
Influence of Initial Severity of Depression on the Effectiveness of a Multimodal Therapy on Depressive Score, Heart Rate Variability, and Hemodynamic Parameters


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurements
2.2.1. Hemodynamic Measurements
2.2.2. Cardiac Autonomic Function
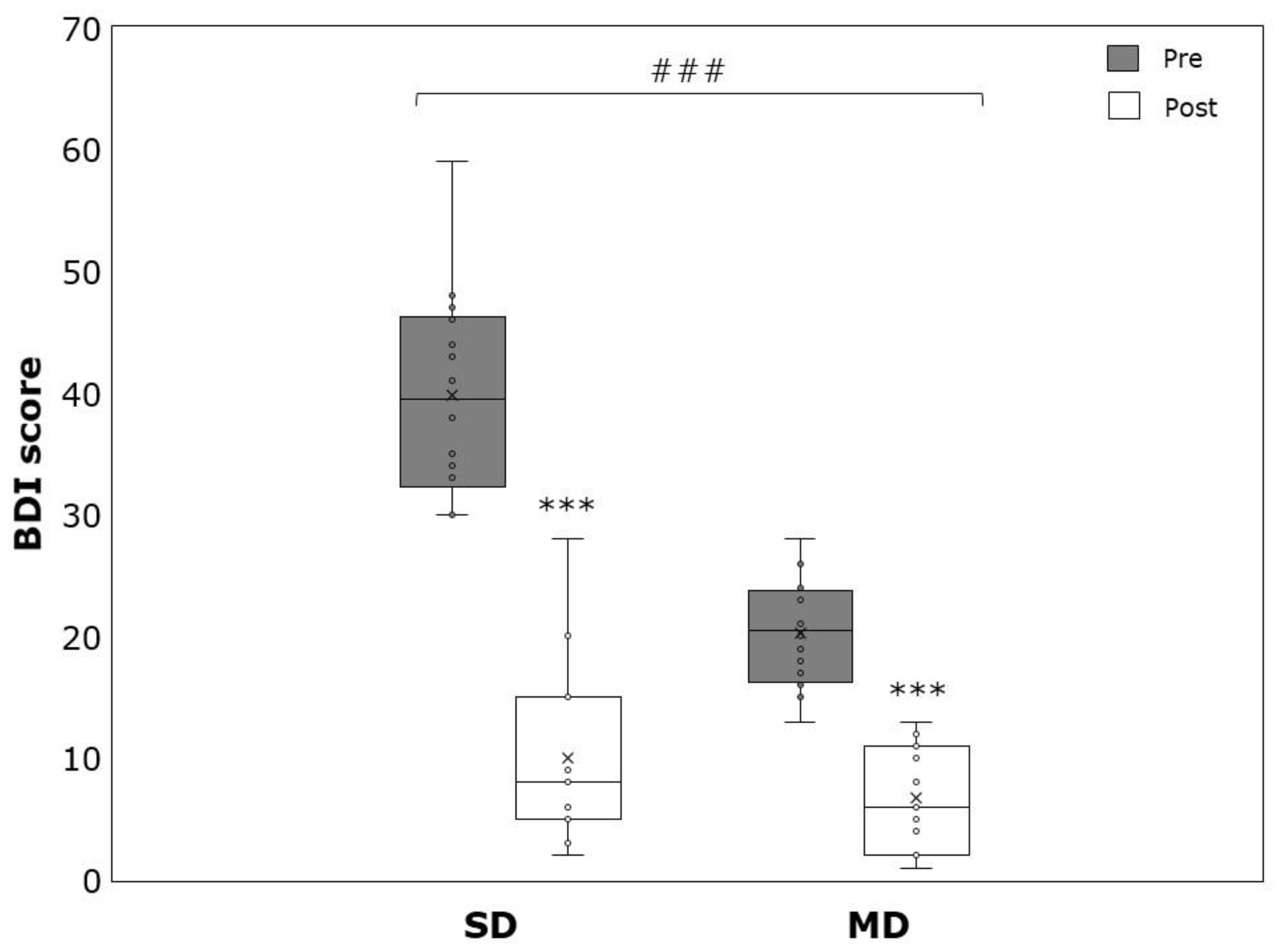
2.2.3. Depression SCORE
2.3. Multimodal Psychosomatic Therapy
2.4. Statistics
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- University of Washington, Institute of Health Metrics and Evaluation. Global Health Data Exchange (GHDx). Available online: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/d780dffbe8a381b25e1416884959e88b (accessed on 11 February 2022).
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of all-cause and suicide mortality in mental disorders: A meta-review. World Psychiatry 2014, 13, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correll, C.U.; Solmi, M.; Veronese, N.; Bortolato, B.; Rosson, S.; Santonastaso, P.; Thapa-Chhetri, N.; Fornaro, M.; Gallicchio, D.; Collantoni, E.; et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: A large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry 2017, 16, 163–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, L.; Chen, D.; Yang, Y.; Zheng, Y.; Hui, R. Depression increases the risk of hypertension incidence: A meta-analysis of prospective cohort studies. J. Hypertens. 2012, 30, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Kling, J.M. Depression and the Risk of Myocardial Infarction and Coronary Death. Medicine 2016, 95, e2815. [Google Scholar] [CrossRef]
- Gan, Y.; Gong, Y.; Tong, X.; Sun, H.; Cong, Y.; Dong, X.; Wang, Y.; Xu, X.; Yin, X.; Deng, J.; et al. Depression and the risk of coronary heart disease: A meta-analysis of prospective cohort studies. BMC Psychiatry 2014, 14, 371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhat, S.K.; Beilin, L.J.; Robinson, M.; Burrows, S.; Mori, T.A. Relationships between depression and anxiety symptoms scores and blood pressure in young adults. J. Hypertens. 2017, 35, 1983–1991. [Google Scholar] [CrossRef] [PubMed]
- Kampling, H.; Petrak, F.; Farin, E.; Kulzer, B.; Herpertz, S.; Mittag, O. Trajectories of depression in adults with newly diagnosed type 1 diabetes: Results from the German Multicenter Diabetes Cohort Study. Diabetologia 2017, 60, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Ladwig, K.H.; Baumert, J.; Marten-Mittag, B.; Lukaschek, K.; Johar, H.; Fang, X.; Ronel, J.; Meisinger, C.; Peters, A. Room for depressed and exhausted mood as a risk predictor for all-cause and cardiovascular mortality beyond the contribution of the classical somatic risk factors in men. Atherosclerosis 2017, 257, 224–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahl, T.; Steinsbekk, S.; Wichstrøm, L. Physical activity, sedentary behavior, and symptoms of major depression in middle childhood. Pediatrics 2017, 139, e20161711. [Google Scholar] [CrossRef] [Green Version]
- Svensson, M.; Brundin, L.; Erhardt, S.; Madaj, Z.; Hållmarker, U.; James, S.; Deierborg, T. Long distance ski racing is associated with lower long-term incidence of depression in a population based, large-scale study. Psychiatry Res. 2019, 281, 112546. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; De Leon, A.P.; Dunn, A.L.; Deslandes, A.C.; et al. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef] [PubMed]
- Bennie, J.A.; De Cocker, K.; Biddle, S.J.H.; Teychenne, M.J. Joint and dose-dependent associations between aerobic and muscle-strengthening activity with depression: A cross-sectional study of 1.48 million adults between 2011 and 2017. Depress. Anxiety 2020, 37, 166–178. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, J.A.; Babyak, M.A.; Moore, K.A.; Craighead, W.E.; Herman, S.; Khatri, P.; Waugh, R.; Napolitano, M.A.; Forman, L.M.; Appelbaum, M.; et al. Effects of exercise training on older patients with major depression. Arch. Intern. Med. 1999, 159, 2349–2356. [Google Scholar] [CrossRef]
- Gordon, B.R.; McDowell, C.P.; Hallgren, M.; Meyer, J.D.; Lyons, M.; Herring, M.P. Association of efficacy of resistance exercise training with depressive symptoms meta-analysis and meta-regression: Analysis of randomized clinical trials. JAMA Psychiatry 2018, 75, 566–576. [Google Scholar] [CrossRef]
- Stanton, R.; Reaburn, P. Exercise and the treatment of depression: A review of the exercise program variables. J. Sci. Med. Sport 2014, 17, 177–182. [Google Scholar] [CrossRef]
- Cooney, G.; Dwan, K.; Mead, G. Exercise for depression. JAMA—J. Am. Med. Assoc. 2014, 311, 2432–2433. [Google Scholar] [CrossRef]
- Hoffman, B.M.; Babyak, M.A.; Craighead, W.E.; Sherwood, A.; Doraiswamy, P.M.; Coons, M.J.; Blumenthal, J.A. Exercise and Pharmacotherapy in Patients with Major Depression. Psychosom. Med. 2011, 73, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Brenes, G.A.; Williamson, J.D.; Messier, S.P.; Rejeski, W.J.; Pahor, M.; Ip, E.; Penninx, B.W.J.H. Treatment of minor depression in older adults: A pilot study. Aging Ment. Health 2007, 11, 61–68. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Babyak, M.A.; Doraiswamy, P.M.; Watkins, L.; Hoffman, B.M.; Barbour, K.A.; Herman, S.; Craighead, W.E.; Brosse, A.L.; Waugh, R.; et al. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom. Med. 2007, 69, 587–596. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Kahlmeier, S. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. Available online: https://pubmed.ncbi.nlm.nih.gov/23525435/ (accessed on 1 December 2020). [CrossRef] [Green Version]
- Wang, K.L.; Cheng, H.M.; Chuang, S.Y.; Spurgeon, H.A.; Ting, C.T.; Lakatta, E.G.; Yin, F.C.P.; Chou, P.; Chen, C.H. Central or peripheral systolic or pulse pressure: Which best relates to target organs and future mortality? J. Hypertens. 2009, 27, 461–467. [Google Scholar] [CrossRef] [Green Version]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef]
- Driessen, E.; Cuijpers, P.; Hollon, S.D.; Dekker, J.J.M. Does pretreatment severity moderate the efficacy of psychological treatment of adult outpatient depression? A meta-analysis. J. Consult. Clin. Psychol. 2010, 78, 668–680. [Google Scholar] [CrossRef] [Green Version]
- De Graaf, L.E.; Gerhards, S.A.H.; Arntz, A.; Riper, H.; Metsemakers, J.F.M.; Evers, S.M.A.A.; Severens, J.L.; Widdershoven, G.; Huibers, M.J.H. Clinical effectiveness of online computerised cognitive-behavioural therapy without support for depression in primary care: Randomised trial. Br. J. Psychiatry 2009, 195, 73–80. [Google Scholar] [CrossRef]
- Lovell, K.; Bower, P.; Richards, D.; Barkham, M.; Sibbald, B.; Roberts, C.; Davies, L.; Rogers, A.; Gellatly, J.; Hennessy, S. Developing guided self-help for depression using the Medical Research Council complex interventions framework: A description of the modelling phase and results of an exploratory randomised controlled trial. BMC Psychiatry 2008, 8, 91. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, T.A.; Weitz, E.S.; Tanaka, S.; Hollon, S.D.; Hofmann, S.G.; Andersson, G.; Twisk, J.; DeRubeis, R.J.; Dimidjian, S.; Hegerl, U.; et al. Initial severity of depression and efficacy of cognitive-behavioural therapy: Individual-participant data meta-analysis of pill-placebo-controlled trials. Br. J. Psychiatry 2017, 210, 190–196. [Google Scholar] [CrossRef] [Green Version]
- Bower, P.; Kontopantelis, E.; Sutton, A.; Kendrick, T.; Richards, D.A.; Gilbody, S.; Knowles, S.; Cuijpers, P.; Andersson, G.; Christensen, H.; et al. Influence of initial severity of depression on effectiveness of low intensity interventions: Meta-analysis of individual patient data. BMJ 2013, 346, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory, 2nd ed.; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Franssen, P.M.; Imholz, B.P. Evaluation of the Mobil-O-Graph new generation ABPM device using the ESH criteria. Blood Press. Monit. 2010, 15, 229–231. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Tarvainen, M.P.; Niskanen, J.P.; Lipponen, J.A.; Ranta-aho, P.O.; Karjalainen, P.A. Kubios HRV—Heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Malik, M. Standard measurement of heart rate variability. In Dynamic Electrocardiography; Malik, M., Camm, J., Eds.; Blackwell Publishing: New York, NY, USA, 2008; pp. 13–21. [Google Scholar]
- Piotrowski, C.; Sherry, D.; Keller, J.W. Psychodiagnostic Test Usage: A Survey of the Society for Personality Assessment. J. Pers. Assess. 1985, 49, 115–119. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Garbin, M.G. The psychometric validation of the Sheehan Disability Scale (SDS) in patients with bipolar disorder. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Geue, K.; Strauß, B.; Brähler, E. Diagnostische Verfahren in Der Psychotherapie, 3rd ed.; Hogrefe: Göttingen, Germany, 2016. [Google Scholar]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Weisell, R.C. Body mass index as an indicator of obesity. Asia Pac. J. Clin. Nutr. 2002, 11, S681–S684. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; Simone, G.D.; Dominiczak, A.; et al. 2018 practice guidelines for the management of arterial hypertension of the European society of cardiology and the European society of hypertension ESC/ESH task force for the management of arterial hypertension. J. Hypertens. 2018, 36, 2284–2309. [Google Scholar] [CrossRef] [Green Version]
- Cuijpers, P.; Turner, E.H.; Mohr, D.C.; Hofmann, S.G.; Andersson, G.; Berking, M.; Coyne, J. Comparison of psychotherapies for adult depression to pill placebo control groups: A meta-analysis. Psychol. Med. 2014, 44, 685–695. [Google Scholar] [CrossRef] [Green Version]
- Catalina-Romero, C.; Calvo-Bonacho, E. Depression and cardiovascular disease: Time for clinical trials. Atherosclerosis 2017, 257, 250–252. [Google Scholar] [CrossRef]
- Ahmadpanah, M.; Paghale, S.J.; Bakhtyari, A.; Kaikhavani, S.; Aghaei, E.; Nazaribadie, M.; Holsboer-Trachsler, E.; Brand, S. Effects of psychotherapy in combination with pharmacotherapy, when compared to pharmacotherapy only on blood pressure, depression, and anxiety in female patients with hypertension. J. Health Psychol. 2016, 21, 1216–1227. [Google Scholar] [CrossRef]
- Abbott, R.A.; Whear, R.; Rodgers, L.R.; Bethel, A.; Thompson Coon, J.; Kuyken, W.; Stein, K.; Dickens, C. Effectiveness of mindfulness-based stress reduction and mindfulness based cognitive therapy in vascular disease: A systematic review and meta-analysis of randomised controlled trials. J. Psychosom. Res. 2014, 76, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Yung, P.M.B.; Keltner, A.A. A controlled comparison on the effect of muscle and cognitive relaxation procedures on blood pressure: Implications for the behavioural treatment of borderline hypertensives. Behav. Res. Ther. 1996, 34, 821–826. [Google Scholar] [CrossRef]
- Law, M.R.; Morris, J.K.; Wald, N.J. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: Meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009, 338, 1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kučerová, J.; Filipovský, J.; Staessen, J.A.; Cwynar, M.; Wojciechowska, W.; Stolarz, K.; Kuznetsova, T.; Gąsowski, J.; Dolejsová, M.; Grodzicki, T. Arterial characteristics in normotensive offspring of parents with or without a history of hypertension. Am. J. Hypertens. 2006, 19, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollias, A.; Lagou, S.; Zeniodi, M.E.; Boubouchairopoulou, N.; Stergiou, G.S. Association of Central Versus Brachial Blood Pressure With Target-Organ Damage: Systematic Review and Meta-Analysis. Hypertension 2016, 67, 183–190. [Google Scholar] [CrossRef] [Green Version]
- Ben-Shlomo, Y.; Spears, M.; Boustred, C.; MAy, M.; Anderson, S.; Benjamin, E.; Benjamin, E.J.; Boutouyrie, P.; Cameron, J.; Chen, C.H.; et al. Aortic pulse wave velocity improves cardiovascular event prediction: An individual participant meta-analysis of prospective observational data from 17,635 subjects. J. Am. Coll. Cardiol. 2014, 63, 636–646. [Google Scholar] [CrossRef]
- Beck, D.T.; Martin, J.S.; Casey, D.P.; Braith, R.W. Exercise training reduces peripheral arterial stiffness and myocardial oxygen demand in young prehypertensive subjects. Am. J. Hypertens. 2013, 26, 1093–1102. [Google Scholar] [CrossRef] [Green Version]
- Peng, L.; Bi, S.; Liu, X.; Long, T.; Zhao, Y.; Li, F.; Yang, T.; Zhang, C. Association between depressive symptoms and arterial stiffness: A cross-sectional study in the general Chinese population. BMJ Open 2020, 10, e033408. [Google Scholar] [CrossRef] [Green Version]
- Tiemeier, H.; Breteler, M.M.B.; Van Popele, N.M.; Hofman, A.; Witteman, J.C.M. Late-life depression is associated with arterial stiffness: A population-based study. J. Am. Geriatr. Soc. 2003, 51, 1105–1110. [Google Scholar] [CrossRef]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ. Res. 1986, 59, 178–193. [Google Scholar] [CrossRef] [Green Version]
- Billman, G.E. Cardiac autonomic neural remodeling and susceptibility to sudden cardiac death: Effect of endurance exercise training. Am. J. Physiol.-Hear Circ. Physiol. 2009, 297, H1171–H1193. [Google Scholar] [CrossRef] [Green Version]
- Sgoifo, A.; Carnevali, L.; Pico Alfonso, M.D.L.A.; Amore, M. Autonomic dysfunction and heart rate variability in depression. Stress 2015, 18, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Koschke, M.; Boettger, M.K.; Schulz, S.; Berger, S.; Terhaar, J.; Voss, A.; Yeragani, V.K.; Bär, K.-J. Autonomy of autonomic dysfunction in major depression. Psychosom. Med. 2009, 71, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Kemp, A.H.; Quintana, D.S.; Gray, M.A.; Felmingham, K.L.; Brown, K.; Gatt, J.M. Impact of Depression and Antidepressant Treatment on Heart Rate Variability: A Review and Meta-Analysis. Biol. Psychiatry 2010, 67, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Licht, C.M.M.; De Geus, E.J.C.; Van Dyck, R.; Penninx, B.W.J.H. Longitudinal evidence for unfavorable effects of antidepressants on heart rate variability. Biol. Psychiatry 2010, 68, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Karavidas, M.K.; Lehrer, P.M.; Vaschillo, E.; Vaschillo, B.; Marin, H.; Buyske, S.; Malinovsky, I.; Radvanski, D.; Hassett, A. Preliminary results of an open label study of heart rate variability biofeedback for the treatment of major depression. Appl. Psychophysiol. Biofeedback 2007, 32, 19–30. [Google Scholar] [CrossRef]
- Caldwell, Y.T.; Steffen, P.R. Adding HRV biofeedback to psychotherapy increases heart rate variability and improves the treatment of major depressive disorder. Int. J. Psychophysiol. 2018, 131, 96–101. [Google Scholar] [CrossRef]
- Ladwig, K.H.; Marten-Mittag, B.; Löwel, H.; Döring, A.; Koenig, W. C-reactive protein, depressed mood, and the prediction of coronary heart disease in initially healthy men: Results from the MONICA-KORA Augsburg Cohort Study 1984–1998. Eur. Heart J. 2005, 26, 2537–2542. [Google Scholar] [CrossRef]
- Huffman, J.C.; Celano, C.M.; Beach, S.R.; Motiwala, S.R.; Januzzi, J.L. Depression and cardiac disease: Epidemiology, mechanisms, and diagnosis. Cardiovasc. Psychiatry Neurol. 2013, 2013, 695925. [Google Scholar] [CrossRef] [Green Version]
- Mavrides, N.; Nemeroff, C. Treatment of depression in cardiovascular disease. Depress. Anxiety 2013, 30, 328–341. [Google Scholar] [CrossRef]
- Von Känel, R.; Mills, P.J.; Fainman, C.; Dimsdale, J.E. Effects of psychological stress and psychiatric disorders on blood coagulation and fibrinolysis: A biobehavioral pathway to coronary artery disease? Psychosom. Med. 2001, 63, 531–544. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Milaneschi, Y.; Lamers, F.; Vogelzangs, N. Understanding the somatic consequences of depression: Biological mechanisms and the role of depression symptom profile. BMC Med. 2013, 11, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham, J.A.; Kypri, K.; Mccambridge, J. Exploratory randomized controlled trial evaluating the impact of a waiting list control design. BMC Med. Res. Methodol. 2013, 13, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Posternak, M.A.; Miller, I. Untreated short-term course of major depression: A meta-analysis of outcomes from studies using wait-list control groups. J. Affect. Disord. 2001, 66, 139–146. [Google Scholar] [CrossRef]
- Ogliari, G.; Mahinrad, S.; Stott, D.J.; Jukema, J.W.; Mooijaart, S.P.; Macfarlane, P.W.; Clark, E.N.; Kearney, P.; Westendorp, R.G.; de Craen, A.J.M.; et al. Resting heart rate, heart rate variability and functional decline in old age. Can. Med. Assoc. J. 2015, 187, E442–E449. [Google Scholar] [CrossRef] [Green Version]
- Hallgren, M.; Helgadóttir, B.; Herring, M.P.; Zeebari, Z.; Lindefors, N.; Kaldo, V.; Öjehagen, A.; Forsell, Y. Exercise and internet-based cognitive-behavioural therapy for depression: Multicentre randomized controlled trial with 12-month follow-up. Br. J. Psychiatry 2016, 209, 414–420. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Total (n = 30) | MD (n = 16) | SD (n = 14) | |
|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | p-Value | |
| F/M (n) | 18/12 | 9/7 | 9/5 | 0.743 |
| Age (yrs) | 47.9 ± 12.3 | 53.1 ± 7.6 | 43.2 ± 13.7 | 0.051 |
| BMI (kg·m−2) | 26.2 ± 4.1 | 25.8 ± 4.6 | 26.5 ± 3.8 | 0.989 |
| WHtR | 0.51 ± 0.08 | 0.51 ± 0.08 | 0.51 ± 0.07 | 0.974 |
| BDI | 29.4 ± 11.7 | 18.3 ± 2.4 | 39.9 ± 8.5 | <0.001 |
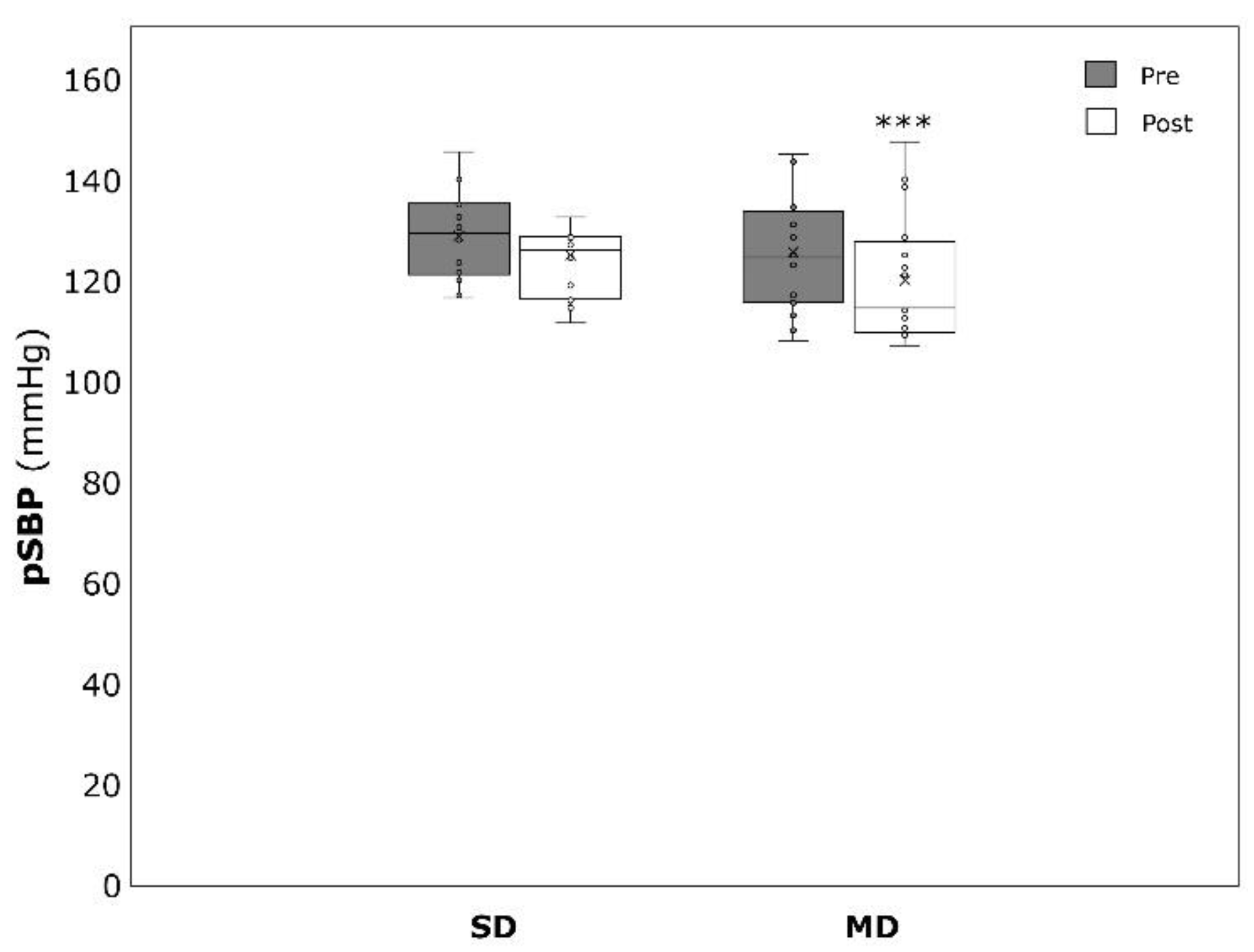
| pSBP (mmHg) | 127.1 ± 10.6 | 125.6 ± 12.0 | 128.7 ± 8.7 | 0.201 |
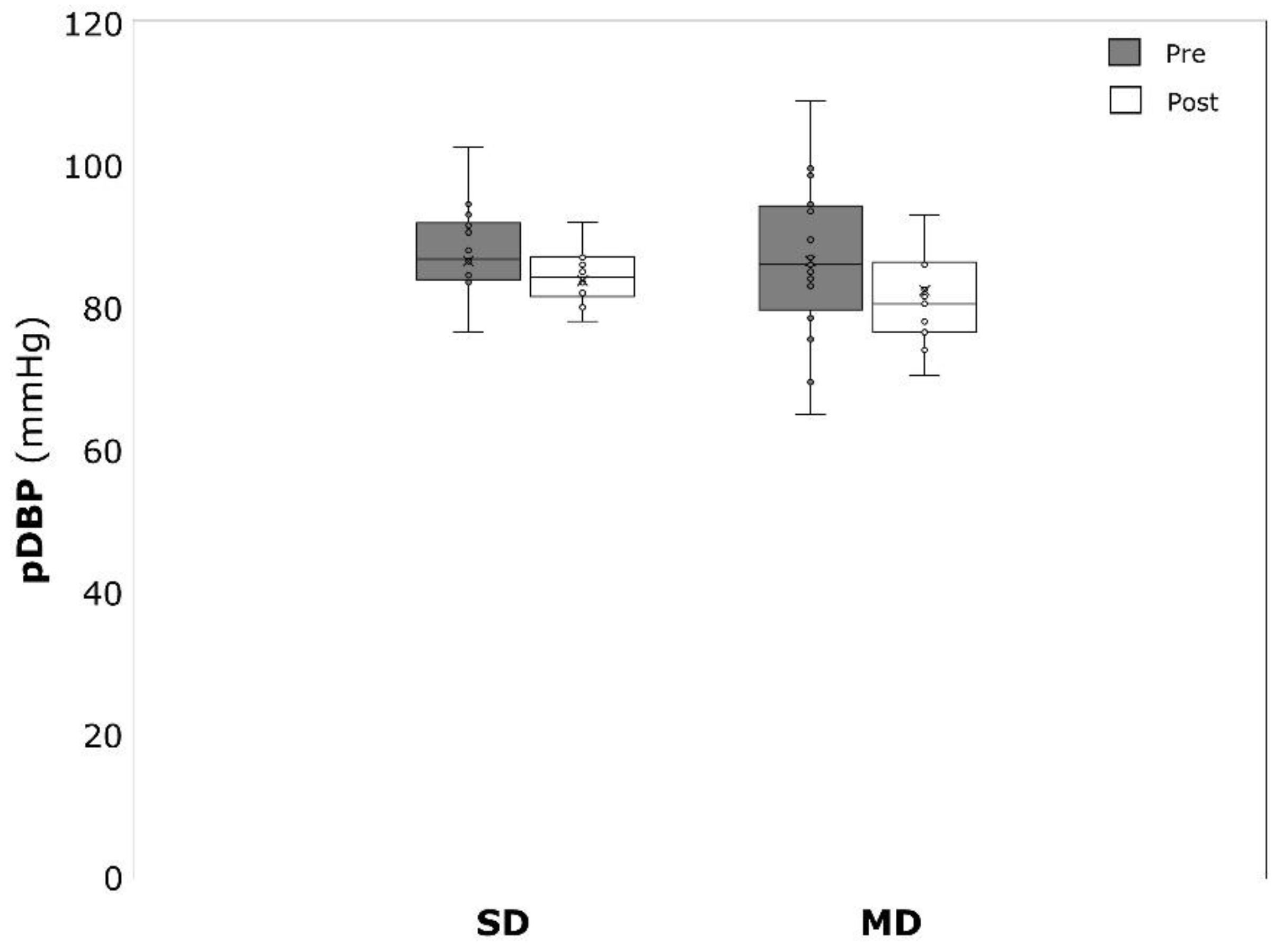
| pDBP(mmHg) | 85.0 ± 10.0 | 86.5 ± 11.3 | 86.5 ± 8.8 | 0.365 |
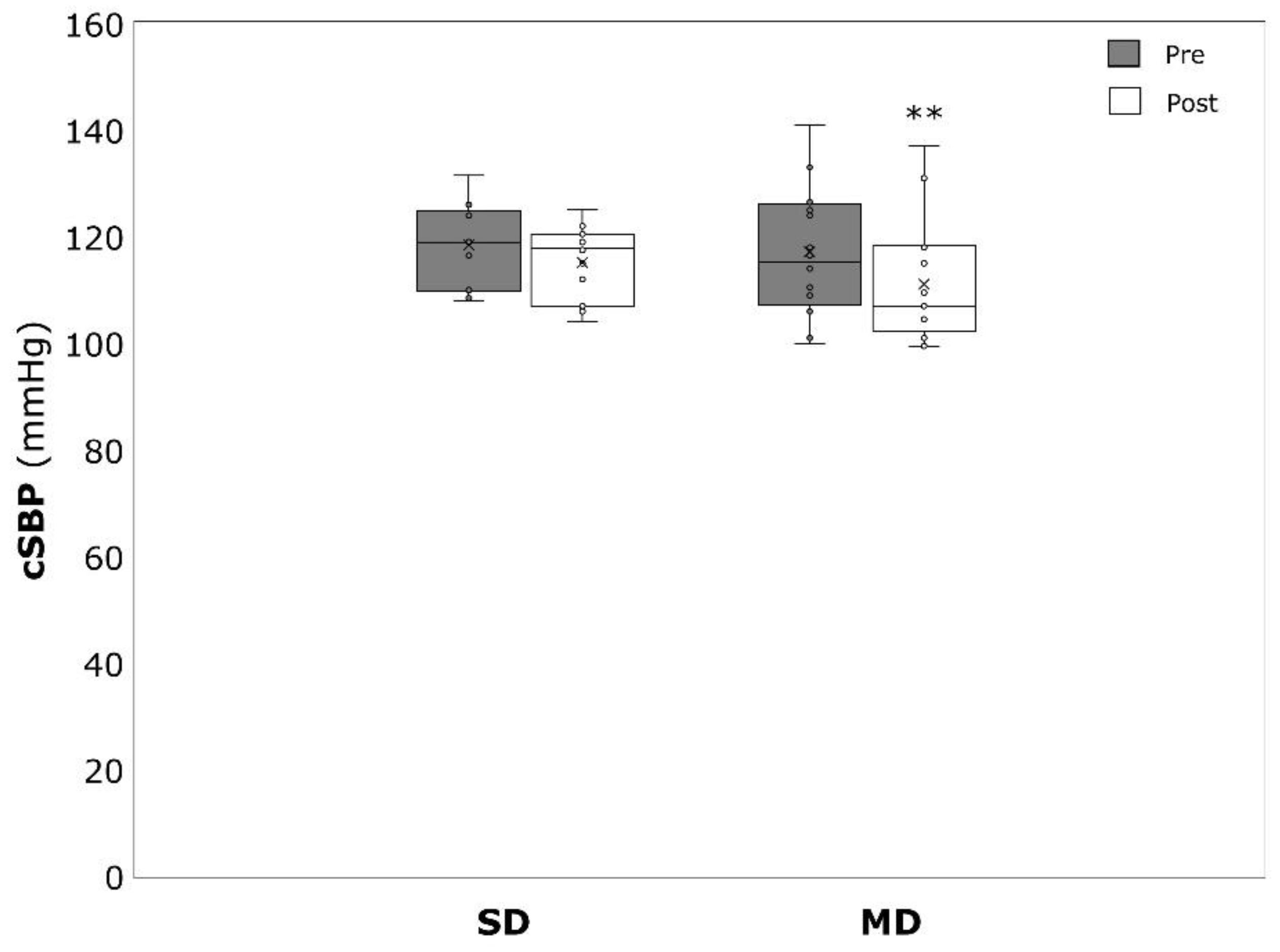
| cSBP (mmHg) | 117.8 ± 10.1 | 117.2 ± 12.2 | 118.4 ± 7.5 | 0.055 |
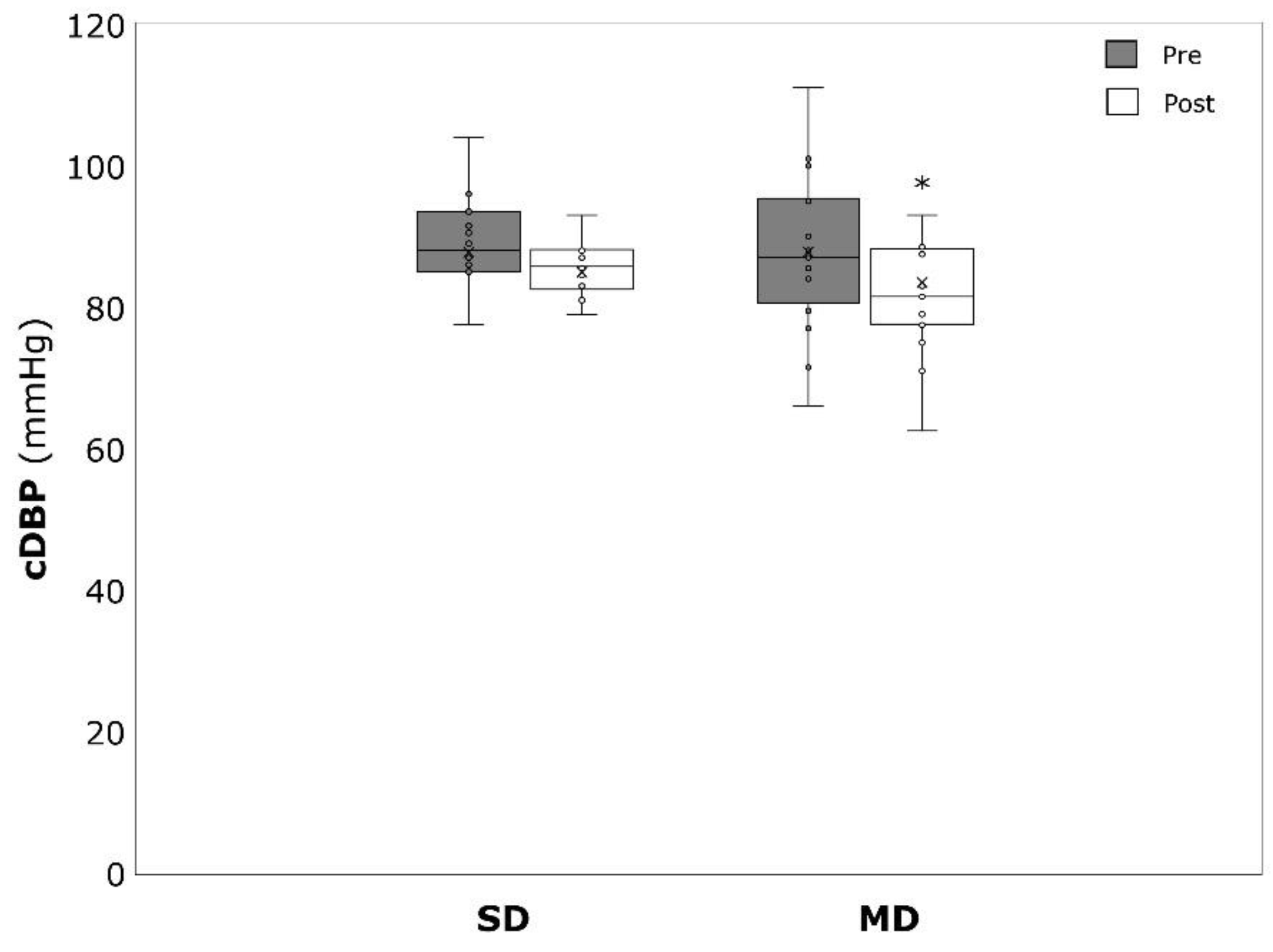
| cDBP (mmHg) | 87.8 ± 10.2 | 87.8 ± 11.3 | 87.8 ± 9.1 | 0.438 |
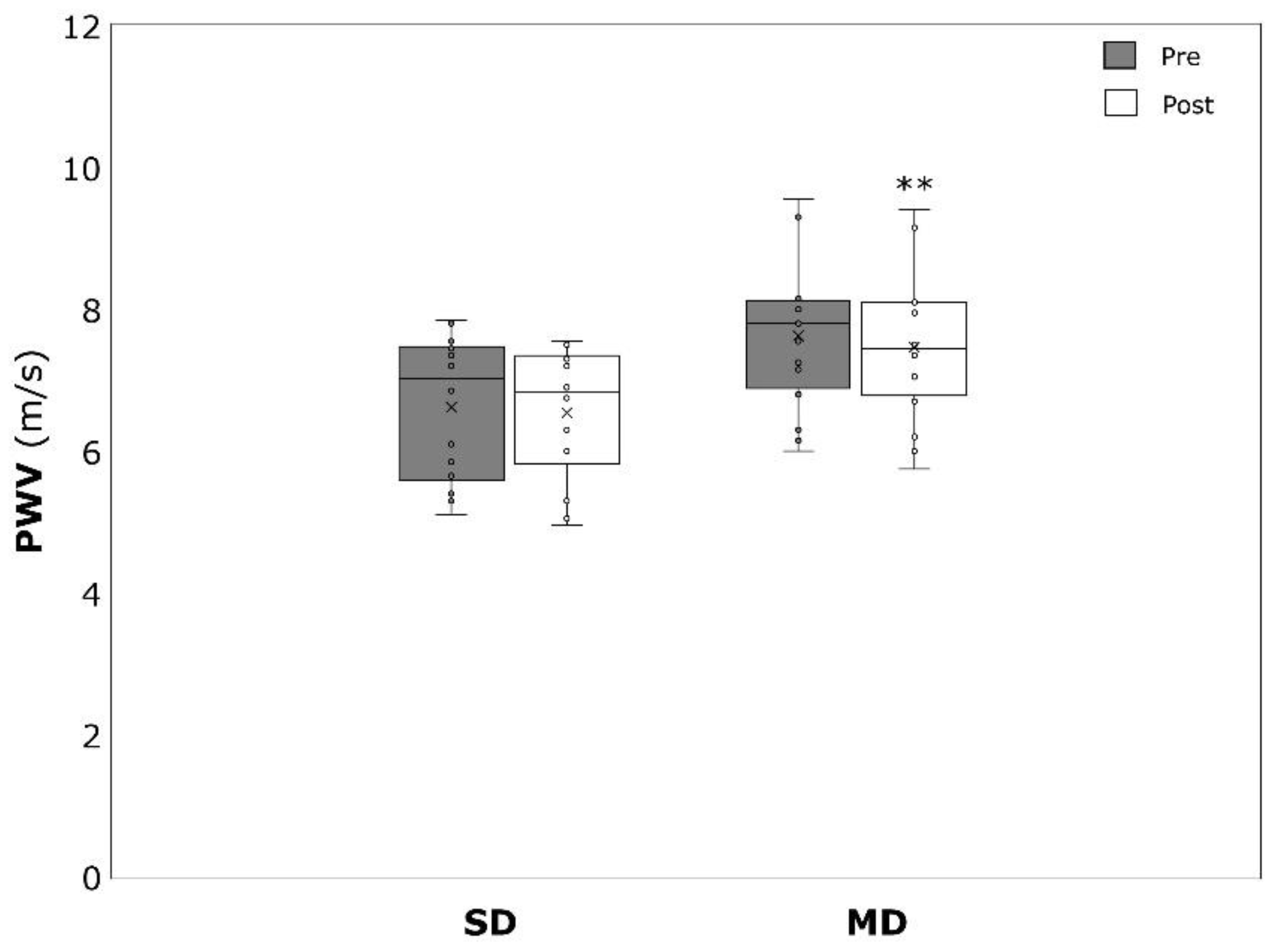
| PWV (m/s) | 7.2 ± 1.1 | 7.6 ± 1.0 | 6.8 ± 1.0 | 0.495 |
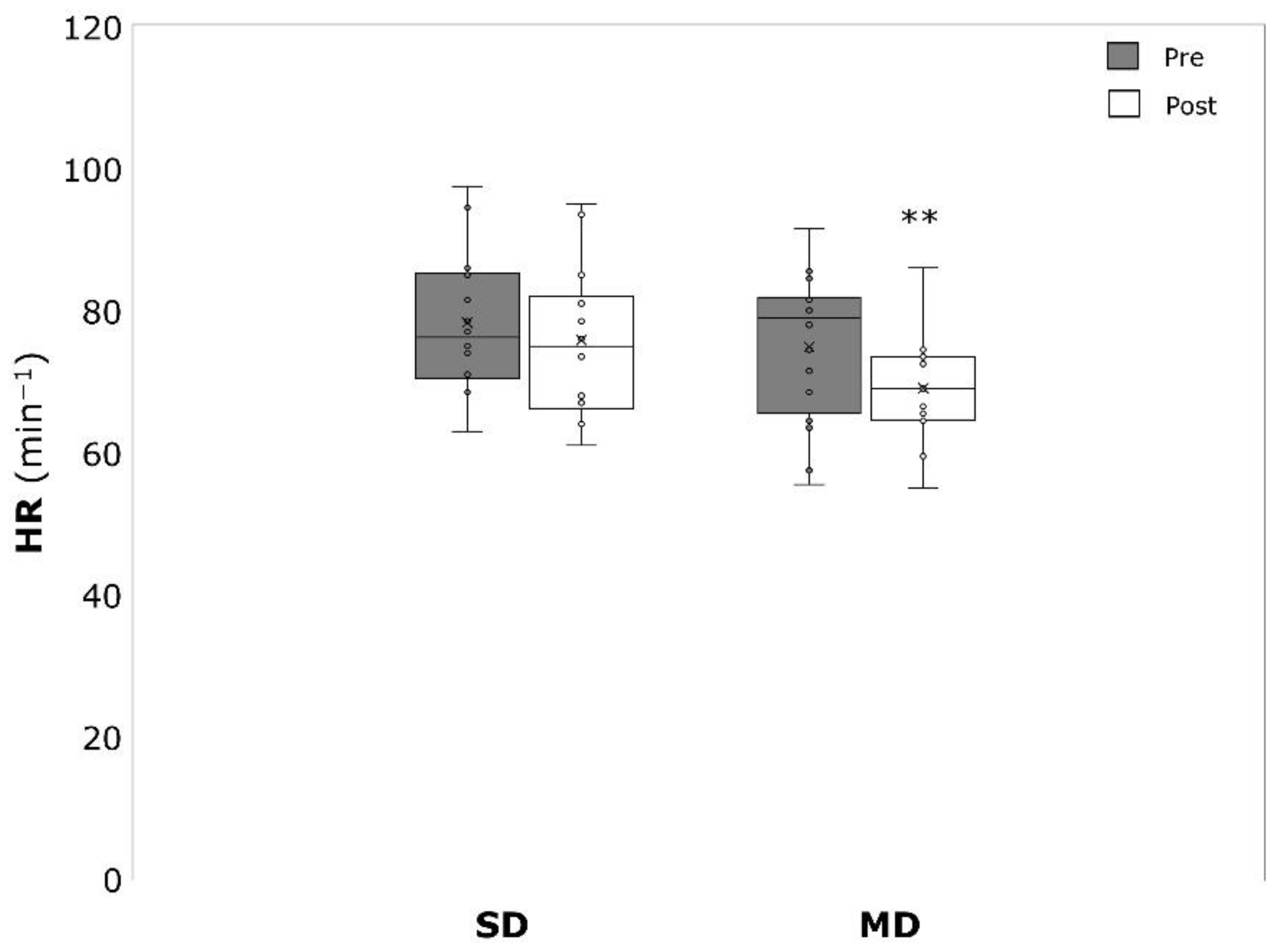
| HR (min−1) | 69.7 ± 9.4 | 67.9 ± 9.5 | 72.4 ± 9.1 | 0.908 |
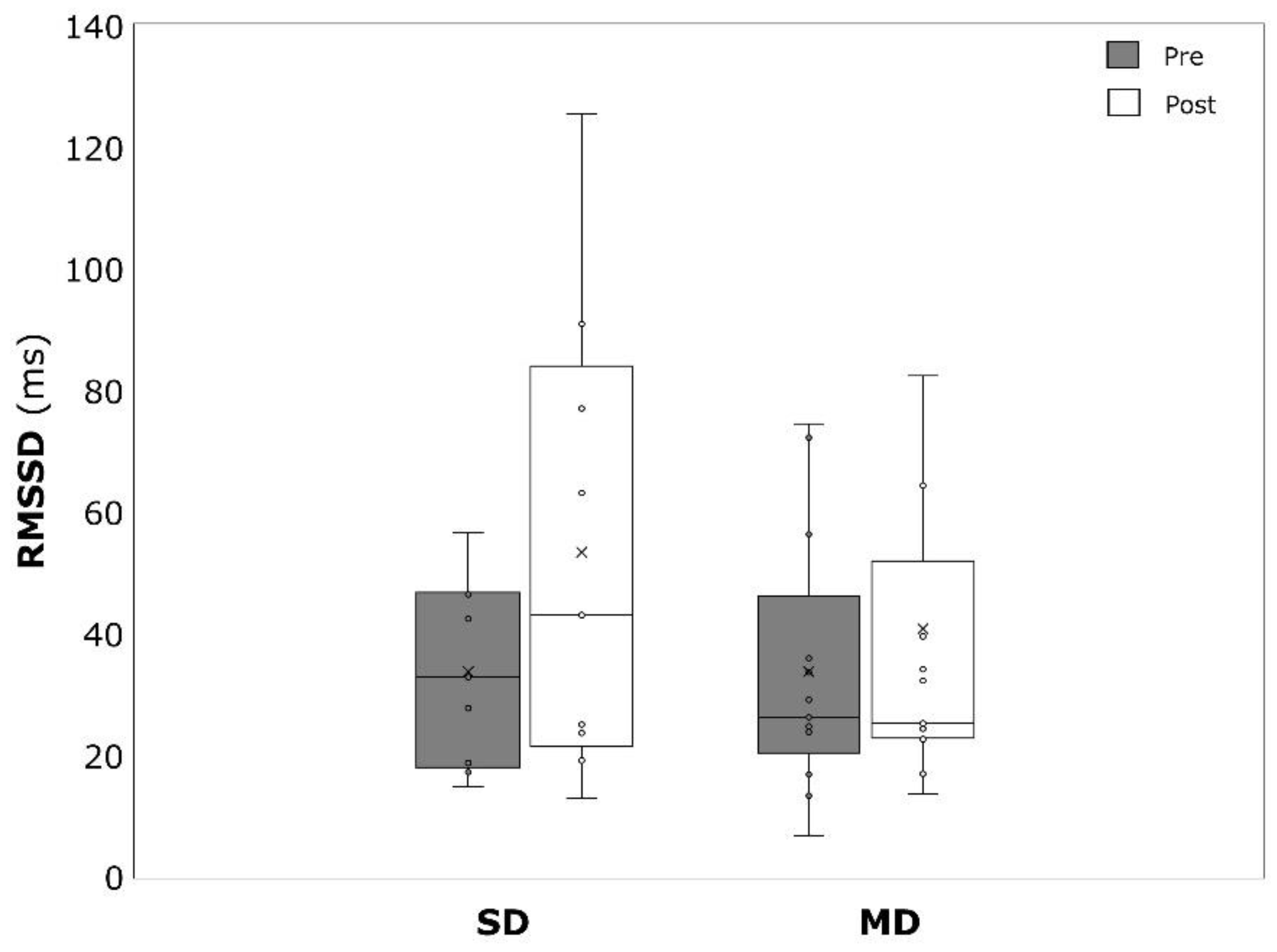
| RMSSD (ms) | 33.7 ± 18.6 | 33.7 ± 21.2 | 33.7 ± 15.1 | 0.510 |
| SDNN (ms) | 38.0 ± 18.2 | 35.6 ± 18.9 | 41.5 ± 17.6 | 0.899 |
| Outcomes | Total (n = 30) | ||||
|---|---|---|---|---|---|
| Mean Change | p-Values (Time) | η2 | p-Values (Time × Group) | η2 | |
| BMI (kg·m−2) | 0.14 ± 0.61 | 0.236 | 0.05 | 0.715 | 0.005 |
| WHtR | −0.002 ± 0.009 | 0.306 | 0.037 | 0.203 | 0.057 |
| BDI | −20.0 ± 11.6 | <0.001 | 0.871 | p < 0.001 | 0.543 |
| pSBP (mmHg) | −4.7 ± 6.8 | <0.001 | 0.322 | 0.458 | 0.020 |
| pDBP (mmHg) | −3.5 ± 6.9 | 0.011 | 0.209 | 0.596 | 0.010 |
| cSBP (mmHg) | −4.8 ± 6.5 | <0.001 | 0.355 | 0.239 | 0.049 |
| cDBP (mmHg) | −3.6 ± 6.8 | 0.008 | 0.226 | 0.566 | 0.012 |
| PWV (m/s) | −0.13 ± 0.23 | 0.008 | 0.229 | 0.340 | 0.033 |
| HR (min−1) | −4.3 ± 8.8 | 0.015 | 0.193 | 0.301 | 0.038 |
| RMSSD (ms) | 12.2 ± 23.9 | 0.017 | 0.251 | 0.236 | 0.069 |
| SDNN (ms) | 10.5 ± 17.8 | 0.005 | 0.330 | 0.108 | 0.124 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ketelhut, S.; Wehlan, E.; Bayer, G.; Ketelhut, R.G. Influence of Initial Severity of Depression on the Effectiveness of a Multimodal Therapy on Depressive Score, Heart Rate Variability, and Hemodynamic Parameters. Int. J. Environ. Res. Public Health 2022, 19, 9836. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19169836
Ketelhut S, Wehlan E, Bayer G, Ketelhut RG. Influence of Initial Severity of Depression on the Effectiveness of a Multimodal Therapy on Depressive Score, Heart Rate Variability, and Hemodynamic Parameters. International Journal of Environmental Research and Public Health. 2022; 19(16):9836. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19169836
Chicago/Turabian StyleKetelhut, Sascha, Emanuel Wehlan, Gerhart Bayer, and Reinhard G. Ketelhut. 2022. "Influence of Initial Severity of Depression on the Effectiveness of a Multimodal Therapy on Depressive Score, Heart Rate Variability, and Hemodynamic Parameters" International Journal of Environmental Research and Public Health 19, no. 16: 9836. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19169836