
Spatio-Temporal Variation of Lung Cancer in Crete, 1992–2013. Economic or Health Crisis?
 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Study Population
2.2. Incidence and Mortality Rates and Other Indexes
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
3.1. Changing Trends of LC and Associated Factors before and after the Economic Crisis
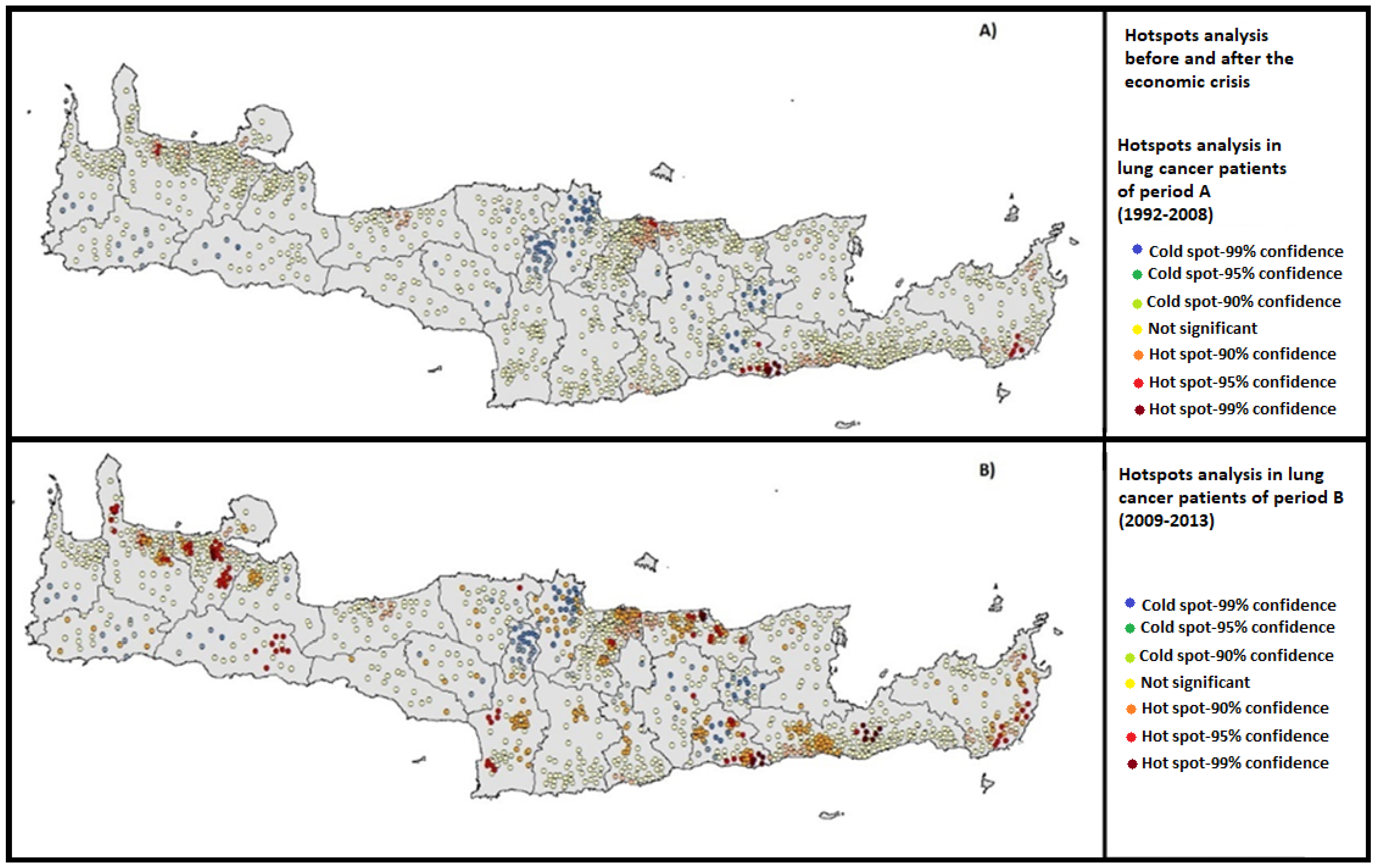
3.2. LC Hot Spots before and after the Economic Crisis
3.3. Predictors and Overall Risk of LC Mortality
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Otker-Robe, I.; Podpiera, A. The Social Impact of Financial Crises: Evidence from the Global Financial Crisis; Policy Research Working Paper No. 6703; World Bank: Washington, DC, USA, 2013. [Google Scholar]
- Karanikolos, M.; Mladovsky, P.; Cylus, J.; Thomson, S.; Basu, S.; Stuckler, D.; Mackenbach, J.P.; McKee, M. Financial crisis, austerity, and health in Europe. Lancet 2013, 381, 1323–1331. [Google Scholar] [CrossRef]
- Stuckler, D.; Basu, S.; Suhrcke, M.; Coutts, A.; McKee, M. The public health effect of economic crises and alternative policy responses in Europe: An empirical analysis. Lancet 2009, 374, 315–323. [Google Scholar] [CrossRef]
- Economou, C.; Kaitelidou, D.; Kentikelenis, A.; Maresso, A.; Sissouras, A. The Impact of the Financial Crisis on the Health System and Health in Greece; World Health Organization and European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2014. [Google Scholar]
- Zavras, D.; Zavras, A.I.; Kyriopoulos, I.-I.; Kyriopoulos, J. Economic crisis, austerity and unmet healthcare needs: The case of Greece. BMC Health Serv. Res. 2016, 16, 309. [Google Scholar] [CrossRef]
- Tapia-Granados, J.A.; Rodriguez, J.M. Health, economic crisis, and austerity: A comparison of Greece, Finland and Iceland. Health Policy 2015, 119, 941–953. [Google Scholar] [CrossRef]
- Branas, C.C.; Kastanaki, A.E.; Michalodimitrakis, M.; Tzougas, J.; Kranioti, E.F.; Theodorakis, P.N.; Carr, B.G.; Wiebe, D.J. The impact of economic austerity and prosperity events on suicide in Greece: A 30-year interrupted time-series analysis. BMJ Open 2015, 5, e005619. [Google Scholar] [CrossRef] [PubMed]
- Antonakakis, N.; Collins, A. The impact of fiscal austerity on suicide: On the empirics of a modern Greek tragedy. Soc. Sci. Med. 2014, 112, 39–50. [Google Scholar] [CrossRef]
- Rachiotis, G.; Stuckler, D.; McKee, M.; Hadjichristodoulou, C. What has happened to suicides during the Greek economic crisis? Findings from an ecological study of suicides and their determinants (2003–2012). BMJ Open 2015, 5, e007295. [Google Scholar] [CrossRef]
- Laliotis, I.; Ioannidis, J.P.; Stavropoulou, C. Total and cause-specific mortality before and after the onset of the Greek economic crisis: An interrupted time-series analysis. Lancet Public Health 2016, 1, e56–e65. [Google Scholar] [CrossRef]
- Drydakis, N. The Relationship between Recessions and Health; IZA World Labor: Bonn, Germany, 2021; p. 283. [Google Scholar]
- Petrovici, I.; Ionica, M.; Neagoe, O.C. Economic Crisis: A Factor for the Delayed Diagnosis of Breast Cancer. Int. J. Environ. Res. Public Health 2021, 18, 3998. [Google Scholar] [CrossRef]
- Ennis, K.Y.; Chen, M.-H.; Smith, G.C.; D’Amico, A.V.; Zhang, Y.; Quinn, S.A.; Ryemon, S.N.; Goltz, D.; Harrison, L.B.; Ennis, R.D. The Impact of Economic Recession on the Incidence and Treatment of Cancer. J. Cancer 2015, 6, 727–733. [Google Scholar] [CrossRef] [Green Version]
- Maruthappu, M.; Watkins, J.; Noor, A.M.; Williams, C.; Ali, R.; Sullivan, R.; Zeltner, T.; Atun, R. Economic downturns, universal health coverage, and cancer mortality in high-income and middle-income countries, 1990–2010: A longitudinal analysis. Lancet 2016, 388, 684–695. [Google Scholar] [CrossRef]
- Saloustros, E.; Vichas, G.; Margiolaki, A.; Koumiotaki, S.; Androulakis, N.; Georgoulias, V. Lung cancer in the era of Greek economic crisis. Lung Cancer 2014, 86, 112–113. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R.; Kontos, E.Z.; Viswanath, K.; Haas, J.S.; Lathan, C.S.; MacConaill, L.E.; Chen, J.; Ayanian, J.Z. Integrating Multiple Social Statuses in Health Disparities Research: The Case of Lung Cancer. Health Serv. Res. 2012, 47, 1255–1277. [Google Scholar] [CrossRef] [PubMed]
- Boscoe, F.P.; Mph, C.J.J.; Sherman, R.L.; Ms, D.G.S.; Lin, G.; Henry, K.A. The relationship between area poverty rate and site-specific cancer incidence in the United States. Cancer 2014, 120, 2191–2198. [Google Scholar] [CrossRef] [PubMed]
- United Nations Development Programme. Human Development Report 2015: Sustaining Human Progress: Reducing Vulnerabilities and Building Resilience; Human Development Report Office: New York, NY, USA, 2015. [Google Scholar]
- Vlachonikolis, I.; Philalithis, A.; Brittan, Y.; Georgoulias, V. Mortality from malignant neoplasms in Crete, 1992–1993. J. Epidemiol. Community Health 1998, 52, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Tsiligianni, I.G. COPD patients trapped in the financial crisis in rural Crete. Lancet Respir. Med. 2013, 1, e31–e32. [Google Scholar] [CrossRef]
- Sifaki-Pistolla, D.; Lionis, C.; Georgoulias, V.; Kyriakidis, P.; Koinis, F.; Aggelaki, S.; Tzanakis, N. Lung cancer and tobacco smoking: Reflections from a population-based cancer registry. Tob. Induc. Dis. 2017, 15, 6. [Google Scholar] [CrossRef]
- Sifaki-Pistolla, D.; Lionis, C.; Koinis, F.; Georgoulias, V.; Tzanakis, N. Lung cancer and annual mean exposure to outdoor air pollution in Crete, Greece. Eur. J. Cancer Prev. 2017, 26, S208–S214. [Google Scholar] [CrossRef]
- Lazaridis, M.; Dzumbova, L.; Kopanakis, I.; Ondracek, J.; Glytsos, T.; Aleksandropoulou, V.; Voulgarakis, A.; Katsivela, E.; Mihalopoulos, N.; Eleftheriadis, K. PM10 and PM2.5 Levels in the Eastern Mediterranean (Akrotiri Research Station, Crete, Greece). Water Air Soil Pollut. 2008, 189, 85–101. [Google Scholar] [CrossRef]
- Bray, F.; Parkin, D.M. Evaluation of data quality in the cancer registry: Principles and methods. Part I: Comparability, validity and timeliness. Eur. J. Cancer 2009, 45, 747–755. [Google Scholar] [CrossRef]
- Alkire, S.; Conconi, A.; Roche, J.M. Multidimensional Poverty Index 2012: Brief Methodological Note and Results; Oxford University Department of International Development Working Paper: Oxford, UK, 2013. [Google Scholar]
- Ravallion, M. On multidimensional indices of poverty. J. Econ. Inequal. 2011, 9, 235–248. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Ganti, A.K.; Siedlik, E.; Marr, A.S.; Loberiza, F.R.; Kessinger, A. Predictive Ability of Charlson Comorbidity Index on Outcomes From Lung Cancer. Am. J. Clin. Oncol. 2011, 34, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.A.; Neoh, H.-M.; Rahim, S.S.S.A.; Azhar, Z.I.; Hassan, M.R.; Safian, N.; Jamal, R. Spatial Analysis of Colorectal Cancer Cases in Kuala Lumpur. Asian Pac. J. Cancer Prev. 2013, 15, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- McEntee, J.C.; Ogneva-Himmelberger, Y. Diesel particulate matter, lung cancer, and asthma incidences along major traffic corridors in MA, USA: A GIS analysis. Health Place 2008, 14, 817–828. [Google Scholar] [CrossRef]
- Khang, Y.H.; Lynch, J.W.; Kaplan, G.A. Impact of economic crisis on cause-specific mortality in South Korea. Int. J. Epid. 2005, 34, 1291–1301. [Google Scholar] [CrossRef]
- Blakely, T.; Tobias, M.; Atkinson, J. Inequalities in mortality during and after restructuring of the New Zealand economy: Repeated cohort studies. BMJ 2008, 336, 371–375. [Google Scholar] [CrossRef]
- Fawcett, J.; Blakely, T. Cancer is overtaking cardiovascular disease as the main driver of socioeconomic inequalities in mortality: New Zealand (1981–99). J. Epidemiol. Community Health 2007, 61, 59–66. [Google Scholar] [CrossRef]
- Regidor, E.; Mateo, A.; Barrio, G.; De La Fuente, L. Mortality in Spain in the Context of the Economic Crisis and Austerity Policies. Am. J. Public Health 2019, 109, 1043–1049. [Google Scholar] [CrossRef]
- Samet, J.M. Is there more to learn about the epidemiology of lung cancer? Eur. J. Epidemiol. 2016, 31, 1159–1160. [Google Scholar] [CrossRef]
- Bray, F.; Jemal, A.; Grey, N.; Ferlay, J.; Forman, D. Global cancer transitions according to the Human Development Index (2008–2030): A population-based study. Lancet Oncol. 2012, 13, 790–801. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Anttila, A.; von Karsa, L.; Alfonso-Sanchez, J.L.; Gorgojo, L. Cancer screening and health system resilience: Keys to protecting and bolstering preventive services during a financial crisis. Eur. J. Cancer 2012, 48, 2212–2218. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, J.; Malvezzi, M.; Negri, E.; La Vecchia, C.; Boffetta, P. Risk factors for lung cancer worldwide. Eur. Respir. J. 2016, 48, 889–902. [Google Scholar] [CrossRef]
- Ancona, C.; Badaloni, C.; Mataloni, F.; Bolignano, A.; Bucci, S.; Cesaroni, G.; Sozzi, R.; Davoli, M.; Forastiere, F. Mortality and morbidity in a population exposed to multiple sources of air pollution: A retrospective cohort study using air dispersion models. Environ. Res. 2015, 137, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Tammemagi, C.M.; Neslund-Dudas, C.; Simoff, M.; Kvale, P. Smoking and lung cancer survival: The role of comorbidity and treatment. CHEST J. 2004, 125, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Morelli, X.; Rieux, C.; Cyrys, J.; Forsberg, B.; Slama, R. Air pollution, health and social deprivation: A fine-scale risk assessment. Environ. Res. 2016, 147, 59–70. [Google Scholar] [CrossRef]
- Aldrich, M.C.; Munro, H.M.; Mumma, M.; Grogan, E.L.; Massion, P.P.; Blackwell, T.S.; Blot, W.J. Chronic Obstructive Pulmonary Disease and Subsequent Overall and Lung Cancer Mortality in Low-Income Adults. PLoS ONE 2015, 10, e0121805. [Google Scholar] [CrossRef]
- Ifanti, A.A.; Argyriou, A.A.; Kalofonou, F.H.; Kalofonos, H.P. Financial crisis and austerity measures in Greece: Their impact on health promotion policies and public health care. Health Policy 2013, 113, 8–12. [Google Scholar] [CrossRef]
- Simou, E.; Koutsogeorgou, E. Effects of the economic crisis on health and healthcare in Greece in the literature from 2009 to 2013: A systematic review. Health Policy 2014, 115, 111–119. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | Lung Cancer Cases | Variation Rate from 1992 to 2013 | p Value | |
|---|---|---|---|---|
| Period A (1992–2008) | Period B (2009–2013) | |||
| ASIR/100,000/year | 37.9 | 47.8 | +9.8 | 0.01 |
| ASMR/100,000/year | 30.5 | 43.8 | +13.3 | <0.001 |
| 5 year Net-Survival (%) | 14.6 | 12.1 | −2.5 | 0.04 |
| Gender (%) | 0.01 | |||
| Males | 91.8 | 82.4 | −9.3 | |
| Females | 8.2 | 17.6 | +9.4 | |
| Age at year of diagnosis (Median) | 68 | 77 | +9 | <0.001 |
| Stage at year of diagnosis (%) | <0.001 | |||
| I | 17.1 | 6.1 | −11 | |
| II | 12.2 | 8.2 | −7.9 | |
| III | 13 | 17.2 | +8.2 | |
| IV | 39.7 | 44.8 | +10.2 | |
| Not known | 18 | 18.1 | +0.2 | |
| Adjusted Charlson Comorbidity Index-CCI% (Median) | 3 | 4 | +1 | 0.04 |
| Family medical history of LC or other lung disease | 0.62 | |||
| No | 15.1 | 15.0 | −0.1 | |
| Yes | 67.6 | 67.5 | −0.1 | |
| Not known | 17.3 | 17.5 | +0.2 | |
| Smoking status (%) | 0.02 | |||
| Never smoker | 19.9 | 12.8 | −7.1 | |
| Ever smoker | 71.8 | 79.2 | +7.4 | |
| Not known | 8.3 | 8 | −0.3 | |
| Alcohol consumption (%) | 0.02 | |||
| No | 29.9 | 21.1 | −8.8 | |
| Yes | 32 | 41.4 | +9.4 | |
| Not known | 38.1 | 37.5 | −0.6 | |
| Exposure to OAP (% of LC patients potentially exposed) | 25.1 | 34.9 | +9.8 | <0.001 |
| Deprivation Index (Median) | 17.5 | 29.2 | +11.7 | <0.001 |
| Covariates | Period A (1992–2008) | Period B (2009–2013) | ||
|---|---|---|---|---|
| Relative Risk * of LC Death (95%CI) | p Value | Relative Risk * of LC Death (95%CI) | p Value | |
| Adjusted Charlson’s Comorbidity Index-CCI% | 4.1 (3.8–4.4) | 0.02 | 4.9 (4.4–5.5) | 0.04 |
| Family medical history of LC or other lung disease | 4.0 (3.5–4.6) | 0.03 | 4.0 (3.3–4.8) | 0.04 |
| Ever smokers | 4.8 (4.6–5.1) | 0.01 | 5.7 (5.2–6.3) | 0.03 |
| Alcohol consumers | 1.8 (1.2–2.4) | 0.02 | 2.1 (1.3–3.0) | 0.04 |
| Exposure to OAP | 1.9 (1.6–2.1) | 0.02 | 2.3 (1.9–2.8) | 0.03 |
| Deprivation Index | 1.5 (1.1–2.0) | 0.03 | 5.4 (5.1–5.8) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sifaki-Pistolla, D.; Chatzea, V.E.; Mechili, E.A.; Koinis, F.; Georgoulias, V.; Lionis, C.; Tzanakis, N. Spatio-Temporal Variation of Lung Cancer in Crete, 1992–2013. Economic or Health Crisis? Int. J. Environ. Res. Public Health 2022, 19, 12161. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912161
Sifaki-Pistolla D, Chatzea VE, Mechili EA, Koinis F, Georgoulias V, Lionis C, Tzanakis N. Spatio-Temporal Variation of Lung Cancer in Crete, 1992–2013. Economic or Health Crisis? International Journal of Environmental Research and Public Health. 2022; 19(19):12161. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912161
Chicago/Turabian StyleSifaki-Pistolla, Dimitra, Vasiliki Eirini Chatzea, Enkeleint A. Mechili, Filippos Koinis, Vassilis Georgoulias, Christos Lionis, and Nikos Tzanakis. 2022. "Spatio-Temporal Variation of Lung Cancer in Crete, 1992–2013. Economic or Health Crisis?" International Journal of Environmental Research and Public Health 19, no. 19: 12161. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912161