
Effects of Tobacco Smoking on the Survivability of Patients with Multiple Cancers and Single Lung Cancer


Abstract
:1. Introduction
- Smoking is an important factor in the development of neoplastic diseases and affects the survival of patients.
- Smoking cessation contributes to extending the life span of patients.
- The patients’ survival depends on the risk factors, including the previous treatment of the neoplastic disease.
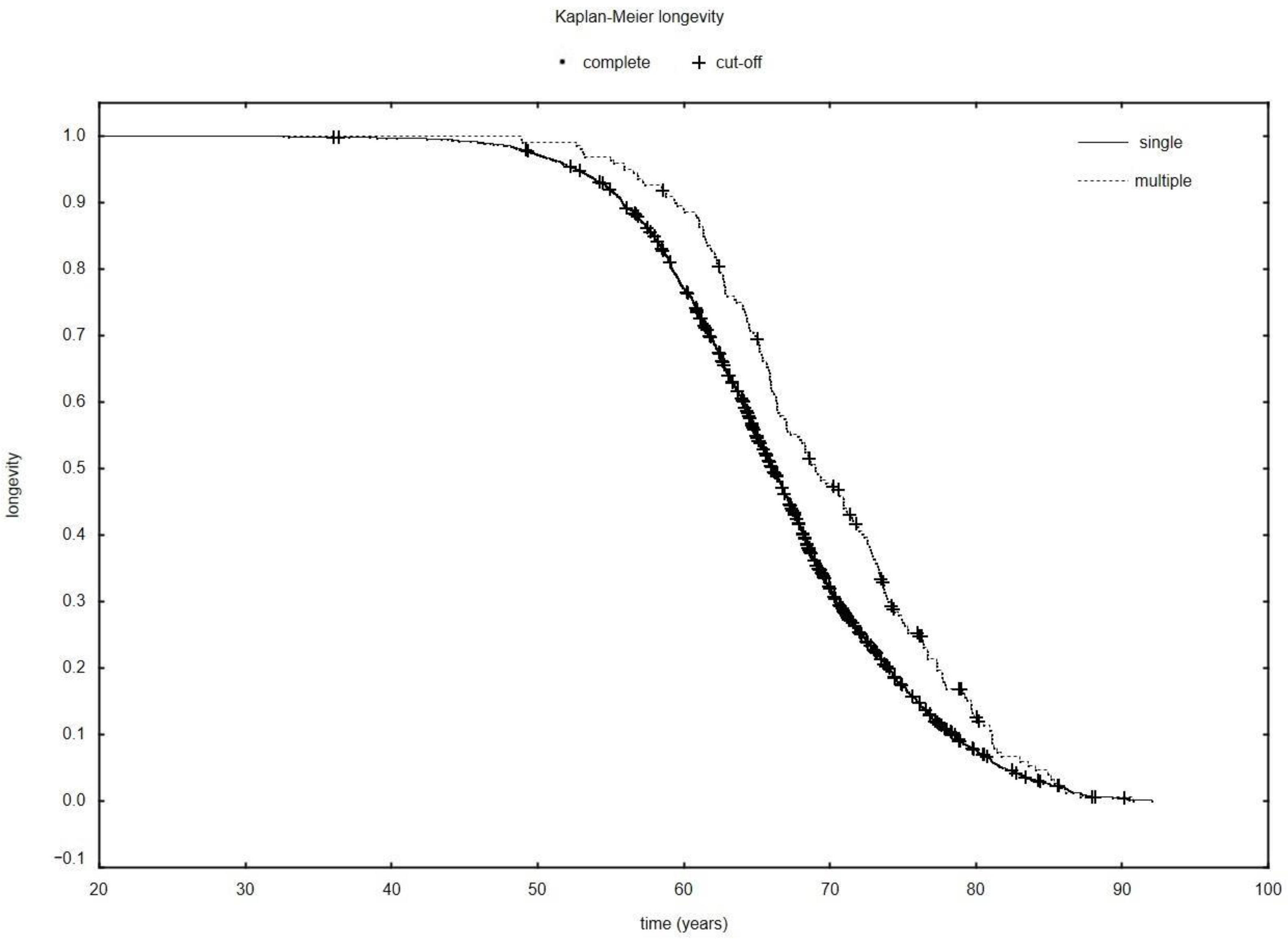
- Patients with multiple cancers whose last cancer process was lung cancer live longer than patients with single lung cancer.
2. Materials and Methods
2.1. Patient and Study Design
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethics Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. International Agency for Research on Cancer; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Luciani, A.; Balducci, L. Multiple primary malignancies. Semin. Oncol. 2004, 31, 264–273. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Shao, M.; He, X.; Ren, S.; Tian, T. Risk of lung cancer due to external environmental factor and epidemiological data analysis. Math. Biosci. Eng. 2021, 18, 6079–6094. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.; Dubey, A.; Saini, D.; Singh, M.; Prasad, C.P.; Roy, S.; Bharati, S.J.; Rinki, M.; Singh, N.; Seth, T.; et al. Environmental and occupational determinants of lung cancer. Transl. Lung Cancer Res. 2019, 8, S31. [Google Scholar] [CrossRef] [PubMed]
- Bonner, M.R.; Freeman, L.E.B.; Hoppin, J.A.; Koutros, S.; Sandler, D.P.; Lynch, C.F.; Hines, C.J.; Thomas, K.; Blair, A.; Alavanja, M.C.R. Occupational exposure to pesticides and the incidence of lung cancer in the agricultural health study. Environ. Health Perspect. 2017, 125, 544–551. [Google Scholar] [CrossRef] [Green Version]
- Kangkhetkron, T.; Juntarawijit, C. Pesticide exposure and lung cancer risk: A case-control study in Nakhon Sawan, Thailand. F1000Research 2020, 9, 492. [Google Scholar] [CrossRef]
- MacLeod, J.S.; Harris, M.A.; Tjepkema, M.; Peters, P.A.; Demers, P.A. Cancer risks among welders and occasional welders in a national population-based cohort study: Canadian census health and environmental cohort. Saf. Health Work. 2017, 8, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Honaryar, M.K.; Lunn, R.M.; Luce, D.; Ahrens, W.; Hansen, J.; Bouaoun, L.; Loomis, D.; Byrnes, G.; Vilahur, N.; Stayner, L.; et al. Welding fumes and lung cancer: A meta-analysis of case-control and cohort studies. Occup. Environ. Med. 2019, 76, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Centrum Badania Opinii Społecznych. Komunikat z Badań. Palenie Tytoniu; Fundacja Centrum Badania Opinii Społeczne: Warsaw, Poland, 2019; Volume 104. [Google Scholar]
- Nagah, A.; Amer, A. Different Mechanisms of Cigarette Smoking-Induced Lung Cancer. Acta Biotheor. 2021, 69, 37–52. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.; Hu, S.; Li, C.; Ma, H.; Wang, Q.; Meng, G.; Guo, T.; Zhang, J. Cigarette smoke induced lung barrier dysfunction, EMT, and tissue remodeling: A possible link between COPD and lung cancer. BioMed Res. Int. 2019, 2019, 2025636. [Google Scholar] [CrossRef] [PubMed]
- MacRosty, C.R.; Rivera, M.P. Lung cancer in women: A modern epidemic. Clin. Chest Med. 2020, 41, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. Cancer survivors--United States. MMWR Morb. Mortal. Wkly. Rep. 2011, 60, 269–272. [Google Scholar]
- Khuder, S.A.; Mutgi, A.B. Effect of smoking cessation on major histologic types of lung cancer. Chest 2001, 120, 1577–1583. [Google Scholar] [CrossRef] [Green Version]
- Shiels, M.S.; Gibson, T.; Sampson, J.; Albanes, D.; Andreotti, G.; Freeman, L.B.; de Gonzalez, A.B.; Caporaso, N.; Curtis, R.E.; Elena, J.; et al. Cigarette smoking prior to first cancer and risk of second smoking-associated cancers among survivors of bladder, kidney, head and neck, and stage I lung cancers. J. Clin. Oncol. 2014, 32, 3989. [Google Scholar] [CrossRef] [Green Version]
- Romaszko-Wojtowicz, A.; Buciński, A.; Doboszyńska, A. Impact of smoking on multiple primary cancers survival: A retrospective analysis. Clin. Exp. Med. 2018, 18, 391–397. [Google Scholar] [CrossRef] [Green Version]
- Ozasa, K.; Katanoda, K.; Tamakoshi, A.; Sato, H.; Tajima, K.; Suzuki, T.; Tsugane, S.; Sobue, T. Reduced life expectancy due to smoking in large-scale cohort studies in Japan. J. Epidemiol. 2008, 18, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Aredo, J.V.; Luo, S.J.; Gardner, R.M.; Sanyal, N.; Choi, E.; Hickey, T.P.; Riley, T.L.; Huang, W.; Kurian, A.W.; Leung, A.N.; et al. Tobacco smoking and risk of second primary lung cancer. J. Thorac. Oncol. 2021, 16, 968–979. [Google Scholar] [CrossRef]
- Moertel, C.G.; Dockerty, M.B.; Baggenstoss, A.H. Multiple primary malignant neoplasms. I. Introduction and presentation of data. Cancer 1961, 14, 221–230. [Google Scholar] [CrossRef]
- West, R. Tobacco smoking: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 1018–1036. [Google Scholar]
- Dubin, S.; Griffin, D. Lung cancer in non-smokers. Mo. Med. 2020, 117, 375. [Google Scholar]
- Wang, S.; Takayama, K.; Tanaka, K.; Takeshita, M.; Nakagaki, N.; Ijichi, K.; Li, H.; Nakanishi, Y. Nicotine induces resistance to epidermal growth factor receptor tyrosine kinase inhibitor by α1 nicotinic acetylcholine receptor–mediated activation in PC9 cells. J. Thorac. Oncol. 2013, 8, 719–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jemal, A.; Ward, E.; Thun, M.J. Contemporary lung cancer trends among US women. Cancer Epidemiol. Biomark. Prev. 2005, 14, 582–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, M.; Lao, X.Q.; Ho, K.-F.; Goggins, W.B.; Tse, S.L. Incidence and mortality of lung cancer: Global trends and association with socioeconomic status. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Harris, J.E. Cigarette smoking among successive birth cohorts of men and women in the United States during 1900. J. Natl. Cancer Inst. 1983, 71, 473–479. [Google Scholar]
- Egleston, B.L.; Meireles, S.I.; Flieder, D.B.; Clapper, M.L. (Eds.) Population-based trends in lung cancer incidence in women. Semin. Oncol. 2009, 36, 506–515. [Google Scholar] [CrossRef] [Green Version]
- Kligerman, S.; White, C. Epidemiology of lung cancer in women: Risk factors, survival, and screening. Am. J. Roentgenol. 2011, 196, 287–295. [Google Scholar] [CrossRef]
- Thun, M.J.; Carter, B.D.; Feskanich, D.; Freedman, N.D.; Prentice, R.; Lopez, A.D.; Hartge, P.; Gapstur, S.M. 50-year trends in smoking-related mortality in the United States. N. Engl. J. Med. 2013, 368, 351–364. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Lei, H.; Li, X.; Zhou, W.; Wang, G.; Sun, A.; Wang, Y.; Wu, Y.; Peng, B. Lung Cancer-Specific Mortality Risk and Public Health Insurance: A Prospective Cohort Study in Chongqing, Southwest China. Front. Public Health 2022, 10, 842844. [Google Scholar] [CrossRef]
- Buist, A.S.; McBurnie, M.A.; Vollmer, W.M.; Gillespie, S.; Burney, P.; Mannino, D.M.; Menezes, A.M.; Sullivan, S.D.; Lee, T.A.; Weiss, K.B.; et al. International variation in the prevalence of COPD (the BOLD Study): A population-based prevalence study. Lancet 2007, 370, 741–750. [Google Scholar] [CrossRef]
- Risch, H.A.; Howe, G.R.; Jain, M.; Burch, J.D.; Holowaty, E.J.; Miller, A.B. Are female smokers at higher risk for lung cancer than male smokers? A case-control analysis by histologic type. Am. J. Epidemiol. 1993, 138, 281–293. [Google Scholar] [CrossRef]
- Barrera-Rodriguez, R.; Morales-Fuentes, J. Lung cancer in women. Lung Cancer Targets Ther. 2012, 3, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Din, N.U.; Ukoumunne, O.C.; Rubin, G.; Hamilton, W.; Carter, B.; Stapley, S.; Neal, R.D. Age and gender variations in cancer diagnostic intervals in 15 cancers: Analysis of data from the UK Clinical Practice Research Datalink. PLoS ONE 2015, 10, e0127717. [Google Scholar] [CrossRef] [Green Version]
- Ek, S. Gender differences in health information behaviour: A Finnish population-based survey. Health Promot. Int. 2015, 30, 736–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- General, U.S. The Health Benefits of Smoking Cessation; Department of Health and Human Services: Washington, DC, USA, 1990; pp. 11–17.
- Lung Cancer Survival Rate. American Cancer Society. Available online: https://www.cancer.org/cancer/lung-cancer/detection-diagnosis-staging/survival-rates.html (accessed on 10 April 2022).
- Smith, P.H.; Bessette, A.J.; Weinberger, A.H.; Sheffer, C.E.; McKee, S.A. Sex/gender differences in smoking cessation: A review. Prev. Med. 2016, 92, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Jarvis, M.J.; Cohen, J.E.; Delnevo, C.D.; Giovino, G.A. Dispelling myths about gender differences in smoking cessation: Population data from the USA, Canada and Britain. Tob. Control 2013, 22, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, M. Gender and smoking: Do women really find it harder to give up? Br. J. Addict. 1984, 79, 383–387. [Google Scholar] [CrossRef]
- Amer, M.H. Multiple neoplasms, single primaries, and patient survival. Cancer Manag. Res. 2014, 6, 119. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 2301) | Neoplasms | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Single | Multiple | Neoplasmsa | ||||||||||
| Women | Men | p | Women | Men | p | Women | Men | p | Single | Multiple | p | |
| n; % | n; % | n; % | n; % | n; % | n; % | n; % | n; % | |||||
| 724; 31.47 | 1577; 68.53 | 654; 31.46 | 1425; 68.54 | 70; 31.53 | 152; 68.47 | 2079; 90.35 | 222; 9.65 | |||||
| Smokers | 461; 63.67 | 1035; 65.63 | 0.361 (1) | 428; 65.44 | 964; 67.65 | 0.320 (1) | 33; 47.14 | 71; 46.71 | 0.952 (1) | 1392; 66.96 | 104; 46.85 | 0.000 (1) |
| Ex-smokers | 194; 26.80 | 484; 30.69 | 0.057 (1) | 170; 25.99 | 411; 28.84 | 0.179 (1) | 24; 34.29 | 73; 48.03 | 0.055 (1) | 581; 27.95 | 97; 43.69 | 0.000 (1) |
| Non-smokers | 69; 9.53 | 58; 3.68 | 0.000 (1) | 56; 8.56 | 50; 3.51 | 0.000 (1) | 13; 18.57 | 8; 5.26 | 0.002 (1) | 106; 5.09 | 21; 9.46 | 0.007 (1) |
| AVG; SD; M; n | AVG; SD; M; n | p | AVG; SD; M; n | AVG; SD; M; n | p | AVG; SD; M; n | AVG; SD; M; n | p | AVG; SD; M; n | AVG; SD; M; n | p | |
| Packyears | 32.98; 19.02; 30; 722 | 39.44; 20.22; 40; 1577 | 0.000 (2) | 33.58; 18.19; 30; 654 | 39.30; 19.86; 40; 1425 | 0.000 (2) | 27.15; 19.39; 30; 68 | 40.72; 23.38; 40; 152 | 0.000 (2) | 37.50; 19.73; 40; 2079 | 36.53; 23.05; 40; 220 | 0.296 (2) |
| Packyears smokers | 38.78; 16.65; 40; 461 | 42.41; 19.69; 40; 1035 | 0.000 (2) | 38.84; 16.71 40; 428 | 42.23; 19; 54 40; 964 | 0.000 (2) | 37.91; 16.15; 40; 33 | 44.87; 21.70; 40; 71 | 0.131 (2) | 41.19; 18.77; 40; 1392 | 42.66; 20.29; 40; 104 | 0.655 (2) |
| Packyears ex-smokers | 30.11; 14.97; 30; 192 | 37.34; 17.33; 40; 484 | 0.000 (2) | 30.51; 15.22; 30; 170 | 36.66; 16.28; 40; 411 | 0.000 (2) | 27.05; 12.79; 25; 22 | 41.15; 22.07; 40; 73 | 0.004 (2) | 34.86; 16.21; 30; 581 | 37.88; 21.11; 35; 95 | 0.366 (2) |
| Packyears non-smokers | 2.22; 10.95; 0; 69 | 3.79; 15.25; 0; 58 | 0.529 (2) | 2.73; 12.11 0; 56 | 4.40; 16.37; 0; 50 | 0.581 (2) | 0.00; 0.00; 0; 13 | 0.00; 0.00; 0; 8 | 0.971 (2) | 3.51; 14.23; 0; 106 | 0.00; 0.00 0; 21 | 0.231 (2) |
| Variable | Total (n = 2301) | Neoplasms | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Single | Multiple | Neoplasma | ||||||||||
| Women | Men | p | Women | Men | p | Women | Men | p | Single | Multiple | p | |
| AVG; SD; M; n | AVG; SD; M; n | AVG; SD; M; n | AVG; SD; M; n | AVG; SD; M; n | AVG; SD; M; n | AVG; SD; M; n | AVG; SD; M; n | |||||
| Age of 1st cancer | 63.19; 9.00; 63; 724 | 64.71; 8.40; 65; 1577 | 0.000 (2) | 63.80; 8.53; 63; 654 | 64.91; 8.32; 65; 1425 | 0.007 (2) | 57.41; 11.07; 58; 70 | 62.87; 8.95; 62; 152 | 0.001 (1) | 64.56; 8.40; 64; 2079 | 61.15; 9.97; 61; 222 | 0.000 (2) |
| Age of 2nd cancer | 66.20; 7.96; 65; 70 | 68.63; 7.84; 68; 152 | 0.015 (1) | 66.20; 7.96; 65; 70 | 68.63; 7.84; 68; 152 | 0.015 (1) | 67.86; 7.94; 67; 222 | |||||
| Interval between 1st and 2nd cancer (years) | 8.79; 8.88; 6; 70 | 5.76; 6.52; 4;152 | 0.015 (2) | 6.71; 7.46; 4; 222 | ||||||||
| General total survival time (years) | 65.33; 8.47; 65; 724 | 66.5; 8.35; 66; 1577 | 0.003 (2) | 65.09; 8.51; 65; 654 | 66.13; 8.31; 66; 1425 | 0.012 (2) | 67.60; 7.77; 66; 70 | 69.91; 7.97; 71; 152 | 0.037 (1) | 65.80; 8.39; 66; 2079 | 69.18; 7.96; 69; 222 | 0.000 (2) |
| Smokers’ total survival time (years) | 64.49; 7.78; 64.06; 461 | 65.11; 8.05; 65.00; 1035 | 0.055 (2) | 64.35; 7.71; 63.95; 428 | 64.98; 8.07; 64.90; 964 | 0.071 (2) | 66.32; 8.48; 66.32; 33 | 66.94; 7.47; 66.83; 71 | 0.708 (1) | 64.78; 7.97; 64.63; 1392 | 66.74; 7.77; 66.11; 104 | 0.014 (2) |
| Ex-smokers’ survival time (years) | 66.14; 8.40; 66.36; 194 | 68.89; 8.05; 68.53; 484 | 0.000 (2) | 66.05; 8.69; 66.33; 170 | 68.28; 8.06; 67.85; 411 | 0.007 (2) | 66.82; 6.11; 66.79; 24 | 72.32; 7.11; 73.22; 73 | 0.001 (1) | 67.63; 8.30; 67.33; 581 | 70.96; 7.25; 71.51; 97 | 0.000 (2) |
| Non-smokers’ total survival time (years) | 68.28; 11.74; 68.67; 69 | 70.17; 10.17; 68.39; 58 | 0.336 (1) | 67.40; 12.40; 67.35; 56 | 69.65; 10.08; 69.65; 50 | 0.310 (1) | 72.06; 7.54; 72.31; 13 | 73.44; 10.79; 67.28; 8 | 0.799 (2) | 68.46; 11.37; 68.25; 106 | 72.58; 8.68; 69.64; 21 | 0.136 (2) |
| Survival time since 1st cancer (years) | 2.20; 4.04; 0.98; 723 | 1.85; 3.00; 0.88; 1576 | 0.075 (2) | 1.35; 1.44; 0.85; 653 | 1.30; 1.50; 0.78; 1424 | 0.228 (2) | 10.19; 8.93; 7.76; 70 | 7.02; 6.56; 5.12; 152 | 0.010 (2) | 1.31; 1.48; 0.80; 2077 | 8.02; 7.52; 5.61; 222 | 0.000 (2) |
| Total Survival Time | ||||
|---|---|---|---|---|
| Smoker | Ex-Smoker | Non-Smoker | ANOVA | |
| AVG; SD; M; n | AVG; SD; M; n | AVG; SD; M; n | p | |
| Women (2) | 64.49; 7.78; 64.06; 461 a B | 66.14; 8.40; 66.36; 194 a | 68.28; 11.74; 68.67; 69 B | 0.001 |
| Men (1) | 65.11; 8.05; 65.00; 1035 A B | 68.89; 8.05; 68.53; 484 A | 70.17; 10.17; 68.39; 58 B | 0.000 |
| Single neoplasm—general (2) | 64.78; 7.97; 64.63; 1392 A B | 67.63; 8.30; 67.33; 581 A | 68.46; 11.37; 68.25; 106 B | 0.000 |
| Single neoplasm—women (2) | 64.35; 7.71; 63.95; 428 a b | 66.05; 8.69; 66.33; 170 a | 67.40; 12.40; 67.35; 56 b | 0.002 |
| Single neoplasm—men (1) | 64.98; 8.07; 64.90; 964 A B | 68.28; 8.06; 67.85; 411 A | 69.65; 10.08; 69.65; 50 B | 0.000 |
| Multiple neoplasms—general (2) | 66.74; 7.77; 66.11; 104 A b | 70.96; 7.25; 71.51; 97 A | 72.58; 8.68; 69.64; 21 b | 0.000 |
| Multiple neoplasms—women (1) | 66.32; 8.48; 66.32; 33 | 66.82; 6.11; 66.79; 24 | 72.06; 7.54; 72.31; 13 | 0.065 |
| Multiple neoplasms—men (2) | 66.94; 7.47; 66.83; 71 A | 72.32; 7.11; 73.22; 73 A | 73.44; 10.79; 67.28; 8 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romaszko-Wojtowicz, A.; Lorenc, A.; Buciński, A.; Doboszyńska, A. Effects of Tobacco Smoking on the Survivability of Patients with Multiple Cancers and Single Lung Cancer. Int. J. Environ. Res. Public Health 2022, 19, 9179. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159179
Romaszko-Wojtowicz A, Lorenc A, Buciński A, Doboszyńska A. Effects of Tobacco Smoking on the Survivability of Patients with Multiple Cancers and Single Lung Cancer. International Journal of Environmental Research and Public Health. 2022; 19(15):9179. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159179
Chicago/Turabian StyleRomaszko-Wojtowicz, Anna, Andżelika Lorenc, Adam Buciński, and Anna Doboszyńska. 2022. "Effects of Tobacco Smoking on the Survivability of Patients with Multiple Cancers and Single Lung Cancer" International Journal of Environmental Research and Public Health 19, no. 15: 9179. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159179