
A Cross-Sectional, Questionnaire-Based Survey on Air Infection Control among Romanian People
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. The Survey
2.3. Study Group
2.4. Demographic Characteristics
2.5. Domain: Knowledge Data
2.6. Data Analysis
3. Results
3.1. Demographic Data
3.2. Assessing the Level of Knowledge Regarding Airborne Infection Transmission
3.3. Evaluation of the Level of Knowledge Regarding the Attitude of the Subjects in the Context of Airborne Infection Control
3.4. Evaluation of the Level of Knowledge Regarding the Attitude of the Subjects towards the Use of Protective Masks
3.5. Evaluation of the Level of Knowledge on the Compliance of the Subjects Regarding the Administration of Vaccines for Diseases Transmitted through the Air
4. Discussion
4.1. Assessment of the Level of Knowledge Regarding the Transmission of Infection by Air
4.2. Assessment of the Level of Knowledge Regarding the Attitude of the Subjects Regarding the Control of Airborne Infection
4.3. Assessing the Level of Knowledge Regarding the Attitude of Subjects towards the Use of Protective Masks
4.4. Assessing of the Level of Knowledge Regarding the Compliance of the Subjects According the Administration of Vaccines for Airborne Diseases
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Infection Prevention and Control of Epidemic- and Pandemic-Prone Acute Respiratory Infections in Health Care. 2014. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?adgroupsurvey={adgroupsurvey}&gclid=Cj0KCQjw1bqZBhDXARIsANTjCPLJlzyNX3iJKA9W6HV8IwgODYCXCQWmaWagg024ehRC9449Qxk2FWYaAg_UEALw_wcB (accessed on 18 August 2022).
- Li, X.; Ma, X. Acute respiratory failure in COVID-19: Is it “typical” ARDS? Crit. Care 2020, 24, 198. [Google Scholar] [CrossRef] [PubMed]
- Roehrig, S.; Ait Hssain, A.; Shallik, N.; Elsaid, I.; Mustafa, S.F.; Smain, O.; Molokhia, A.A.; Lance, M.D. Flow controlled ventilation in acute respiratory distress syndrome associated with COVID-19: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 781. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Adil, S.F.; Alkhathlan, H.Z.; Tahir, M.N.; Saif, S.; Khan, M.; Khan, S.T. COVID-19: A Global Challenge with Old History, Epidemiology and Progress So Far. Molecules 2020, 26, 39. [Google Scholar] [CrossRef] [PubMed]
- Rabaan, A.A.; Al-Ahmed, S.H.; Sah, R.; Tiwari, R.; Yatoo, M.I.; Patel, S.K.; Pathak, M.; Malik, Y.S.; Dhama, K.; Singh, K.P.; et al. SARS-CoV-2/COVID-19 and advances in developing potential therapeutics and vaccines to counter this emerging pandemic. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 40. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Emerging Microbial Threats to Health; Lederberg, J.; Shope, R.E.; Oaks, S.C., Jr. Emerging Infections: Microbial Threats to Health in the United, States; National Academies Press: Washington, DC, USA, 1992. [Google Scholar]
- Ghai, S. If COVID-19 becomes endemic will the current dental guidelines still remain valid? Oral Dis. 2021, 27 (Suppl. 3), 787–788. [Google Scholar] [CrossRef] [PubMed]
- Mattos, F.F.; Pordeus, I.A. COVID-19: A new turning point for dental practice. Braz. Oral Res. 2020, 34, e085. [Google Scholar] [CrossRef] [PubMed]
- Amato, A.; Caggiano, M.; Amato, M.; Moccia, G.; Capunzo, M.; De Caro, F. Infection Control in Dental Practice During the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 4769. [Google Scholar] [CrossRef]
- Lo Giudice, R. The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS CoV-2) in Dentistry. Management of Biological Risk in Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3067. [Google Scholar] [CrossRef]
- Peres, D.; Boléo-Tomé, J.P.; Santos, G. Proteção Facial e Respiratória: Perspetivas Atuais no Contexto da Pandemia por COVID-19 [Respiratory and Facial Protection: Current Perspectives in the Context of the COVID-19 Pandemic]. Acta Med. Port. 2020, 33, 583–592. [Google Scholar] [CrossRef]
- Conly, J.; Seto, W.H.; Pittet, D.; Holmes, A.; Chu, M.; Hunter, P.R.; WHO Infection Prevention and Control Research and Development Expert Group for COVID-19. Use of medical face masks versus particulate respirators as a component of personal protective equipment for health care workers in the context of the COVID-19 pandemic. Antimicrob. Resist. Infect. Control 2020, 9, 126. [Google Scholar] [CrossRef]
- Bennett, A.M.; Fulford, M.R.; Walker, J.T.; Bradshaw, D.J.; Martin, M.V.; Marsh, P.D. Microbial aerosols in general dental practice. Br. Dent. J. 2000, 189, 664–667. [Google Scholar] [CrossRef] [PubMed]
- Prospero, E.; Savini, S.; Annino, I. Microbial aerosol contamination of dental healthcare workers’ faces and other surfaces in dental practice. Infect. Control Hosp. Epidemiol. 2003, 24, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Liu, H.; Chu, C.; Li, X.; Liu, S.; Lu, S. Transmission routes of SARS-CoV-2 and protective measures in dental clinics during the COVID-19 pandemic. Am. J. Dent. 2020, 33, 129–134. [Google Scholar] [PubMed]
- Bauch, C.T.; Lloyd-Smith, J.O.; Coffee, M.P.; Galvani, A.P. Dynamically modeling SARS and other newly emerging respiratory illnesses: Past, present, and future. Epidemiology 2005, 16, 791–801. [Google Scholar] [CrossRef]
- Negucioiu, M.; Bucur, A.; Lucaciu, O.; Soanca, A.; Roman, A. Management of SARS-CoV-2 Transmission in Emergency Dental Settings: Current Knowledge and Personal Experience. Disaster Med. Public Health Prep. 2020, 16, 1604–1611. [Google Scholar] [CrossRef]
- Izzetti, R.; Nisi, M.; Gabriele, M.; Graziani, F. COVID-19 Transmission in Dental Practice: Brief Review of Preventive Measures in Italy. J. Dent. Res. 2020, 99, 1030–1038. [Google Scholar] [CrossRef]
- Storr, J.; Twyman, A.; Zingg, W.; Damani, N.; Kilpatrick, C.; Reilly, J.; Price, L.; Egger, M.; Grayson, M.L.; Kelley, E.; et al. Core components for effective infection prevention and control programmes: New WHO evidence-based recommendations. Antimicrob. Resist. Infect. Control 2017, 6, 6. [Google Scholar] [CrossRef]
- Jamal, M.; Shah, M.; Almarzooqi, S.H.; Aber, H.; Khawaja, S.; El Abed, R.; Alkhatib, Z.; Samaranayake, L.P. Overview of transnational recommendations for COVID-19 transmission control in dental care settings. Oral Dis. 2021, 27 (Suppl. 3), 655–664. [Google Scholar] [CrossRef]
- Migas, K.; Marczak, M.; Kozłowski, R.; Kot, A.; Wysocka, A.; Sierocka, A. Impact of the COVID-19 Pandemic on the Dental Preferences of Patients in the Private Sector. Int. J. Environ. Res. Public Health 2022, 19, 2183. [Google Scholar] [CrossRef]
- Zingg, W.; Storr, J.; Park, B.J.; Ahmad, R.; Tarrant, C.; Castro-Sanchez, E.; Tomczyk, S.; Kilpatrick, C.; Allegranzi, B.; Cardo, D.; et al. Implementation research for the prevention of antimicrobial resistance and healthcare-associated infections; 2017 Geneva infection prevention and control (IPC)-think tank (part 1). Antimicrob. Resist. Infect. Control 2019, 8, 87. [Google Scholar] [CrossRef] [Green Version]
- Xia, F.; Hughes, J.P.; Voldal, E.C.; Heagerty, P.J. Power and sample size calculation for stepped-wedge designs with discrete outcomes. Trials 2021, 22, 598. [Google Scholar] [CrossRef] [PubMed]
- Likert-Scale-Response-Options_MWCC. Available online: https://mwcc.edu/wp-content/uploads/2020/09/Likert-Scale-Response-Options_MWCC.pdf (accessed on 18 May 2022).
- Razavi, M.; Butt, Z.A.; Chen, H.; Tan, Z. In Situ Measurement of Airborne Particle Concentration in a Real Dental Office: Implications for Disease Transmission. Int. J. Environ. Res. Public Health 2021, 18, 8955. [Google Scholar] [CrossRef] [PubMed]
- Resendiz, M.; Blanchard, D.M.; Lustik, M.B.; Horseman, T.S.; West, G.F. Effect of SARs-CoV-2 pandemic on infection prevention behaviors and bacterial burden of high touch surfaces in a medical/surgical setting. Sci. Rep. 2022, 12, 5561. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Environmental Disinfection of a Dental Clinic during the Covid-19 Pandemic: A Narrative Insight. BioMed Res. Int. 2020, 2020, 8896812. [Google Scholar] [CrossRef]
- Tysiąc-Miśta, M.; Dubiel, A.; Brzoza, K.; Burek, M.; Pałkiewicz, K. Air disinfection procedures in the dental office during the COVID-19 pandemic. Med. Pr. 2021, 72, 39–48. [Google Scholar] [CrossRef]
- Ibrahim, N.K.; Alwafi, H.A.; Sangoof, S.O.; Turkistani, A.K.; Alattas, B.M. Cross-infection and infection control in dentistry: Knowledge, attitude and practice of patients attended dental clinics in King Abdulaziz University Hospital, Jeddah, Saudi Arabia. J. Infect. Public Health 2017, 10, 438–445. [Google Scholar] [CrossRef]
- Kajal, K.; Mohammadnezhad, M. Behavioral Preventative Strategies Undertaken by Dental Clinics in Fiji during COVID-19 Pandemic. J. Int. Soc. Prev. Community Dent. 2022, 12, 376–384. [Google Scholar] [CrossRef]
- Gurgel, B.; Borges, S.B.; Borges, R.; Calderon, P. COVID-19: Perspectives for the management of dental care and education. J. Appl. Oral Sci. Rev. FOB 2020, 28, e20200358. [Google Scholar] [CrossRef]
- Tysiąc-Miśta, M.; Dziedzic, A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 4703. [Google Scholar] [CrossRef]
- Adhikari, S.P.; Meng, S.; Wu, Y.J.; Mao, Y.P.; Ye, R.X.; Wang, Q.Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.; Jernigan, D.B.; 2019-nCoV CDC Response Team. Initial Public Health Response and Interim Clinical Guidance for the 2019 Novel Coronavirus Outbreak—United States, 31 December 2019–4 February 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Sukumar, S.; Dracopoulos, S.A.; Martin, F.E. Dental education in the time of SARS-CoV-2. Eur. J. Dent. Educ. Off. J. Assoc. Dent. Educ. Eur. 2021, 25, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Deery, C. The COVID-19 pandemic: Implications for dental education. Evid.-Based Dent. 2020, 21, 46–47. [Google Scholar] [CrossRef] [PubMed]
- Iyer, P.; Aziz, K.; Ojcius, D.M. Impact of COVID-19 on dental education in the United States. J. Dent. Educ. 2020, 84, 718–722. [Google Scholar] [CrossRef]
- Mahida, N. Hand hygiene compliance: Are we kidding ourselves? J. Hosp. Infect. 2016, 92, 307–308. [Google Scholar] [CrossRef]
- Carrouel, F.; Gonçalves, L.S.; Conte, M.P.; Campus, G.; Fisher, J.; Fraticelli, L.; Gadea-Deschamps, E.; Ottolenghi, L.; Bourgeois, D. Antiviral Activity of Reagents in Mouth Rinses against SARS-CoV-2. J. Dent. Res. 2021, 100, 124–132. [Google Scholar] [CrossRef]
- Davies, K.; Buczkowski, H.; Welch, S.R.; Green, N.; Mawer, D.; Woodford, N.; Roberts, A.; Nixon, P.J.; Seymour, D.W.; Killip, M.J. Effective in vitro inactivation of SARS-CoV-2 by commercially available mouthwashes. J. Gen. Virol. 2021, 102, 001578. [Google Scholar] [CrossRef]
- Seneviratne, C.J.; Balan, P.; Ko, K.; Udawatte, N.S.; Lai, D.; Ng, D.; Venkatachalam, I.; Lim, K.S.; Ling, M.L.; Oon, L.; et al. Efficacy of commercial mouth-rinses on SARS-CoV-2 viral load in saliva: Randomized control trial in Singapore. Infection 2021, 49, 305–311. [Google Scholar] [CrossRef]
- Vergara-Buenaventura, A.; Castro-Ruiz, C. Use of mouthwashes against COVID-19 in dentistry. Br. J. Oral Maxillofac. Surg. 2020, 58, 924–927. [Google Scholar] [CrossRef]
- Ferrer, M.D.; Barrueco, Á.S.; Martinez-Beneyto, Y.; Mateos-Moreno, M.V.; Ausina-Márquez, V.; García-Vázquez, E.; Puche-Torres, M.; Giner, M.; González, A.C.; Coello, J.; et al. Clinical evaluation of antiseptic mouth rinses to reduce salivary load of SARS-CoV-2. Sci. Rep. 2021, 11, 24392. [Google Scholar] [CrossRef]
- Gandhi, G.; Thimmappa, L.; Upadhya, N.; Carnelio, S. Could mouth rinses be an adjuvant in the treatment of SARS-CoV-2 patients? An appraisal with a systematic review. Int. J. Dent. Hyg. 2022, 20, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Liang, M.; Gao, L.; Cheng, C.; Zhou, Q.; Uy, J.P.; Heiner, K.; Sun, C. Efficacy of face mask in preventing respiratory virus transmission: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 36, 101751. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.B.; Skaria, S.D.; Mansour, M.M.; Smaldone, G.C. Respiratory source control using a surgical mask: An in vitro study. J. Occup. Environ. Hyg. 2016, 13, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Grinshpun, S.A.; Haruta, H.; Eninger, R.M.; Reponen, T.; McKay, R.T.; Lee, S.A. Performance of an N95 filtering facepiece particulate respirator and a surgical mask during human breathing: Two pathways for particle penetration. J. Occup. Environ. Hyg. 2009, 6, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Rengasamy, S.; Eimer, B.C.; Szalajda, J. A quantitative assessment of the total inward leakage of NaCl aerosol representing submicron-size bioaerosol through N95 filtering facepiece respirators and surgical masks. J. Occup. Environ. Hyg. 2014, 11, 388–396. [Google Scholar] [CrossRef]
- Cho, K.J.; Reponen, T.; McKay, R.; Shukla, R.; Haruta, H.; Sekar, P.; Grinshpun, S.A. Large particle penetration through N95 respirator filters and facepiece leaks with cyclic flow. Ann. Occup. Hyg. 2010, 54, 68–77. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Reponen, T.; McKay, R.T.; Grinshpun, S.A. Effect of Particle Size on the Performance of an N95 Filtering Facepiece Respirator and a Surgical Mask at Various Breathing Conditions. Aerosol Sci. Technol. J. Am. Assoc. Aerosol Res. 2013, 47, 1180–1187. [Google Scholar] [CrossRef]
- He, X.; Reponen, T.; McKay, R.; Grinshpun, S.A. How does breathing frequency affect the performance of an N95 filtering facepiece respirator and a surgical mask against surrogates of viral particles? J. Occup. Environ. Hyg. 2014, 11, 178–185. [Google Scholar] [CrossRef]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.; Pollard, A.J. What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect. Dis. 2021, 21, e26–e35. [Google Scholar] [CrossRef]
- Martinez, L.; Cords, O.; Liu, Q.; Acuna-Villaorduna, C.; Bonnet, M.; Fox, G.J.; Carvalho, A.; Chan, P.C.; Croda, J.; Hill, P.C.; et al. Infant BCG vaccination and risk of pulmonary and extrapulmonary tuberculosis throughout the life course: A systematic review and individual participant data meta-analysis. Lancet Glob. Health 2022, 10, e1307–e1316. [Google Scholar] [CrossRef]
- Vasireddy, D.; Vanaparthy, R.; Mohan, G.; Malayala, S.V.; Atluri, P. Review of COVID-19 Variants and COVID-19 Vaccine Efficacy: What the Clinician Should Know? J. Clin. Med. Res. 2021, 13, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease 2019 Cancer Collaboration; Kocarnik, J.M.; Compton, K.; Dean, F.E.; Fu, W.; Gaw, B.L.; Harvey, J.D.; Henrikson, H.J.; Lu, D.; Pennini, A.; et al. Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef] [PubMed]
- Martinez, L.; Cords, O.; Horsburgh, C.R.; Andrews, J.R.; Pediatric TB Contact Studies Consortium. The risk of tuberculosis in children after close exposure: A systematic review and individual-participant meta-analysis. Lancet 2020, 395, 973–984. [Google Scholar] [CrossRef]
- Vonasek, B.; Ness, T.; Takwoingi, Y.; Kay, A.W.; van Wyk, S.S.; Ouellette, L.; Marais, B.J.; Steingart, K.R.; Mandalakas, A.M. Screening tests for active pulmonary tuberculosis in children. Cochrane Database Syst. Rev. 2021, 6, CD013693. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Question | Total | Gender | p | χ2 | Environment | p | χ2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | Female | Male | Rural | Urban | |||||||||
| N | % | N | % | N | % | N | % | |||||||
| Q 4 = Do you believe that the dental team is required to wear protective equipment even if you are healthy? | ||||||||||||||
| Strongly Agree | 124 | 61.39 | 74 | 36.63 | 50 | 24.75 | 0.955 a, b | 0.67 | 49 | 24.26 | 75 | 37.13 | 0.271 a, b | 5.16 |
| Agree | 60 | 29.70 | 35 | 17.33 | 25 | 12.38 | 22 | 10.89 | 38 | 18.81 | ||||
| Undecided | 13 | 6.44 | 9 | 4.46 | 4 | 1.98 | 7 | 3.47 | 6 | 2.97 | ||||
| Disagree | 2 | 0.99 | 1 | 0.50 | 1 | 0.50 | 2 | 0.99 | 0 | 0.00 | ||||
| Strongly Disagree | 3 | 1.49 | 2 | 0.99 | 1 | 0.50 | 2 | 0.99 | 1 | 0.50 | ||||
| Q 5 = Do you consider the dentist’s office a source of airborne infection? | ||||||||||||||
| Strongly Agree | 21 | 10.40 | 12 | 5.94 | 9 | 4.46 | 0.847 | 1.38 | 5 | 2.48 | 16 | 7.92 | 0.570 | 2.93 |
| Agree | 37 | 18.32 | 23 | 11.39 | 14 | 6.93 | 15 | 7.43 | 22 | 10.89 | ||||
| Undecided | 61 | 30.20 | 37 | 18.32 | 24 | 11.88 | 27 | 13.37 | 34 | 16.83 | ||||
| Disagree | 58 | 28.71 | 32 | 15.84 | 26 | 12.87 | 24 | 11.88 | 34 | 16.83 | ||||
| Strongly Disagree | 25 | 12.38 | 17 | 8.42 | 8 | 3.96 | 11 | 5.45 | 14 | 6.93 | ||||
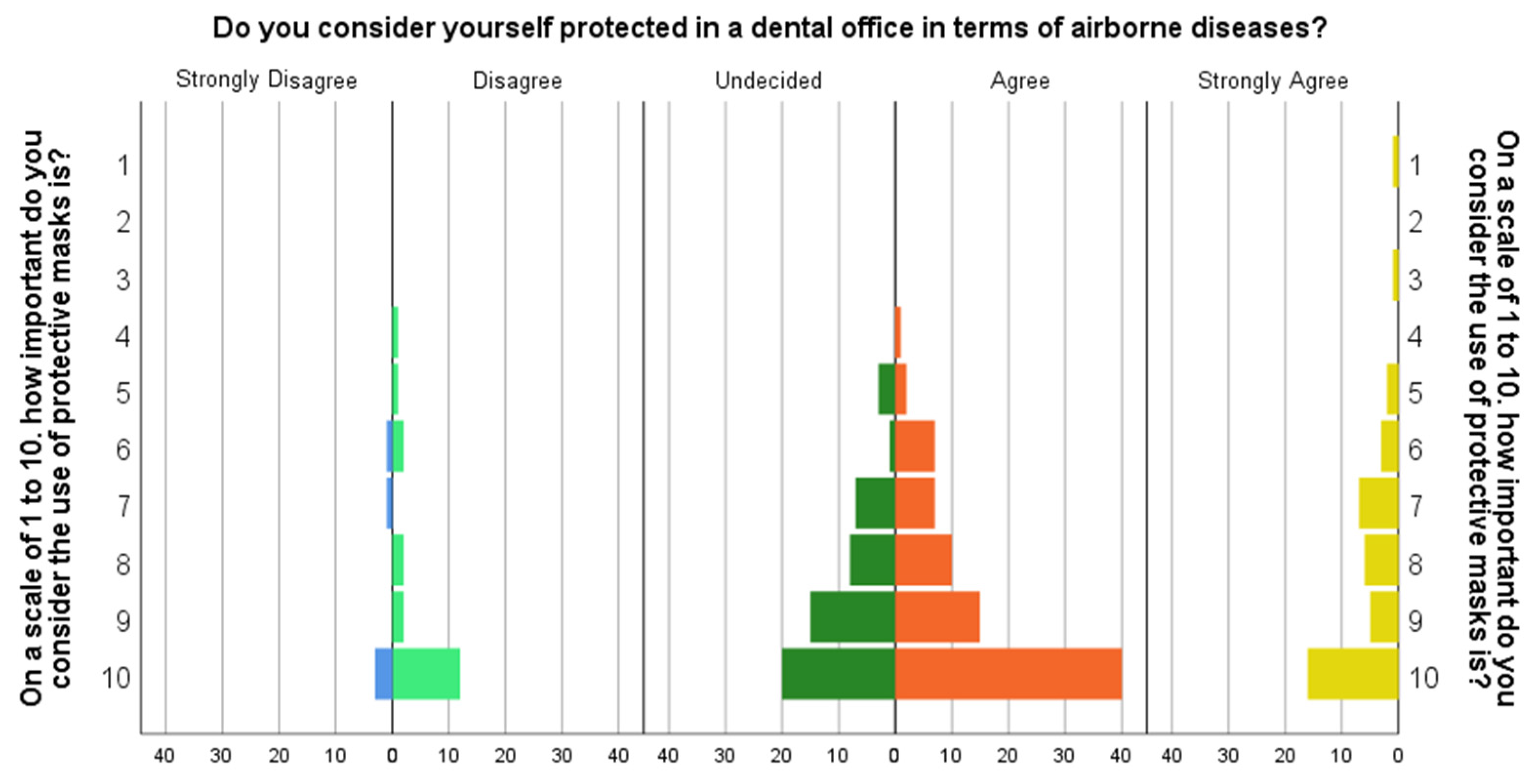
| Q 6 = Do you consider yourself protected in a dental office in terms of airborne diseases? | ||||||||||||||
| Strongly Agree | 41 | 20.30 | 21 | 10.40 | 20 | 9.90 | 0.493 a | 3.40 | 15 | 7.43 | 26 | 12.87 | 0.309 a | 4.80 |
| Agree | 82 | 40.59 | 47 | 23.27 | 35 | 17.33 | 29 | 14.36 | 53 | 26.24 | ||||
| Undecided | 54 | 26.73 | 37 | 18.32 | 17 | 8.42 | 27 | 13.37 | 27 | 13.37 | ||||
| Disagree | 20 | 9.90 | 13 | 6.44 | 7 | 3.47 | 10 | 4.95 | 10 | 4.95 | ||||
| Strongly Disagree | 5 | 2.48 | 3 | 1.49 | 2 | 0.99 | 1 | 0.50 | 4 | 1.98 | ||||
| Q7 = Did you know that respiratory infections can be transmitted when you talk? | ||||||||||||||
| Strongly Agree | 81 | 40.10 | 47 | 23.27 | 34 | 16.83 | 0.677 a | 2.32 | 24 | 11.88 | 57 | 28.22 | 0.055 a | 9.25 |
| Agree | 89 | 44.06 | 51 | 25.25 | 38 | 18.81 | 42 | 20.79 | 47 | 23.27 | ||||
| Undecided | 22 | 10.89 | 16 | 7.92 | 6 | 2.97 | 9 | 4.455 | 13 | 6.436 | ||||
| Disagree | 7 | 3.47 | 5 | 2.48 | 2 | 0.99 | 5 | 2.475 | 2 | 0.99 | ||||
| Strongly Disagree | 3 | 1.49 | 2 | 0.99 | 1 | 0.495 | 2 | 0.99 | 1 | 0.495 | ||||
| Q 8 = Do you think that an outpatient diagnosed with TB under treatment is contagious? | ||||||||||||||
| Strongly Agree | 51 | 25.25 | 29 | 14.36 | 22 | 10.89 | 0.413 a | 3.95 | 16 | 7.921 | 35 | 17.33 | 0.370 a | 4.28 |
| Agree | 76 | 37.62 | 42 | 20.79 | 34 | 16.83 | 32 | 15.84 | 44 | 21.78 | ||||
| Undecided | 50 | 24.75 | 31 | 15.35 | 19 | 9.406 | 23 | 11.39 | 27 | 13.37 | ||||
| Disagree | 19 | 9.41 | 15 | 7.43 | 4 | 1.98 | 7 | 3.465 | 12 | 5.941 | ||||
| Strongly Disagree | 6 | 2.97 | 4 | 1.98 | 2 | 0.99 | 4 | 1.98 | 2 | 0.99 | ||||
| Q 9 = Do you think that the airing of the space where you usually sit is sufficient for air decontamination? | ||||||||||||||
| Strongly Agree | 32 | 15.84 | 17 | 8.42 | 15 | 7.43 | 0.799 a | 1.653 | 11 | 5.45 | 21 | 10.40 | 0.390 a | 4.119 |
| Agree | 66 | 32.67 | 42 | 20.79 | 24 | 11.88 | 29 | 14.36 | 37 | 18.32 | ||||
| Undecided | 63 | 31.19 | 36 | 17.82 | 27 | 13.37 | 21 | 10.40 | 42 | 20.79 | ||||
| Disagree | 37 | 18.32 | 23 | 11.39 | 14 | 6.93 | 19 | 9.41 | 18 | 8.91 | ||||
| Strongly Disagree | 4 | 1.98 | 3 | 1.49 | 1 | 0.50 | 2 | 0.99 | 2 | 0.99 | ||||
| Question | Total | Gender | p | χ2 | Environment | p | χ2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | Female | Male | Rural | Urban | |||||||||
| N | % | N | % | N | % | N | % | |||||||
| Q 10 = Do you think it is important to inform the dentist when you suffer from an infection transmitted by air? | ||||||||||||||
| Unimportant | 2 | 0.99 | 1 | 0.50 | 1 | 0.50 | 0.799 a, b | 1.01 | 1 | 0.50 | 1 | 0.50 | 0.868 a, b | 0.72 |
| Slightly Important | 12 | 5.94 | 6 | 2.97 | 6 | 2.97 | 4 | 1.98 | 8 | 3.96 | ||||
| Important | 66 | 32.67 | 38 | 18.81 | 28 | 13.86 | 29 | 14.36 | 37 | 18.32 | ||||
| Very Important | 122 | 60.40 | 76 | 37.62 | 46 | 22.77 | 48 | 23.76 | 74 | 36.63 | ||||
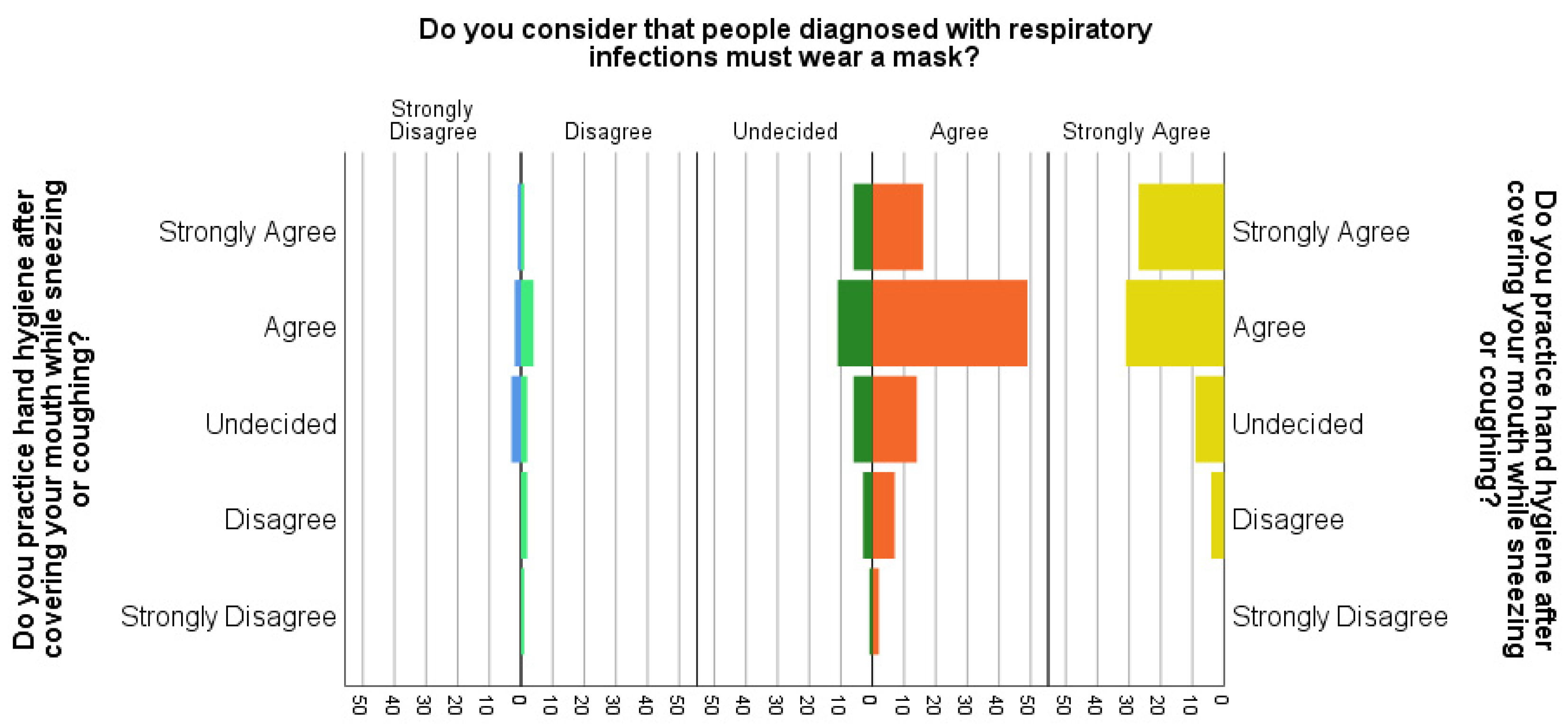
| Q 11 = Do you practice hand hygiene after covering your mouth while sneezing or coughing? | ||||||||||||||
| Strongly Agree | 51 | 25.25 | 32 | 15.84 | 19 | 9.41 | 0.953 a | 0.69 | 23 | 11.39 | 28 | 13.86 | 0.158 a | 6.61 |
| Agree | 97 | 48.02 | 59 | 29.21 | 38 | 18.81 | 34 | 16.83 | 63 | 31.19 | ||||
| Undecided | 34 | 16.83 | 19 | 9.41 | 15 | 7.43 | 18 | 8.91 | 16 | 7.92 | ||||
| Disagree | 16 | 7.92 | 9 | 4.46 | 7 | 3.47 | 7 | 3.47 | 9 | 4.46 | ||||
| Strongly Disagree | 4 | 1.98 | 2 | 0.99 | 2 | 0.99 | 0 | 0.00 | 4 | 1.98 | ||||
| Q 12 = Do you use mouthwash on a daily basis? | ||||||||||||||
| Strongly Agree | 30 | 14.85 | 22 | 10.89 | 8 | 3.96 | 0.111 | 7.51 | 9 | 4.46 | 21 | 10.40 | 0.318 | 4.71 |
| Agree | 62 | 30.69 | 34 | 16.83 | 28 | 13.86 | 25 | 12.38 | 37 | 18.32 | ||||
| Undecided | 46 | 22.77 | 22 | 10.89 | 24 | 11.88 | 16 | 7.92 | 30 | 14.85 | ||||
| Disagree | 46 | 22.77 | 32 | 15.84 | 14 | 6.93 | 22 | 10.89 | 24 | 11.88 | ||||
| Strongly Disagree | 18 | 8.91 | 11 | 5.45 | 7 | 3.47 | 10 | 4.95 | 8 | 3.96 | ||||
| Question | Total | Gender | p | χ2 | Environment | p | χ2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | Female | Male | Rural | Urban | |||||||||
| N | % | N | % | N | % | N | % | |||||||
| Q 13 = On a scale of 1 to 10. how important do you consider the use of protective masks is? | ||||||||||||||
| 1 | 1 | 0.50 | 1 | 0.50 | 0 | 0.00 | 0.155 a, b | 11.91 | 0 | 0.00 | 1 | 0.50 | 0.332 a, b | 9.12 |
| 2 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | ||||
| 3 | 1 | 0.50 | 0 | 0.00 | 1 | 0.50 | 1 | 0.50 | 0 | 0.00 | ||||
| 4 | 2 | 0.99 | 0 | 0.00 | 2 | 0.99 | 0 | 0.00 | 2 | 0.99 | ||||
| 5 | 8 | 3.96 | 6 | 2.97 | 2 | 0.99 | 6 | 2.97 | 2 | 0.99 | ||||
| 6 | 14 | 6.93 | 9 | 4.46 | 5 | 2.48 | 6 | 2.97 | 8 | 3.96 | ||||
| 7 | 22 | 10.89 | 10 | 4.95 | 12 | 5.94 | 9 | 4.46 | 13 | 6.44 | ||||
| 8 | 26 | 12.87 | 12 | 5.94 | 14 | 6.93 | 8 | 3.96 | 18 | 8.91 | ||||
| 9 | 37 | 18.32 | 22 | 10.89 | 15 | 7.43 | 17 | 8.42 | 20 | 9.90 | ||||
| 10 | 91 | 45.05 | 61 | 30.20 | 30 | 14.85 | 35 | 17.33 | 56 | 27.72 | ||||
| Q 14 = When purchasing a mask, do you take into account its cost? | ||||||||||||||
| Strongly Agree | 33 | 16.34 | 19 | 9.41 | 14 | 6.93 | 0.735 a | 2.00 | 17 | 8.42 | 16 | 7.92 | 0.194 a | 6.06 |
| Agree | 80 | 39.60 | 46 | 22.77 | 34 | 16.83 | 30 | 14.85 | 50 | 24.75 | ||||
| Undecided | 58 | 28.71 | 39 | 19.31 | 19 | 9.41 | 26 | 12.87 | 32 | 15.84 | ||||
| Disagree | 23 | 11.39 | 13 | 6.44 | 10 | 4.95 | 5 | 2.48 | 18 | 8.91 | ||||
| Strongly Disagree | 8 | 3.96 | 4 | 1.98 | 4 | 1.98 | 4 | 1.98 | 4 | 1.98 | ||||
| Q 15 = When choosing a protective mask, do you take its filtering capacity into account? | ||||||||||||||
| Strongly Agree | 33 | 16.34 | 24 | 11.88 | 9 | 4.46 | 0.498 | 3.37 | 11 | 5.45 | 22 | 10.89 | 0.356 | 4.39 |
| Agree | 70 | 34.65 | 39 | 19.31 | 31 | 15.35 | 31 | 15.35 | 39 | 19.31 | ||||
| Undecided | 62 | 30.69 | 36 | 17.82 | 26 | 12.87 | 24 | 11.88 | 38 | 18.81 | ||||
| Disagree | 27 | 13.37 | 17 | 8.42 | 10 | 4.95 | 14 | 6.93 | 13 | 6.44 | ||||
| Strongly Disagree | 10 | 4.95 | 5 | 2.48 | 5 | 2.48 | 2 | 0.99 | 8 | 3.96 | ||||
| Q 16 = When choosing a mask, do you take its breathing capacity into account? | ||||||||||||||
| Strongly Agree | 50 | 24.75 | 39 | 19.31 | 11 | 5.45 | 0.031 a, * | 10.62 | 17 | 8.42 | 33 | 16.34 | 0.589 a | 2.82 |
| Agree | 64 | 31.68 | 37 | 18.32 | 27 | 13.37 | 26 | 12.87 | 38 | 18.81 | ||||
| Undecided | 55 | 27.23 | 28 | 13.86 | 27 | 13.37 | 25 | 12.38 | 30 | 14.85 | ||||
| Disagree | 25 | 12.38 | 14 | 6.93 | 11 | 5.45 | 12 | 5.94 | 13 | 6.44 | ||||
| Strongly Disagree | 8 | 3.96 | 3 | 1.49 | 5 | 2.48 | 2 | 0.99 | 6 | 2.97 | ||||
| Q 17 = How long do you think that a surgical mask offers you protection against the transmission of infection through the air? | ||||||||||||||
| 30 min | 27 | 13.37 | 16 | 7.92 | 11 | 5.45 | 0.060 | 10.59 | 14 | 6.93 | 13 | 6.44 | 0.190 | 7.44 |
| 1 h | 37 | 18.32 | 23 | 11.39 | 14 | 6.93 | 20 | 9.90 | 17 | 8.42 | ||||
| 2 h | 46 | 22.77 | 21 | 10.40 | 25 | 12.38 | 13 | 6.44 | 33 | 16.34 | ||||
| 3 h | 38 | 18.81 | 29 | 14.36 | 9 | 4.46 | 14 | 6.93 | 24 | 11.88 | ||||
| 4 h | 47 | 23.27 | 26 | 12.87 | 21 | 10.40 | 18 | 8.91 | 29 | 14.36 | ||||
| All the time unless it is damaged | 7 | 3.47 | 6 | 2.97 | 1 | 0.50 | 3 | 1.49 | 4 | 1.98 | ||||
| Q 18 = Do you think the removal of protective masks from crowded spaces is putting you at risk? | ||||||||||||||
| Strongly Agree | 43 | 21.29 | 23 | 11.39 | 20 | 9.90 | 0.135 a | 7.02 | 19 | 9.41 | 24 | 11.88 | 0.347 a | 4.46 |
| Agree | 87 | 43.07 | 53 | 26.24 | 34 | 16.83 | 40 | 19.80 | 47 | 23.27 | ||||
| Undecided | 48 | 23.76 | 33 | 16.34 | 15 | 7.43 | 15 | 7.43 | 33 | 16.34 | ||||
| Disagree | 18 | 8.91 | 7 | 3.47 | 11 | 5.45 | 5 | 2.48 | 13 | 6.44 | ||||
| Strongly Disagree | 6 | 2.97 | 5 | 2.48 | 1 | 0.50 | 3 | 1.49 | 3 | 1.49 | ||||
| Q 19 = Do you consider that people diagnosed with respiratory infections must wear a mask? | ||||||||||||||
| Strongly Agree | 71 | 35.15 | 44 | 21.78 | 27 | 13.37 | 0.693 a | 0.693 a | 27 | 13.37 | 44 | 21.78 | 0.714 a | 0.714 a |
| Agree | 88 | 43.56 | 48 | 23.76 | 40 | 19.80 | 36 | 17.82 | 52 | 25.74 | ||||
| Undecided | 27 | 13.37 | 18 | 8.91 | 9 | 4.46 | 10 | 4.95 | 17 | 8.42 | ||||
| Disagree | 10 | 4.95 | 7 | 3.47 | 3 | 1.49 | 6 | 2.97 | 4 | 1.98 | ||||
| Strongly Disagree | 6 | 2.97 | 4 | 1.98 | 2 | 0.99 | 3 | 1.49 | 3 | 1.49 | ||||
| Question | Total | Gender | p | χ2 | Environment | p | χ2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | Female | Male | Rural | Urban | |||||||||
| N | % | N | % | N | % | N | % | |||||||
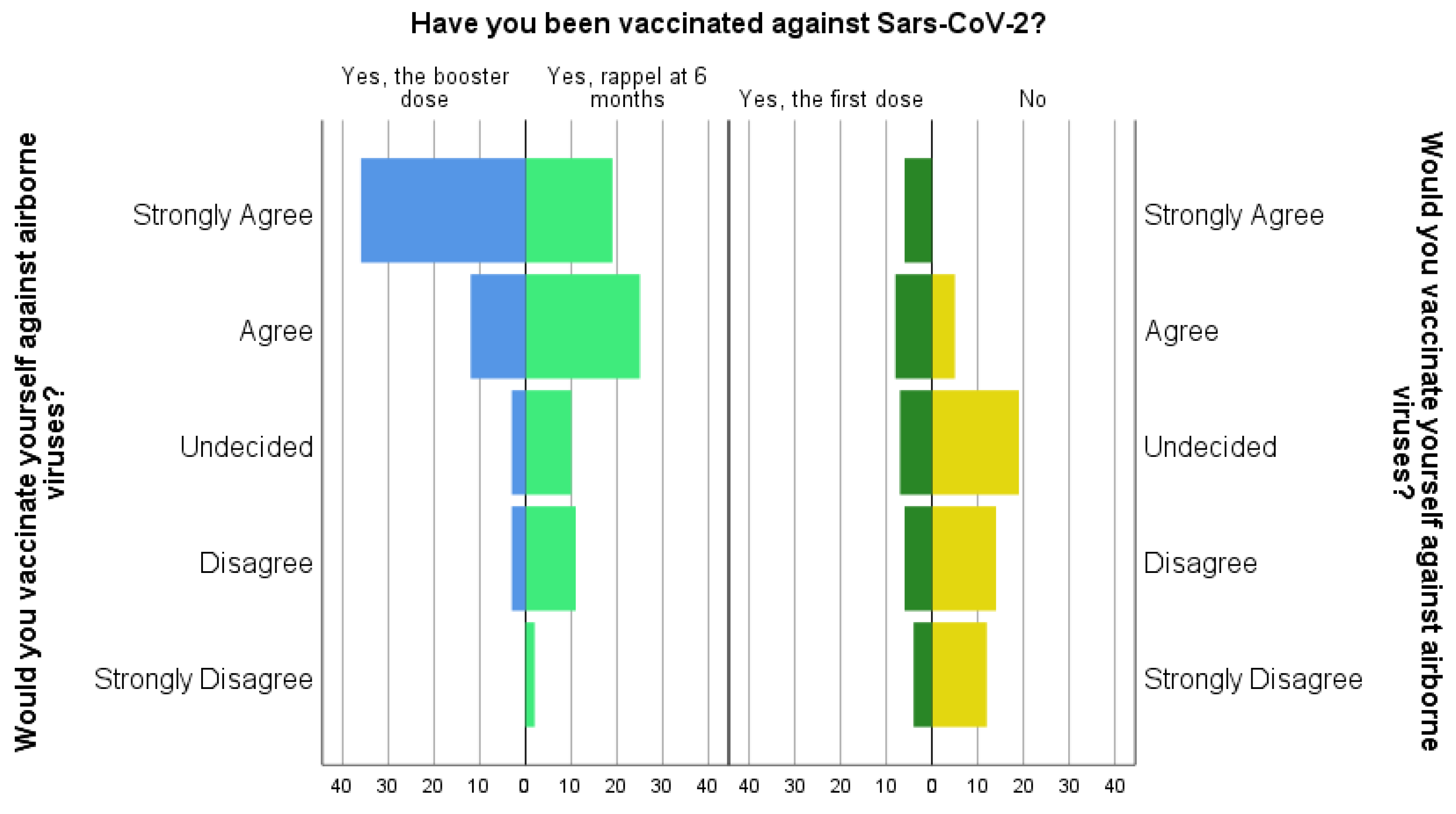
| Q 20 = Would you vaccinate yourself against airborne viruses? | ||||||||||||||
| Strongly Agree | 61 | 30.20 | 39 | 19.31 | 22 | 10.89 | 0.412 | 3.96 | 22 | 10.89 | 39 | 19.31 | 0.519 | 3.24 |
| Agree | 50 | 24.75 | 27 | 13.37 | 23 | 11.39 | 22 | 10.89 | 28 | 13.86 | ||||
| Undecided | 39 | 19.31 | 22 | 10.89 | 17 | 8.42 | 16 | 7.92 | 23 | 11.39 | ||||
| Disagree | 34 | 16.83 | 19 | 9.41 | 15 | 7.43 | 17 | 8.42 | 17 | 8.42 | ||||
| Strongly Disagree | 18 | 8.91 | 14 | 6.93 | 4 | 1.98 | 5 | 2.48 | 13 | 6.44 | ||||
| Q 21 = Have you been vaccinated against Sars-CoV-2? | ||||||||||||||
| No | 50 | 24.75 | 33 | 16.34 | 17 | 8.42 | 0.615 | 1.80 | 18 | 8.91 | 32 | 15.84 | 0.010 * | 11.29 |
| Yes, the first dose | 31 | 15.35 | 20 | 9.90 | 11 | 5.45 | 21 | 10.40 | 10 | 4.95 | ||||
| Yes, rappel at 6 months | 67 | 33.17 | 37 | 18.32 | 30 | 14.85 | 23 | 11.39 | 44 | 21.78 | ||||
| Yes, the booster dose | 54 | 26.73 | 31 | 15.35 | 23 | 11.39 | 20 | 9.90 | 34 | 16.83 | ||||
| Q 22 = Are you vaccinated against tuberculosis? | ||||||||||||||
| Yes | 58 | 28.71 | 34 | 16.83 | 24 | 11.88 | 0.972 | 0.06 | 19 | 9.41 | 39 | 19.31 | 0.278 | 2.56 |
| No | 71 | 35.15 | 43 | 21.29 | 28 | 13.86 | 29 | 14.36 | 42 | 20.79 | ||||
| I do not know | 73 | 36.14 | 44 | 21.78 | 29 | 14.36 | 34 | 16.83 | 39 | 19.31 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saveanu, C.I.; Zetu, I.N.; Scheuleac, A.; Saveanu, A.E.; Romanec, C.L. A Cross-Sectional, Questionnaire-Based Survey on Air Infection Control among Romanian People. Int. J. Environ. Res. Public Health 2022, 19, 12140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912140
Saveanu CI, Zetu IN, Scheuleac A, Saveanu AE, Romanec CL. A Cross-Sectional, Questionnaire-Based Survey on Air Infection Control among Romanian People. International Journal of Environmental Research and Public Health. 2022; 19(19):12140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912140
Chicago/Turabian StyleSaveanu, Catalina Iulia, Irina Nicoleta Zetu, Alexandra Scheuleac, Alexandra Ecaterina Saveanu, and Cristian Liviu Romanec. 2022. "A Cross-Sectional, Questionnaire-Based Survey on Air Infection Control among Romanian People" International Journal of Environmental Research and Public Health 19, no. 19: 12140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912140