
Monitoring of Thermal Comfort and Air Quality for Sustainable Energy Management inside Hospitals Based on Online Analytical Processing and the Internet of Things

 , ,
, ,  , , , and
, , , and
Abstract
:1. Introduction
Thermal Comfort and Air Quality in Hospitals
2. Chilean Public Hospital System
2.1. Classification of Public Hospitals
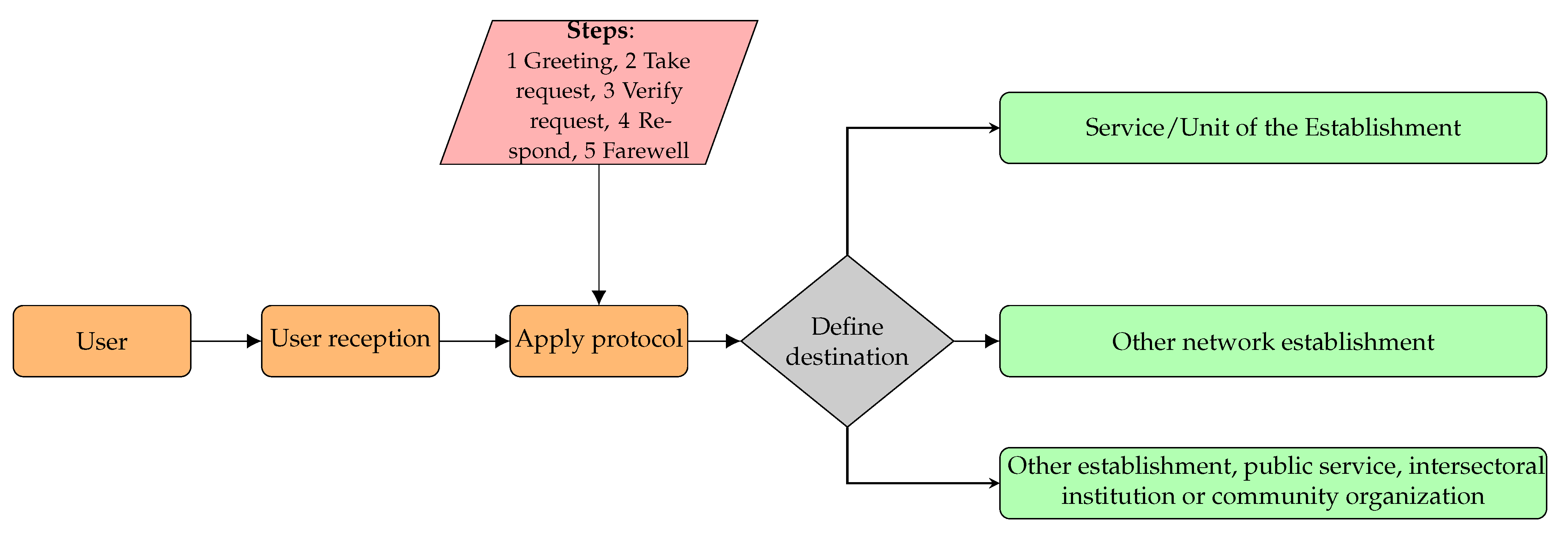
2.2. Care Protocol of a Chilean Public Hospital of High Complexity
2.3. Characterization of the Energy Matrix in a Highly Complex Hospital
2.4. Motivation
3. Materials and Methods
- Design a cyber–physical conceptual model that can be implemented in the hospital and that allows efficient decision-making.
- Create conceptual and logical models of multidimensional databases that will allow the subsequent implementation of computer systems.
4. Hospital Cyber–Physical System
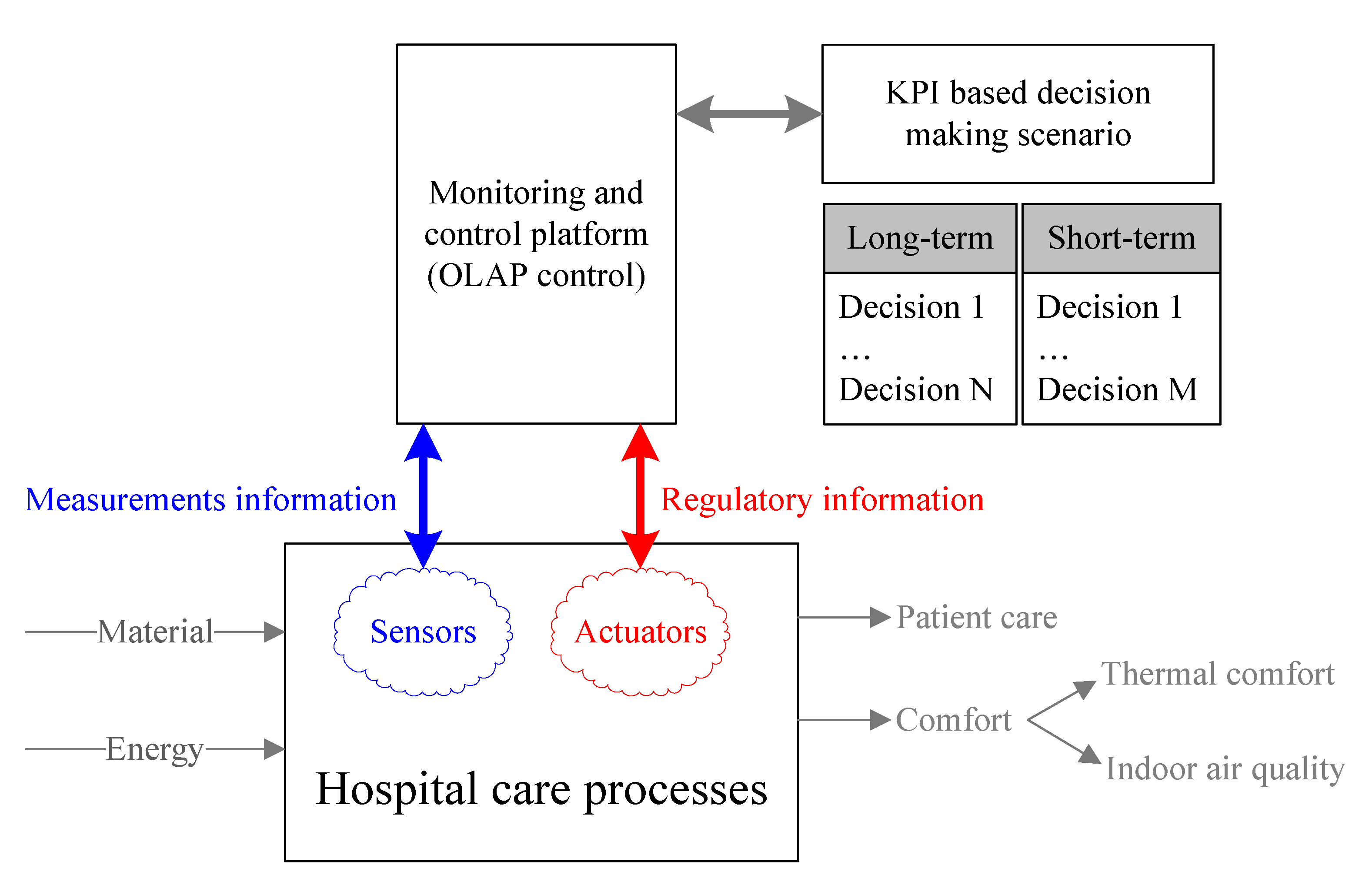
4.1. IoT Platform as a Cyber–Physical System
4.2. Design of the Cyber–Physical System
5. Monitoring System for Thermal Comfort and IAQ in a Hospital
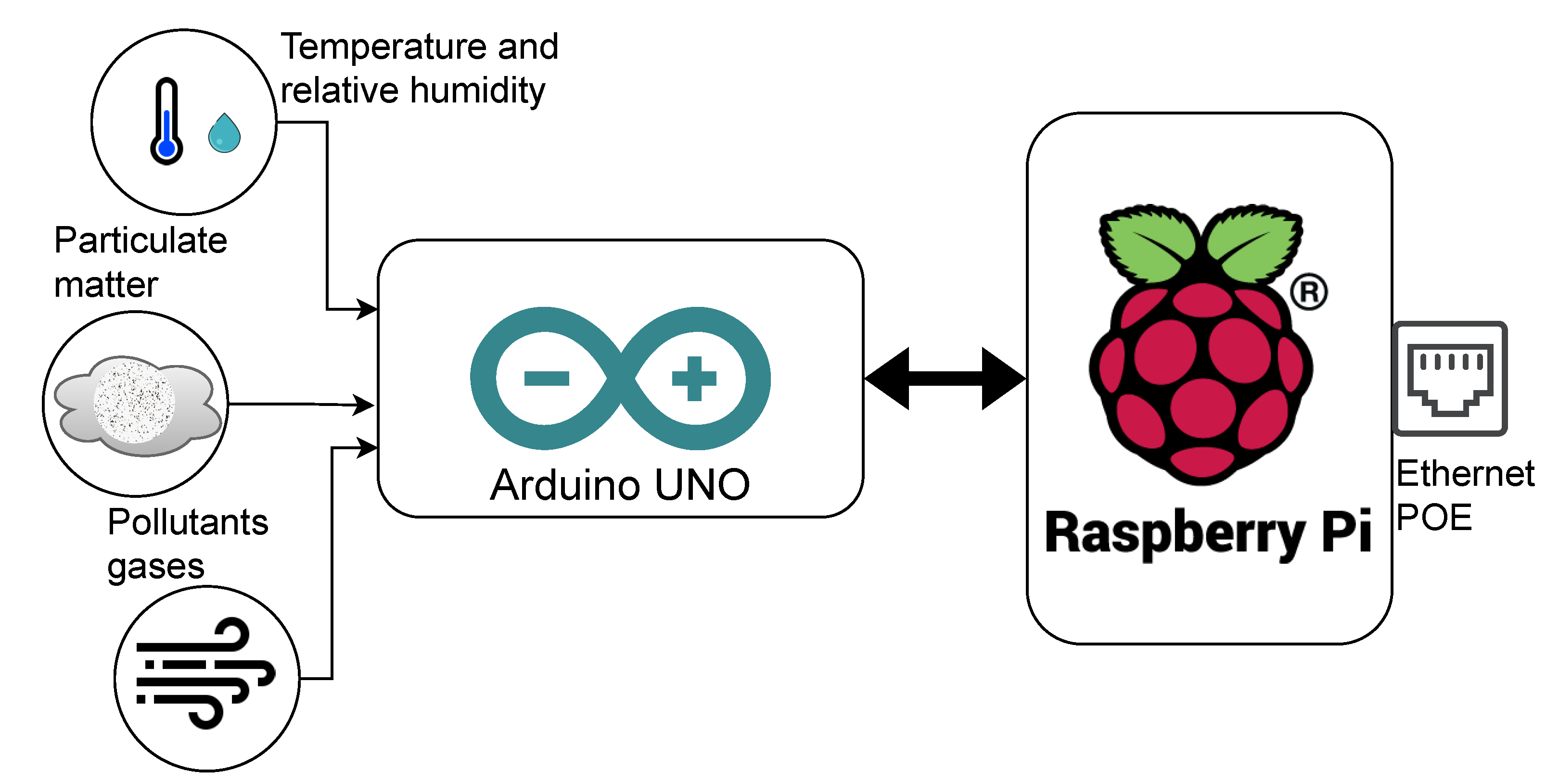
5.1. Main IoT Platform Components
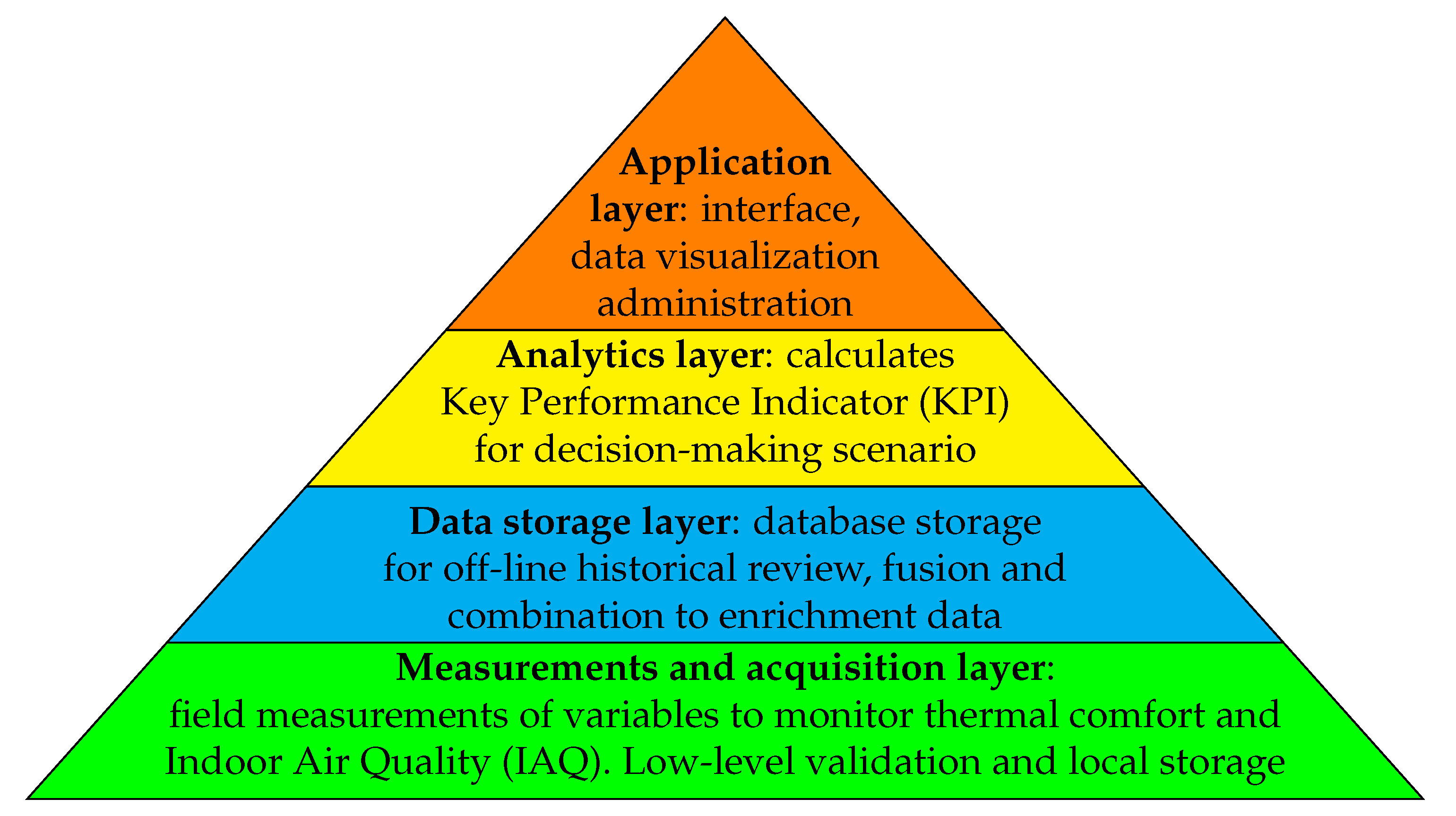
5.2. Data Processing and Indicator Management Sub-System
- Physical location: Refers to buildings within well-defined limits, which are made up of multiple and different types of dependencies, which are intended to provide public use services for different types of people.
- Spaces: They are specific dependencies belonging to and contained within an enclosure, which are used by certain types of people (users). Usually, each space has one or more specific functions designed to satisfy all or part of the needs of the direct or indirect users of the site.
- Activities: These are specific functions that are within the work or service, which are developed by people or machiNES under the supervision of specialized personnel and have the purpose of providing direct or indirect service for the benefit of users to whom the venue is dedicated.
- Temporality: Provides temporal anchoring information that allows all the information contained in the system to be accurately located in time, to reflect different states of the reality of the premises, depending on the different needs for analysis time required by the different monitoring and follow-up procedures.
5.3. Multidimensional Sub-System
- Additive (or fractional) indicators: These are those in which the computation formula complies with the additivity property [83] or if it is possible to break it down into simpler expressions that do. This allows them to be obtained directly through a single OLAP operation from a multidimensional cube with aggregated information.
- Non-additive indicators: These are those indicators whose formula does not admit a decomposition into additive components. From this group, we will be particularly interested in those indicators whose computation is possible in two stages, where the first stage (much more demanding in terms of volume of data and number of computations) can be calculated from summaries contained in the database and, in the second stage, the partial results can be used to obtain the final value of the indicator.
6. Discussion of Results
6.1. Feasibility of Technological Infrastructure
6.2. Installation of the Environmental Data Collection Platform
6.3. Computer Platform for Monitoring Environmental Indicators
6.4. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CHOH | Ethanol |
| CO | Carbon Monoxide |
| CO | Carbon Dioxide |
| CPS | Cyber–Physical System |
| ETL | Extract, Transform and Load |
| GDP | Gross Domestic Production |
| GHG | Greenhouse Gas |
| HVAC | Heating, Ventilation, and Air Conditioning |
| IAQ | Indoor Air Quality |
| ICS | Information and Communications Systems |
| IoT | Internet of Things |
| IP | Internet Protocol |
| KPI | Key Performance Indicator |
| MAF | Multiple Aggregation Function |
| NES | National Electricity System |
| NO | Nitrogen Dioxide |
| NOx | Nitrogen Oxides |
| OECD | Organisation for Economic Co-operation and Development |
| OLAP | On-Line Analytical Processing |
| OPC UA | Open Platform Communications Unified Architecture |
| PM | Particulate Matter 10 micrometers or less in diameter |
| PM | Particulate Matter 2.5 micrometers or less in diameter |
| PMV | Predicted Mean Vote |
| PoE | Power over Ethernet |
| PPD | Percentage of People Dissatisfied |
| RH | Relative Humidity |
| ROLAP | Relational Online Analytical Processing |
| SBC | Sustainable Building Certification |
| SDGs | Sustainable Development Goals |
| SO | Sulfur Dioxide |
| UI | User Interface |
| VOC | Volatile Organic Compound |
References
- United Nations. #17goals17days: Progress Made on Global Goals. 2016. Available online: https://www.un.org/sustainabledevelopment/blog/2016/07/17goals17days-progress-made-on-sustainable-development-goals/ (accessed on 17 June 2022).
- Siksnelyte-Butkiene, I.; Streimikiene, D.; Lekavicius, V.; Balezentis, T. Energy poverty indicators: A systematic literature review and comprehensive analysis of integrity. Sustain. Cities Soc. 2021, 67, 102756. [Google Scholar] [CrossRef]
- Nguyen, C.P.; Su, T.D. The influences of government spending on energy poverty: Evidence from developing countries. Energy 2022, 238, 121785. [Google Scholar] [CrossRef]
- Knox, S.; Hannon, M.; Stewart, F.; Ford, R. The (in)justices of smart local energy systems: A systematic review, integrated framework, and future research agenda. Energy Res. Soc. Sci. 2022, 83, 102333. [Google Scholar] [CrossRef]
- Le, T.H.; Nguyen, C.P.; Park, D. Financing renewable energy development: Insights from 55 countries. Energy Res. Soc. Sci. 2020, 68, 101537. [Google Scholar] [CrossRef]
- Novikova, A.; Csoknyai, T.; Szalay, Z. Low carbon scenarios for higher thermal comfort in the residential building sector of South Eastern Europe. Energy Effic. 2018, 11, 845–875. [Google Scholar] [CrossRef]
- Ma, Y.; Tao, Y.; Shi, L.; Liu, Q.G.; Wang, Y.; Tu, J.Y. Investigations on the thermal performance of a novel thermal energy storage unit for poor solar conditions. Renew. Energy 2021, 180, 166–177. [Google Scholar] [CrossRef]
- Cao, X.; Dai, X.; Liu, J. Building energy-consumption status worldwide and the state-of-the-art technologies for zero-energy buildings during the past decade. Energy Build. 2016, 128, 198–213. [Google Scholar] [CrossRef]
- Banerjee, R.; Mishra, V.; Maruta, A.A. Energy poverty, health and education outcomes: Evidence from the developing world. Energy Econ. 2021, 101, 105447. [Google Scholar] [CrossRef]
- Chen, C.; Pinar, M.; Stengos, T. Renewable energy consumption and economic growth nexus: Evidence from a threshold model. Energy Policy 2020, 139, 111295. [Google Scholar] [CrossRef]
- Murshed, M. Are Trade Liberalization policies aligned with Renewable Energy Transition in low and middle income countries? An Instrumental Variable approach. Renew. Energy 2020, 151, 1110–1123. [Google Scholar] [CrossRef]
- Salari, M.; Javid, R.J.; Noghanibehambari, H. The nexus between CO2 emissions, energy consumption, and economic growth in the U.S. Econ. Anal. Policy 2021, 69, 182–194. [Google Scholar] [CrossRef]
- Ritchie, H.; Roser, M. CO2 and Greenhouse Gas Emissions—Our World in Data. 2020. Available online: https://ourworldindata.org/co2-and-other-greenhouse-gas-emissions (accessed on 19 June 2022).
- Kim, S.H.; Moon, H.J. Case study of an advanced integrated comfort control algorithm with cooling, ventilation, and humidification systems based on occupancy status. Build. Environ. 2018, 133, 246–264. [Google Scholar] [CrossRef]
- Kapwata, T.; Language, B.; Piketh, S.; Wright, C.Y. Variation of Indoor Particulate Matter Concentrations and Association with Indoor/Outdoor Temperature: A Case Study in Rural Limpopo, South Africa. Atmosphere 2018, 9, 124. [Google Scholar] [CrossRef]
- Salata, F.; Golasi, I.; Verrusio, W.; de Lieto Vollaro, E.; Cacciafesta, M.; de Lieto Vollaro, A. On the necessities to analyse the thermohygrometric perception in aged people. A review about indoor thermal comfort, health and energetic aspects and a perspective for future studies. Sustain. Cities Soc. 2018, 41, 469–480. [Google Scholar] [CrossRef]
- Kallio, J.; Vildjiounaite, E.; Koivusaari, J.; Räsänen, P.; Similä, H.; Kyllönen, V.; Muuraiskangas, S.; Ronkainen, J.; Rehu, J.; Vehmas, K. Assessment of perceived indoor environmental quality, stress and productivity based on environmental sensor data and personality categorization. Build. Environ. 2020, 175, 106787. [Google Scholar] [CrossRef]
- Zuhaib, S.; Manton, R.; Griffin, C.; Hajdukiewicz, M.; Keane, M.M.; Goggins, J. An Indoor Environmental Quality (IEQ) assessment of a partially-retrofitted university building. Build. Environ. 2018, 139, 69–85. [Google Scholar] [CrossRef]
- Zeng, C.; Liu, S.; Shukla, A.; Yang, B. Identifying the occupant’s satisfaction and awareness for the performance of Eco houses in the United Kingdom. J. Build. Eng. 2018, 18, 281–291. [Google Scholar] [CrossRef]
- Ortiz, M.A.; Kurvers, S.R.; Bluyssen, P.M. A review of comfort, health, and energy use: Understanding daily energy use and wellbeing for the development of a new approach to study comfort. Energy Build. 2017, 152, 323–335. [Google Scholar] [CrossRef]
- Alanne, K.; Sierla, S. An overview of machine learning applications for smart buildings. Sustain. Cities Soc. 2022, 76, 103445. [Google Scholar] [CrossRef]
- Zhai, Z.J.; Metzger, I.D. Insights on critical parameters and conditions for personalized ventilation. Sustain. Cities Soc. 2019, 48, 101584. [Google Scholar] [CrossRef]
- Hashempour, N.; Taherkhani, R.; Mahdikhani, M. Energy performance optimization of existing buildings: A literature review. Sustain. Cities Soc. 2020, 54, 101967. [Google Scholar] [CrossRef]
- Lamnabhi-Lagarrigue, F.; Annaswamy, A.; Engell, S.; Isaksson, A.; Khargonekar, P.; Murray, R.M.; Nijmeijer, H.; Samad, T.; Tilbury, D.; Van den Hof, P. Systems & Control for the future of humanity, research agenda: Current and future roles, impact and grand challenges. Annu. Rev. Control 2017, 43, 1–64. [Google Scholar] [CrossRef]
- Becerra, M.; Jerez, A.; Valenzuela, M.; Garcés, H.O.; Demarco, R. Life quality disparity: Analysis of indoor comfort gaps for Chilean households. Energy Policy 2018, 121, 190–201. [Google Scholar] [CrossRef]
- Comité Técnico AEN/CTN 81 Prevención y Medios de Protección Personal y Colectiva en el Trabajo. Ergonomía del Ambiente Térmico: Determinación Analítica e Interpretación del Bienestar Térmico Mediante el Cálculo de los Índices PMV y PPD y los Criterios de Bienestar Térmico Local; AENOR: Madrid, Spain, 2006; p. 58. [Google Scholar]
- ASHRAE Standard; American National Standards Institute. ASHRAE 55-2013: Standard 55-2013—Thermal Environmental Conditions for Human Occupancy; ANSI/ASHRAE Standard: Atlanta, GA, USA, 2013; Volume 55-2013, p. 54. [Google Scholar]
- Xie, D.; Yu, L.; Jiang, T.; Zou, Y. Distributed Energy Optimization for HVAC Systems in University Campus Buildings. IEEE Access 2018, 6, 59141–59151. [Google Scholar] [CrossRef]
- Mantovani, G.; Ferrarini, L. Temperature Control of a Commercial Building with Model Predictive Control Techniques. IEEE Trans. Ind. Electron. 2015, 62, 2651–2660. [Google Scholar] [CrossRef]
- Yang, Y.; Hu, G.; Spanos, C.J. HVAC Energy Cost Optimization for a Multizone Building via a Decentralized Approach. IEEE Trans. Autom. Sci. Eng. 2020, 17, 1950–1960. [Google Scholar] [CrossRef]
- Fanger, P.O. Thermal Comfort: Analysis and Applications in Environmental Engineering; Danish Kr. 76, 50; Danish Technical Press: Copenhagen, Denmark, 1970; 244p. [Google Scholar] [CrossRef]
- Pereira, P.F.; Broday, E.E.; Xavier, A.A. Thermal Comfort Applied in Hospital Environments: A Literature Review. Appl. Sci. 2020, 10, 7030. [Google Scholar] [CrossRef]
- Yuan, F.; Yao, R.; Sadrizadeh, S.; Li, B.; Cao, G.; Zhang, S.; Zhou, S.; Liu, H.; Bogdan, A.; Croitoru, C.; et al. Thermal comfort in hospital buildings—A literature review. J. Build. Eng. 2022, 45, 103463. [Google Scholar] [CrossRef]
- ASHRAE. 2019 ASHRAE Handbook—HVAC Applications (SI); ASHRAE: Atlanta, GA, USA, 2019; p. 1408. [Google Scholar]
- Guyot, G.; Sherman, M.H.; Walker, I.S. Smart ventilation energy and indoor air quality performance in residential buildings: A review. Energy Build. 2018, 165, 416–430. [Google Scholar] [CrossRef] [Green Version]
- European Standards. UNE EN 16798-3:2018 Energy Performance of Buildings—Ventilation for Buildings—Part 3: For Non-Residential Buildings—Performance Requirements for Ventilation and Room-Conditioning Systems (Modules M5-1, M5-4); Technical Report; Asociación Española de Normalización: Madrid, Spain, 2018. [Google Scholar]
- Eijkelenboom, A.; Kim, D.H.; Bluyssen, P.M. First results of self-reported health and comfort of staff in outpatient areas of hospitals in the Netherlands. Build. Environ. 2020, 177, 106871. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, Z.; Zhang, Z.; Hong, J.; Lin, B. Investigation on the Indoor Environment Quality of health care facilities in China. Build. Environ. 2018, 141, 273–287. [Google Scholar] [CrossRef]
- Saini, J.; Dutta, M.; Marques, G. Indoor Air Quality Monitoring Systems Based on Internet of Things: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4942. [Google Scholar] [CrossRef] [PubMed]
- Cociorva, S.; Iftene, A. Indoor Air Quality Evaluation in Intelligent Building. Energy Procedia 2017, 112, 261–268. [Google Scholar] [CrossRef]
- Prieto-Parra, L.; Yohannessen, K.; Brea, C.; Vidal, D.; Ubilla, C.A.; Ruiz-Rudolph, P. Air pollution, PM2.5 composition, source factors, and respiratory symptoms in asthmatic and nonasthmatic children in Santiago, Chile. Environ. Int. 2017, 101, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Rudolph, P.; Arias, N.; Pardo, S.; Meyer, M.; Mesías, S.; Galleguillos, C.; Schiattino, I.; Gutiérrez, L. Impact of large industrial emission sources on mortality and morbidity in Chile: A small-areas study. Environ. Int. 2016, 92–93, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Cayir Ervural, B.; Evren, R.; Delen, D. A multi-objective decision-making approach for sustainable energy investment planning. Renew. Energy 2018, 126, 387–402. [Google Scholar] [CrossRef]
- Carvalhais, C.; Santos, J.; Vieira da Silva, M. Analytical and subjective interpretation of thermal comfort in hospitals: A case study in two sterilization services. J. Toxicol. Environ. Health Part A 2016, 79, 299–306. [Google Scholar] [CrossRef]
- Fabbri, K.; Gaspari, J.; Vandi, L. Indoor Thermal Comfort of Pregnant Women in Hospital: A Case Study Evidence. Sustainability 2019, 11, 6664. [Google Scholar] [CrossRef]
- Zhang, W.; Hu, W.; Wen, Y. Thermal Comfort Modeling for Smart Buildings: A Fine-Grained Deep Learning Approach. IEEE Internet Things J. 2019, 6, 2540–2549. [Google Scholar] [CrossRef]
- Yang, Y.; Srinivasan, S.; Hu, G.; Spanos, C.J. Distributed Control of Multizone HVAC Systems Considering Indoor Air Quality. IEEE Trans. Control Syst. Technol. 2021, 29, 2586–2597. [Google Scholar] [CrossRef]
- Urbina Henríquez, I.; Sugg Herrera, D. Análisis de la Eficiencia: De los Hospitales púBlicos de Alta Complejidad en Chile Entre 2014 y 2018. In Estudios de Finanzas Públicas; Dirección de Presupuestos del Ministerio de Hacienda: Santiago, Chile, 2021; Volume 21, p. 39. [Google Scholar]
- Alvial, X.; Rojas, A.; Carrasco, R.; Duran, C.; Fernandez-Campusano, C. Overuse of Health Care in the Emergency Services in Chile. Int. J. Environ. Res. Public Health 2021, 18, 3082. [Google Scholar] [CrossRef]
- Coss-Mandiola, J.; Vanegas-López, J.; Rojas, A.; Carrasco, R.; Dubo, P.; Campillay-Campillay, M. Characterization of Communes with Quality Accredited Primary Healthcare Centers in Chile. Int. J. Environ. Res. Public Health 2022, 19, 9189. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud. Decreto 140: Reglamento Orgánico de los Servicios de Salud; Ministerio de Salud: Santiago, Chile, 2005. [Google Scholar]
- Departamento de Estadísticas e Información de Salud. Datos Abiertos: Establecimientos de Salud: 2021: Listado de Establecimientos de Salud; Ministerio de Salud, Gobierno de Chile: Santiago, Chile, 2022. [Google Scholar]
- Grimaz, S.; Ruzzene, E.; Zorzini, F. Situational assessment of hospital facilities for modernization purposes and resilience improvement. Int. J. Disaster Risk Reduct. 2021, 66, 102594. [Google Scholar] [CrossRef]
- Simsek, Y.; Lorca, Á.; Urmee, T.; Bahri, P.A.; Escobar, R. Review and assessment of energy policy developments in Chile. Energy Policy 2019, 127, 87–101. [Google Scholar] [CrossRef]
- Agencia de Sostenibilidad Energética. Programa de Eficiencia Energética en Edificios Públicos—Agencia de Sostenibilidad Energética, 2022.
- Servicio de Salud Metropolitano Sur Oriente. Atención Centrada en el Usuario. 2021. Available online: https://redsalud.ssmso.cl/atencion-centrada-en-el-usuario/ (accessed on 22 January 2022).
- Ministerio de Salud de Chile; Subsecretaría de Salud Pública. Ley 20.584: Regula los Derechos y Deberes que Tienen las Personas en Relación con Acciones Vinculadas a su Atención en Salud; Ministerio de Salud: Santiago, Chile, 2012. [Google Scholar]
- Ministerio de Salud; Subsecretaría de Salud Pública. DFL 1: Fija texto refundido, coordinado y sistematizado del Decreto Ley N° 2763, de 1979 y de las leyes N° 18933 y N° 18469. Bibl. Congr. Nac. Chile / BCN 2006, 1, 1–197. [Google Scholar]
- NuNES d’Albuquerque, M.A.; Moreira da Silva, R.; Barreto Gomes, M.D.L. Eficiência energética em uma edificação pública: Uma análise das possibilidades. Electron. J. Manag. Syst. 2017, 12, 462–470. [Google Scholar] [CrossRef]
- Prada, M.; Prada, I.F.; Cristea, M.; Popescu, D.E.; Bungău, C.; Aleya, L.; Bungău, C.C. New solutions to reduce greenhouse gas emissions through energy efficiency of buildings of special importance—Hospitals. Sci. Total Environ. 2020, 718, 137446. [Google Scholar] [CrossRef]
- Ministerio del Medio Ambiente. Planes de Prevención y/o Descontaminación Atmosférica. 2022. Available online: https://ppda.mma.gob.cl/ (accessed on 20 April 2022).
- Coordinador Eléctrico Nacional. Sistema Eléctrico Nacional. 2022. Available online: https://www.coordinador.cl/sistemaelectrico/ (accessed on 20 April 2022).
- Agencia Chilena de Eficiencia Energética (AChEE). Manual de Gestor en Eficiencia Energética, Sector Hospitalario; Ministerio de Energía: Santiago, Chile, 2013; p. 84. [Google Scholar]
- División de Planificación y Desarrollo Regional del Gobierno Regional del Biobío. Estrategia Regional de Desarrollo 2015–2030: Región del Biobío; Technical Report; Consejo de Gobierno Regional (CORE): Concepción, Chile, 2015. [Google Scholar]
- Ministerio de Energía. Publicación Resultados Gestiona Energía 2021 Sector Público. 2022. Available online: https://sectorpublico.gestionaenergia.cl/ (accessed on 20 April 2022).
- Instituto de la Construcción. CES Hospitales: Evaluación y Califi Cación: Sistema Nacional de Certificación de Calidad Ambiental y Eficiencia Energética para Edificios de Uso Público; Certificación Edificio Sustentable, Instituto de la Construcción: Santiago, Chile, 2017; Volume 12BPC2-134, p. 168. [Google Scholar]
- European Committee for Standardization. EN 16798-3 Energy Performance of Buildings—Ventilation for Buildings—Part 3: For Non-Residential Buildings—Performance Requirements for Ventilation and Room-Conditioning Systems (Modules M5–1, M5–4); European Committee for Standardization: Brussels, Belgium, 2017; p. 58. [Google Scholar]
- Garcés, H.O.; Morales, E.; Gómez, R.; Cabrera, H.; Espinosa, E. Design and Calibration of Low Cost Sensor Node for Thermal Comfort Estimation. In Proceedings of the 2021 29th Mediterranean Conference on Control and Automation (MED), Puglia, Italy, 22–25 June 2021; IEEE: Puglia, Italy, 2021; pp. 1215–1221. [Google Scholar] [CrossRef]
- Filali-Yachou, S.; González-González, C.S.; Lecuona-Rebollo, C. HMI/ SCADA standards in the design of data center interfaces: A network operations center case study. DYNA 2015, 82, 180–186. [Google Scholar] [CrossRef]
- Aristodemou, L.; Tietze, F.; O’Leary, E.; Shaw, M. A Literature Review on Technology Development Process (TDP) Models. Cent. Technol. Manag. Work. Pap. Ser. 2019, 6, 1–30. [Google Scholar] [CrossRef]
- Graube, M.; Hensel, S.; Iatrou, C.; Urbas, L. Information models in OPC UA and their advantages and disadvantages. In Proceedings of the 2017 22nd IEEE International Conference on Emerging Technologies and Factory Automation (ETFA), Limassol, Cyprus, 12–15 September 2017; IEEE: Limassol, Cyprus, 2017; pp. 1–8. [Google Scholar] [CrossRef]
- Zhang, G.; Navimipour, N.J. A comprehensive and systematic review of the IoT-based medical management systems: Applications, techniques, trends and open issues. Sustain. Cities Soc. 2022, 82, 103914. [Google Scholar] [CrossRef]
- Asaad, S.M.; Maghdid, H.S. A Comprehensive Review of Indoor/Outdoor Localization Solutions in IoT era: Research Challenges and Future Perspectives. Comput. Netw. 2022, 212, 109041. [Google Scholar] [CrossRef]
- Akbarzadeh, O.; Baradaran, M.; Khosravi, M.R. IoT-Based Smart Management of Healthcare Services in Hospital Buildings during COVID-19 and Future Pandemics. Wirel. Commun. Mob. Comput. 2021, 2021, 5533161. [Google Scholar] [CrossRef]
- Javdani, H.; Kashanian, H. Internet of things in medical applications with a service-oriented and security approach: A survey. Health Technol. 2018, 8, 39–50. [Google Scholar] [CrossRef]
- Khajenasiri, I.; Estebsari, A.; Verhelst, M.; Gielen, G. A Review on Internet of Things Solutions for Intelligent Energy Control in Buildings for Smart City Applications. Energy Procedia 2017, 111, 770–779. [Google Scholar] [CrossRef]
- Jayaratne, M.; Nallaperuma, D.; De Silva, D.; Alahakoon, D.; Devitt, B.; Webster, K.E.; Chilamkurti, N. A data integration platform for patient-centered e-healthcare and clinical decision support. Futur. Gener. Comput. Syst. 2019, 92, 996–1008. [Google Scholar] [CrossRef]
- Chen, T.; Keravnou-Papailiou, E.; Antoniou, G. Medical analytics for healthcare intelligence—Recent advances and future directions. Artif. Intell. Med. 2021, 112, 102009. [Google Scholar] [CrossRef]
- Palladino, D.; Nardi, I.; Buratti, C. Artificial Neural Network for the Thermal Comfort Index Prediction: Development of a New Simplified Algorithm. Energies 2020, 13, 4500. [Google Scholar] [CrossRef]
- Enescu, D. A review of thermal comfort models and indicators for indoor environments. Renew. Sustain. Energy Rev. 2017, 79, 1353–1379. [Google Scholar] [CrossRef]
- Palominos, F.E.; Durán, C.A.; Córdova, F.M. Improve efficiency in multidimensional database queries through the use of additives aggregation functions. Procedia Comput. Sci. 2019, 162, 754–761. [Google Scholar] [CrossRef]
- Kaplan, R.; Norton, D. The balanced scorecard: Measures that drive performance. Harv. Bus. Rev. 1992, 70, 71–79. [Google Scholar]
- Palominos, F.E.; Córdova, F.; Durán, C.; Nuñez, B. A Simpler and Semantic Multidimensional Database Query Language to Facilitate Access to Information in Decision-making. Int. J. Comput. Commun. Control 2020, 15, 1–10. [Google Scholar] [CrossRef]
- ISO/TC 159/SC 5 Ergonomics of the Physical Environment. Ed. ISO-ISO 8996:2021—Ergonomics of the Thermal Environment—Determination of Metabolic Rate, 3rd ed.; International Organization for Standardization: Geneva, Switzerland, 2021; p. 28. [Google Scholar]
- ASHRAE Standard; American National Standards Institute. ASHRAE Standard 62.1-2013 Ventilation for Acceptable Indoor Air Quality; ANSI/ASHRAE Standard: Atlanta, GA, USA, 2013; Volume 62.1-2013, p. 54. [Google Scholar]
- ASHRAE Standard; American Society for Healthcare Engineering; American National Standards Institute. ASHRAE Standard 170-2017—Ventilation of Health Care Facilities; ANSI/ASHRAE/ASHE Standard: Atlanta, GA, USA, 2017; Volume 8400, p. 42. [Google Scholar]
- Golfarelli, M.; Rizzi, S. Data Warehouse Design: Modern Principles and Methodologies; McGraw-Hill: New York, NY, USA, 2009; p. 458. [Google Scholar]
- Dirección de Presupuesto. Informe de Ejecución Mensual Periodo 2021: 160205: Financiamiento Hospitales por Grupo Relacionado de Diagnóstico; Technical Report; Ministerio de Hacienda: Santiago, Chile, 2021. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Node | Location | Floor | Category | Location Description |
|---|---|---|---|---|
| 1 | Data center | 3 | other | Data center |
| 2 | Ambulatory care center waiting room | 4 | waiting room | Neurology waiting room |
| 3 | Ambulatory care center waiting room | 4 | waiting room | Otolaryngology-bronchopulmonary waiting room |
| 4 | Ambulatory care center waiting room | 4 | waiting room | Ophthalmology waiting room |
| 5 | Ambulatory care center waiting room | 2 | waiting room | Cardiology waiting room |
| 6 | Ambulatory care center waiting room | 2 | waiting room | Cardiology waiting room |
| 7 | Auditorium—ambulatory care center | 1 | auditorium | Auditorium—ambulatory care center |
| 8 | Meeting room—ambulatory care center | 6 | other | Meeting room—ambulatory care center |
| 9 | Adult emergency waiting room—critical patient tower | 1 | waiting room | Adult medicine emergency-nursing station |
| 10 | Adult emergency waiting room—critical patient tower | 1 | waiting room | ER corridor |
| 11 | Adult emergency waiting room—critical patient tower | 1 | waiting room | Emergency waiting room |
| 12 | Adult emergency waiting room—critical patient tower | 1 | waiting room | Emergency waiting room |
| 13 | Emergency waiting room for children critical patient tower baseboard | −1 | waiting room | Emergency waiting room for children critical patient tower baseboard |
| 14 | Emergency waiting room for children critical patient tower baseboard | −1 | waiting room | Emergency waiting room for children critical patient tower baseboard |
| 15 | Sterilization tower critical patient baseboard | −1 | services | Sterilization tower critical patient baseboard |
| 16 | Sterilization tower critical patient baseboard | −1 | services | Sterilization tower critical patient baseboard |
| 17 | General pharmacy | 1 | services | Pharmacy warehouse-central: stores insulin and hormoNES that need refrigeration |
| 18 | General pharmacy | 1 | services | General pharmacy |
| 19 | Laundry | 1 | services | Laundry |
| 20 | Laundry | 1 | services | Laundry |
| 21 | Feeding | 1 | services | Food Center |
| 22 | Monoblock | 2 | waiting room | Pensioners—nursing station |
| 23 | Monoblock | 2 | hallway | pensioners-outside room 22 |
| 24 | Monoblock | 3 | hallway | Aisle—medicine women |
| 25 | Monoblock | 3 | hallway | Aisle—ICU covid—room 39 |
| 26 | Monoblock | 2 | hallway | Aisle (swap 1) |
| 27 | Monoblock | 4 | hallway | Aisle—delivery room |
| 28 | Monoblock | 4 | hallway | Aisle obstetric recovery |
| 29 | Monoblock | 5 | services | Milk dietary Services room |
| 30 | Monoblock | 5 | hallway | Pediatrics |
| 31 | Monoblock | 5 | hallway | Neonatology |
| 32 | Monoblock | 4 | hallway | Gynecology |
| 33 | Monoblock | 3 | hallway | Pediatrics—critical patient unit |
| 34 | Pharmacy mix | 5 | services | Pharmacy mix |
| 35 | Monoblock baseboard mechanical workshop | 1 | services | Monoblock workshop |
| Indicador | Description | Additivity | Source |
|---|---|---|---|
| Ind | Energy consumption per m | Yes | [63] |
| Ind | Energy consumption per user | Yes | [63] |
| Ind | Installed power | Yes | [63] |
| Ind | CO | Yes | [67] |
| Ind | Estimated CO generation per person | No | [84] |
| Ind | Thermal comfort level | No | [31] |
| Ind | Compliance level ASHRAE Standard 62.1 2013 and 170. 2017 | No | [85,86] |
| Ind | pm25 standard compliance level | No | [85] |
| Ind | pm10 standard compliance level | No | [85] |
| Ind | Indoor ambient temperature | Yes | [86] |
| Ind | Outdoor ambient temperature | Yes | [86] |
| Ind | Perception of thermal comfort vs. number of pathologies | No | Hospital staff |
| Ind | Number of COVID-19 infections | Yes | Hospital staff |
| Ind | Number of infections Influenza | Yes | Hospital staff |
| Ind | Relationship between CO and viral transmission COVID | Yes | Hospital staff |
| Ind | Relationship between CO and influenza viral transmission | Yes | Hospital staff |
| Dimension | Degree | Hierarchies |
|---|---|---|
| Time | 5 | |
| Building | 2 | |
| Activity | 3 | |
| Space | 5 |
| Specificity | Degree | Hierarchy | Cardinality |
|---|---|---|---|
| minute | 6 | 7,778,000 | |
| hour | 5 | 133,920 | |
| tract | 4 | 32,400 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcés, H.O.; Durán, C.; Espinosa, E.; Jerez, A.; Palominos, F.; Hinojosa, M.; Carrasco, R. Monitoring of Thermal Comfort and Air Quality for Sustainable Energy Management inside Hospitals Based on Online Analytical Processing and the Internet of Things. Int. J. Environ. Res. Public Health 2022, 19, 12207. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912207
Garcés HO, Durán C, Espinosa E, Jerez A, Palominos F, Hinojosa M, Carrasco R. Monitoring of Thermal Comfort and Air Quality for Sustainable Energy Management inside Hospitals Based on Online Analytical Processing and the Internet of Things. International Journal of Environmental Research and Public Health. 2022; 19(19):12207. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912207
Chicago/Turabian StyleGarcés, Hugo O., Claudia Durán, Eduardo Espinosa, Alejandro Jerez, Fredi Palominos, Marcela Hinojosa, and Raúl Carrasco. 2022. "Monitoring of Thermal Comfort and Air Quality for Sustainable Energy Management inside Hospitals Based on Online Analytical Processing and the Internet of Things" International Journal of Environmental Research and Public Health 19, no. 19: 12207. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912207