
Mental Health Promotion and Intervention in Occupational Settings: Protocol for a Pilot Study of the MENTUPP Intervention

 , , , ,
, , , ,  , , , , , and
, , , , , and
Abstract
:1. Introduction
- ○
- Evaluate the delivery of the interventions via the MENTUPP Hub;
- ○
- Evaluate the procedures and instruments that will be used to evaluate the MENTUPP intervention;
- ○
- Examine the implementation strategy of the MENTUPP intervention;
- ○
- Estimate parameters required in the power calculations for the MENTUPP cRCT.
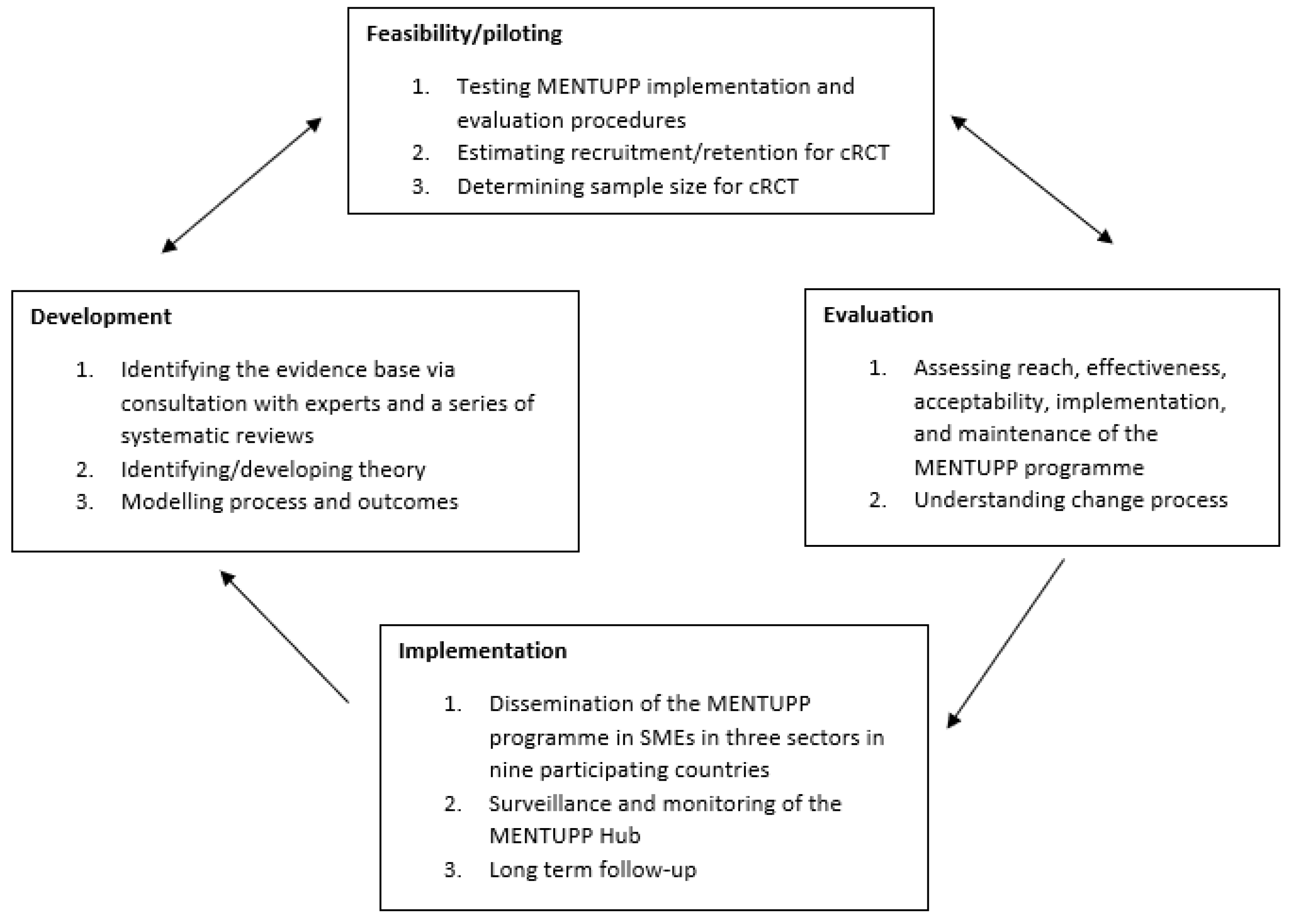
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.2.1. Organisation Level
2.2.2. Individual Level
2.2.3. Sample Size
2.3. Description of the Study Intervention
2.4. Procedure
- (a)
- the agreement to develop a project planning group, with the local research officer, local SME representatives, and a local MENTUPP ‘champion’ (a designated employee within the participating SME who will be leading on the promotion, engagement, and implementation of the project),
- (b)
- the understanding that data on individuals will be kept confidential, will not be shared with the SME, and will only be fed back in aggregated form to provide a high-level overview of how participants responded to the survey,
- (c)
- the permission from management for employees to engage with the intervention during paid work hours.

{kind=link}
{kind=link}
| Module | Aims/Objectives | Material Type(s) | General Material | Sector Specific Versions of the Material | For Employees | For Supervisors |
|---|---|---|---|---|---|---|
| Understanding Mental Wellbeing, Stress and Burnout |
| Online written material | YES | YES | YES | |
| Toolkit: Mental Wellbeing and Stress Management |
| Online written material, reflective exercises, practical exercises | NO | YES | YES | |
| Toolkit: Supervisor Training- Creating Mentally Healthy Workplaces |
| Online written material, | YES | NO | YES | |
| Reflective exercises, | |||||
| Practical checklists | |||||
| Interactive scenarios | |||||
| Toolkit: Supporting Each Other at Work |
| Online written material, Videos, Practical Exercises Resources | YES | YES | NO | |
| Understanding Depression and anxiety |
| Online written material | YES | NO | YES | YES |
| Videos | |||||
| Interactive learning activities | |||||
| Toolkit—Supervisor Training—how to address mental illness in the workplace |
| Online written material, Videos, Practical Exercises | YES | NO | NO | YES |
| Challenging stigma—a guide for employees and leaders |
| Online written material | YES | NO | YES | YES |
| Challenging stigma—a guide for people with mental health issues |
| Online written material | YES | NO | YES | YES |
| Understanding stigma and discrimination—for all |
| Online written material | YES | NO | YES | YES |
| Test your stigma! |
| Online written material | YES | NO | YES | YES |
2.5. Data Collection
Process Evaluation
- ○
- Mental wellbeing and quality of life: The World Health Organisation—Five Wellbeing Index (WHO-5) [85]
- ○
- Depression and anxiety: Patient Health Questionnaire Anxiety and Depression Scale (PHQ-ADS) [86]
- ○
- Depression stigma: Depression Stigma Scale (DSS) [87]
- ○
- Presenteeism in the workplace: Stanford Presenteeism Scale (SPS-6) [88]
- ○
- Productivity: Work Productivity and Activity Impairment—General Health V2.0 (WPAI-GH 2.0) [89]
- ○
- ○
- Help-seeking behaviour: Attitudes Towards Seeking Professional Psychological Help-Short Form (ATSPPH) [91]
- ○
- Presence (level) of psychosocial risk factors and stressors: Selected items and scales from the Copenhagen Psychosocial Questionnaire (COPSOQ) [92]
2.6. Data Management
2.7. Data Analysis
Process and Preliminary Outcome Evaluation
2.8. Ethical Considerations
2.8.1. Duty of Care
2.8.2. Data Protection
3. Discussion
Strengths and Limitations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mishra, S.; Kapoor, S. Employee welfare activities and occupational stress. J. Int. Pharm. Res. 2018, 45, 225–232. [Google Scholar]
- Bonde, J.P.E. Psychosocial factors at work and risk of depression: A systematic review of the epidemiological evidence. Occup. Environ. Med. 2008, 65, 438–445. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Global Plan of Action on Workers’ health (2008–2017): Baseline for Implementation. Available online: https://www.who.int/occupational_health/who_workers_health_web.pdf (accessed on 27 April 2021).
- Cottini, E.; Lucifora, C. Mental Health and Working Conditions in Europe. ILR Rev. 2013, 66, 958–988. [Google Scholar] [CrossRef]
- Weigl, M.; Schneider, A.; Hoffmann, F.; Angerer, P. Work stress, burnout, and perceived quality of care: A cross-sectional study among hospital pediatricians. Eur. J. Pediatr. 2015, 174, 1237–1246. [Google Scholar] [CrossRef]
- Eurofound. Violence and Harassment in European Workplaces: Extent, Impacts and Policies. Available online: https://www.eurofound.europa.eu/publications/report/2015/violence-and-harassment-in-european-workplaces-extent-impacts-and-policies (accessed on 27 April 2021).
- Virtanen, M.; Jokela, M.; Madsen, I.E.; Hanson, L.L.M.; Ll, M.H.; Nyberg, S.T.; Alfredsson, L.; Batty, G.; Bjorner, J.B.; Borritz, M.; et al. Long working hours and depressive symptoms: Systematic review and meta-analysis of published studies and unpublished individual participant data. Scand. J. Work. Environ. Health 2018, 44, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Tijani, B.; Jin, X.; Osei-Kyei, R. A systematic review of mental stressors in the construction industry. Int. J. Build. Pathol. Adapt. 2020, 39, 433–460. [Google Scholar] [CrossRef]
- Chan, A.P.C.; Nwaogu, J.M.; Naslund, J.A. Mental Ill-Health Risk Factors in the Construction Industry: Systematic Review. J. Constr. Eng. Manag. 2020, 146, 04020004. [Google Scholar] [CrossRef]
- OECD. European Union. Health at a Glance: Europe 2020: State of Health in the EU Cycle. 2020. Available online: https://0-www-oecd--ilibrary-org.brum.beds.ac.uk/social-issues-migration-health/health-at-a-glance-europe-2020_82129230-en (accessed on 11 May 2021).
- Wan Mohd Yunus, W.M.A.; Musiat, P.; Brown, J.S.L. Systematic review of universal and targeted workplace interventions for depression. Occup. Environ. Med. 2018, 75, 66. [Google Scholar] [CrossRef]
- Hawton, K.; i Comabella, C.C.; Haw, C.; Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect. Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef]
- Ahola, K.; Hakanen, J.; Perhoniemi, R.; Mutanen, P. Relationship between burnout and depressive symptoms: A study using the person-centred approach. Burn. Res. 2014, 1, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Harvey, S.B.; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Niedhammer, I.; Bertrais, S.; Witt, K. Psychosocial work exposures and health outcomes: A meta-review of 72 literature reviews with meta-analysis. Scand. J. Work Environ. Health 2021, 47, 489–508. [Google Scholar] [CrossRef] [PubMed]
- Shoman, Y.; El May, E.; Marca, S.C.; Wild, P.; Bianchi, R.; Bugge, M.D.; Caglayan, C.; Cheptea, D.; Gnesi, M.; Godderis, L.; et al. Predictors of Occupational Burnout: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 9188. [Google Scholar] [CrossRef] [PubMed]
- Arensman, E.; Wall, A.; McAuliffe, C.; Corcoran, P.; Williamson, E.; McCarthy, J.; Duggan, A.; Perry, I.J. Second Report of the Suicide Support and Information System; National Suicide Research Foundation: Cork, Ireland, 2013; ISSN 2009-4949. [Google Scholar]
- Chen, Z.; Leng, J.; Pang, Y.; He, Y.; Heng, F.; Tang, L. Demographic, occupational, and societal features associated with burnout among medical oncology staff members: Cross-sectional results of a Cancer Center in Beijing, China. Psychooncology 2019, 28, 2365–2373. [Google Scholar] [CrossRef]
- Wong, K.; Chan, A.H.S.; Ngan, S.C. The Effect of Long Working Hours and Overtime on Occupational Health: A Meta-Analysis of Evidence from 1998 to 2018. Int. J. Environ. Res. Public Health 2019, 16, 2102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lartey, J.K.S.; Osafo, J.; Andoh-Arthur, J.; Asante, K.O. Emotional experiences and coping strategies of nursing and midwifery practitioners in Ghana: A qualitative study. BMC Nurs. 2020, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.; Hawgood, J.; Klieve, H.; Kõlves, K.; De Leo, D. Suicide in Selected Occupations in Queensland: Evidence from the State Suicide Register. Aust. N. Z. J. Psychiatry 2010, 44, 243–249. [Google Scholar] [CrossRef]
- Burki, T. Mental health in the construction industry. Lancet Psychiatry 2018, 5, 303. [Google Scholar] [CrossRef]
- Milner, A.; Niven, H.; LaMontagne, A.D. Suicide by occupational skill level in the Australian construction industry: Data from 2001 to 2010. Aust. N. Z. J. Public Health 2014, 38, 281–285. [Google Scholar] [CrossRef]
- National Statistics Office. Suicide by Occupation, England 2011–2015. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/suicidebyoccupation/england2011to2015 (accessed on 27 April 2021).
- Heller, T.S.; Hawgood, J.; De Leo, D. Correlates of Suicide in Building Industry Workers. Arch. Suicide Res. 2007, 11, 105–117. [Google Scholar] [CrossRef]
- Gullestrup, J.; Lequertier, B.; Martin, G. MATES in Construction: Impact of a Multimodal, Community-Based Program for Suicide Prevention in the Construction Industry. Int. J. Environ. Res. Public Health 2011, 8, 4180–4196. [Google Scholar] [CrossRef] [PubMed]
- Boschman, J.; van der Molen, H.; Sluiter, J.; Frings-Dresen, M. Psychosocial work environment and mental health among construction workers. Appl. Ergon. 2013, 44, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Berg-Beckhoff, G.; Nielsen, G.; Larsen, E.L. Use of information communication technology and stress, burnout, and mental health in older, middle-aged, and younger workers—Results from a systematic review. Int. J. Occup. Environ. Health 2017, 23, 160–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padma, V.; Anand, N.N.; Gurukul, S.S.; Javid, S.S.M.; Prasad, A.; Arun, S. Health problems and stress in Information Tech-nology and Business Process Outsourcing employees. J. Pharm. Bioallied Sci. 2015, 7 (Suppl. 1), S9–S13. [Google Scholar] [CrossRef]
- Ross, V.; Caton, N.; Gullestrup, J.; Kõlves, K. Understanding the Barriers and Pathways to Male Help-Seeking and Help-Offering: A Mixed Methods Study of the Impact of the Mates in Construction Program. Int. J. Environ. Res. Public Health 2019, 16, 2979. [Google Scholar] [CrossRef] [Green Version]
- Kuster, A.T.; Dalsbø, T.K.; Thanh, B.Y.L.; Agarwal, A.; Durand-Moreau, Q.V.; Kirkehei, I. Computer-based versus in-person interventions for preventing and reducing stress in workers. Cochrane Database Syst. Rev. 2017, 2017, CD011899. [Google Scholar] [CrossRef]
- Giorgi, G.; Lecca, L.I.; Alessio, F.; Finstad, G.L.; Bondanini, G.; Lulli, L.G.; Arcangeli, G.; Mucci, N. COVID-19-Related Mental Health Effects in the Workplace: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 7857. [Google Scholar] [CrossRef]
- Martin, A.; Kilpatrick, M.; Scott, J.; Cocker, F.; Dawkins, S.; Brough, P.; Sanderson, K. Protecting the Mental Health of Small-to-Medium Enterprise Owners. J. Occup. Environ. Med. 2020, 62, 503–510. [Google Scholar] [CrossRef]
- Cocker, F.; Martin, A.; Scott, J.; Venn, A.; Sanderson, K. Psychological distress and related work attendance among small-to-medium enterprise owner/managers: Literature review and research agenda. Int. J. Ment. Health Promot. 2012, 14, 219–236. [Google Scholar] [CrossRef]
- Linnan, L.; Bowling, M.; Childress, J.; Lindsay, G.; Blakey, C.; Pronk, S.; Wieker, S.; Royall, P. Results of the 2004 National Worksite Health Promotion Survey. Am. J. Public Health 2008, 98, 1503–1509. [Google Scholar] [CrossRef]
- Martin, A.; Sanderson, K.; Scott, J.; Brough, P. Promoting mental health in small-medium enterprises: An evaluation of the “Business in Mind” program. BMC Public Health 2009, 9, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, A.; Karanika-Murray, M.; Biron, C.; Sanderson, K. The Psychosocial Work Environment, Employee Mental Health and Organizational Interventions: Improving Research and Practice by Taking a Multilevel Approach. Stress Health 2014, 32, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.A.; McHugh, M.D.; Aiken, L.H. Nurse Outcomes in Magnet® and Non-Magnet Hospitals. JONA. J. Nurs. Adm. 2011, 41, 428–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, L.; Wang, M.-J.; Modini, M.; Joyce, S.; Mykletun, A.; Christensen, H.; Harvey, S.B. Preventing the development of depression at work: A systematic review and meta-analysis of universal interventions in the workplace. BMC Med. 2014, 12, 74. [Google Scholar] [CrossRef] [Green Version]
- Kubo, H.; Urata, H.; Katsuki, R.; Hirashima, M.; Ueno, S.; Suzuki, Y.; Fujisawa, D.; Hashimoto, N.; Kobara, K.; Cho, T.; et al. Development of MHFA-based 2-h educational program for early intervention in depression among office workers: A single-arm pilot trial. PLoS ONE 2018, 13, e0208114. [Google Scholar] [CrossRef] [Green Version]
- McBeath, M.; Drysdale, M.T.; Bohn, N. Work-integrated learning and the importance of peer support and sense of belonging. Educ. + Train. 2018, 60, 39–53. [Google Scholar] [CrossRef]
- Milner, A.; Maheen, H.; Currier, D.; Lamontagne, A.D. Male suicide among construction workers in Australia: A qualitative analysis of the major stressors precipitating death. BMC Public Health 2017, 17, 584. [Google Scholar] [CrossRef] [Green Version]
- Milner, A.; Page, K.; Spencer-Thomas, S.; LaMontagne, A.D. Workplace suicide prevention: A systematic review of published and unpublished activities. Health Promot. Int. 2014, 30, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Milner, A.; Spittal, M.; Pirkis, J.; LaMontagne, A.D. Suicide by occupation: Systematic review and meta-analysis. Br. J. Psychiatry 2013, 203, 409–416. [Google Scholar] [CrossRef]
- Leka, S.; Iavicoli, S. The psychosocial work environment in times of change: Society and the workplace. Saf. Sci. 2017, 100, 1–3. [Google Scholar] [CrossRef]
- WHO. Mental Health Atlas 2017; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Cancelliere, C.; Cassidy, J.D.; Ammendolia, C.; Côté, P. Are workplace health promotion programs effective at improving pres-enteeism in workers? a systematic review and best evidence synthesis of the literature. BMC Public Health 2011, 11, 395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsutsumi, A.; Nagami, M.; Yoshikawa, T.; Kogi, K.; Kawakami, N. Participatory Intervention for Workplace Improvements on Mental Health and Job Performance Among Blue-Collar Workers: A Cluster Randomized Controlled Trial. J. Occup. Environ. Med. 2009, 51, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-A.; Suh, C.; Park, M.-H.; Kim, K.; Lee, C.-K.; Son, B.-C.; Kim, J.-H.; Lee, J.-T.; Woo, K.-H.; Kang, K.; et al. Effectiveness of a Comprehensive Stress Management Program to Reduce Work-Related Stress in a Medium-Sized Enterprise. Ann. Occup. Environ. Med. 2014, 26, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordoza, M.; Ulrich, R.S.; Manulik, B.J.; Gardiner, S.K.; Fitzpatrick, P.S.; Hazen, T.M.; Mirka, A.; Perkins, R.S. Impact of Nurses Taking Daily Work Breaks in a Hospital Garden on Burnout. Am. J. Crit. Care 2018, 27, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Linzer, M.; Poplau, S.; Grossman, E.; Varkey, A.; Yale, S.; Williams, E.; Hicks, L.; Brown, R.L.; Wallock, J.; Kohnhorst, D.; et al. A Cluster Randomized Trial of Interventions to Improve Work Conditions and Clinician Burnout in Primary Care: Results from the Healthy Work Place (HWP) Study. J. Gen. Intern. Med. 2015, 30, 1105–1111. [Google Scholar] [CrossRef]
- Deneckere, S.; Euwema, M.; Lodewijckx, C.; Panella, M.; Mutsvari, T.; Sermeus, W.; Vanhaecht, K. Better Interprofessional Teamwork, Higher Level of Organized Care, and Lower Risk of Burnout in Acute Health Care Teams Using Care Pathways: A Cluster Randomized Controlled Trial. Med. Care 2013, 51, 99–107. [Google Scholar] [CrossRef]
- DeChant, P.F.; Acs, A.; Rhee, K.B.; Boulanger, T.S.; Snowdon, J.L.; Tutty, M.A.; Sinsky, C.A.; Craig, K.J.T. Effect of organization-directed workplace interventions on physician burnout: A systematic review. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 384–408. [Google Scholar] [CrossRef] [Green Version]
- Panagioti, M.; Panagopoulou, E.; Bower, P.; Lewith, G.; Kontopantelis, E.; Chew-Graham, C.; Dawson, S.; Van Marwijk, H.; Geraghty, K.; Esmail, A. Controlled interventions to reduce burnout in physicians: A systematic review and meta-analysis. JAMA Intern. Med. 2017, 177, 195–205. [Google Scholar] [CrossRef]
- Eren, N.B.; Oztunc, G. The Effects of Aromatherapy on the Stress and Anxiety Levels of Nurses Working in Intensive Care Units. Int. J. Caring Sci. 2017, 10, 1615–1623. [Google Scholar]
- Markwell, P.; Polivka, B.J.; Morris, K.; Ryan, C.; Taylor, A. Snack and Relax®: A Strategy to Address Nurses’ Professional Quality of Life. J. Holist. Nurs. 2016, 34, 80–90. [Google Scholar] [CrossRef]
- Havermans, B.M.; Boot, C.R.; Brouwers, E.P.; Houtman, I.L.; Heerkens, Y.F.; Zijlstra-Vlasveld, M.C.; Twisk, J.W.; Anema, J.R.; Van Der Beek, A.J. Effectiveness of a digital platform-based implementation strategy to prevent work stress in a healthcare organization: A 12-month follow-up controlled trial. Scand. J. Work. Environ. Health 2018, 44, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Muuraiskangas, S.; Harjumaa, M.; Kaipainen, K.; Ermes, M. Process and Effects Evaluation of a Digital Mental Health Intervention Targeted at Improving Occupational Well-Being: Lessons from an Intervention Study with Failed Adoption. JMIR Ment. Health 2016, 3, e13. [Google Scholar] [CrossRef] [PubMed]
- Goode, A.D.; Hadgraft, N.T.; Neuhaus, M.; Healy, G.N. Perceptions of an online “train-the-champion” approach to increase workplace movement. Health Promot Int. 2019, 34, 1179–1190. [Google Scholar] [CrossRef] [PubMed]
- LaMontagne, A.D.; Keegel, T.; Louie, A.M.; Ostry, A. Job stress as a preventable upstream determinant of common mental dis-orders: A review for practitioners and policy-makers. Adv. Ment. Health 2010, 9, 17–35. [Google Scholar] [CrossRef]
- Biggio, G.; Cortese, C.G. Well-Being in the Workplace through Interaction between Individual Characteristics and Organizational Context. 2013. Available online: https://pubmed.ncbi.nlm.nih.gov/23422265/ (accessed on 1 January 2021).
- Pidd, K.; Roche, A.; Cameron, J.; Lee, N.; Jenner, L.; Duraisingam, V. Workplace alcohol harm reduction intervention in Australia: Cluster non-randomised controlled trial: Workplace alcohol harm reduction. Drug Alcohol Rev. 2018, 37, 502–513. [Google Scholar] [CrossRef]
- Reavley, N.; Livingston, J.; Buchbinder, R.; Bennell, K.; Stecki, C.; Osborne, R.H. A systematic grounded approach to the development of complex interventions: The Australian WorkHealth Program—Arthritis as a case study. Soc. Sci. Med. 2010, 70, 342–350. [Google Scholar] [CrossRef]
- Von Thiele Schwarz, U.; Nielsen, K.; Edwards, K.; Hasson, H.; Ipsen, C.; Savage, C.; Simonsen Abildgaard, J.; Richter, A.; Lornudd, C.; Mazzocato, P.; et al. How to design, implement and evaluate organizational interventions for maximum impact: The Sigtuna Principles. Eur. J. Work. Organ. Psychol. 2021, 30, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Sharma, S.D.; Sharma, M. Mental health promotion: A narrative review of emerging trends. Curr. Opin. Psychiatry 2017, 30, 339–345. [Google Scholar] [CrossRef]
- Bostock, S.; Crosswell, A.D.; Prather, A.A.; Steptoe, A. Mindfulness on-the-go: Effects of a mindfulness meditation app on work stress and well-being. J. Occup. Health Psychol. 2019, 24, 127–138. [Google Scholar] [CrossRef]
- Karyotaki, E.; Efthimiou, O.; Miguel, C.; Bermpohl, F.M.G.; Furukawa, T.A.; Cuijpers, P.; Riper, H.; Patel, V.; Mira, A.; Gemmil, A.W.; et al. Internet-Based Cognitive Behavioral Therapy for Depression: A Systematic Review and Individual Patient Data Network Meta-analysis. JAMA Psychiatry 2021, 78, 361–371. [Google Scholar] [CrossRef]
- Lehto, R.H.; Heeter, C.; Allbritton, M.; Wiseman, M. Hospice and Palliative Care Provider Experiences with Meditation Using Mobile Applications. Oncol. Nurs. Forum 2018, 45, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Petrie, K.; Joyce, S.; Tan, L.; Henderson, M.; Johnson, A.; Nguyen, H.; Modini, M.; Groth, M.; Glozier, N.; Harvey, S.B. A framework to create more mentally healthy workplaces: A viewpoint. Aust. N. Z. J. Psychiatry 2017, 52, 15–23. [Google Scholar] [CrossRef] [PubMed]
- LaMontagne, A.D.; Martin, A.; Page, K.M.; Reavley, N.J.; Noblet, A.J.; Milner, A.J.; Keegel, T.; Smith, P.M. Workplace mental health: Developing an integrated intervention approach. BMC Psychiatry 2014, 14, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joyce, S.; Modini, M.; Christensen, H.; Mykletun, A.; Bryant, R.; Mitchell, P.; Harvey, S. Workplace interventions for common mental disorders: A systematic meta-review. Psychol. Med. 2016, 46, 683–697. [Google Scholar] [CrossRef]
- Harris, F.M.; Maxwell, M.; O’Connor, R.C.; Coyne, J.; Arensman, E.; Székely, A.; Gusmão, R.; Coffey, C.; Costa, S.; Cserháti, Z.; et al. Developing social capital in implementing a complex intervention: A process evaluation of the early implementation of a suicide prevention intervention in four European countries. BMC Public Health 2013, 13, 158. [Google Scholar] [CrossRef] [Green Version]
- Billmann, M.; Böhm, M.; Krcmar, H. Use of workplace health promotion apps: Analysis of employee log data. Health Policy Technol. 2020, 9, 285–293. [Google Scholar] [CrossRef]
- Jorm, A.F. Mental health literacy: Empowering the community to take action for better mental health. Am. Psychol. 2012, 67, 231–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donker, T.; Griffiths, K.M.; Cuijpers, P.; Christensen, H. Psychoeducation for depression, anxiety and psychological distress: A meta-analysis. BMC Med. 2009, 7, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smit, E.S.; Linn, A.J.; van Weert, J.C. Taking online computer-tailoring forward: The potential of tailoring the message frame and delivery mode of online health behaviour change interventions. Eur. Health Psychol. 2015, 17, 25–31. Available online: https://www.ehps.net/ehp/index.php/contents/article/view/762 (accessed on 23 September 2021).
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W. Process Evaluation of Complex Interventions Guidance: UK Medical Research Council (MRC) Guidance. MRC Popul. Health Sci. Res. Netw. 2014, 134. Available online: http://eprints.gla.ac.uk/102517/ (accessed on 9 April 2021).
- European Commission. User Guide to SME Definition. Available online: https://ec.europa.eu/regional_policy/sources/conferences/state-aid/sme/smedefinitionguide_en.pdf (accessed on 27 April 2021).
- Eurostat. Statistics on Small and Medium-Sized Enterprises—Statistics Explained. ec.europa.eu. 2020. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php/Statistics_on_small_and_medium-sized_enterprises#General_overview (accessed on 9 April 2021).
- Lamontagne, A.D.; Shann, C.; Martin, A. Developing an Integrated Approach to Workplace Mental Health: A Hypothetical Conversation with a Small Business Owner. Ann. Work Expo. Health 2018, 62, S93–S100. [Google Scholar] [CrossRef] [PubMed]
- Paterson, C.; Leduc, C.; Maxwell, M.; Aust, B.; Amann, B.L.; Cerga-Pashoja, A.; Coppens, E.; Couwenbergh, C.; O’Connor, C.; Arensman, E.; et al. Evidence for implementation of interventions to promote mental health in the workplace: A systematic scoping review protocol. Syst. Rev. 2021, 10, 1–8. [Google Scholar] [CrossRef]
- Biron, C.; Baril-Gingras, G.; Lefebvre, R.; Chabot, S.; Boulay-Leclerc, S. Factors influencing managers’ ownership of organisational health interventions. In Psychosocial Safety Climate. A New Work Stress Theory, 1st ed.; Dolard, M.F., Dormann, C., Idris, M.A., Eds.; Springer Nature: Cham, Switzerland, 2019; pp. 365–384. [Google Scholar]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Kroenke, K.; Wu, J.; Yu, Z.; Bair, M.J.; Kean, J.; Stump, T.; Monahan, P.O. Patient Health Questionnaire Anxiety and Depression Scale: Initial Validation in Three Clinical Trials. Psychosom. Med. 2016, 78, 716–727. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, K.M.; Christensen, H.; Jorm, A.F.; Evans, K.; Groves, C. Effect of web-based depression literacy and cognitive–behavioural therapy interventions on stigmatising attitudes to depression: Randomised controlled trial. Br. J. Psychiatry 2004, 185, 342–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koopman, C.; Pelletier, K.R.; Murray, J.F.; Sharda, C.E.; Berger, M.L.; Turpin, R.S.; Hackleman, P.; Gibson, P.; Holmes, D.M.; Bendel, T. Stanford presenteeism scale: Health status and employee productivity. J. Occup. Environ. Med. 2002, 44, 14–20. [Google Scholar] [CrossRef]
- Reilly, M.C.; Zbrozek, A.S.; Dukes, E.M. The Validity and Reproducibility of a Work Productivity and Activity Impairment Instrument. PharmacoEconomics 1993, 4, 353–365. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B.; Vardakou, I.; Kantas, A. The convergent validity of two burnout instruments: A multi-trait-multimethod analysis. Eur. J. Psychol. Assess. 2003, 19, 12–23. [Google Scholar] [CrossRef]
- Fischer, E.H.; Farina, A. Attitudes toward seeking professional psychological help: A shortened form and considerations for re-search. J. Coll. Stud. Dev. 1995, 36, 368–373. [Google Scholar]
- Pejtersen, J.; Kristensen, T.; Borg, V.; Bjorner, J. The second version of the Copenhagen Psychosocial Questionnaire (COPSOQ II). Scand. J. Public Health 2010, 38, 8–24. [Google Scholar] [CrossRef] [PubMed]
- O’Nyumba, T.; Wilson, K.; Derrick, C.J.; Mukherjee, N. The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods Ecol. Evol. 2018, 9, 20–32. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Awa, W.L.; Plaumann, M.; Walter, U. Burnout prevention: A review of intervention programs. Patient Educ. Couns. 2010, 78, 184–190. [Google Scholar] [CrossRef]
- Corbière, M.; Shen, J.; Rouleau, M.; Dewa, C.S. A systematic review of preventive interventions regarding mental health issues in organizations. Work 2009, 33, 81–116. [Google Scholar] [CrossRef]
- Lamontagne, A.D.; Keegel, T.; Louie, A.M.; Ostry, A.; Landsbergis, P.A. A Systematic Review of the Job-stress Intervention Evaluation Literature, 1990–2005. Int. J. Occup. Environ. Health 2007, 13, 268–280. [Google Scholar] [CrossRef]
- Van Laar, C.; Meeussen, L.; Veldman, J.; Van Grootel, S.; Sterk, N.; Jacobs, C. Coping with Stigma in the Workplace: Understanding the Role of Threat Regulation, Supportive Factors, and Potential Hidden Costs. Front. Psychol. 2019. Available online: https://www.frontiersin.org/articles/10.3389/fpsyg.2019.01879/full (accessed on 1 July 2021). [CrossRef] [Green Version]
- Schreibauer, E.C.; Hippler, M.; Burgess, S.; Rieger, M.A.; Rind, E. Work-Related Psychosocial Stress in Small and Medium-Sized Enterprises: An Integrative Review. Int. J. Environ. Res. Public Health 2020, 17, 7446. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arensman, E.; O’Connor, C.; Leduc, C.; Griffin, E.; Cully, G.; Ní Dhálaigh, D.; Holland, C.; Van Audenhove, C.; Coppens, E.; Tsantila, F.; et al. Mental Health Promotion and Intervention in Occupational Settings: Protocol for a Pilot Study of the MENTUPP Intervention. Int. J. Environ. Res. Public Health 2022, 19, 947. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020947
Arensman E, O’Connor C, Leduc C, Griffin E, Cully G, Ní Dhálaigh D, Holland C, Van Audenhove C, Coppens E, Tsantila F, et al. Mental Health Promotion and Intervention in Occupational Settings: Protocol for a Pilot Study of the MENTUPP Intervention. International Journal of Environmental Research and Public Health. 2022; 19(2):947. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020947
Chicago/Turabian StyleArensman, Ella, Cliodhna O’Connor, Caleb Leduc, Eve Griffin, Grace Cully, Doireann Ní Dhálaigh, Carolyn Holland, Chantal Van Audenhove, Evelien Coppens, Fotini Tsantila, and et al. 2022. "Mental Health Promotion and Intervention in Occupational Settings: Protocol for a Pilot Study of the MENTUPP Intervention" International Journal of Environmental Research and Public Health 19, no. 2: 947. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020947