
Offered Support and Knowledge about the Menstrual Cycle in the Athletic Community: A Cross-Sectional Study of 1086 Female Athletes
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Population and Distribution of the Survey
2.2. Design and Distribution of the Survey
2.3. Statistical Analysis and Data Categorization
3. Results
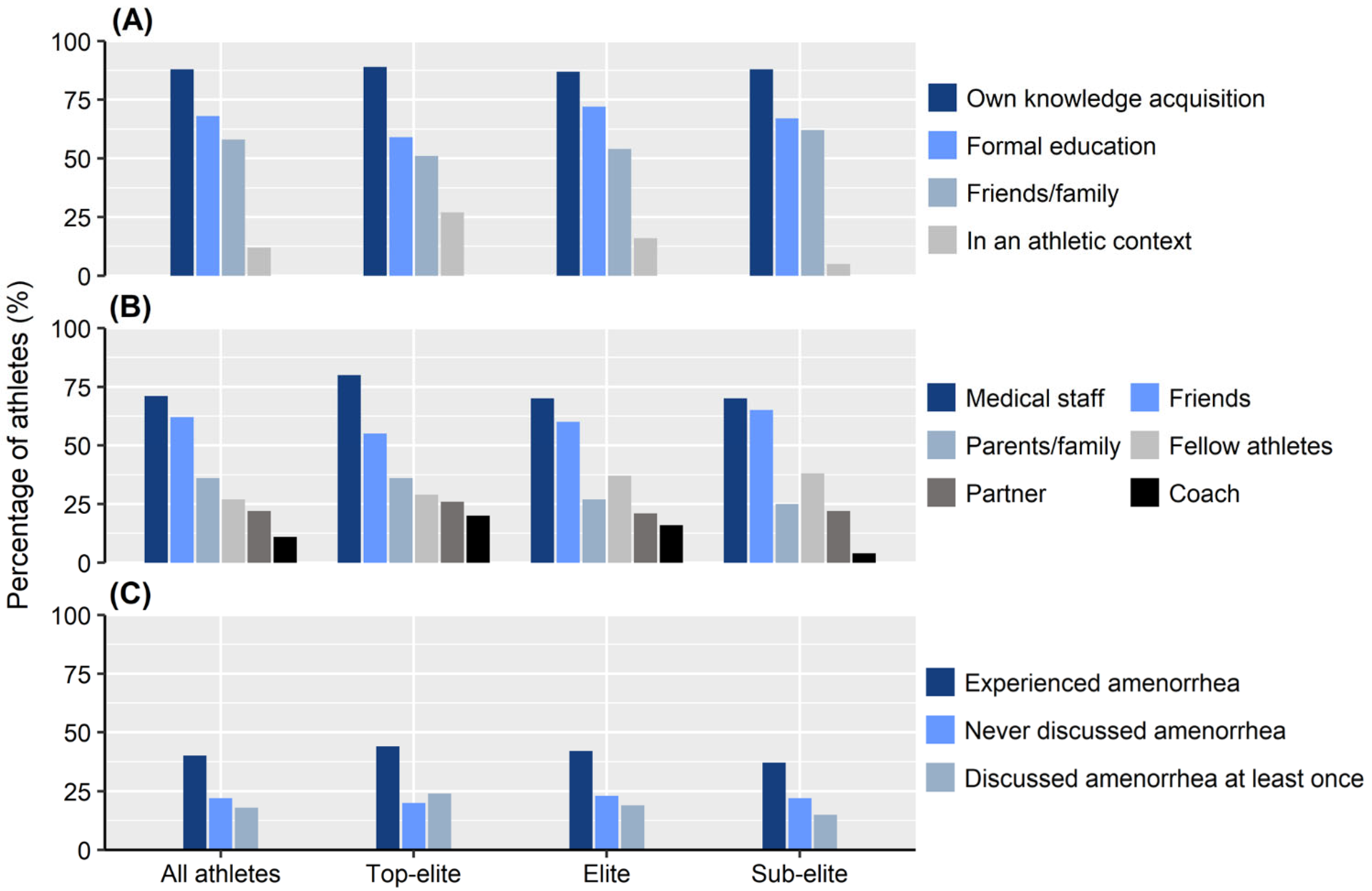
3.1. Support Provided to the Athlete
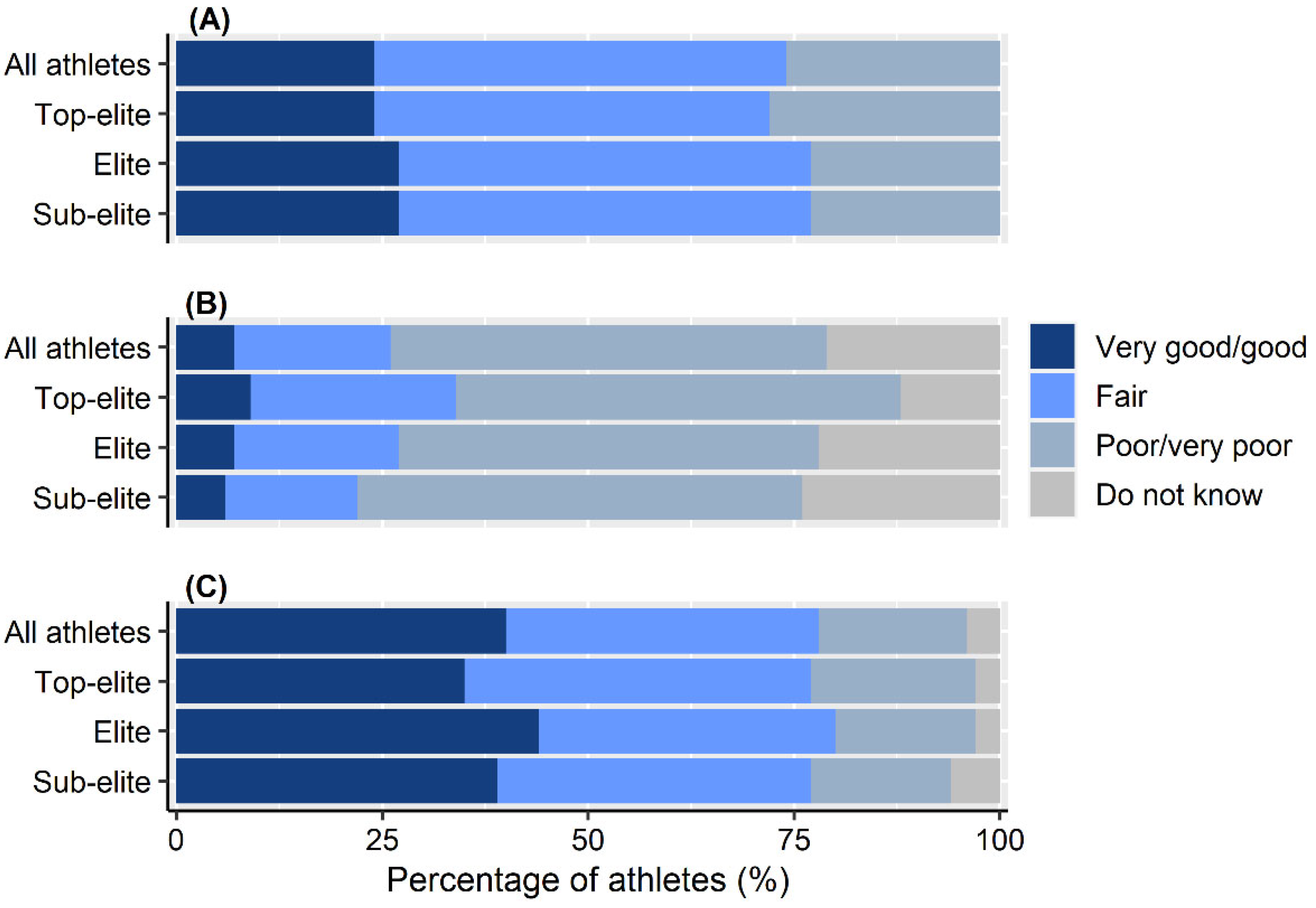
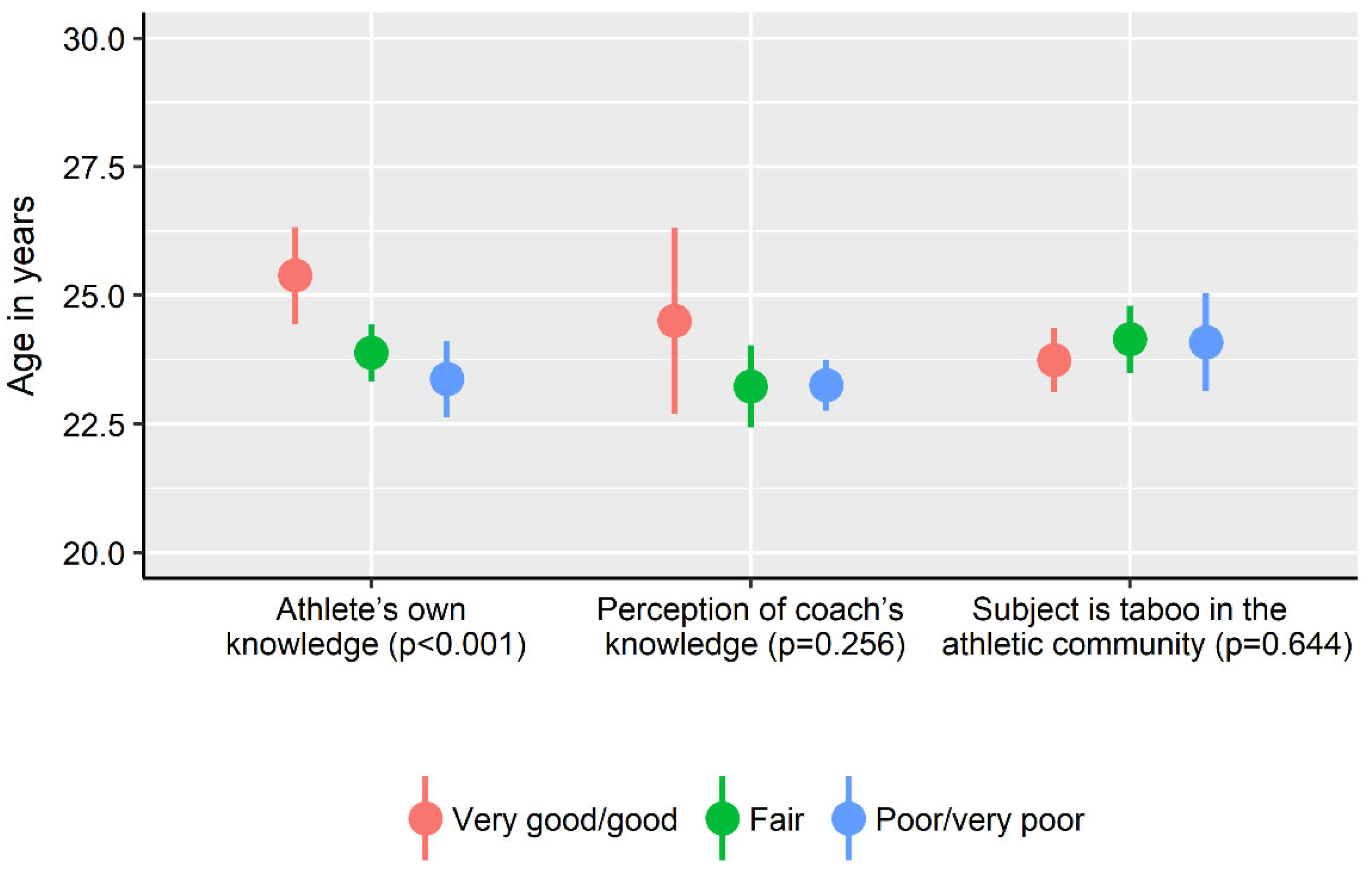
3.2. Knowledge about Aspects of Female Athlete Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Findlay, R.J.; Macrae, E.H.R.; Whyte, I.Y.; Easton, C.; Forrest Née Whyte, L.J. How the menstrual cycle and menstruation affect sporting performance: Experiences and perceptions of elite female rugby players. Br. J. Sports Med. 2020, 54, 1108–1113. [Google Scholar] [CrossRef] [PubMed]
- Solli, G.S.; Sandbakk, S.B.; Noordhof, D.A.; Ihalainen, J.K.; Sandbakk, Ø. Changes in Self-Reported Physical Fitness, Performance, and Side Effects Across the Phases of the Menstrual Cycle Among Competitive Endurance Athletes. Int. J. Sports Physiol. Perform. 2020, 15, 1324–1333. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, M.A.; Thomson, R.L.; Moran, L.J.; Dunstan, J.R.; Nelson, M.J.; Mathai, M.L.; Wycherley, T.P. A Pilot Study on the Impact of Menstrual Cycle Phase on Elite Australian Football Athletes. Int. J. Environ. Res. Public Health 2021, 18, 9591. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.; Sale, C.; Cooper, S.B.; Elliott-Sale, K.J. Period Prevalence and Perceived Side Effects of Hormonal Contraceptive Use and the Menstrual Cycle in Elite Athletes. Int. J. Sports Physiol. Perform. 2018, 13, 926–932. [Google Scholar] [CrossRef]
- Brown, N.; Knight, C.J.; Forrest Née Whyte, L.J. Elite female athletes’ experiences and perceptions of the menstrual cycle on training and sport performance. Scand. J. Med. Sci. Sports 2021, 31, 52–69. [Google Scholar] [CrossRef]
- Bruinvels, G.; Burden, R.; Brown, N.; Richards, T.; Pedlar, C. The Prevalence and Impact of Heavy Menstrual Bleeding (Menorrhagia) in Elite and Non-Elite Athletes. PLoS ONE 2016, 11, e0149881. [Google Scholar] [CrossRef]
- Weissman, A.M.; Hartz, A.J.; Hansen, M.D.; Johnson, S.R. The natural history of primary dysmenorrhoea: A longitudinal study. BJOG 2004, 111, 345–352. [Google Scholar] [CrossRef]
- Nattiv, A.; Loucks, A.B.; Manore, M.M.; Sanborn, C.F.; Sundgot-Borgen, J.; Warren, M.P.; Medicine, A.C.o.S. American College of Sports Medicine position stand. The female athlete triad. Med. Sci. Sports Exerc. 2007, 39, 1867–1882. [Google Scholar] [CrossRef]
- Redman, L.M.; Loucks, A.B. Menstrual disorders in athletes. Sports Med. 2005, 35, 747–755. [Google Scholar] [CrossRef]
- Torstveit, M.K.; Sundgot-Borgen, J. Participation in leanness sports but not training volume is associated with menstrual dysfunction: A national survey of 1276 elite athletes and controls. Br. J. Sports Med. 2005, 39, 141–147. [Google Scholar] [CrossRef] [Green Version]
- De Souza, M.J.; Koltun, K.J.; Williams, N.I. The Role of Energy Availability in Reproductive Function in the Female Athlete Triad and Extension of its Effects to Men: An Initial Working Model of a Similar Syndrome in Male Athletes. Sports Med. 2019, 49, 125–137. [Google Scholar] [CrossRef]
- Thein-Nissenbaum, J. Long term consequences of the female athlete triad. Maturitas 2013, 75, 107–112. [Google Scholar] [CrossRef]
- Höök, M.; Bergström, M.; Sæther, S.A.; McGawley, K. “Do Elite Sport First, Get Your Period Back Later.” Are Barriers to Communication Hindering Female Athletes? Int. J. Environ. Res. Public Health 2021, 18, 2075. [Google Scholar] [CrossRef]
- Elliott-Sale, K.J.; McNulty, K.L.; Ansdell, P.; Goodall, S.; Hicks, K.M.; Thomas, K.; Swinton, P.A.; Dolan, E. The Effects of Oral Contraceptives on Exercise Performance in Women: A Systematic Review and Meta-analysis. Sports Med. 2020, 50, 1785–1812. [Google Scholar] [CrossRef]
- Brown, N.; Knight, C.J. Understanding female coaches’ and practitioners’ experience and support provision in relation to the menstrual cycle. J. Sports Sci. Coach. 2022, 17, 235–243. [Google Scholar] [CrossRef]
- Miller, S.M.; Kukuljan, S.; Turner, A.I.; van der Pligt, P.; Ducher, G. Energy deficiency, menstrual disturbances, and low bone mass: What do exercising Australian women know about the female athlete triad? Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 131–138. [Google Scholar] [CrossRef]
- Brown, K.N.; Wengreen, H.J.; Beals, K.A. Knowledge of the female athlete triad, and prevalence of triad risk factors among female high school athletes and their coaches. J. Pediatr. Adolesc. Gynecol. 2014, 27, 278–282. [Google Scholar] [CrossRef]
- Jowett, S. Coaching effectiveness: The coach-athlete relationship at its heart. Curr. Opin. Psychol. 2017, 16, 154–158. [Google Scholar] [CrossRef]
- Troy, K.; Hoch, A.Z.; Stavrakos, J.E. Awareness and comfort in treating the Female Athlete Triad: Are we failing our athletes? WMJ 2006, 105, 21–24. [Google Scholar]
- Javed, A.; Tebben, P.J.; Fischer, P.R.; Lteif, A.N. Female athlete triad and its components: Toward improved screening and management. Mayo Clin. Proc. 2013, 88, 996–1009. [Google Scholar] [CrossRef] [Green Version]
- Swedish Sports Confederation. Idrottsrörelsen i Siffror. Available online: https://www.rf.se/globalassets/riksidrottsforbundet/nya-dokument/nya-dokumentbanken/idrottsrorelsen-i-siffror/2020-idrotten-i-siffror---sisu.pdf?w=900&h=7002020 (accessed on 17 July 2022).
- Fasting, K.; Sisjord, M.K.; Sand, T.S. Norweigian elite-level coaches: Who are they. Scand. Sport Stud. Forum 2017, 8, 29–47. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| TEAM SPORTS | 627 (58) | Roller derby | 7 (1) |
| Soccer | 312 (29) | Athletics (discus, javelin) | 6 (1) |
| Handball | 243 (22) | Ski jumping | 6 (1) |
| Floorball | 42 (4) | Climbing | 4 (<1) |
| Basketball | 8 (1) | Rowing | 4 (<1) |
| Ice hockey | 8 (1) | Skateboarding | 4 (<1) |
| Volleyball | 6 (1) | Weightlifting | 4 (<1) |
| Rugby | 4 (<1) | Curling | 3 (<1) |
| Beach volleyball | 2 (<1) | Gym training | 3 (<1) |
| American football | 1 (<1) | Judo | 3 (<1) |
| Bandy | 1 (<1) | Badminton | 2 (<1) |
| _______________________ | ________ | Canoeing (sprint) | 2 (<1) |
| INDIVIDUAL SPORTS | 459 (42) | CrossFit | 2 (<1) |
| Orienteering | 94 (9) | Snowboarding | 2 (<1) |
| Cross-country skiing | 58 (5) | Ski orienteering | 2 (<1) |
| Swimming | 35 (3) | Tennis | 2 (<1) |
| Gymnastics | 31 (3) | Equestrian vaulting | 2 (<1) |
| Triathlon | 24 (2) | Wrestling | 2 (<1) |
| Powerlifting | 19 (2) | Aerobics | 1 (<1) |
| Cycling | 17 (2) | Enduro | 1 (<1) |
| Budo | 16 (1) | Free skiing | 1 (<1) |
| Alpine skiing | 15 (1) | Drill | 1 (<1) |
| Biathlon | 15 (1) | Golf | 1 (<1) |
| Figure skating | 14 (1) | Kick boxing | 1 (<1) |
| Athletics (sprint/jump) | 12 (1) | Rhythmic gymnastics | 1 (<1) |
| Athletics (distance running *) | 13 (1) | Shooting | 1 (<1) |
| Canoeing (distance) | 9 (1) | Ski cross | 1 (<1) |
| Equestrian | 8 (1) | Not indicated | 1 (<1) |
| Archery | 7 (1) |
| All Athletes (n = 1086) | Top-Elite (n = 158) | Elite (n = 393) | Sub-Elite (n = 535) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TEAM n = 627 (58) | IND n = 459 (42) | p-Value | TEAM n = 30 (19) | IND n = 128 (81) | p-Value | TEAM n = 146 (37) | IND n = 246 (63) | p-Value | TEAM n = 452 (84) | IND n = 83 (16) | p-Value | |
| Age, mean (SD) | 23.6 (6.3) | 24.8 (7.4) | 0.006 | 26.2 (0.7) | 26.7 (6.4) | 0.766 | 22.6 (5.0) | 22.8 (6.2) | 0.843 | 23.7 (6.7) | 27.9 (10.0) | <0.001 |
| BMI, mean (SD) | 23.6 (2.8) | 22.6 (9.0) | <0.001 | 23.6 (0.5) | 22.4 (2.6) | 0.013 | 23.5 (0.6) | 22.5 (2.6) | <0.001 | 23.5 (8.7) | 23.6 (3.6) | 0.805 |
| Sex of coach, n (%) | ||||||||||||
| Male | 489 (78) | 258 (56) | <0.001 | 25 (86) | 86 (67) | 0.082 | 113 (77) | 140 (57) | <0.001 | 337 (75) | 50 (60) | 0.007 |
| Female | 78 (12) | 65 (14) | 0.407 | 3 (10) | 12 (9) | 0.916 | 21 (15) | 40 (16) | 0.767 | 54 (12) | 14 (17) | 0.216 |
| Male and female | 45 (7) | 44 (9) | 0.191 | 1 (3) | 12 (9) | 0.278 | 9 (6) | 22 (9) | 0.330 | 35 (8) | 10 (12) | 0.194 |
| No main coach | 15 (2) | 93 (20) | <0.001 | 0 | 19 (15) | n.a. | 2 (1) | 44 (18) | <0.001 | 20 (4) | 9 (11) | 0.021 |
| Access to medical staff *, n (%) | ||||||||||||
| Medical staff, overall | 453 (72) | 331 (72) | 0.961 | 29 (97) | 112 (88) | 0.145 | 133 (91) | 181 (74) | <0.001 | 292 (65) | 40 (48) | 0.005 |
| Dietician | 61 (10) | 110 (24) | <0.001 | 17 (57) | 62 (48) | 0.417 | 21 (14) | 46 (18) | 0.280 | 24 (5) | 4 (5) | 0.854 |
| Gynecologist | 9 (1) | 20 (4) | 0.003 | 0 | 13 (10) | n.a. | 3 (2) | 7 (3) | 0.636 | 8 (2) | 1 (1) | 0.713 |
| Physician | 109 (17) | 142 (31) | <0.001 | 25 (83) | 72 (56) | 0.006 | 40 (27) | 63 (26) | 0.680 | 44 (10) | 8 (10) | 0.978 |
| Physiotherapist | 315 (50) | 195 (42) | 0.011 | 30 (100) | 81 (63) | <0.001 | 101 (69) | 101 (41) | <0.001 | 183 (40) | 16 (19) | <0.001 |
| Use of HC | 437 (70) | 242 (53) | <0.001 | 15 (50) | 57 (45) | 0.588 | 107 (73) | 128 (52) | <0.001 | 316 (70) | 41 (49) | <0.001 |
| Male Coach (n = 747) | Female Coach (n = 143) | p-Value | |
|---|---|---|---|
| Do talk about female athlete health with their coach, n (%) | 28 (4) | 78 (55) | 0.002 |
| Opportunity to discuss amenorrhea, n (%) | |||
| Never experienced amenorrhea | 155 (21) | 30 (21) | 0.559 |
| Discussed amenorrhea at least once | 143 (19) | 22 (15) | |
| Experienced amenorrhea | 298 (40) | 52 (36) | |
| Perception of coach’s knowledge, n (%) | |||
| Very good/good | 31 (5) | 31 (30) | <0.001 |
| Fair | 123 (19) | 48 (46) | |
| Very poor/poor | 484 (76) | 25 (24) | |
| Female athlete health is taboo in the athletic community, n (%) | |||
| Strongly agree/agree | 293 (41) | 58 (42) | 0.948 |
| Partly agree | 286 (40) | 53 (39) | |
| Disagree/strongly disagree | 138 (19) | 26 (19) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Rosen, P.; Ekenros, L.; Solli, G.S.; Sandbakk, Ø.; Holmberg, H.-C.; Hirschberg, A.L.; Fridén, C. Offered Support and Knowledge about the Menstrual Cycle in the Athletic Community: A Cross-Sectional Study of 1086 Female Athletes. Int. J. Environ. Res. Public Health 2022, 19, 11932. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191911932
von Rosen P, Ekenros L, Solli GS, Sandbakk Ø, Holmberg H-C, Hirschberg AL, Fridén C. Offered Support and Knowledge about the Menstrual Cycle in the Athletic Community: A Cross-Sectional Study of 1086 Female Athletes. International Journal of Environmental Research and Public Health. 2022; 19(19):11932. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191911932
Chicago/Turabian Stylevon Rosen, Philip, Linda Ekenros, Guro Strøm Solli, Øyvind Sandbakk, Hans-Christer Holmberg, Angelica Lindén Hirschberg, and Cecilia Fridén. 2022. "Offered Support and Knowledge about the Menstrual Cycle in the Athletic Community: A Cross-Sectional Study of 1086 Female Athletes" International Journal of Environmental Research and Public Health 19, no. 19: 11932. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191911932