
The Effectiveness of Interventions to Reduce Sedentary Time in Different Target Groups and Settings in Germany: Systematic Review, Meta-Analysis and Recommendations on Interventions


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
- Study design: included studies needed to be controlled intervention studies (e.g., randomized/non-randomized controlled studies, cross-over randomized/non-randomized studies, cluster randomized/non-randomized controlled studies, controlled before and after studies).
- Population: participants of all ages, with and without chronic diseases were included.
- Intervention: all types of interventions (interventions targeting the physical or social environment, personal behavior and multicomponent interventions) aiming at reducing sedentary time were deemed eligible, irrespective of whether sedentary time was the primary or secondary outcome.
- Control: any control condition was considered eligible; we included controls without intervention, waitlist controls and controls with an alternative intervention.
- Outcome: we included sedentary behavior across different domains of sitting or sedentary time.
- Setting: at least part of the intervention needed to have been implemented in Germany and results had to have been reported separately for Germany.
2.2. Search Strategy
2.3. Study Selection Process and Data Extraction
2.4. Data Synthesis
2.5. Risk of Bias Assessment
3. Results
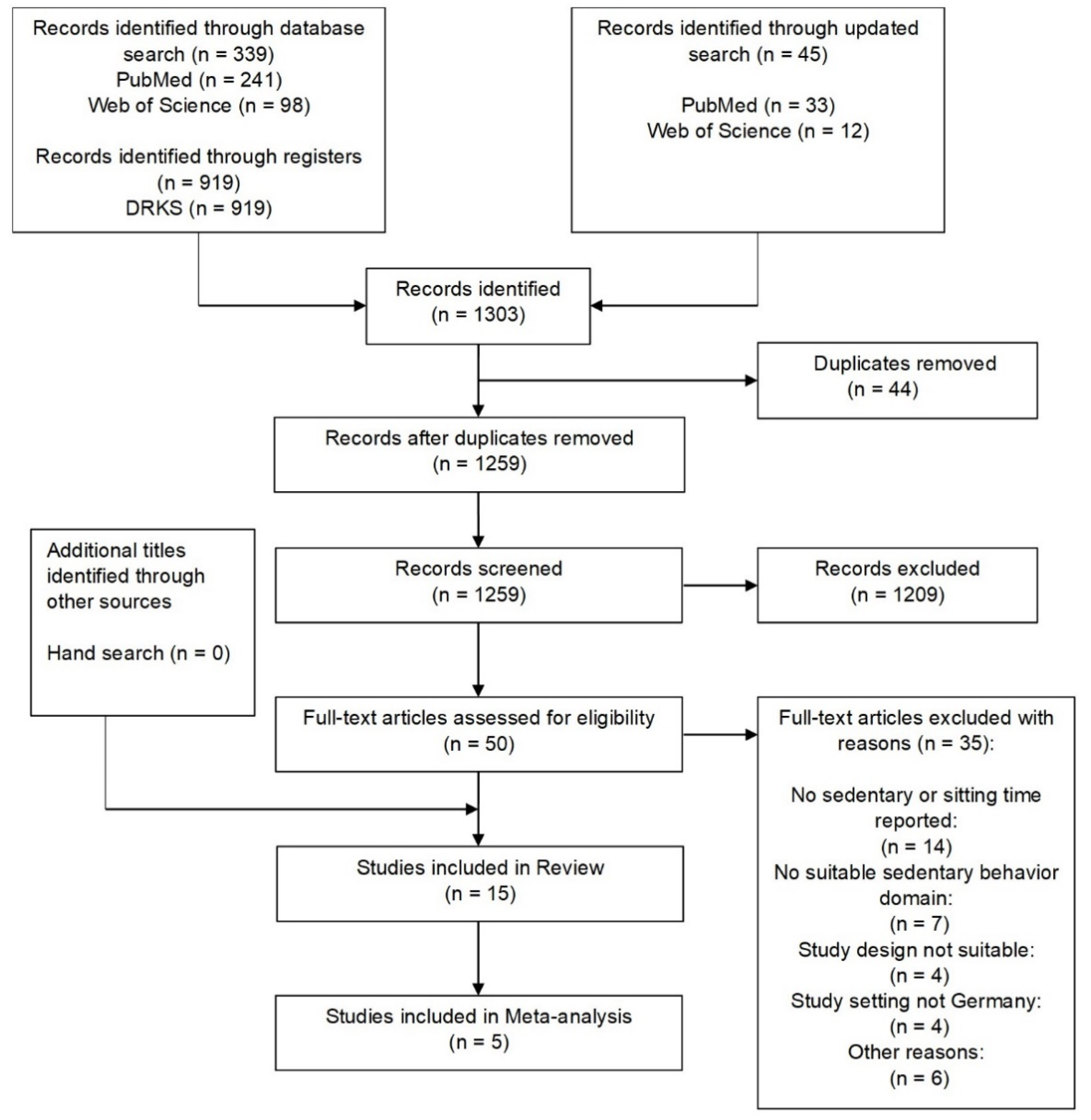
3.1. Study Selection
3.2. Risk of Bias Assessment
3.3. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
| Authors, Year, Funding Source, Trial Registry | Study Design, Health Promotion Program | Population | Intervention Duration, Follow-Up | Intervention Setting, Type of Intervention, Intervention Focus | Intervention Description | Control Condition | Assessment of Outcome, SB Outcomes |
|---|---|---|---|---|---|---|---|
| Children | |||||||
| Brandes et al., 2020 [88] Steenbock et al., 2017 [90] “ German health insurance AOK DRKS00011065 | Cluster non-RCT JolinchenKids (JOKITA; fit and healthy in daycare) | Preschoolers, n = 144, age range: 3–6 y IG: n = 67, mean age: 4.1 y, gender: 46.8% male, 53.2% female CG: n = 77, mean age: 4.3 y, gender: 49.4% male, 50.6% female | 1 year 1 year | Daycare based Multicomponent intervention PA | Five modules: three focused on children (one on PA, nutrition and mental well-being each), one on parents, one on DF staff PA module: instructions for PA games, aim to create movement-friendly areas in DF, additionally: parents received newsletter once yearly and participated in joint activities twice yearly | Wait list | Quantitative (GENEActiv device) Domain SB: total sedentary behavior (min/day) |
| De Bock et al., 2013 [75] Grant from Baden-Württemberg Stiftung * NCT00987532 | Cluster RCT Ene mene fit | Preschoolers, n = 528, age range: 4–6 y mean age: 5.05 y, gender: 52% boys, 48% girls IG: n = 248 CG: n = 280 | IG: 9 months CG: 6 months 6 months, 12 months | Daycare community based Multicomponent intervention PA | Non-participatory PA program: one-hour gym class (twice weekly over 6 months), one meeting of parents and gym class trainer Additionally: participatory intervention, incorporating parents, teachers and other preschool community members, website (www.ene-mene-fit.de (accessed on 2 July 2021)), introductory video, book with project ideas, gym trainers provided support to parents and preschool communities in implementing own interventions | Only non-participatory PA program | Quantitatve (Actiheart) Domain SB: total sedentary behavior (min/day) |
| Verbestel et al., 2015 [89] ** Ahrens et al., 2011 [91] “ n/a | Cluster non-RCT Identification and prevention of Dietary- and lifestyle-induced health EFfects In Children and infantS (IDEFICS) | Toddlers, preschoolers, school children, n = 1097, age range: 2–9.9 y | 2 years 2 years | Community, school and family based Multicomponent intervention SB/PA | Ten intervention modules:
| No intervention | Quantitative (ActiGraphTM GT1 M and ActiTrainerTM) Domain SB: total sedentary time (% of time) |
| Kobel et al., 2020 [78] Funded by Baden-Württemberg Foundation DRKS00000494 | Cluster RCT Join the Healthy Boat | School children, n = 154, age range: 5–8 y IG: n = 102, mean age: 7 y, gender: 48% male, 52% female CG: n = 52, mean age: 7 y, gender: 42.3% male, 57.7% female | 1 year 1 year | School based Multicomponent intervention PA/SB | Primary school teachers trained to conduct change towards movement-friendly school environment and to promote healthy and active lifestyle in lessons, implemented short exercises twice daily to break up SB, held teaching units once weekly (containing 20 lessons dealing with health-related topics, 13 focused on PA and SB). To encourage parental involvement: six family homework assignments, two parents´ nights, additionally: parents received five letters (three were dealing with PA and SB) | No intervention, continued usual school curriculum | Quantitative (Actiheart) Domain SB: total sedentary time total week (min/day) Sedentary time weekdays (min/day) Sedentary time weekend (min/day) |
| Sprengeler et al., 2020 [87] City of Ludwigsburg: height-adjustable standing desks, publication of article funded * | Cross-over RCT n/a | School children, n = 37, Age range: 8–10 y mean age: 8.4 y, gender: 38.5% boys, 61.5% girls G1: n = 19 G2: n = 18 | 2 weeks (each for G1, G2) 2 weeks, 9.43 weeks | School based Physical environment SB | First G1 received height-adjustable standing desks and G2 served as control. After washout period, G2 used height-adjustable standing desks and G1 served as control | Respective group serving as control used traditional working desks | Quantitative (activPAL inclinometer) Domain SB: total, school, leisure time Sitting time (min/day) Sitting time (% of total time during lessons, % of total time during breaks, % of total time during leisure time) |
| Suchert et al., 2015 [76] German Cancer Aid: Primary Prevention of Cancer ISRCTN49482118 | Cluster RCT läuft | Teenagers, n = 1162, age range: 12–17 y IG: n = 702, mean age: 13.7 y, gender: 52.7% male, 47.3% female CG: n = 460, mean age: 13.79 y, gender: 50.9% male, 49.1% female | 12 weeks 12 weeks | School based Multicomponent intervention PA | Pedometers, could record and compare their steps on “läuft” homepage Classes participated in two competitions, attended educational lessons, schools and parents received information material | Regular education | Qualitative (survey) Domain SB: total sedentary behavior (h/day) |
| Adults | |||||||
| Voigt et al., 2018 [70] Federal Ministry of Education and Research NCT02990039 | RCT n/a | Adults, n = 138, age range: 40–65 y, mean age: 54.5, gender: 35.9% male, 64.1% female IG1: n = 69 IG2: n = 69 | 4 months (after split of IG1 and IG2) 1 month, 6 months, 12 months | Home based Personal behavior PA/SB | During first month, IG1 and IG2 were not split up, had an assessment only After separation: IG1 received letters at month 1, 3, 4 (letters were tailored via self-report assessing personal PA and SB behavior) | After separation, participants in IG2 received no letters (only assessed their PA and SB behavior via self-report) | Qualitative (IPAQ) Domain SB: total overall sedentary time (hours/week and sqrt min/week) |
| Livingstone et al., 2020 [72] ** Work supported by European Commission under the Food, Agriculture, Fisheries and Biotechnology Theme * NCT01530139 | RCT Food4Me | Adults IG: n = 63 | 6 months 6 months | Web based Personal behavior PA | Participants randomized to intervention groups L1–L3, all participants received personalized dietary and PA advice but based on different sources (tailored feedback reports at baseline, month three, month six) L1: advised based on current PA and diet L2: additionally advised based on phenotypic data L3: additionally advice based on phenotypic and genotypic data | General (non-personalized) dietary and PA advice | Quantitative (triaxial accelerometer (Tracmor D)) Domain SB: total % of participants benefiting from the intervention (>5% reduction concerning sedentary time from baseline to month 6) |
| Ellegast et al., 2012 [85] German Social Accident Insurance (DGUV) | RCT n/a | Office workers, n = 25, gender: 76% male, 24% female IG: n = 13 CG: n = 12 | 12 weeks 12 weeks | Work based Multicomponent intervention PA/SB | Intervention at the workplace (office), intervention included sit–stand tables, pedometers, face-to-face motivation for, e.g., lunch walks, incentives for bicycle commuting/sports activities | No intervention | Qualitative (activity log), quantitative (CUELA Activity System) Domain SB: office sitting time (min/day) Tasks carried out sitting (%) |
| Pischke et al., 2022 [77] Federal Ministry of Education and Research (project 01EL1822A, 01EL1822F, 01EL1822l and 01EL1822C) DRKS00016073 | Cross-over randomized trial PROMOTE II | Older adults, n = 160, age range: 60–82y IG1 (WEB): n = 59, mean age: 67.9 y, gender: 36% male, 64% female IG2 (WEB+): n = 22, mean age: 70.5 y, gender: 53% male, 47% female IG3 (PRINT): n = 79, mean age: 67.6 y, gender: 24% male, 76% female | 9 months 3 months 9 months | Web and community based Personal behavior PA | WEB intervention group: online WHO PA recommendations, online brochures with instructions for exercises, online PA diary with weekly feedback, smartphone app with additional access to PA diary and exercises, additionally: 90 min weekly group session for 10 weeks After 10 weeks, participants had the option to cross over to another group, then group sessions continued once per month for 6 months WEB+ intervention group: same intervention and intervention materials online as participants in WEB group, additionally: PA tracker | PRINT group: same intervention and intervention materials as participants in WEB and WEB+ group but in printed form, did not receive PA tracker | Quantitative (GT3 x+) Domain SB: total sedentary time (min/day) Sedentary time in 30 min bouts (min/week) |
| Muellmann et al., 2019 [71] German Federal Ministry of Education and Research DRKS00010052 | RCT PROMOTE study | Older adults, n = 405, age range: 62–79 y IG1: n = 146, mean age: 69.6 y, gender: 46.2% men, 53.8% women IG2: n = 119, mean age: 69.6 y, gender: 41.3% men, 58.7% women CG: n = 140, mean age: 69.8 y, gender: 42.6% men, 57.4% women | 10 weeks, 12 weeks | Web and community based Personal behavior PA | IG1: Access to website, weekly group meetings in their community led by trained staff, additionally: instruction brochures tailored to their PA levels and gender, were instructed to exercise regularly Functions of the website: track PA, weekly feedback on predetermined PA goals, online rewards if goals were reached, option to contact other participants IG2: Same intervention as IG1, additionally: Fitbit Zip | Delayed intervention (access to web-based PA intervention, but did not receive Fitbit or group meetings) | Quantitative (ActiGraph GT3 X+) Domain SB: total sedentary time (min/day) Sedentary time in 30 min bouts (min/week) |
| Kleinke et al., 2021 [69] Federal Ministry of Education and Research (funding sign: 81Z7400174) DRKS00010410 | RCT Motivation-Oriented intervention study for the elderly in Greifswald (MOVING-study) | Older adults, n = 166 IG: n = 85, mean age: 70.4 y, gender: 41.2% male, 58.8% female CG: n = 81, mean age: 71.2 y, gender: 42% male, 58% female | 14 weeks 3 months 6 months | Home based Personal behavior PA/SB | Personalized feedback (based on accelerometer data) regarding their PA and SB via mail (after baseline and the 3-month follow-up examination), additionally: WHO PA recommendations | Did not receive any intervention, but received feedback concerning their accelerometer data after end of study | Quantitative (ActiGraph GT3 x-BT) Domain SB: total sedentary time (min/week) |
| Salchow et al., 2021 [73] Authors received no funding DRKS00009453 | RCT Motivate Adolescent and Young Adults (MAYA) | Adults, people with chronic diseases (cancer survivors), n = 69, age range: 15–39 y IG: n = 36, mean age: 23.4 y, gender: 36.1% male, 63.9% female CG: n = 33, mean age: 25.3 y, gender: 48.5% male, 51.5% female | 12 weeks 12 weeks 52 weeks | Home based Personal behavior PA | Sixty minutes of personally tailored PA counselling, containing a PA anamnesis and the development of a personalized PA plan, additionally: PA guidelines for cancer survivors and list with local opportunities for PA | Usual care (consisting of the PA guidelines for cancer survivors) | Qualitative (IPAQ) Domain SB: total sitting (hours/day) |
| Geidl et al., 2021 [74] German Pension Insurance * NCT02966561 | RCT Stay Active after Rehabilitation (STAR) | Adults, people with chronic diseases (COPD), n = 327 IG: n = 167, mean age: 58.01 y, gender: 68.7% male, 31.3% female CG: n = 160, mean age: 58.03 y, gender: 69.4% male, 30.6% female | 3 weeks 11 weeks 31 weeks | Stationary rehabilitation Personal behavior PA | Three-week stationary pulmonal rehabilitation, additionally, pedometer and two 45 min PA lessons | Same 3-week stationary rehabilitation as intervention group, instead of pedometer and PA lessons: repetition of PA information twice for 45 min | Quantitative (ActiGraph wGT3X) Domain SB: total sedentary time (min/day) |
| Wagner et al., 2019 [86] German Social Accident Insurance (DGUV) DRKS00010777 | RCT n/a | Adults, people with chronic diseases (occupational respiratory diseases), n = 137, age range: 45–80 y, mean age: 69.1 y, gender: 95.9% male, 4.1% female IG: n = 67 CG: n = 70 | IG: 7 weeks CG: 4 weeks 4.53 months 8.53 months 14.53 months | Stationary rehabilitation Personal behavior PA | Standardized stationary rehabilitation (similarly to CG) and additional behavior-orientated movement intervention (three weeks, contained three 45 min group sessions per week, tailored work folder with tasks) | Four-week stationary, standardized rehabilitation (included personally tailored interventions and activities) | Quantitative (Actigraph GT3 x) Domain SB: total sedentary behavior (min/day) |
3.4. Description and Effectiveness of Interventions
3.4.1. Adults
3.4.2. Children and Adolescents
3.5. Meta-Analysis
4. Discussion
4.1. Recommendations to Effectively Reduce Sitting Time in Germany
4.2. Strengths and Limitations
4.3. Implications for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Salahuddin, U.; Garg, S.; Ayers, C.; Kulinski, J.; Anand, V.; Mayo, H.; Kumbhani, D.J.; de Lemos, J.; Berry, J.D. Continuous Dose-Response Association Between Sedentary Time and Risk for Cardiovascular Disease: A Meta-analysis. JAMA Cardiol. 2016, 1, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.P.; Hewson, D.J.; Champion, R.B.; Sayegh, S.M. Sitting Time and Risk of Cardiovascular Disease and Diabetes: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2019, 57, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Zhou, Q.; Zhang, D.; Qin, P.; Li, Q.; Tian, G.; Liu, D.; Chen, X.; Liu, L.; Liu, F.; et al. Association of total sedentary behaviour and television viewing with risk of overweight/obesity, type 2 diabetes and hypertension: A dose-response meta-analysis. Diabetes Obes. Metab. 2020, 22, 79–90. [Google Scholar] [CrossRef]
- Patterson, R.; McNamara, E.; Tainio, M.; de Sá, T.H.; Smith, A.D.; Sharp, S.J.; Edwards, P.; Woodcock, J.; Brage, S.; Wijndaele, K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur. J. Epidemiol. 2018, 33, 811–829. [Google Scholar] [CrossRef]
- Hermelink, R.; Leitzmann, M.F.; Markozannes, G.; Tsilidis, K.; Pukrop, T.; Berger, F.; Baurecht, H.; Jochem, C. Sedentary behavior and cancer-an umbrella review and meta-analysis. Eur. J. Epidemiol. 2022, 37, 447–460. [Google Scholar] [CrossRef]
- Shen, D.; Mao, W.; Liu, T.; Lin, Q.; Lu, X.; Wang, Q.; Lin, F.; Ekelund, U.; Wijndaele, K. Sedentary behavior and incident cancer: A meta-analysis of prospective studies. PLoS ONE 2014, 9, e105709. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Wu, X.Y.; Han, L.H.; Zhang, J.H.; Luo, S.; Hu, J.W.; Sun, K. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: A systematic review. PLoS ONE 2017, 12, e0187668. [Google Scholar] [CrossRef]
- Copeland, J.L.; Ashe, M.C.; Biddle, S.J.; Brown, W.J.; Buman, M.P.; Chastin, S.; Gardiner, P.A.; Inoue, S.; Jefferis, B.J.; Oka, K.; et al. Sedentary time in older adults: A critical review of measurement, associations with health, and interventions. Br. J. Sports Med. 2017, 51, 1539. [Google Scholar] [CrossRef]
- Huang, Y.; Li, L.; Gan, Y.; Wang, C.; Jiang, H.; Cao, S.; Lu, Z. Sedentary behaviors and risk of depression: A meta-analysis of prospective studies. Transl. Psychiatry 2020, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.; Zhang, Y.; Zhang, D. Sedentary behaviour and the risk of depression: A meta-analysis. Br. J. Sports Med. 2015, 49, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Bu, W.; Chen, Y.; Chen, X. The Dose-Response Associations of Sedentary Time with Chronic Diseases and the Risk for All-Cause Mortality Affected by Different Health Status: A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2020, 24, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Heron, L.; O’Neill, C.; McAneney, H.; Kee, F.; Tully, M.A. Direct healthcare costs of sedentary behaviour in the UK. J. Epidemiol. Community Health 2019, 73, 625–629. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Mayo, X.; Liguori, G.; Copeland, R.J.; Lamb, M.; Jimenez, A. Changes in sedentary behaviour in European Union adults between 2002 and 2017. BMC Public Health 2020, 20, 1206. [Google Scholar] [CrossRef]
- Yang, L.; Cao, C.; Kantor, E.D.; Nguyen, L.H.; Zheng, X.; Park, Y.; Giovannucci, E.L.; Matthews, C.E.; Colditz, G.A.; Cao, Y. Trends in Sedentary Behavior Among the US Population, 2001–2016. JAMA 2019, 321, 1587–1597. [Google Scholar] [CrossRef]
- Froböse, I.; Wallmann, B. DKV-Report “Wie Gesund Lebt Deutschland?” 2012. Available online: https://www.dkv.com/downloads/DKV-Report-2012.pdf (accessed on 26 October 2021).
- Froböse, I.; Biallas, B.; Wallmann-Sperlich, B. Der DKV-Report 2018: Wie Gesund Lebt Deutschland? Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwia3rH3kejzAhXQGewKHb9aAXAQFnoECBQQAQ&url=https%3A%2F%2Fwww1.wdr.de%2Fnachrichten%2Fdkv-gesundheitsreport-102.pdf&usg=AOvVaw3QPlaNKdLG_U_Oet0SP4qN (accessed on 26 October 2021).
- Harvey, J.A.; Chastin, S.F.M.; Skelton, D.A. How Sedentary are Older People? A Systematic Review of the Amount of Sedentary Behavior. J. Aging Phys. Act. 2015, 23, 471–487. [Google Scholar] [CrossRef]
- Bauman, A.E.; Petersen, C.B.; Blond, K.; Rangul, V.; Hardy, L.L. The Descriptive Epidemiology of Sedentary Behaviour. In Sedentary Behaviour Epidemiology; Leitzmann, M.F., Jochem, C., Schmid, D., Eds.; Springer International Publishing: Cham, Switerland, 2018; pp. 73–106. ISBN 978-3-319-61552-3. [Google Scholar]
- Lam, K.; Baurecht, H.; Pahmeier, K.; Niemann, A.; Romberg, C.; Biermann-Stallwitz, J.; Neusser, S.; Wasem, J.; Mugler, N.; Welker, C.; et al. How effective and how expensive are interventions to reduce sedentary behavior? An umbrella review and meta-analysis. Obes. Rev. 2022, 23, e13422. [Google Scholar] [CrossRef]
- Ludwig, K.; Arthur, R.; Sculthorpe, N.; Fountain, H.; Buchan, D.S. Text Messaging Interventions for Improvement in Physical Activity and Sedentary Behavior in Youth: Systematic Review. Jmir Mhealth Uhealth 2018, 6, e10799. [Google Scholar] [CrossRef]
- Langford, R.; Bonell, C.P.; Jones, H.E.; Pouliou, T.; Murphy, S.M.; Waters, E.; Komro, K.A.; Gibbs, L.F.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst. Rev. 2014, 16, CD008958. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.; Kukkonen-Harjula, K.T.; Verbeek, J.H.; Ijaz, S.; Hermans, V.; Pedisic, Z. Workplace interventions for reducing sitting at work. Cochrane Database Syst. Rev. 2018, 12, CD010912. [Google Scholar] [CrossRef] [PubMed]
- Eurofound 2017. Sixth European Working Conditions Survey: Overview Report (2017 Update). Available online: https://www.eurofound.europa.eu/de/publications/report/2016/working-conditions/sixth-european-working-conditions-survey-overview-report (accessed on 26 October 2021).
- Eurostat. Living Conditions in Europe: 2018 Edition. Available online: https://ec.europa.eu/eurostat/web/products-statistical-books/-/KS-DZ-18-001 (accessed on 26 October 2021).
- OECD 2022. Hours Worked (Indicator). Available online: https://data.oecd.org/emp/hours-worked.htm (accessed on 4 August 2022).
- Steene-Johannessen, J.; Hansen, B.H.; Dalene, K.E.; Kolle, E.; Northstone, K.; Møller, N.C.; Grøntved, A.; Wedderkopp, N.; Kriemler, S.; Page, A.S.; et al. Variations in accelerometry measured physical activity and sedentary time across Europe—harmonized analyses of 47,497 children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 38. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. 2021. Available online: https://www.R-project.org/ (accessed on 12 August 2022).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Brehm, W.; Wagner, P.; Sygusch, R.; Schönung, A.; Hahn, U. Health promotion by means of health sport—A framework and a controlled intervention study with sedentary adults. Scand. J. Med. Sci. Sports 2005, 15, 13–20. [Google Scholar] [CrossRef]
- Franke, K.-J.; Domanski, U.; Schroeder, M.; Jansen, V.; Artmann, F.; Weber, U.; Ettler, R.; Nilius, G. Telemonitoring of home exercise cycle training in patients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 2821–2829. [Google Scholar] [CrossRef]
- Gába, A.; Cuberek, R.; Svoboda, Z.; Chmelík, F.; Pelclová, J.; Lehnert, M.; Frömel, K. The effect of brisk walking on postural stability, bone mineral density, body weight and composition in women over 50 years with a sedentary occupation: A randomized controlled trial. BMC Womens. Health 2016, 16, 63. [Google Scholar] [CrossRef]
- Hötting, K.; Schauenburg, G.; Röder, B. Long-term effects of physical exercise on verbal learning and memory in middle-aged adults: Results of a one-year follow-up study. Brain Sci. 2012, 2, 332–346. [Google Scholar] [CrossRef]
- Kemmler, W.; Kohl, M.; Fröhlich, M.; Jakob, F.; Engelke, K.; von Stengel, S.; Schoene, D. Effects of High-Intensity Resistance Training on Osteopenia and Sarcopenia Parameters in Older Men with Osteosarcopenia-One-Year Results of the Randomized Controlled Franconian Osteopenia and Sarcopenia Trial (FrOST). J. Bone Miner. Res. 2020, 35, 1634–1644. [Google Scholar] [CrossRef] [PubMed]
- Konradt, U.; Heblich, F.; Krys, S.; Garbers, Y.; Otte, K.-P. Beneficial, adverse, and spiraling health-promotion effects: Evidence from a longitudinal randomized controlled trial of working at sit-stand desks. J. Occup. Health Psychol. 2020, 25, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Kraushaar, L.E.; Krämer, A. Web-enabled feedback control over energy balance promotes an increase in physical activity and a reduction of body weight and disease risk in overweight sedentary adults. Prev. Sci. 2014, 15, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Stenner, H.T.; Eigendorf, J.; Kerling, A.; Kueck, M.; Hanke, A.A.; Boyen, J.; Nelius, A.-K.; Melk, A.; Boethig, D.; Bara, C.; et al. Effects of six month personalized endurance training on work ability in middle-aged sedentary women: A secondary analysis of a randomized controlled trial. J. Occup. Med. Toxicol. 2020, 15, 8. [Google Scholar] [CrossRef]
- Streber, A.; Abu-Omar, K.; Hentschke, C.; Rütten, A. A multicenter controlled study for dementia prevention through physical, cognitive and social activities—GESTALT-kompakt. Clin. Interv. Aging 2017, 12, 2109–2121. [Google Scholar] [CrossRef]
- Wolff, J.K.; Warner, L.M.; Ziegelmann, J.P.; Wurm, S. What do targeting positive views on ageing add to a physical activity intervention in older adults? Results from a randomised controlled trial. Psychol. Health 2014, 29, 915–932. [Google Scholar] [CrossRef]
- Peters, S.; Hentschke, C.; Pfeifer, K. Internet-based “e-training” as exercise intervention for health promotion: Results from 2 intervention studies. Rehabilitation 2013, 52, 173–181. [Google Scholar] [CrossRef]
- Pressler, A.; Knebel, U.; Esch, S.; Kölbl, D.; Esefeld, K.; Scherr, J.; Haller, B.; Schmidt-Trucksäss, A.; Krcmar, H.; Halle, M.; et al. An internet-delivered exercise intervention for workplace health promotion in overweight sedentary employees: A randomized trial. Prev. Med. 2010, 51, 234–239. [Google Scholar] [CrossRef]
- Reljic, D.; Wittmann, F.; Fischer, J.E. Effects of low-volume high-intensity interval training in a community setting: A pilot study. Eur. J. Appl. Physiol. 2018, 118, 1153–1167. [Google Scholar] [CrossRef]
- Reljic, D.; Frenk, F.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Low-volume high-intensity interval training improves cardiometabolic health, work ability and well-being in severely obese individuals: A randomized-controlled trial sub-study. J. Transl. Med. 2020, 18, 419. [Google Scholar] [CrossRef]
- de Bourdeaudhuij, I.; Verbestel, V.; de Henauw, S.; Maes, L.; Huybrechts, I.; Mårild, S.; Eiben, G.; Moreno, L.A.; Barba, G.; Kovács, É.; et al. Behavioural effects of a community-oriented setting-based intervention for prevention of childhood obesity in eight European countries. Main results from the IDEFICS study. Obes. Rev. 2015, 16 (Suppl. 2), 30–40. [Google Scholar] [CrossRef] [PubMed]
- Knaus, M.C.; Lechner, M.; Reimers, A.K. For better or worse?—The effects of physical education on child development. Labour Econ. 2020, 67, 101904. [Google Scholar] [CrossRef]
- Kobel, S.; Lämmle, C.; Wartha, O.; Kesztyüs, D.; Wirt, T.; Steinacker, J.M. Effects of a Randomised Controlled School-Based Health Promotion Intervention on Obesity Related Behavioural Outcomes of Children with Migration Background. J. Immigr. Minor. Health 2017, 19, 254–262. [Google Scholar] [CrossRef]
- Latomme, J.; Cardon, G.; de Bourdeaudhuij, I.; Iotova, V.; Koletzko, B.; Socha, P.; Moreno, L.; Androutsos, O.; Manios, Y.; de Craemer, M. Effect and process evaluation of a kindergarten-based, family-involved intervention with a randomized cluster design on sedentary behaviour in 4- to 6- year old European preschool children: The ToyBox-study. PLoS ONE 2017, 12, e0172730. [Google Scholar] [CrossRef]
- Liersch, S.; Henze, V.; Sterdt, E.; Sayed, M.; Röbl, M.; Schnitzerling, J.; Suermann, T.; Mayr, E.; Krauth, C.; Walter, U. Effectiveness and Cost-Effectiveness of Daily School Sport in the Primary School--Project: “fit for pisa”. Gesundheitswesen 2015, 77 (Suppl. 1), S72–S73. [Google Scholar] [CrossRef] [PubMed]
- Miguel-Berges, M.L.; Santaliestra-Pasias, A.M.; Mouratidou, T.; Flores-Barrantes, P.; Androutsos, O.; de Craemer, M.; Galcheva, S.; Koletzko, B.; Kulaga, Z.; Manios, Y.; et al. Parental perceptions, attitudes and knowledge on European preschool children’s total screen time: The ToyBox-study. Eur. J. Public Health 2020, 30, 105–111. [Google Scholar] [CrossRef]
- Siegrist, M.; Schönfeld, J. Körperliche Fitness und Gesundheitsverhalten von Kindern in fit4future- Schulen: Abschlussbericht nach drei Projektjahren in den Phase-1-Schulen (Zeitraum 2016 bis 2019). Available online: https://www.dak.de/dak/download/bericht-2237170.pdf (accessed on 10 November 2021).
- Smith, M.P.; Berdel, D.; Nowak, D.; Heinrich, J.; Schulz, H. Physical Activity Levels and Domains Assessed by Accelerometry in German Adolescents from GINIplus and LISAplus. PLoS ONE 2016, 11, e152217. [Google Scholar] [CrossRef]
- Rank, M.; Wilks, D.C.; Foley, L.; Jiang, Y.; Langhof, H.; Siegrist, M.; Halle, M. Health-Related Quality of Life and Physical Activity in Children and Adolescents 2 Years after an Inpatient Weight-Loss Program. J. Pediatr. 2014, 165, 732–737. [Google Scholar] [CrossRef]
- Schwarzfischer, P.; Gruszfeld, D.; Stolarczyk, A.; Ferre, N.; Escribano, J.; Rousseaux, D.; Moretti, M.; Mariani, B.; Verduci, E.; Koletzko, B.; et al. Physical Activity and Sedentary Behavior from 6 to 11 Years. Pediatrics 2019, 143, e20180994. [Google Scholar] [CrossRef]
- Schwenk, M.; Bergquist, R.; Boulton, E.; van Ancum, J.M.; Nerz, C.; Weber, M.; Barz, C.; Jonkman, N.H.; Taraldsen, K.; Helbostad, J.L.; et al. The Adapted Lifestyle-Integrated Functional Exercise Program for Preventing Functional Decline in Young Seniors: Development and Initial Evaluation. Gerontology 2019, 65, 362–374. [Google Scholar] [CrossRef]
- Szczuka, Z.; Kulis, E.; Boberska, M.; Banik, A.; Kruk, M.; Keller, J.; Knoll, N.; Scholz, U.; Abraham, C.; Luszczynska, A. Can individual, dyadic, or collaborative planning reduce sedentary behavior? A randomized controlled trial. Soc. Sci. Med. 2021, 287, 114336. [Google Scholar] [CrossRef]
- Zusman, E.Z.; Dawes, M.; Fleig, L.; McAllister, M.M.; Cook, W.L.; Guy, P.; Brasher, P.M.A.; McKay, H.A.; Khan, K.M.; Ashe, M.C. Older Adults’ Sedentary Behavior and Physical Activity After Hip Fracture: Results from an Outpatient Rehabilitation Randomized Controlled Trial. J. Geriatr. Phys. Ther. 2019, 42, E32–E38. [Google Scholar] [CrossRef] [PubMed]
- Notthoff, N.; Klomp, P.; Doerwald, F.; Scheibe, S. Positive messages enhance older adults’ motivation and recognition memory for physical activity programmes. Eur. J. Ageing 2016, 13, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Noz, M.P.; Hartman, Y.A.W.; Hopman, M.T.E.; Willems, P.H.G.M.; Tack, C.J.; Joosten, L.A.B.; Netea, M.G.; Thijssen, D.H.J.; Riksen, N.P. Sixteen-Week Physical Activity Intervention in Subjects with Increased Cardiometabolic Risk Shifts Innate Immune Function Towards a Less Proinflammatory State. J. Am. Heart Assoc. 2019, 8, e013764. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.; Schmidt, S.; Neuberger, E.W.I.; Kirsch, P.; Simon, P.; Dettweiler, U. Children’s Cortisol and Cell-Free DNA Trajectories in Relation to Sedentary Behavior and Physical Activity in School: A Pilot Study. Front. Public Health 2019, 7, 26. [Google Scholar] [CrossRef]
- Ludwig, O.; Kelm, J.; Hammes, A.; Schmitt, E.; Fröhlich, M. Targeted Athletic Training Improves the Neuromuscular Performance in Terms of Body Posture From Adolescence to Adulthood—Long-Term Study Over 6 Years. Front. Physiol. 2018, 9, 1620. [Google Scholar] [CrossRef]
- Marschin, V.; Herbert, C. A Short, Multimodal Activity Break Incorporated Into the Learning Context During the COVID–19 Pandemic: Effects of Physical Activity and Positive Expressive Writing on University Students’ Mental Health-Results and Recommendations From a Pilot Study. Front. Psychol. 2021, 12, 645492. [Google Scholar] [CrossRef]
- Vik, F.N.; Lien, N.; Berntsen, S.; de Bourdeaudhuij, I.; Grillenberger, M.; Manios, Y.; Kovacs, E.; Chinapaw, M.J.M.; Brug, J.; Bere, E. Evaluation of the UP4FUN intervention: A cluster randomized trial to reduce and break up sitting time in European 10-12-year-old children. PLoS ONE 2015, 10, e0122612. [Google Scholar] [CrossRef]
- Wang, Y.; König, L.M.; Reiterer, H. A Smartphone App to Support Sedentary Behavior Change by Visualizing Personal Mobility Patterns and Action Planning (SedVis): Development and Pilot Study. JMIR Form. Res. 2021, 5, e15369. [Google Scholar] [CrossRef]
- Ratz, T.; Pischke, C.R.; Voelcker-Rehage, C.; Lippke, S. Distinct physical activity and sedentary behavior trajectories in older adults during participation in a physical activity intervention: A latent class growth analysis. Eur. Rev. Aging Phys. Act. 2022, 19, 1. [Google Scholar] [CrossRef]
- Kleinke, F.; Ulbricht, S.; Dorr, M.; Penndorf, P.; Hoffmann, W.; van den Berg, N. A low-threshold intervention to increase physical activity and reduce physical inactivity in a group of healthy elderly people in Germany: Results of the randomized controlled MOVING study. PLoS ONE 2021, 16, e257326. [Google Scholar] [CrossRef] [PubMed]
- Voigt, L.; Baumann, S.; Ullrich, A.; Weymar, F.; John, U.; Ulbricht, S. The effect of mere measurement from a cardiovascular examination program on physical activity and sedentary time in an adult population. BMC Sports Sci. Med. Rehabil. 2018, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Muellmann, S.; Buck, C.; Voelcker-Rehage, C.; Bragina, I.; Lippke, S.; Meyer, J.; Peters, M.; Pischke, C.R. Effects of two web-based interventions promoting physical activity among older adults compared to a delayed intervention control group in Northwestern Germany: Results of the PROMOTE community-based intervention trial. Prev. Med. Rep. 2019, 15, 100958. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, K.M.; Celis-Morales, C.; Navas-Carretero, S.; San-Cristobal, R.; Forster, H.; Woolhead, C.; O’Donovan, C.B.; Moschonis, G.; Manios, Y.; Traczyk, I.; et al. Characteristics of participants who benefit most from personalised nutrition: Findings from the pan-European Food4Me randomised controlled trial. Br. J. Nutr. 2020, 123, 1396–1405. [Google Scholar] [CrossRef]
- Salchow, J.; Koch, B.; Mann, J.; von Grundherr, J.; Elmers, S.; Dwinger, S.; Escherich, G.; Vettorazzi, E.; Reer, R.; Sinn, M.; et al. Effects of a structured counselling-based intervention to improve physical activity behaviour of adolescents and young adult cancer survivors—The randomized phase II Motivate AYA—MAYA trial. Clin. Rehabil. 2021, 35, 1164–1174. [Google Scholar] [CrossRef]
- Geidl, W.; Carl, J.; Schuler, M.; Mino, E.; Lehbert, N.; Wittmann, M.; Pfeifer, K.; Schultz, K. Long-Term Benefits of Adding a Pedometer to Pulmonary Rehabilitation for COPD: The Randomized Controlled STAR Trial. Int. J. Chron. Obstruct. Pulmon. Dis. 2021, 16, 1977–1988. [Google Scholar] [CrossRef]
- de Bock, F.; Genser, B.; Raat, H.; Fischer, J.E.; Renz-Polster, H. A participatory physical activity intervention in preschools: A cluster randomized controlled trial. Am. J. Prev. Med. 2013, 45, 64–74. [Google Scholar] [CrossRef]
- Suchert, V.; Isensee, B.; Sargent, J.; Weisser, B.; Hanewinkel, R. Prospective effects of pedometer use and class competitions on physical activity in youth: A cluster-randomized controlled trial. Prev. Med. 2015, 81, 399–404. [Google Scholar] [CrossRef]
- Pischke, C.R.; Voelcker-Rehage, C.; Ratz, T.; Peters, M.; Buck, C.; Meyer, J.; von Holdt, K.; Lippke, S. Web-Based Versus Print-Based Physical Activity Intervention for Community-Dwelling Older Adults: Crossover Randomized Trial. JMIR Mhealth Uhealth 2022, 10, e32212. [Google Scholar] [CrossRef]
- Kobel, S.; Dreyhaupt, J.; Wartha, O.; Kettner, S.; Hoffmann, B.; Steinacker, J.M. Intervention Effects of the Health Promotion Programme “Join the Healthy Boat” on Objectively Assessed Sedentary Time in Primary School Children in Germany. Int. J. Environ. Res. Public Health 2020, 17, 9029. [Google Scholar] [CrossRef]
- Kleinke, F.; Schwaneberg, T.; Weymar, F.; Penndorf, P.; Ulbricht, S.; Lehnert, K.; Doerr, M.; Hoffmann, W.; van den Berg, N. MOVING: Motivation-Oriented interVention study for the elderly IN Greifswald: Study protocol for a randomized controlled trial. Trials 2018, 19, 57. [Google Scholar] [CrossRef] [PubMed]
- Geidl, W.; Semrau, J.; Streber, R.; Lehbert, N.; Wingart, S.; Tallner, A.; Wittmann, M.; Wagner, R.; Schultz, K.; Pfeifer, K. Effects of a brief, pedometer-based behavioral intervention for individuals with COPD during inpatient pulmonary rehabilitation on 6-week and 6-month objectively measured physical activity: Study protocol for a randomized controlled trial. Trials 2017, 18, 396. [Google Scholar] [CrossRef] [PubMed]
- de Bock, F.; Fischer, J.E.; Hoffmann, K.; Renz-Polster, H. A participatory parent-focused intervention promoting physical activity in preschools: Design of a cluster-randomized trial. BMC Public Health 2010, 10, 49. [Google Scholar] [CrossRef]
- Dreyhaupt, J.; Koch, B.; Wirt, T.; Schreiber, A.; Brandstetter, S.; Kesztyues, D.; Wartha, O.; Kobel, S.; Kettner, S.; Prokopchuk, D.; et al. Evaluation of a health promotion program in children: Study protocol and design of the cluster-randomized Baden-Wurttemberg primary school study [DRKS-ID: DRKS00000494]. BMC Public Health 2012, 12, 157. [Google Scholar] [CrossRef] [PubMed]
- Suchert, V.; Isensee, B.; Hansen, J.; Johannsen, M.; Krieger, C.; Müller, K.; Sauer, I.; Weisser, B.; Sargent, J.D.; Hanewinkel, R. “läuft.”—A school-based multi-component program to establish a physically active lifestyle in adolescence: Study protocol for a cluster-randomized controlled trial. Trials 2013, 14, 416. [Google Scholar] [CrossRef]
- Pischke, C.R.; Voelcker-Rehage, C.; Peters, M.; Ratz, T.; Pohlabeln, H.; Meyer, J.; von Holdt, K.; Lippke, S. Implementation and Effects of Information Technology-Based and Print-Based Interventions to Promote Physical Activity Among Community-Dwelling Older Adults: Protocol for a Randomized Crossover Trial. JMIR Res. Protoc. 2020, 9, e15168. [Google Scholar] [CrossRef]
- Ellegast, R.; Weber, B.; Mahlberg, R. Method inventory for assessment of physical activity at VDU workplaces. Work 2012, 41 (Suppl. 1), 2355–2359. [Google Scholar] [CrossRef]
- Wagner, P.; Gimpel, C.; Müller, K.; Noack, E.; Bieber, S.; König, S. Abschlussbericht zum Vorhaben “Entwicklung und Evaluation Einer Verhaltensorientierten Bewegungsintervention zur Aufrechterhaltung der Körperlichen Aktivität Sowie Deren Wirkung auf die Psychische Gesundheit von Patienten*Innen Mit Berufsbedingten Lungen- und Atemwegserkrankungen in Kooperation mit der BG Klinik für Berufskrankheiten Falkenstein”. Available online: https://docplayer.org/185947303-Abschlussbericht-zum-vorhaben.html (accessed on 13 October 2021).
- Sprengeler, O.; Hebestreit, A.; Gohres, H.; Bucksch, J.; Buck, C. Effects of Installing Height-Adjustable Standing Desks on Daily and Domain-Specific Duration of Standing, Sitting, and Stepping in 3rd Grade Primary School Children. Front. Public Health 2020, 8, 396. [Google Scholar] [CrossRef]
- Brandes, B.; Buck, C.; Wright, M.N.; Pischke, C.R.; Brandes, M. Impact of “JolinchenKids-Fit and Healthy in Daycare” on Children’s Objectively Measured Physical Activity: A Cluster-Controlled Study. J. Phys. Act. Health 2020, 17, 1025–1033. [Google Scholar] [CrossRef]
- Verbestel, V.; de Henauw, S.; Barba, G.; Eiben, G.; Gallois, K.; Hadjigeorgiou, C.; Konstabel, K.; Maes, L.; Mårild, S.; Molnár, D.; et al. Effectiveness of the IDEFICS intervention on objectively measured physical activity and sedentary time in European children. Obes. Rev. 2015, 16 (Suppl. 2), 57–67. [Google Scholar] [CrossRef]
- Steenbock, B.; Zeeb, H.; Rach, S.; Pohlabeln, H.; Pischke, C.R. Design and methods for a cluster-controlled trial conducted at sixty-eight daycare facilities evaluating the impact of “JolinchenKids—Fit and Healthy in Daycare”, a program for health promotion in 3- to 6-year-old children. BMC Public Health 2017, 18, 6. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, W.; Bammann, K.; Siani, A.; Buchecker, K.; de Henauw, S.; Iacoviello, L.; Hebestreit, A.; Krogh, V.; Lissner, L.; Mårild, S.; et al. The IDEFICS cohort: Design, characteristics and participation in the baseline survey. Int. J. Obes. 2011, 35 (Suppl. 1), S3–S15. [Google Scholar] [CrossRef] [PubMed]
- Del Pozo-Cruz, J.; García-Hermoso, A.; Alfonso-Rosa, R.M.; Alvarez-Barbosa, F.; Owen, N.; Chastin, S.; Del Pozo-Cruz, B. Replacing Sedentary Time: Meta-analysis of Objective-Assessment Studies. Am. J. Prev. Med. 2018, 55, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Hadgraft, N.T.; Winkler, E.; Climie, R.E.; Grace, M.S.; Romero, L.; Owen, N.; Dunstan, D.; Healy, G.; Dempsey, P.C. Effects of sedentary behaviour interventions on biomarkers of cardiometabolic risk in adults: Systematic review with meta-analyses. Br. J. Sports Med. 2021, 55, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.; Le, L.K.-D.; Nguyen, D.; Gao, L.; Dunstan, D.W.; Moodie, M. The effectiveness of sedentary behaviour interventions on sitting time and screen time in children and adults: An umbrella review of systematic reviews. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 117. [Google Scholar] [CrossRef]
- Blackburn, N.E.; Wilson, J.J.; McMullan, I.I.; Caserotti, P.; Giné-Garriga, M.; Wirth, K.; Coll-Planas, L.; Alias, S.B.; Roqué, M.; Deidda, M.; et al. The effectiveness and complexity of interventions targeting sedentary behaviour across the lifespan: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 53. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Petrolini, I.; Pearson, N. Interventions designed to reduce sedentary behaviours in young people: A review of reviews. Br. J. Sports Med. 2014, 48, 182–186. [Google Scholar] [CrossRef]
- Marsh, S.; Foley, L.S.; Wilks, D.C.; Maddison, R. Family-based interventions for reducing sedentary time in youth: A systematic review of randomized controlled trials. Obes. Rev. 2014, 15, 117–133. [Google Scholar] [CrossRef]
- Verjans-Janssen, S.R.B.; van de Kolk, I.; van Kann, D.H.H.; Kremers, S.P.J.; Gerards, S.M.P.L. Effectiveness of school-based physical activity and nutrition interventions with direct parental involvement on children’s BMI and energy balance-related behaviors—A systematic review. PLoS ONE 2018, 13, e0204560. [Google Scholar] [CrossRef]
- Mollborn, S.; Lawrence, E. Family, Peer, and School Influences on Children’s Developing Health Lifestyles. J. Health Soc. Behav. 2018, 59, 133–150. [Google Scholar] [CrossRef]
- Chase, J.-A.D.; Otmanowski, J.; Rowland, S.; Cooper, P.S. A systematic review and meta-analysis of interventions to reduce sedentary behavior among older adults. Transl. Behav. Med. 2020, 10, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Guirado, T.; Chambonnière, C.; Chaput, J.-P.; Metz, L.; Thivel, D.; Duclos, M. Effects of Classroom Active Desks on Children and Adolescents’ Physical Activity, Sedentary Behavior, Academic Achievements and Overall Health: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 2828. [Google Scholar] [CrossRef] [PubMed]
- Minges, K.E.; Chao, A.M.; Irwin, M.L.; Owen, N.; Park, C.; Whittemore, R.; Salmon, J. Classroom Standing Desks and Sedentary Behavior: A Systematic Review. Pediatrics 2016, 137, e20153087. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.H.; Pearson, N.; Ross, G.M.; Braithwaite, R. Tracking of sedentary behaviours of young people: A systematic review. Prev. Med. 2010, 51, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.A.; Hinkley, T.; Okely, A.D.; Salmon, J. Tracking physical activity and sedentary behavior in childhood: A systematic review. Am. J. Prev. Med. 2013, 44, 651–658. [Google Scholar] [CrossRef]
- van Ekris, E.; Wijndaele, K.; Altenburg, T.M.; Atkin, A.J.; Twisk, J.; Andersen, L.B.; Janz, K.F.; Froberg, K.; Northstone, K.; Page, A.S.; et al. Tracking of total sedentary time and sedentary patterns in youth: A pooled analysis using the International Children’s Accelerometry Database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2020, 17, 65. [Google Scholar] [CrossRef]
- Murtagh, E.M.; Murphy, M.H.; Milton, K.; Roberts, N.W.; O’Gorman, C.S.; Foster, C. Interventions outside the workplace for reducing sedentary behaviour in adults under 60 years of age. Cochrane Database Syst. Rev. 2020, 7, CD012554. [Google Scholar] [CrossRef]
- Shrestha, N.; Grgic, J.; Wiesner, G.; Parker, A.; Podnar, H.; Bennie, J.A.; Biddle, S.J.H.; Pedisic, Z. Effectiveness of interventions for reducing non-occupational sedentary behaviour in adults and older adults: A systematic review and meta-analysis. Br. J. Sports Med. 2019, 53, 1206–1213. [Google Scholar] [CrossRef]
- Prince, S.A.; Saunders, T.J.; Gresty, K.; Reid, R.D. A comparison of the effectiveness of physical activity and sedentary behaviour interventions in reducing sedentary time in adults: A systematic review and meta-analysis of controlled trials. Obes. Rev. 2014, 15, 905–919. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mugler, N.; Baurecht, H.; Lam, K.; Leitzmann, M.; Jochem, C. The Effectiveness of Interventions to Reduce Sedentary Time in Different Target Groups and Settings in Germany: Systematic Review, Meta-Analysis and Recommendations on Interventions. Int. J. Environ. Res. Public Health 2022, 19, 10178. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191610178
Mugler N, Baurecht H, Lam K, Leitzmann M, Jochem C. The Effectiveness of Interventions to Reduce Sedentary Time in Different Target Groups and Settings in Germany: Systematic Review, Meta-Analysis and Recommendations on Interventions. International Journal of Environmental Research and Public Health. 2022; 19(16):10178. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191610178
Chicago/Turabian StyleMugler, Nida, Hansjörg Baurecht, Kevin Lam, Michael Leitzmann, and Carmen Jochem. 2022. "The Effectiveness of Interventions to Reduce Sedentary Time in Different Target Groups and Settings in Germany: Systematic Review, Meta-Analysis and Recommendations on Interventions" International Journal of Environmental Research and Public Health 19, no. 16: 10178. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191610178