
Clinical Validation of a Deep-Learning Segmentation Software in Head and Neck: An Early Analysis in a Developing Radiation Oncology Center

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Auto-Segmentation Process
2.3. Evaluation Metrics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- AIOM. I Numeri del Cancro in Italia. Available online: https://www.aiom.it/i-numeri-del-cancro-in-italia/ (accessed on 24 March 2022).
- Patterson, J.M.; Lu, L.; Watson, L.-J.; Harding, S.; Ness, A.R.; Thomas, S.; Waylen, A.; Pring, M.; Waterboer, T.; Sharp, L. Associations between markers of social functioning and depression and quality of life in survivors of head and neck cancer: Findings from the Head and Neck Cancer 5000 study. Psycho-Oncol. 2022, 31, 478–485. [Google Scholar] [CrossRef]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef]
- Lo Nigro, C.; Denaro, N.; Merlotti, A.; Merlano, M. Head and neck cancer: Improving outcomes with a multidisciplinary approach. Cancer Manag. Res. 2017, 9, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Machiels, J.-P.; Leemans, C.R.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef]
- Grégoire, V.; Guckenberger, M.; Haustermans, K.; Lagendijk, J.J.W.; Ménard, C.; Pötter, R.; Slotman, B.J.; Tanderup, K.; Thorwarth, D.; van Herk, M.; et al. Image guidance in radiation therapy for better cure of cancer. Mol. Oncol. 2020, 14, 1470–1491. [Google Scholar] [CrossRef]
- LaVigne, A.W.; Margalit, D.N.; Rawal, B.; Puzanov, M.; Annino, D.J.; Goguen, L.A.; Sher, D.J.; Schoenfeld, J.D.; Chau, N.G.; Lorch, J.H.; et al. IMRT-based treatment of unknown primary malignancy of the head and neck: Outcomes and improved toxicity with decreased mucosal dose and larynx sparing. Head Neck 2019, 41, 959–966. [Google Scholar] [CrossRef]
- Kam, M.K.M.; Leung, S.-F.; Zee, B.; Chau, R.M.C.; Suen, J.J.S.; Mo, F.; Lai, M.; Ho, R.; Cheung, K.; Yu, B.K.H.; et al. Prospective randomized study of intensity-modulated radiotherapy on salivary gland function in early-stage nasopharyngeal carcinoma patients. J. Clin. Oncol. 2007, 25, 4873–4879. [Google Scholar] [CrossRef]
- Brouwer, C.L.; Steenbakkers, R.J.; van den Heuvel, E.; Duppen, J.C.; Navran, A.; Bijl, H.P.; Chouvalova, O.; Burlage, F.R.; Meertens, H.; Langendijk, J.A.; et al. 3D Variation in delineation of head and neck organs at risk. Radiat. Oncol. 2012, 7, 32. [Google Scholar] [CrossRef] [Green Version]
- Geets, X.; Daisne, J.-F.; Arcangeli, S.; Coche, E.; Poel, M.D.; Duprez, T.; Nardella, G.; Grégoire, V. Inter-observer variability in the delineation of pharyngo-laryngeal tumor, parotid glands and cervical spinal cord: Comparison between CT-scan and MRI. Radiother. Oncol. 2005, 77, 25–31. [Google Scholar] [CrossRef]
- Piras, A.; Boldrini, L.; Menna, S.; Venuti, V.; Pernice, G.; Franzese, C.; Angileri, T.; Daidone, A. Hypofractionated Radiotherapy in Head and Neck Cancer Elderly Patients: A Feasibility and Safety Systematic Review for the Clinician. Front. Oncol. 2021, 11, 761393. [Google Scholar] [CrossRef]
- Brouwer, C.L.; Steenbakkers, R.J.H.M.; Bourhis, J.; Budach, W.; Grau, C.; Grégoire, V.; van Herk, M.; Lee, A.; Maingon, P.; Nutting, C.; et al. CT-based delineation of organs at risk in the head and neck region: DAHANCA, EORTC, GORTEC, HKNPCSG, NCIC CTG, NCRI, NRG Oncology and TROG consensus guidelines. Radiother. Oncol. 2015, 117, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Cusumano, D.; Boldrini, L.; Dhont, J.; Fiorino, C.; Green, O.; Güngör, G.; Jornet, N.; Klüter, S.; Landry, G.; Mattiucci, G.C.; et al. Artificial Intelligence in magnetic Resonance guided Radiotherapy: Medical and physical considerations on state of art and future perspectives. Phys. Med. 2021, 85, 175–191. [Google Scholar] [CrossRef]
- Fionda, B.; Boldrini, L.; D’Aviero, A.; Lancellotta, V.; Gambacorta, M.A.; Kovács, G.; Patarnello, S.; Valentini, V.; Tagliaferri, L. Artificial intelligence (AI) and interventional radiotherapy (brachytherapy): State of art and future perspectives. J. Contemp. Brachyther. 2020, 12, 497–500. [Google Scholar] [CrossRef]
- Cusumano, D.; Lenkowicz, J.; Votta, C.; Boldrini, L.; Placidi, L.; Catucci, F.; Dinapoli, N.; Antonelli, M.V.; Romano, A.; de Luca, V.; et al. A deep learning approach to generate synthetic CT in low field MR-guided adaptive radiotherapy for abdominal and pelvic cases. Radiother. Oncol. 2020, 153, 205–212. [Google Scholar] [CrossRef]
- Brouwer, C.L.; Dinkla, A.M.; Vandewinckele, L.; Crijns, W.; Claessens, M.; Verellen, D.; van Elmpt, W. Machine learning applications in radiation oncology: Current use and needs to support clinical implementation. Phys. Imaging Radiat. Oncol. 2020, 16, 144–148. [Google Scholar] [CrossRef]
- Wong, J.; Fong, A.; McVicar, N.; Smith, S.; Giambattista, J.; Wells, D.; Kolbeck, C.; Giambattista, J.; Gondara, L.; Alexander, A. Comparing deep learning-based auto-segmentation of organs at risk and clinical target volumes to expert inter-observer variability in radiotherapy planning. Radiother. Oncol. 2020, 144, 152–158. [Google Scholar] [CrossRef]
- Wong, J.; Huang, V.; Wells, D.; Giambattista, J.; Giambattista, J.; Kolbeck, C.; Otto, K.; Saibishkumar, E.P.; Alexander, A. Implementation of deep learning-based auto-segmentation for radiotherapy planning structures: A workflow study at two cancer centers. Radiat. Oncol. 2021, 16, 101. [Google Scholar] [CrossRef]
- Wong, J.; Huang, V.; Giambattista, J.A.; Teke, T.; Kolbeck, C.; Giambattista, J.; Atrchian, S. Training and Validation of Deep Learning-Based Auto-Segmentation Models for Lung Stereotactic Ablative Radiotherapy Using Retrospective Radiotherapy Planning Contours. Front. Oncol. 2021, 11, 626499. [Google Scholar] [CrossRef] [PubMed]
- Vinod, S.K.; Min, M.; Jameson, M.G.; Holloway, L.C. A review of interventions to reduce inter-observer variability in volume delineation in radiation oncology. J. Med. Imaging Radiat. Oncol. 2016, 60, 393–406. [Google Scholar] [CrossRef]
- Patrick, H.M.; Souhami, L.; Kildea, J. Reduction of inter-observer contouring variability in daily clinical practice through a retrospective, evidence-based intervention. Acta Oncol. 2021, 60, 229–236. [Google Scholar] [CrossRef]
- Ayyalusamy, A.; Vellaiyan, S.; Subramanian, S.; Ilamurugu, A.; Satpathy, S.; Nauman, M.; Katta, G.; Madineni, A. Auto-segmentation of head and neck organs at risk in radiotherapy and its dependence on anatomic similarity. Radiat. Oncol. J. 2019, 37, 134–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolov, S.; Blackwell, S.; Zverovitch, A.; Mendes, R.; Livne, M.; de Fauw, J.; Patel, Y.; Meyer, C.; Askham, H.; Romera-Paredes, B.; et al. Clinically Applicable Segmentation of Head and Neck Anatomy for Radiotherapy: Deep Learning Algorithm Development and Validation Study. J. Med. Internet Res. 2021, 23, e26151. [Google Scholar] [CrossRef] [PubMed]
- Van Dijk, L.V.; den Bosch, L.V.; Aljabar, P.; Peressutti, D.; Both, S.; Steenbakkers, R.J.H.M.; Langendijk, J.A.; Gooding, M.J.; Brouwer, C.L. Improving automatic delineation for head and neck organs at risk by Deep Learning Contouring. Radiother. Oncol. 2020, 142, 115–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.Y.; Leech, M. Use of auto-segmentation in the delineation of target volumes and organs at risk in head and neck. Acta Oncol. 2016, 55, 799–806. [Google Scholar] [CrossRef]
- Eekers, D.B.; In’t Ven, L.; Roelofs, E.; Postma, A.; Alapetite, C.; Burnet, N.G.; Calugaru, V.; Compter, I.; Coremans, I.E.M.; Høyer, M.; et al. The EPTN consensus-based atlas for CT- and MR-based contouring in neuro-oncology. Radiother. Oncol. 2018, 128, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Scoccianti, S.; Detti, B.; Gadda, D.; Greto, D.; Furfaro, I.; Meacci, F.; Simontacchi, G.; di Brina, L.; Bonomo, P.; Giacomelli, I.; et al. Organs at risk in the brain and their dose-constraints in adults and in children: A radiation oncologist’s guide for delineation in everyday practice. Radiother. Oncol. 2015, 114, 230–238. [Google Scholar] [CrossRef]
- Yeghiazaryan, V.; Voiculescu, I. Family of boundary overlap metrics for the evaluation of medical image segmentation. J. Med. Imaging 2018, 5, 015006. [Google Scholar] [CrossRef]
- Ibragimov, B.; Xing, L. Segmentation of organs-at-risks in head and neck CT images using convolutional neural networks. Med. Phys. 2017, 44, 547–557. [Google Scholar] [CrossRef] [Green Version]
- La Macchia, M.; Fellin, F.; Amichetti, M.; Cianchetti, M.; Gianolini, S.; Paola, V.; Lomax, A.J.; Widesott, L. Systematic evaluation of three different commercial software solutions for automatic segmentation for adaptive therapy in head-and-neck, prostate and pleural cancer. Radiat. Oncol. 2012, 7, 160. [Google Scholar] [CrossRef] [Green Version]
- Mattiucci, G.C.; Boldrini, L.; Placidi, L.; Azario, L.; Dinapoli, N.; Chiloiro, G.; Pasini, D.; Piccari, D.; Gambacorta, M.A.; Balducci, M.; et al. Beyond geometrical overlap: A Dosimetrical Evaluation of automated volumes Adaptation (DEA) in head and neck replanning. Tech. Innov. Patient Support Radiat. Oncol. 2017, 3–4, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Vrtovec, T.; Močnik, D.; Strojan, P.; Pernuš, F.; Ibragimov, B. Auto-segmentation of organs at risk for head and neck radiotherapy planning: From atlas-based to deep learning methods. Med. Phys. 2020, 47, e929–e950. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
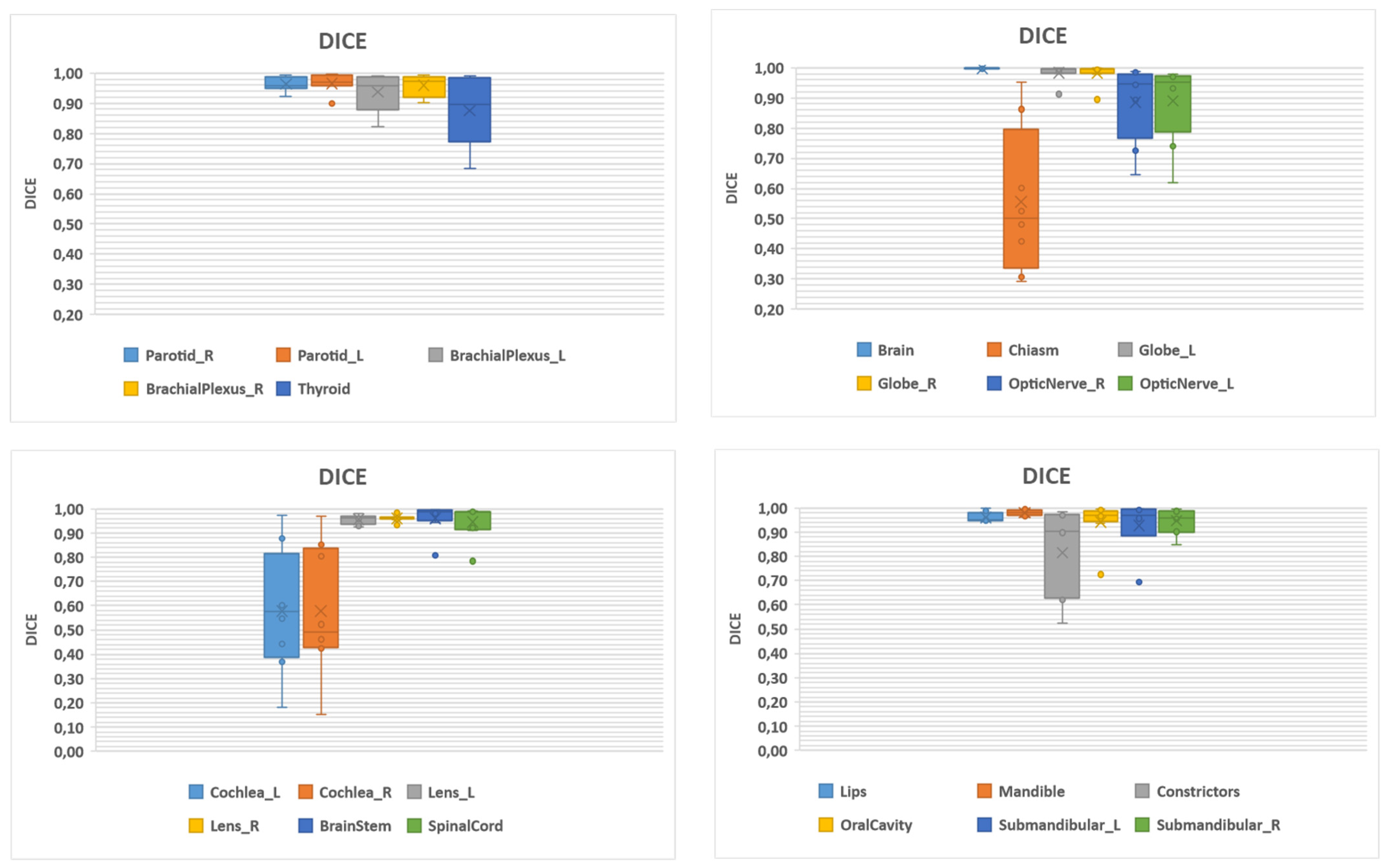
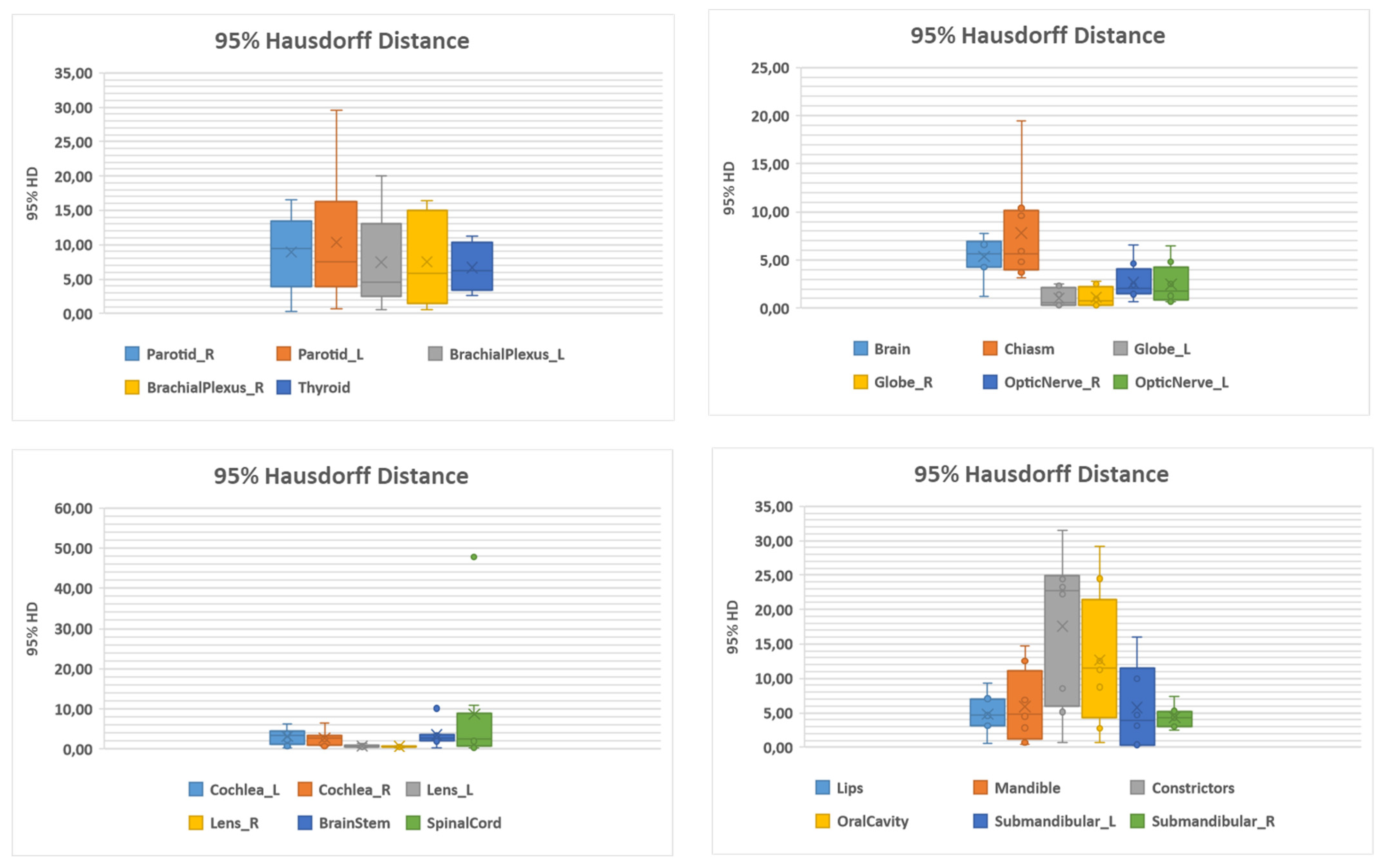
| Structure | Number | DSC | 95% HD (mm) | ||
|---|---|---|---|---|---|
| Mean (SD) | Median (Range) | Mean (SD) | Median (Range) | ||
| Brachial plexus L | 12 | 0.94 (0.06) | 0.96 (0.82–0.99) | 7.47 (6.71) | 4.51 (0.58–20.01) |
| Brachial plexus R | 12 | 0.96 (0.04) | 0.97 (0.90–0.99) | 7.53 (6.46) | 5.84 (0.52–16.42) |
| Brain | 12 | 1.00 (0.01) | 1.00 (0.99–1.00) | 5.35 (7.90) | 5.60 (1.26–7.79) |
| Brainstem | 12 | 0.96 (0.06) | 0.99 (0.81–0.1) | 3.46 (2.88) | 2.78 (0.29–10.12) |
| Cochlea L | 12 | 0.58 (0.26) | 0.57 (0.18–0.98) | 3.11 (1.99) | 3.34 (0.29–6.24) |
| Cochlea R | 12 | 0.58 (0.27) | 0.49 (0.15–0.97) | 2.69 (1.88) | 2.78 (0.73–6.51) |
| Optic chiasm | 12 | 0.56 (0.24) | 0.50 (0.29–0.95) | 7.79 (5.36) | 5.63 (3.20–19.41) |
| Pharyngeal constrictors | 12 | 0.82 (0.19) | 0.90 (0.52–0.99) | 17.59 (11.15) | 22.71 (0.74–31.52) |
| Eye globe L | 12 | 0.98 (0.03) | 1.00 (0.91–1.00) | 1.03 (0.93) | 0.59 (0.27–2.50) |
| Eye globe R | 12 | 0.98 (0.04) | 1.00 (0.89–1.00) | 1.13 (1.01) | 0.75 (0.29–2.84 |
| Lens L | 12 | 0.96 (0.02) | 0.96 (0.92–0.98) | 0.75 (0.39) | 0.58 (0.28–1.44) |
| Lens R | 12 | 0.96 (0.01) | 0.96 (0.93–0.98) | 0.57 (0.16) | 0.58 (0.27–0.74) |
| Lips | 12 | 0.96 (0.02) | 0.95 (0.94–1.00) | 4.79 (2.83) | 4.62 (0.53–9.37) |
| Mandible | 12 | 0.98 (0.01) | 0.98 (0.96–1.00) | 5.93 (5.26) | 4.75 (0.37–14.72) |
| Optic nerve L | 12 | 0.89 (0.14) | 0.95 (0.62–0.98) | 2.67 (1.96) | 2.03 (0.65–6.57) |
| Optic nerve R | 12 | 0.89 (0.13) | 0.95 (0.65–0.99) | 2.49 (2.09) | 1.74 (0.65–6.48) |
| Oral cavity | 12 | 0.94 (0.09) | 0.97 (0.72–1.00) | 12.67 (9.79) | 11.56 (0.65–29.11) |
| Parotid L | 12 | 0.97 (0.03) | 0.97 (0.90–1.00) | 8.96 (5.79) | 9.44 (0.29–16.57) |
| Parotid R | 12 | 0.96 (0.02) | 0.96 (0.92–0.99) | 10.33 (9.37) | 7.50 (0.64–29.54) |
| Spinal cord | 12 | 0.95 (0.07) | 0.99 (0.78–0.99) | 8.70 (16.12) | 2.59 (0.29–47.74) |
| Submandibular gland L | 11 | 0.93 (0.12) | 0.97 (0.69–1) | 5.75 (6.17) | 3.92 (0.29–16.04) |
| Submandibular gland R | 11 | 0.95 (0.05) | 0.96 (0.85–0.99) | 4.39 (1.69) | 4.36 (2.55–7.44) |
| Thyroid | 12 | 0.88 (0.11) | 0.90 (0.69–0.99) | 6.71 (3.49) | 6.24 (2.55–11.21) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Aviero, A.; Re, A.; Catucci, F.; Piccari, D.; Votta, C.; Piro, D.; Piras, A.; Di Dio, C.; Iezzi, M.; Preziosi, F.; et al. Clinical Validation of a Deep-Learning Segmentation Software in Head and Neck: An Early Analysis in a Developing Radiation Oncology Center. Int. J. Environ. Res. Public Health 2022, 19, 9057. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159057
D’Aviero A, Re A, Catucci F, Piccari D, Votta C, Piro D, Piras A, Di Dio C, Iezzi M, Preziosi F, et al. Clinical Validation of a Deep-Learning Segmentation Software in Head and Neck: An Early Analysis in a Developing Radiation Oncology Center. International Journal of Environmental Research and Public Health. 2022; 19(15):9057. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159057
Chicago/Turabian StyleD’Aviero, Andrea, Alessia Re, Francesco Catucci, Danila Piccari, Claudio Votta, Domenico Piro, Antonio Piras, Carmela Di Dio, Martina Iezzi, Francesco Preziosi, and et al. 2022. "Clinical Validation of a Deep-Learning Segmentation Software in Head and Neck: An Early Analysis in a Developing Radiation Oncology Center" International Journal of Environmental Research and Public Health 19, no. 15: 9057. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159057