
HIV Knowledge and Stigmatizing Attitude towards People Living with HIV/AIDS among Medical Students in Jordan

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Permission
2.3. HIV Knowledge Survey Items
2.4. Assessment of the Stigmatizing Attitude towards PLWHA
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
3.2. Variable Levels of HIV/AIDS Knowledge Based on the Survey Item
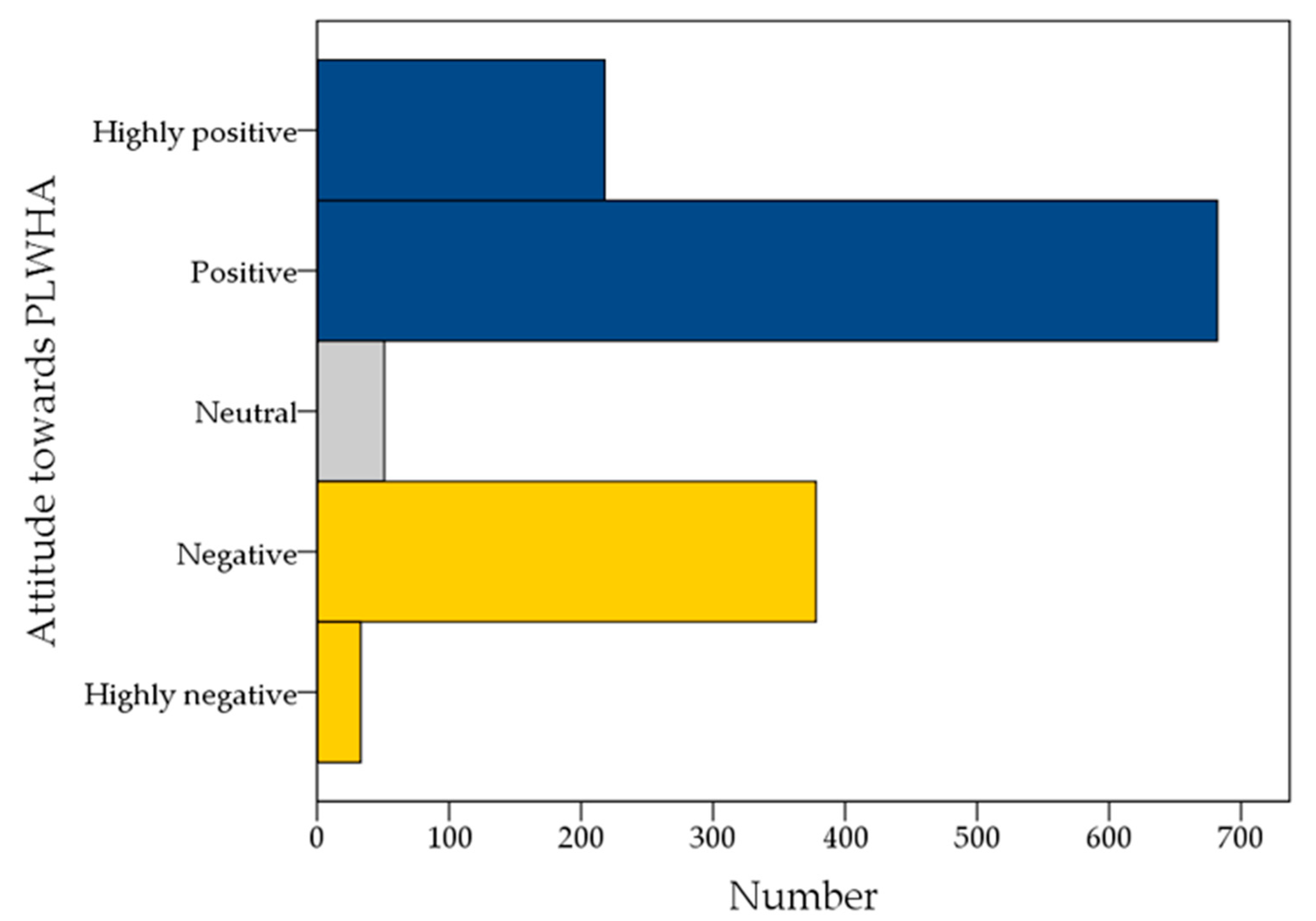
3.3. Analysis of the Stigmatizing Attitude towards PLWHA
3.4. Predictors of HIV Stigmatizing Attitude among the Study Respondents Based on HIV-Stigma Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Cock, K.M.; Jaffe, H.W.; Curran, J.W. Reflections on 40 Years of AIDS. Emerg. Infect. Dis. 2021, 27, 1553–1560. [Google Scholar] [CrossRef]
- Stangl, A.L.; Lloyd, J.K.; Brady, L.M.; Holland, C.E.; Baral, S. A systematic review of interventions to reduce HIV-related stigma and discrimination from 2002 to 2013: How far have we come? J. Int. AIDS Soc. 2013, 16 (Suppl. 2), 18734. [Google Scholar] [CrossRef]
- Katz, I.T.; Ryu, A.E.; Onuegbu, A.G.; Psaros, C.; Weiser, S.D.; Bangsberg, D.R.; Tsai, A.C. Impact of HIV-related stigma on treatment adherence: Systematic review and meta-synthesis. J. Int. AIDS Soc. 2013, 16 (Suppl. 2), 18640. [Google Scholar] [CrossRef]
- Tran, B.X.; Phan, H.T.; Latkin, C.A.; Nguyen, H.L.T.; Hoang, C.L.; Ho, C.S.H.; Ho, R.C.M. Understanding Global HIV Stigma and Discrimination: Are Contextual Factors Sufficiently Studied? (GAP(RESEARCH)). Int. J. Environ. Res. Public Health 2019, 16, 1899. [Google Scholar] [CrossRef] [Green Version]
- Greenwood, G.L.; Wilson, A.; Bansal, G.P.; Barnhart, C.; Barr, E.; Berzon, R.; Boyce, C.A.; Elwood, W.; Gamble-George, J.; Glenshaw, M.; et al. HIV-Related Stigma Research as a Priority at the National Institutes of Health. AIDS Behav. 2021, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Florom-Smith, A.L.; De Santis, J.P. Exploring the concept of HIV-related stigma. Nurs. Forum 2012, 47, 153–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambers, L.A.; Rueda, S.; Baker, D.N.; Wilson, M.G.; Deutsch, R.; Raeifar, E.; Rourke, S.B. Stigma, HIV and health: A qualitative synthesis. BMC Public Health 2015, 15, 848. [Google Scholar] [CrossRef] [Green Version]
- Parker, R.; Aggleton, P. HIV and AIDS-related stigma and discrimination: A conceptual framework and implications for action. Soc. Sci. Med. 2003, 57, 13–24. [Google Scholar] [CrossRef]
- McCrae, R.R.; Costa, P.T.; Martin, T.A.; Oryol, V.E.; Senin, I.G.; O’Cleirigh, C. Personality correlates of HIV stigmatization in Russia and the United States. J. Res. Personal. 2007, 41, 190–196. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L.; Phelan, J.C.; Link, B.G. Stigma as a fundamental cause of population health inequalities. Am. J. Public Health 2013, 103, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Vorasane, S.; Jimba, M.; Kikuchi, K.; Yasuoka, J.; Nanishi, K.; Durham, J.; Sychareun, V. An investigation of stigmatizing attitudes towards people living with HIV/AIDS by doctors and nurses in Vientiane, Lao PDR. BMC Health Serv. Res. 2017, 17, 125. [Google Scholar] [CrossRef] [Green Version]
- Rintamaki, L.; Kosenko, K.; Hogan, T.; Scott, A.M.; Dobmeier, C.; Tingue, E.; Peek, D. The Role of Stigma Management in HIV Treatment Adherence. Int. J. Environ. Res. Public Health 2019, 16, 5003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, L.; Macintyre, K.; Trujillo, L. Interventions to reduce HIV/AIDS stigma: What have we learned? AIDS Educ. Prev. 2003, 15, 49–69. [Google Scholar] [CrossRef] [PubMed]
- Vanable, P.A.; Carey, M.P.; Blair, D.C.; Littlewood, R.A. Impact of HIV-related stigma on health behaviors and psychological adjustment among HIV-positive men and women. AIDS Behav. 2006, 10, 473–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masedo, A.; Grandón, P.; Saldivia, S.; Vielma-Aguilera, A.; Castro-Alzate, E.S.; Bustos, C.; Romero-López-Alberca, C.; Pena-Andreu, J.M.; Xavier, M.; Moreno-Küstner, B. A multicentric study on stigma towards people with mental illness in health sciences students. BMC Med. Educ. 2021, 21, 324. [Google Scholar] [CrossRef]
- Platten, M.; Pham, H.N.; Nguyen, H.V.; Nguyen, N.T.; Le, G.M. Knowledge of HIV and factors associated with attitudes towards HIV among final-year medical students at Hanoi medical university in Vietnam. BMC Public Health 2014, 14, 265. [Google Scholar] [CrossRef] [Green Version]
- Machowska, A.; Bamboria, B.L.; Bercan, C.; Sharma, M. Impact of ‘HIV-related stigma-reduction workshops’ on knowledge and attitude of healthcare providers and students in Central India: A pre-test and post-test intervention study. BMJ Open 2020, 10, e033612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyblade, L.; Stangl, A.; Weiss, E.; Ashburn, K. Combating HIV stigma in health care settings: What works? J. Int. AIDS Soc. 2009, 12, 15. [Google Scholar] [CrossRef] [Green Version]
- Boakye, D.S.; Mavhandu-Mudzusi, A.H. Nurses knowledge, attitudes and practices towards patients with HIV and AIDS in Kumasi, Ghana. Int. J. Afr. Nurs. Sci. 2019, 11, 100147. [Google Scholar] [CrossRef]
- Ding, L.; Landon, B.E.; Wilson, I.B.; Wong, M.D.; Shapiro, M.F.; Cleary, P.D. Predictors and consequences of negative physician attitudes toward HIV-infected injection drug users. Arch. Intern. Med. 2005, 165, 618–623. [Google Scholar] [CrossRef]
- Harapan, H.; Feramuhawan, S.; Kurniawan, H.; Anwar, S.; Andalas, M.; Hossain, M.B. HIV-related stigma and discrimination: A study of health care workers in Banda Aceh, Indonesia. Med. J. Indones. 2013, 22, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Fauk, N.K.; Ward, P.R.; Hawke, K.; Mwanri, L. HIV Stigma and Discrimination: Perspectives and Personal Experiences of Healthcare Providers in Yogyakarta and Belu, Indonesia. Front. Med. 2021, 8, 625787. [Google Scholar] [CrossRef] [PubMed]
- Cowgill, B.O.; Bogart, L.M.; Corona, R.; Ryan, G.; Schuster, M.A. Fears about HIV transmission in families with an HIV-infected parent: A qualitative analysis. Pediatrics 2008, 122, e950–e958. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, M.L.; Bharat, S.; Ramakrishna, J.; Heylen, E. Blame, symbolic stigma and HIV misconceptions are associated with support for coercive measures in urban India. AIDS Behav. 2012, 16, 700–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gökengin, D.; Doroudi, F.; Tohme, J.; Collins, B.; Madani, N. HIV/AIDS: Trends in the Middle East and North Africa region. Int. J. Infect. Dis. 2016, 44, 66–73. [Google Scholar] [CrossRef] [Green Version]
- Sallam, M.; Şahin, G.; Ingman, M.; Widell, A.; Esbjörnsson, J.; Medstrand, P. Genetic characterization of human immunodeficiency virus type 1 transmission in the Middle East and North Africa. Heliyon 2017, 3, e00352. [Google Scholar] [CrossRef] [Green Version]
- UNAIDS. 2020 Global AIDS Update—Seizing the Moment—Tackling Entrenched Inequalities to End Epidemics. Available online: https://www.unaids.org/sites/default/files/media_asset/2020_global-aids-report_executive-summary_en.pdf (accessed on 18 October 2021).
- Shawky, S.; Soliman, C.; Kassak, K.M.; Oraby, D.; El-Khoury, D.; Kabore, I. HIV surveillance and epidemic profile in the Middle East and North Africa. J. Acquir. Immune Defic. Syndr. 2009, 51 (Suppl. 3), S83–S95. [Google Scholar] [CrossRef] [Green Version]
- El Feki, S. Middle-Eastern AIDS efforts are starting to tackle taboos. Lancet 2006, 367, 975–976. [Google Scholar] [CrossRef]
- Abou El Fadl, R.K.; Abdelmoety, A.; Farahat, Z.; Hussein, M.A. Assessing the levels of HIV-related knowledge and attitudes toward HIV-infected patients among undergraduate dental students: A cross-sectional study. HIV AIDS 2019, 11, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Badahdah, A.M. Stigmatization of persons with HIV/AIDS in Saudi Arabia. J. Transcult. Nurs. 2010, 21, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Aldhaleei, W.A.; Bhagavathula, A.S. HIV/AIDS-knowledge and attitudes in the Arabian Peninsula: A systematic review and meta-analysis. J. Infect. Public Health 2020, 13, 939–948. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Ettarras, H.; Jaafreh, D.; Hasan, H.; Al-Salahat, K.; Al-Fraihat, E.; Hassona, Y.; et al. Lack of knowledge regarding HPV and its relation to oropharyngeal cancer among medical students. Cancer Rep. 2021, e1517. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Fraihat, E.; Dababseh, D.; Yaseen, A.; Taim, D.; Zabadi, S.; Hamdan, A.A.; Hassona, Y.; Mahafzah, A.; Şahin, G. Dental students’ awareness and attitudes toward HPV-related oral cancer: A cross sectional study at the University of Jordan. BMC Oral Health 2019, 19, 171. [Google Scholar] [CrossRef] [Green Version]
- Haroun, D.; El Saleh, O.; Wood, L.; Mechli, R.; Al Marzouqi, N.; Anouti, S. Assessing Knowledge of, and Attitudes to, HIV/AIDS among University Students in the United Arab Emirates. PLoS ONE 2016, 11, e0149920. [Google Scholar] [CrossRef] [Green Version]
- Memish, Z.A.; Filemban, S.M.; Bamgboyel, A.; Al Hakeem, R.F.; Elrashied, S.M.; Al-Tawfiq, J.A. Knowledge and Attitudes of Doctors Toward People Living With HIV/AIDS in Saudi Arabia. J. Acquir. Immune Defic. Syndr. 2015, 69, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Lyons, C.E.; Schwartz, S.R.; Murray, S.M.; Shannon, K.; Diouf, D.; Mothopeng, T.; Kouanda, S.; Simplice, A.; Kouame, A.; Mnisi, Z.; et al. The role of sex work laws and stigmas in increasing HIV risks among sex workers. Nat. Commun. 2020, 11, 773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abou Kassm, S.; Naja, W.; Haddad, R.; Baddoura, R.; Mdawar, B.; Riachy, N.; Azar, S.; Zrour, C.; Mokhbat, J. Lebanese People Living with HIV: Psychiatric Co-morbidities and Psycho-Social Environment. Community Ment. Health J. 2021, 57, 1400–1408. [Google Scholar] [CrossRef] [PubMed]
- McFarland, W.; Abu-Raddad, L.J.; Mahfoud, Z.; DeJong, J.; Riedner, G.; Forsyth, A.; Khoshnood, K. HIV/AIDS in the Middle East and North Africa: New study methods, results, and implications for prevention and care. AIDS 2010, 24 (Suppl. 2), S1–S4. [Google Scholar] [CrossRef] [Green Version]
- Checkmarket. Sample Size Calculator. Available online: https://www.checkmarket.com/ (accessed on 8 March 2021).
- Baytner-Zamir, R.; Lorber, M.; Hermoni, D. Assessment of the knowledge and attitudes regarding HIV/AIDS among pre-clinical medical students in Israel. BMC Res. Notes 2014, 7, 168. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Wu, Z.; Wu, S.; Zhaoc, Y.; Jia, M.; Yan, Z. HIV-related stigma in health care settings: A survey of service providers in China. AIDS Patient Care STDS 2007, 21, 753–762. [Google Scholar] [CrossRef]
- Beaulieu, M.; Adrien, A.; Potvin, L.; Dassa, C.; Comité Consultatif sur les Attitudes Envers les PVVIH. Stigmatizing attitudes towards people living with HIV/AIDS: Validation of a measurement scale. BMC Public Health 2014, 14, 1246. [Google Scholar] [CrossRef] [Green Version]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Alwafi, H.A.; Meer, A.M.T.; Shabkah, A.; Mehdawi, F.S.; El-Haddad, H.; Bahabri, N.; Almoallim, H. Knowledge and attitudes toward HIV/AIDS among the general population of Jeddah, Saudi Arabia. J. Infect. Public Health 2018, 11, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Al-Rabeei, N.A.; Dallak, A.M.; Al-Awadi, F.G. Knowledge, attitude and beliefs towards HIV/AIDS among students of health institutes in Sana’a city. East. Mediterr. Health J. 2012, 18, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Al-Khasawneh, E.M.; Ismayilova, L.; Seshan, V.; Hmoud, O.; El-Bassel, N. Predictors of Human Immunodeficiency Virus Knowledge among Jordanian Youths. Sultan Qaboos Univ. Med. J. 2013, 13, 232–240. [Google Scholar] [CrossRef] [Green Version]
- Sallam, M.; Al-Mahzoum, K.; Eid, H.; Assaf, A.M.; Abdaljaleel, M.; Al-Abbadi, M.; Mahafzah, A. Attitude towards HPV Vaccination and the Intention to Get Vaccinated among Female University Students in Health Schools in Jordan. Vaccines 2021, 9, 1432. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Ghanem, K.G.; Feizzadeh, A.; Setayesh, H.; Calleja, J.M.; Riedner, G. HIV and other sexually transmitted infection research in the Middle East and North Africa: Promising progress? Sex. Transm. Infect. 2013, 89 (Suppl. 3), iii1–iii4. [Google Scholar] [CrossRef] [Green Version]
- Mumtaz, G.R.; Riedner, G.; Abu-Raddad, L.J. The emerging face of the HIV epidemic in the Middle East and North Africa. Curr. Opin HIV AIDS 2014, 9, 183–191. [Google Scholar] [CrossRef]
- Mumtaz, G.; Hilmi, N.; McFarland, W.; Kaplan, R.L.; Akala, F.A.; Semini, I.; Riedner, G.; Tawil, O.; Wilson, D.; Abu-Raddad, L.J. Are HIV epidemics among men who have sex with men emerging in the Middle East and North Africa? A systematic review and data synthesis. PLoS Med. 2010, 8, e1000444. [Google Scholar] [CrossRef] [Green Version]
- Mumtaz, G.R.; Weiss, H.A.; Thomas, S.L.; Riome, S.; Setayesh, H.; Riedner, G.; Semini, I.; Tawil, O.; Akala, F.A.; Wilson, D.; et al. HIV among people who inject drugs in the Middle East and North Africa: Systematic review and data synthesis. PLoS Med. 2014, 11, e1001663. [Google Scholar] [CrossRef] [Green Version]
- Chemaitelly, H.; Weiss, H.A.; Calvert, C.; Harfouche, M.; Abu-Raddad, L.J. HIV epidemiology among female sex workers and their clients in the Middle East and North Africa: Systematic review, meta-analyses, and meta-regressions. BMC Med. 2019, 17, 119. [Google Scholar] [CrossRef] [PubMed]
- Heijnen, M.; Mumtaz, G.R.; Abu-Raddad, L.J. Status of HIV and hepatitis C virus infections among prisoners in the Middle East and North Africa: Review and synthesis. J. Int. AIDS Soc. 2016, 19, 20873. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A.P.; Sayles, J.N.; Patel, V.A.; Remien, R.H.; Sawires, S.R.; Ortiz, D.J.; Szekeres, G.; Coates, T.J. Stigma in the HIV/AIDS epidemic: A review of the literature and recommendations for the way forward. AIDS 2008, 22 (Suppl. 2), S67–S79. [Google Scholar] [CrossRef] [Green Version]
- Badahdah, A.M.; Sayem, N. HIV-related knowledge and AIDS stigma among college students in Yemen. East. Mediterr. Health J. 2010, 16, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Al-Amoudi, S.M.; Al-Harbi, A.A.; Al-Sayegh, N.Y.; Eldeek, B.S.; Kafy, S.M.; Al-Ahwal, M.S.; Bondagji, N.S. Health rights knowledge among medical school students at King Abdulaziz University, Jeddah, Saudi Arabia. PLoS ONE 2017, 12, e0176714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawwad, T.A.; Washburn, M.; Torres, L.R.; Sampson, M. HIV Knowledge of Middle Eastern and North Africans 18-35 Residing in the U.S.: A Cross Sectional Study. Soc. Work Public Health 2020, 35, 494–509. [Google Scholar] [CrossRef]
- Nguyen, T.A.; Oosterhoff, P.; Pham, Y.N.; Hardon, A.; Wright, P. Health workers’ views on quality of prevention of mother-to-child transmission and postnatal care for HIV-infected women and their children. Hum. Resour. Health 2009, 7, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Tadakamadla, J.; Areeshi, A.Y.B.H.; Tobaigy, H.A.W.M. Knowledge and attitudes towards HIV/AIDS among dental students of Jazan University, Kingdom Saudi Arabia. Saudi Dent. J. 2018, 30, 47–52. [Google Scholar] [CrossRef]
- Abdelrahman, I.; Lohiniva, A.L.; Kandeel, A.; Benkirane, M.; Atta, H.; Saleh, H.; El Sayed, N.; Talaat, M. Learning about Barriers to Care for People Living with HIV in Egypt: A Qualitative Exploratory Study. J. Int. Assoc. Provid. AIDS Care 2015, 14, 141–147. [Google Scholar] [CrossRef] [Green Version]
- Hassan, Z.M.; Wahsheh, M.A. Knowledge and attitudes of Jordanian nurses towards patients with HIV/AIDS: Findings from a nationwide survey. Issues Ment. Health Nurs. 2011, 32, 774–784. [Google Scholar] [CrossRef]
- Algaralleh, A.; Altwalbeh, D.; Al-Tarawneh, F. Health-Related Quality of Life among Persons Living with HIV/AIDS in Jordan: An Exploratory Study. HIV AIDS 2020, 12, 897–907. [Google Scholar] [CrossRef]
- Mahafzah, A.M.; Al-Ramahi, M.Q.; Asa’d, A.M.; El-Khateeb, M.S. Prevalence of sexually transmitted infections among sexually active Jordanian females. Sex. Transm. Dis. 2008, 35, 607–610. [Google Scholar] [CrossRef]
- Kabotho, K.T.; Chivese, T. Occupational exposure to HIV among nurses at a major tertiary hospital: Reporting and utilization of post-exposure prophylaxis; A cross-sectional study in the Western Cape, South Africa. PLoS ONE 2020, 15, e0230075. [Google Scholar] [CrossRef] [PubMed]
- Khuri-Bulos, N.A.; Toukan, A.; Mahafzah, A.; Al Adham, M.; Faori, I.; Abu Khader, I.; Abu Rumeileh, Z.I. Epidemiology of needlestick and sharp injuries at a university hospital in a developing country: A 3-year prospective study at the Jordan University Hospital, 1993 through 1995. Am. J. Infect. Control 1997, 25, 322–329. [Google Scholar] [CrossRef]
- Attal, B.A.; Al-Rowaishan, K.M.; Akeel, A.A.; AlAmmar, F.K. HIV stigma in the teaching hospitals in Sana’a, Yemen: A conflict and low-resource setting. BMC Public Health 2021, 21, 1793. [Google Scholar] [CrossRef]
- Alshouibi, E.; Alaqil, F. HIV-Related Discrimination among Senior Dental Students in Jeddah. J. Int. Soc. Prev. Community Dent. 2019, 9, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Badahdah, A.M.; Foote, C.E. Role of shame in the stigmatization of people with human immunodeficiency virus: A survey of female college students in 3 Arab countries. East. Mediterr. Health J. 2010, 16, 982–987. [Google Scholar] [CrossRef]
- Pulerwitz, J.; Michaelis, A.; Weiss, E.; Brown, L.; Mahendra, V. Reducing HIV-related stigma: Lessons learned from Horizons research and programs. Public Health Rep. 2010, 125, 272–281. [Google Scholar] [CrossRef]
- Mohammadi, M.; Bagheri, M.; Jafari, P.; Bazrafkan, L. Motivating medical students for social accountability in medical schools. J. Adv. Med. Educ. Prof. 2020, 8, 90–99. [Google Scholar] [CrossRef]
- Farsi, N.J.; Al Sharif, S.; Al Qathmi, M.; Merdad, M.; Marzouki, H.; Merdad, L. Knowledge of Human Papillomavirus (HPV) and Oropharyngeal Cancer and Acceptability of the HPV Vaccine among Dental Students. Asian Pac. J. Cancer Prev. 2020, 21, 3595–3603. [Google Scholar] [CrossRef]
- Chew, B.H.; Cheong, A.T. Assessing HIV/AIDS Knowledge and Stigmatizing Attitudes among Medical Students in Universiti Putra Malaysia. Med. J. Malays. 2013, 68, 24–29. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Number | Percentage |
|---|---|---|---|
| Sex | Male | 582 | 42.7% |
| Female | 780 | 57.3% | |
| Nationality | Jordanian | 1138 | 83.6% |
| Non-Jordanian 2 | 222 | 16.3% | |
| Preferred not to say | 2 | 0.1% | |
| University | University of Jordan | 802 | 58.9% |
| JUST 3 | 219 | 16.1% | |
| Mutah University | 75 | 5.5% | |
| Hashemite University | 93 | 6.8% | |
| Al-Balqa’ Applied University | 74 | 5.4% | |
| Yarmouk University | 99 | 7.3% | |
| Curriculum year | 1st year | 266 | 19.5% |
| 2nd year | 343 | 25.2% | |
| 3rd year | 244 | 17.9% | |
| 4th year | 218 | 16.0% | |
| 5th year | 164 | 12.0% | |
| 6th year | 127 | 9.3% | |
| Level of study | Pre-clinical | 853 | 62.6% |
| Clinical | 509 | 37.4% | |
| Latest GPA 1 | 3.50–4.00 | 697 | 51.2% |
| 3.00–3.49 | 427 | 31.4% | |
| 2.50–2.99 | 199 | 14.6% | |
| 2.00–2.49 | 36 | 2.6% | |
| Less than 2.00 | 3 | 0.2% |
| HIV Knowledge Item | Level | Pre-Clinical | Clinical | p Value 3 |
|---|---|---|---|---|
| Response 1 | N 2 (%) | N (%) | ||
| HIV can be transmitted through sexual relations | Correct | 838 (98.2) | 508 (99.8) | 0.03239 |
| Incorrect | 9 (1.1) | 1 (0.2) | ||
| I don’t know | 6 (0.7) | 0 | ||
| HIV can be transmitted through infected syringes and needles | Correct | 809 (94.8) | 506 (99.4) | 0.00005 |
| Incorrect | 19 (2.2) | 1 (0.2) | ||
| I don’t know | 25 (2.9) | 2 (0.4) | ||
| HIV can be transmitted through blood transfusion | Correct | 820 (96.1) | 504 (99.0) | 0.00329 |
| Incorrect | 14 (1.6) | 0 | ||
| I don’t know | 19 (2.2) | 5 (1.0) | ||
| HIV can be transmitted from mother to child during pregnancy and labor | Correct | 626 (73.4) | 476 (93.5) | <0.00001 |
| Incorrect | 56 (6.6) | 14 (2.8) | ||
| I don’t know | 171 (20.0) | 19 (3.7) | ||
| HIV can be transmitted through mother to child via breastfeeding | Correct | 360 (42.2) | 196 (38.5) | 0.00005 |
| Incorrect | 202 (23.7) | 176 (34.6) | ||
| I don’t know | 291 (34.1) | 137 (26.9) | ||
| HIV can be transmitted through handshake | Correct | 783 (91.8) | 489 (96.1) | 0.00155 |
| Incorrect | 33 (3.9) | 4 (0.8) | ||
| I don’t know | 37 (4.3) | 16 (3.1) | ||
| HIV can be transmitted through mosquito bites | Correct | 429 (50.3) | 335 (65.8) | <0.00001 |
| Incorrect | 200 (23.4) | 85 (16.7) | ||
| I don’t know | 224 (26.3) | 89 (17.5) | ||
| HIV can be transmitted through hugging a person with HIV infection | Correct | 759 (89.0) | 491 (96.5) | <0.00001 |
| Incorrect | 43 (5.0) | 3 (0.6) | ||
| I don’t know | 51 (6.0) | 15 (2.9) | ||
| HIV can be transmitted through saliva of a person with HIV/AIDS | Correct | 348 (40.8) | 232 (45.6) | 0.21665 |
| Incorrect | 358 (42.0) | 199 (39.1) | ||
| I don’t know | 147 (17.2) | 78 (15.3) | ||
| HIV can be transmitted through using the same tableware used by a person with HIV | Correct | 480 (56.3) | 339 (66.6) | 0.00001 |
| Incorrect | 200 (23.4) | 67 (13.2) | ||
| I don’t know | 173 (20.3) | 103 (20.2) | ||
| It is possible to prevent HIV transmission from mother to fetus | Correct | 333 (39.0) | 332 (65.2) | <0.00001 |
| Incorrect | 79 (9.3) | 29 (5.7) | ||
| I don’t know | 441 (51.7) | 148 (29.1) | ||
| The chance of HIV infection after exposure could be lowered if treatment is given on time after conducting unprotected sexual intercourse | Correct | 432 (50.6) | 334 (65.6) | <0.00001 |
| Incorrect | 138 (16.2) | 44 (8.6) | ||
| I don’t know | 283 (33.2) | 131 (25.7) | ||
| The chance of HIV infection after exposure could be lowered if treatment is given on time after a prick from an infected needle | Correct | 386 (45.3) | 323 (63.5) | <0.00001 |
| Incorrect | 135 (15.8) | 42 (8.3) | ||
| I don’t know | 332 (38.9) | 144 (28.3) | ||
| HIV treatment prolongs the life expectancy of people living with HIV/AIDS | Correct | 659 (77.3) | 442 (86.8) | 0.00003 |
| Incorrect | 70 (8.2) | 17 (3.3) | ||
| I don’t know | 124 (14.5) | 50 (9.8) |
| HIV Knowledge Item (Negative HIV Stigma Compared to Positive Attitude as the Reference) | OR (95% CI) 2 | p Value |
|---|---|---|
| HIV can be transmitted through sexual relations (incorrect response) | 6.84 (0.71–65.77) | 0.096 |
| I don’t know | 2.31 (0.24–22.41) | 0.470 |
| Correct response (reference) | . | . |
| HIV can be transmitted through infected syringes and needles (incorrect response) | 2.61 (0.71–9.58) | 0.150 |
| I don’t know | 0.67 (0.22–2.05) | 0.478 |
| Correct response (reference) | . | . |
| HIV can be transmitted through blood transfusion (incorrect response) | 1.72 (0.26–11.40) | 0.575 |
| I don’t know | 0.54 (0.16–1.85) | 0.330 |
| Correct response (reference) | . | . |
| HIV can be transmitted from mother to child during pregnancy and labor (incorrect response) | 1.51 (0.84–2.71) | 0.173 |
| I don’t know | 0.99 (0.65–1.49) | 0.944 |
| Correct response (reference) | . | . |
| HIV can be transmitted from mother to child via breastfeeding (incorrect response) | 0.71 (0.51–0.99) | 0.045 * |
| I don’t know | 0.85 (0.62–1.17) | 0.327 |
| Correct response (reference) | . | . |
| HIV can be transmitted through handshaking (incorrect response) | 0.34 (0.10–1.13) | 0.077 |
| I don’t know | 0.82 (0.33–2.05) | 0.676 |
| Correct response (reference) | . | . |
| HIV can be transmitted through mosquito bites (incorrect response) | 1.52 (1.10–2.10) | 0.012 * |
| I don’t know | 1.04 (0.74–1.47) | 0.815 |
| Correct response (reference) | . | . |
| HIV can be transmitted through hugging a person with HIV (incorrect response) | 9.88 (2.84–34.34) | <0.001 * |
| I don’t know | 1.67 (0.76–3.64) | 0.202 |
| Correct response (reference) | . | . |
| HIV can be transmitted through saliva of a person with HIV/AIDS (incorrect response) | 1.71 (1.22–2.40) | 0.002 * |
| I don’t know | 1.02 (0.66–1.57) | 0.936 |
| Correct response (reference) | . | . |
| HIV can be transmitted through using the same tableware used by a person with HIV/AIDS (incorrect response) | 2.02 (1.37–2.99) | <0.001 * |
| I don’t know | 1.56 (1.09–2.24) | 0.015 * |
| Correct response (reference) | . | . |
| Nowadays, it is possible to prevent HIV transmission from mother to fetus (incorrect response) | 2.08 (1.27–3.39) | 0.003 * |
| I don’t know | 1.05 (0.78–1.40) | 0.769 |
| Correct response (reference) | . | . |
| The chance of HIV infection after exposure could be lowered if given on time after conducting unprotected sexual intercourse (incorrect response) | 1.19 (0.73–1.94) | 0.479 |
| I don’t know | 1.38 (0.95–1.98) | 0.088 |
| Correct response (reference) | . | . |
| The chance of HIV infection after exposure could be lowered if given on time after a prick from an infected needle (incorrect response) | 0.90 (0.55–1.47) | 0.663 |
| I don’t know | 0.83 (0.58–1.19) | 0.310 |
| Correct response (reference) | . | . |
| The chance of HIV infection after exposure could be lowered if given on time after a prick from an infected needle (incorrect response) | 2.22 (1.32–3.74) | 0.003 * |
| I don’t know | 1.43 (0.97–2.10) | 0.075 |
| Correct response (reference) | . | . |
| Covariates | ||
| Age | 1.23 (0.80–1.90) | 0.350 |
| Sex | 0.81 (0.62–1.05) | 0.113 |
| Nationality | 1.05 (0.73–1.51) | 0.801 |
| Medical school | 1.54 (1.14–2.08) | 0.005 |
| Level of study | 0.82 (0.52–1.30) | 0.406 |
| Latest GPA 1 | 1.19 (0.83–1.71) | 0.341 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sallam, M.; Alabbadi, A.M.; Abdel-Razeq, S.; Battah, K.; Malkawi, L.; Al-Abbadi, M.A.; Mahafzah, A. HIV Knowledge and Stigmatizing Attitude towards People Living with HIV/AIDS among Medical Students in Jordan. Int. J. Environ. Res. Public Health 2022, 19, 745. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020745
Sallam M, Alabbadi AM, Abdel-Razeq S, Battah K, Malkawi L, Al-Abbadi MA, Mahafzah A. HIV Knowledge and Stigmatizing Attitude towards People Living with HIV/AIDS among Medical Students in Jordan. International Journal of Environmental Research and Public Health. 2022; 19(2):745. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020745
Chicago/Turabian StyleSallam, Malik, Ali M. Alabbadi, Sarah Abdel-Razeq, Kareem Battah, Leen Malkawi, Mousa A. Al-Abbadi, and Azmi Mahafzah. 2022. "HIV Knowledge and Stigmatizing Attitude towards People Living with HIV/AIDS among Medical Students in Jordan" International Journal of Environmental Research and Public Health 19, no. 2: 745. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020745