilage destruction. Oral Dis. 2000, 6, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Costello, N.L.; Bragdon, E.E.; Light, K.C.; Sigurdsson, A.; Bunting, S.; Grewen, K.; Maixner, W. Temporomandibular disorder and optimism: Relationships to ischemic pain sensitivity and interleukin-6. Pain 2002, 100, 99–110. [Google Scholar] [CrossRef]
- Lee, J.K.; Cho, Y.S.; Song, S.I. Relationship of synovial tumor necrosis factor α and interleukin 6 to temporomandibular disorder. J. Oral Maxillofac. Surg. 2010, 68, 1064–1068. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, J.N.; Gan, Y.H.; Zhou, Y.H. Current understanding of pathogenesis and treatment of TMJ osteoarthritis. J. Dent. Res. 2015, 94, 666–673. [Google Scholar] [CrossRef]
- Kapoor, M.; Martel-Pelletier, J.; Lajeunesse, D.; Pelletier, J.P.; Fahmi, H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nat. Rev. Rheumatol. 2011, 7, 33–42. [Google Scholar] [CrossRef]
- Gulen, H.; Ataoglu, H.; Haliloglu, S.; Isik, K. Proinflammatory cytokines in temporomandibular joint synovial fluid before and after arthrocentesis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, e1–e4. [Google Scholar] [CrossRef]
- Mendieta, D.; De la Cruz-Aguilera, D.L.; Barrera-Villalpando, M.I.; Becerril-Villanueva, E.; Arreola, R.; Hernández-Ferreira, E.; Pérez-Tapia, S.M.; Pérez-Sánchez, G.; Garcés-Alvarez, M.E.; Aguirre-Cruz, L.; et al. IL-8 and IL-6 primarily mediate the inflammatory response in fibromyalgia patients. J. Neuroimmunol. 2016, 290, 22–25. [Google Scholar] [CrossRef]
- Jounger, S.L.; Christidis, N.; Svensson, P.; List, T.; Ernberg, M. Increased levels of intramuscular cytokines in patients with jaw muscle pain. J. Headache Pain 2017, 18, 30. [Google Scholar] [CrossRef] [Green Version]
- Cê, P.S.; Barreiro, B.B.; Silva, R.; Oliveira, R.B.; Heitz, C.; Campos, M.M. Salivary Levels of Interleukin-1β in Temporomandibular Disorders and Fibromyalgia. J. Oral Facial Pain Headache 2018, 32, 130–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kacena, M.A.; Merrel, G.A.; Konda, S.R.; Wilson, K.M.; Xi, Y.; Horowitz, M.C. Inflammation and bony changes at the temporomandibular joint. Cells Tissues Organs 2001, 169, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Agha, M.T. Low-level Laser Therapy as a Solution in the Dental Clinic: A Review and Case Report. J. Oral Laser Appl. 2007, 7, 65–73. [Google Scholar]
- De Souza, A.B.; Okawa, R.T.; Silva, C.O.; Araújo, M.G. Short-term changes on C-reactive protein (CRP) levels after non-surgical periodontal treatment in systemically healthy individuals. Clin. Oral Investig. 2017, 21, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Pihut, M.; Ceranowicz, P.; Gala, A. Evaluation of C-reactive protein level in patients with pain form of temporomandibular joint dysfunction. Pain Res. Manag. 2018, 2018, 7958034. [Google Scholar] [CrossRef] [Green Version]
- D’Aiuto, F.; Parkar, M.; Andreou, G.; Suvan, J.; Brett, P.M.; Ready, D.; Tonetti, M.S. Periodontitis and systemic inflammation: Control of the local infection is associated with a reduction in serum inflammatory markers. J. Dent. Res. 2004, 83, 156–160. [Google Scholar] [CrossRef]
- Yamazaki, K.; Honda, T.; Oda, T.; Ueki-Maruyama, K.; Nakajima, T.; Yoshie, H.; Seymour, G.J. Effect of periodontal treatment on the C-reactive protein and proinflammatory cytokine levels in Japanese periodontitis patients. J. Periodontal Res. 2005, 40, 53–58. [Google Scholar] [CrossRef]
- Ramakrishnan, S.N.; Aswath, N. Comparative efficacy of analgesic gel phonophoresis and ultrasound in the treatment of temporomandibular joint disorders. Indian J. Dent. Res. 2019, 30, 512. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD) pg/100 mL | F-Statistic (df) | p-Value |
|---|---|---|---|
| IL-6 overall score | 0.010 (1, 29) | 0.920 | |
| IL-6 at baseline | 5.98(1.50) | ||
| IL-6 directly after treatment | 6.17 (1.08) | ||
| Between treatment group | 3.686 (2, 29) | 0.037 | |
| Time vs. treatment group | 0.471 (2, 29) | 0.629 | |
| IL-6 at baseline * | |||
| Home-based | 1.58 (0.08) | 2.247 (2, 29) | 0.124 |
| LLLT | 7.20 (6.56) | ||
| Combined treatment | 9.16 (12.80) | ||
| IL-6 directly after treatment * | |||
| Home-based | 3.53 (2.73) | 1.576 (2, 29) | 0.224 |
| LLLT | 8.15 (8.35) | ||
| Combined treatment | 6.84 (5.66) |
| Variable | Mean(SD) pg/100 mL | F-Statistic (df) | p-Value |
|---|---|---|---|
| IL-8 overall score | 0.157 (1, 29) | 0.695 | |
| IL-8 at baseline | 92.83 (20.63) | ||
| IL-8 directly after treatment | 108.69 (30.57) | ||
| Between treatment group | 8.844 (2, 29) | 0.001 | |
| Time vs. treatment group | 1.354 (2, 29) | 0.274 | |
| IL-8 at baseline * | |||
| Home-based | 47.35 (71.30) | 10.359 (2, 29) | <0.001 |
| LLLT | 222.11 (186.35) | ||
| Combined treatment | 9.13 (10.24) | ||
| IL-8 directly after treatment * | |||
| Home-based | 142.23 (197.48) | 1.767 (2, 29) | 0.189 |
| LLLT | 155.19 (222.94) | ||
| Combined treatment | 28.65 (41.71) | ||
| Variable | Mean (SD) mg/dL | F-Statistic (df) | p-Value |
|---|---|---|---|
| hs-CRP overall score | 0.137 (1, 29) | 0.714 | |
| CRP at baseline | 2.85 (1.13) | ||
| hs-CRP directly after treatment | 3.58 (1.54) | ||
| Time vs. Treatment group | 0.056 (2, 29) | 0.945 | |
| hs-CRP at baseline | |||
| Home based | 1.63 (2.33) | 0.286 (2, 29) | 0.753 |
| LLLT | 3.55 (9.14) | ||
| Combined treatment | 3.37 (5.40) | ||
| hs-CRP directly after treatment | |||
| Home based | 1.59 (2.36) | 0.422 (2, 29) | 0.660 |
| LLLT | 4.19 (9.72) | ||
| Combined treatment | 4.95 (10.99) | ||
| Biomarkers | VAS Baseline | VAS Directly after Treatment | VAS (4 Weeks) | VAS (8 Weeks) | VAS (12 Weeks) |
|---|---|---|---|---|---|
| IL-6 baseline | −0.08 | 0.36 * | −0.23 | −0.25 | −0.12 |
| IL-6 post-tretament | 0.04 | −0.09 | −0.01 | 0.04 | −0.10 |
| IL-8 baseline | 0.11 | −0.10 | 0.13 | 0.12 | 0.13 |
| IL-8 post-treatment | −0.11 | 0.17 | 0.27 | 0.11 | 0.14 |
| hs-CRP baseline | 0.15 | 0.03 | 0.05 | −0.03 | −0.14 |
| hs-CRP posttreatment | −0.12 | −0.22 | −0.30 | −0.19 | −0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwiri, A.M.; Ahmad, W.M.A.W.; Asif, J.A.; Phaik, K.S.; Husein, A.; Kassim, N.K.; Ab-Ghani, Z. A Randomized Controlled Trial Evaluating the Levels of the Biomarkers hs-CRP, IL-6, and IL-8 in Patients with Temporomandibular Disorder Treated with LLLT, Traditional Conservative Treatment, and a Combination of Both. Int. J. Environ. Res. Public Health 2022, 19, 8987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19158987
Zwiri AM, Ahmad WMAW, Asif JA, Phaik KS, Husein A, Kassim NK, Ab-Ghani Z. A Randomized Controlled Trial Evaluating the Levels of the Biomarkers hs-CRP, IL-6, and IL-8 in Patients with Temporomandibular Disorder Treated with LLLT, Traditional Conservative Treatment, and a Combination of Both. International Journal of Environmental Research and Public Health. 2022; 19(15):8987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19158987
Chicago/Turabian StyleZwiri, Abdalwhab MA, Wan Muhamad Amir W. Ahmad, Jawaad Ahmed Asif, Khoo Suan Phaik, Adam Husein, Nur Karyatee Kassim, and Zuryati Ab-Ghani. 2022. "A Randomized Controlled Trial Evaluating the Levels of the Biomarkers hs-CRP, IL-6, and IL-8 in Patients with Temporomandibular Disorder Treated with LLLT, Traditional Conservative Treatment, and a Combination of Both" International Journal of Environmental Research and Public Health 19, no. 15: 8987. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19158987