
Successful Aging for Community-Dwelling Older Adults: An Experimental Study with a Tablet App


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Technology Training and Support
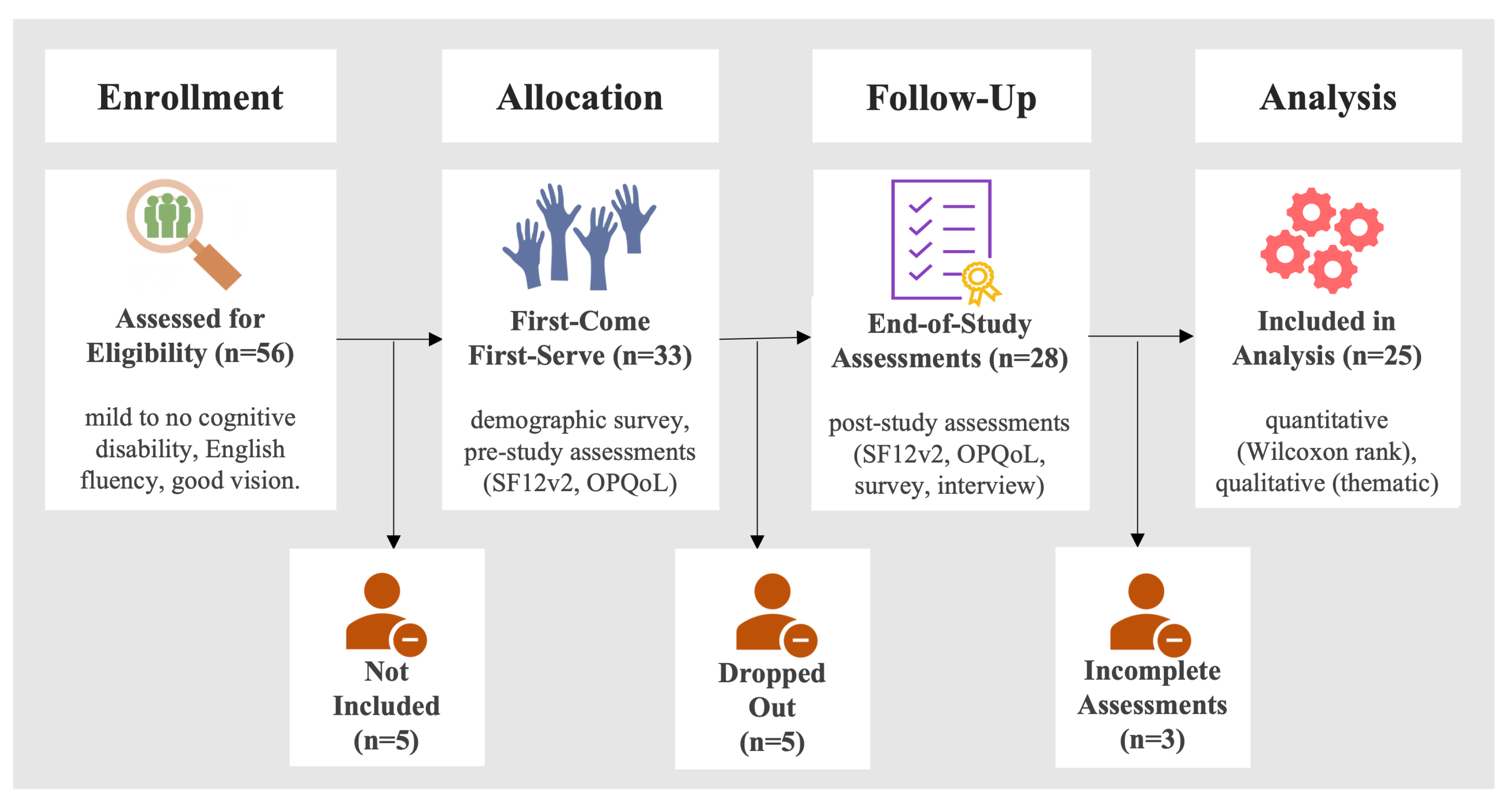
2.3. Study Flow
2.4. Participants
2.5. Tablet Intervention
2.5.1. Platform
2.5.2. Non-Functional Requirements
- (a)
- Performance Requirements
- The applications should be ready for user interaction within 3 s of launch.
- The interfaces should be updated within 2 s of user interaction.
- The database should use normalization to eliminate data redundancy.
- The application should upload new data from the user’s tablets whenever a Wi-Fi connection is available.
- The users’ data from their mobile applications should be uploaded to the central database on a separate thread to prevent the disruption of normal user interactions during the upload.
- (b)
- Safety Requirements
- The data in the central database must be backed up every week.
- (c)
- Security Requirements
- All keys used for the REST API must be stored securely.
- REST API should be the only method of connect to the central database.
- The central database should be behind a firewall.
- The applications must prompt users for password whenever they login.
- (d)
- Software Quality Attributes
- Availability: The AiP staff must be able to access their portal throughout the week at any time during the day. The system unavailability should not be more than one working day, even in the case of unplanned down time.
- Usability: The interface should be easy to learn without a tutorial and should allow users to accomplish their goals without errors.
- Customizable: The system should be flexible to accommodate user specific customizations.
- Accessibility: The system must meet Web Content Accessibility Guidelines 2.1.
2.5.3. Mobile App
- (a)
- Health Goals
- obtain goal suggestions,
- verify goal choices with the care providers,
- set SMART and non-SMART goals,
- track goal progress,
- set reminders about goal tracking,
- obtain help from the AiP staff,
- modify goal choices and settings.
- (b)
- Medication Intake
- enter new medication information (including over-the-counter medication) information, such as medication name, photo, dosage, prescription date, etc.,
- receive medications intake reminders,
- review daily medication schedule,
- track medication count and record intakes,
- review medication intake history,
- request medication refills from the pharmacy,
- update prescription information and medication list.
2.5.4. Web Portal
- review medication and goal tracking history of each participant,
- review new goal and medication entry requests from each participant,
- send messages (reminder or announcements) to each participants,
- read messages sent by each participant,
- create new participant accounts.
- receive medication and goal updates from each participant.
2.5.5. Tablet Games
2.6. Evaluation Questionnaires
2.6.1. Short Form 12-Item (Version 2) Health Survey
2.6.2. Older Person’s Quality of Life
2.6.3. Semi-Structured Interview
2.7. Data Analysis
2.7.1. Descriptive Analysis
2.7.2. Statistical Analysis
2.7.3. Qualitative Analysis
- What benefits of the intervention were perceived by the participants?
- What barriers and challenges of the intervention were perceived by the participants?
3. Results
3.1. Application Usage
3.2. SF12v2 Component Summary Scores
3.2.1. MCS Score
3.2.2. PCS Score
3.3. Health-Related Quality of Life
3.4. Preferences
3.5. Perceived Benefits
3.5.1. Motivation to Care
“It does give you a sense of motivation because once you use the app, you have the things that particular plan when you set the goal you want to accomplish and with the fast pace of life, it is so easy to get distracted from those things and having a tablet would allow you to get back on track. If you are missing out on one area or goals that you set, having the tablet would remind you to remember to set this goal, even though you might have gone outside, you can easily get back on.”
“It has been excellent as far as my medication is concerned. I had gone to a point where I was tired of taking medicine every day and was like not going to do this; so tired of taking this medicine every day. Sometimes, in my mind, I think it would be just okay if I do not take my medication today. Then, the alarms go off, and you are like ‘Okay; it is time for my medication so better to take it now.’”
3.5.2. Awareness of Actions
“It has been very instrumental in helping me see that my medication is very important and maintain a healthy lifestyle because I suffer from depression and I can be sitting in the house, depressed and might have that kind of spell for a week or so. When I am depressed, I want to do nothing. I will clean and only do the necessities. Sometimes, I would take my meds and sometimes I would not, but it [eSeniorCare app] helped me understand it.”
“It made me more aware of my medications. I would not have any problem getting involved with this app, as it is important to track my medications. So, I do not take the same thing more than times that I am supposed to because if I did that, then that could create other medical problems. Thus, it makes a person more conscious of how much medication they are taking. Are they following the medical diagnosis that the doctors have set for them?” (P101).
“It helps me confirm I have taken my medications. The alarm goes off at 9 am and 9 pm. However, I have already taken it; it is right here on the tablet. The tablet is an additional confirmation” (P83).
“It was necessary. This helped me monitor how I spent my time. It told me where I was going. I can visualize my problems. Am I on or off course.”
3.5.3. Better Communication with Providers
“I love my medications on it. When I go to the hospital, they ask you what medications you are on? Here it is on eSeniorCare. Do I carry my prescriptions? No! I present pictures of my meds to the doctor. They appreciate this. They really like the app.” (P110).
“The doctors like it when they can easily see the doses, what you are taking, and how you have taken. Doctors do not have a record and they can only go by what we have told them. It [eSeniorCare] has a record of what you did, are you taking your medicine on time and refilling regularly or not. This makes it easier for doctors because they do not have to look up and ask questions” (P96).
“The app is part of my life. I showed my doctor what I was doing. He was so impressed and said that you were so organized. He told me I could also set a goal to eat more fruits and vegetables to control my depression” (P98).
3.5.4. Self-Management Support
“I used to track using paper. I can replace it with this tablet because when the reminder comes on, you know it is the time to take your medications. I prefer the tablet as it automatically provides reminders and tracks it.”
“When I was taking my insulin, it used to come with little diaries that you could use to write down. I can not write those down now as sometimes my nerves are so sore that writing becomes problematic. After this, I do not plan to go back to paper,” (P101).
3.5.5. Improved Treatment Adherence
“Sometimes I forget to take my medications, when I am at the hall, doing my worship. Then, alarm go off. I like the reminders, they are good,” (P95).
“I like it because it reminds me of my medications. I have never taken medications in my life, so I was not in the practice of taking medications. The app reminds me,” (P98).
“First, I thought I do not need it. I take my medicine on time every day. But now I have started to forget. Sometimes, when I am doing something in the kitchen, I forget it. Then, the alarm goes off and you know it is time to take medications” (P115).
“Technology helps me keep up with my medication. My alarm goes off when it is time to take the medication. I am dependent on my alarms. If I do not hear the alarm, I do not take my medication” (P82).
“One of my goals was to lose some weight. If I do not get up and move, then I am not going to lose weight. I set a goal on the app to go to the gym and that [the eSeniorCare app] made me more accountable” (P110).
3.5.6. Mental Stimulation
“I like tablet games. They are making me think quicker” (P108).
“It is good for the eyes too. It keeps you awake and it keeps you looking. It helps you enjoy. It is beneficial” (P100).
3.6. Perceived Barriers
3.6.1. Misaligned Needs
“It did not help with the medications. I do not have enough medications to where it gets to like” (P102).
“If you could figure out how to put blood pressure on it, that would be key for people checking their blood pressure in the morning and at night. It will be more interesting because people want to know their lifeline because your blood pressure is your number one lifeline” (P133).
3.6.2. Lack of Trust
“I do both because tablet is good to have. I am still a paper-pencil girl. Together they are awesome. Right now, I do it through the tablet. However, there are times when I think I would track with a pencil and paper. I would track the same thing in both places, too many glitches of technology. I once saw a small glitch shut down airlines, so I am likely going to keep both” (P131).
3.6.3. ‘Not-for-Me’ Attitude
“I do not need reminders. I am pretty smart. I wake up, I go to work, I go to the library, and cook supper. I am at the top of my medications. I am constantly aware of time. No alarms help. I know when it is time to take the med. I can take it without looking at time” (P91).
3.6.4. Tracking Burden
“Doing that [goals] and tracking them is hard for me because I am so used to being disciplined in doing things. I don’t think of tracking it. To me, it is normal. It’s like almost second nature” (P76).
“I changed a lot of things. I did not record them, but I looked at the visualizations [goal icons] and knew what I needed to do. So, it did help” (P133).
3.6.5. Privacy Concerns
4. Discussion
Practical Implications
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rowe, J.; Kahn, R. Successful aging. Gerontology 1997, 37, 433–440. [Google Scholar]
- Strawbridge, W.J.; Wallhagen, M.I.; Cohen, R.D. Successful aging and well-being self-rated compared with Rowe and Kahn. Gerontology 2002, 42, 727–733. [Google Scholar]
- Boersma, P.; Black, L.I.; Ward, B.W. Prevalence of Multiple Chronic Conditions Among US Adults, 2018. Prev. Chronic Dis. 2020, 17, 200130. [Google Scholar] [CrossRef] [PubMed]
- Freid, V.M.; Bernstein, A.B.; Bush, M.A. Multiple chronic conditions among adults aged 45 and over; trends over the past 10 years. NCHS Data Briefs 2012, 100, 1–8. [Google Scholar]
- Molton, I.R.; Yorkston, K.M. Growing older with a physical disability: A special application of the successful aging paradigm. J. Gerontol. Ser. B 2017, 72, 290–299. [Google Scholar] [CrossRef] [Green Version]
- Tesch-Römer, C.; Wahl, H.W. Toward a more comprehensive concept of successful aging: Disability and care needs. J. Gerontol. Ser. B 2017, 72, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Bowling, A.; Dieppe, P. What is successful ageing and who should define it? BMJ 2005, 331, 1548–1551. [Google Scholar] [CrossRef] [Green Version]
- Britannica Dictionary. Quality of Life. 2022. Available online: https://www.britannica.com/topic/quality-of-life (accessed on 22 September 2022).
- Roldán González, E.; Lerma Castaño, P.R.; Aranda Zemanate, A.Y.; Caicedo Muñoz, Á.G.; Bonilla Santos, G. Healthy Lifestyles Associated with Socioeconomic Determinants in the Older Adult Population. J. Prim. Care Community Health 2022, 13, 21501319221112808. [Google Scholar] [CrossRef]
- Jang, H.Y. Factors associated with successful aging among community-dwelling older adults based on ecological system model. Int. J. Environ. Res. Public Health 2020, 17, 3220. [Google Scholar] [CrossRef]
- Yoshizawa, Y.; Tanaka, T.; Takahashi, K.; Fujisaki-Sueda-Sakai, M.; Son, B.k.; Iijima, K. Impact of health literacy on the progression of frailty after 4 years among community-dwelling older adults. Int. J. Environ. Res. Public Health 2021, 19, 394. [Google Scholar] [CrossRef]
- Bazargan, M.; Loeza, M.; Ekwegh, T.; Adinkrah, E.K.; Kibe, L.W.; Cobb, S.; Assari, S.; Bazargan-Hejazi, S. Multi-Dimensional Impact of Chronic Low Back Pain among Underserved African American and Latino Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 7246. [Google Scholar] [CrossRef] [PubMed]
- Goda, A.; Murata, S.; Nakano, H.; Nonaka, K.; Iwase, H.; Shiraiwa, K.; Abiko, T.; Anami, K.; Horie, J. The relationship between subjective cognitive decline and health literacy in healthy community-dwelling older adults. Healthcare 2020, 8, 567. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Mira, J.J.; Navarro, I.; Botella, F.; Borrás, F.; Nuño-Solinís, R.; Orozco, D.; Iglesias-Alonso, F.; Pérez-Pérez, P.; Lorenzo, S.; Toro, N. A Spanish pillbox app for elderly patients taking multiple medications: Randomized controlled trial. J. Med. Internet Res. 2014, 16, e99. [Google Scholar] [CrossRef]
- Park, L.G.; Ng, F.; K Shim, J.; Elnaggar, A.; Villero, O. Perceptions and experiences of using mobile technology for medication adherence among older adults with coronary heart disease: A qualitative study. Digit. Health 2020, 6, 2055207620926844. [Google Scholar] [CrossRef] [PubMed]
- Lefler, L.L.; Rhoads, S.J.; Harris, M.; Funderburg, A.E.; Lubin, S.A.; Martel, I.D.; Faulkner, J.L.; Rooker, J.L.; Bell, D.K.; Marshall, H.; et al. Evaluating the use of mobile health technology in older adults with heart failure: Mixed-methods study. JMIR Aging 2018, 1, e12178. [Google Scholar] [CrossRef]
- Case, M.; Burwick, H.; Volpp, K.; Patel, M. Accuracy of smartphone applications and wearable devices for tracking physical activity data. JAMA 2015, 313, 625–626. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, M.D.; Roa, J.R.; Morán, A.L.; Nava-Muñoz, S. CAMMInA: A mobile ambient information system to motivate elders to exercise. Pers. Ubiquitous Comput. 2013, 17, 1127–1134. [Google Scholar] [CrossRef]
- Kim, B.Y.; Lee, J. Smart devices for older adults managing chronic disease: A scoping review. JMIR mHealth uHealth 2017, 5, e69. [Google Scholar] [CrossRef] [Green Version]
- Paiva, J.O.; Andrade, R.M.; de Oliveira, P.A.M.; Duarte, P.; Santos, I.S.; Evangelista, A.L.D.P.; Theophilo, R.L.; de Andrade, L.O.M.; Barreto, I.C.D.H. Mobile applications for elderly healthcare: A systematic mapping. PLoS ONE 2020, 15, e0236091. [Google Scholar] [CrossRef]
- Barbosa Neves, B.; Franz, R.; Judges, R.; Beermann, C.; Baecker, R. Can digital technology enhance social connectedness among older adults? A feasibility study. J. Appl. Gerontol. 2019, 38, 49–72. [Google Scholar] [CrossRef]
- Elavsky, S.; Knapova, L.; Klocek, A.; Smahel, D. Mobile health interventions for physical activity, sedentary behavior, and sleep in adults aged 50 years and older: A systematic literature review. J. Aging Phys. Act. 2019, 27, 565–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, H.y.S.; Shillair, R.; Cotten, S.R.; Winstead, V.; Yost, E. Getting grandma online: Are tablets the answer for increasing digital inclusion for older adults in the US? Educ. Gerontol. 2015, 41, 695–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perimal-Lewis, L.; Maeder, A.; Gordon, S.; Tieman, J. A tablet-based memory enhancement application for older users: Design approach. In Proceedings of the 53rd Hawaii International Conference on System Sciences, Maui, HI, USA, 4–7 January 2020. [Google Scholar]
- Salminen, V.; Sanerma, P.; Niittymäki, S.; Eklund, P. Semantic Infrastructure for Service Environment Supporting Successful Aging. In Data Mining; IntechOpen: London, UK, 2018. [Google Scholar]
- Mehra, S.; Visser, B.; Cila, N.; van den Helder, J.; Engelbert, R.H.; Weijs, P.J.; Kröse, B.J. Supporting older adults to exercise with a tablet: A usability study. JMIR Res. Protoc. 2018, 6, e11598. [Google Scholar]
- Dasgupta, D.; Chaudhry, B.; Koh, E.; Chawla, N.V. A survey of tablet applications for promoting successful aging in older adults. IEEE Access 2016, 4, 9005–9017. [Google Scholar] [CrossRef]
- Dasgupta, D.; Feldman, K.; Waghray, D.; Mikels-Carrasco, W.; Willaert, P.; Raybold, D.; Chawla, N. An integrated and digitized care framework for successful aging. In Proceedings of the 2014 IEEE-EMBS International Conference on Biomedical and Health Informatics (BHI), Valencia, Spain, 1–4 June 2014; pp. 440–443. [Google Scholar]
- Chaudhry, B.; Reeves, K.G.; Chawla, N.V. Successful Aging for Low-Income Older Adults: Towards Design Principles. In Pervasive Health; ACM: New York, NY, USA, 2016; pp. 109–113. [Google Scholar]
- Dasgupta, D.; Reeves, K.G.; Chaudhry, B.; Duarte, M.; Chawla, N.V. eseniorcare: Technology for promoting well-being of older adults in independent living facilities. In Proceedings of the 2016 IEEE International Conference on Healthcare Informatics (ICHI), Chicago, IL, USA, 4–7 October 2016; pp. 461–472. [Google Scholar]
- Dasgupta, D.; Johnson, R.A.; Chaudhry, B.; Reeves, K.G.; Willaert, P.; Chawla, N.V. Design and evaluation of a medication adherence application with communication for seniors in independent living communities. In Proceedings of the Amia Annual Symposium Proceedings, American Medical Informatics Association, Chicago, IL, USA, 12–16 November 2016; Volume 2016, p. 480. [Google Scholar]
- Dasgupta, D.; Chaudhry, B.; Chawla, N. A Qualitative Usability Evaluation of Tablets and Accessibility Settings by Older Adults. In Proceedings of the International Conference on Human-Computer Interaction, Yokohama, Japan, 8–13 May 2021; Springer: Cham, Switzerland, 2021; pp. 183–204. [Google Scholar]
- Chaudhry, B.M.; Dasgupta, D.; Chawla, N.V. Formative Evaluation of a Tablet Application to Support Goal-Oriented Care in Community-Dwelling Older Adults. In Proceedings of the ACM on Human-Computer Interaction (MHCI), New York, NY, USA, 27 May 2022; ACM: New York, NY, USA, 2022; pp. 1–21. [Google Scholar]
- Tariq, S.H.; Tumosa, N.; Chibnall, J.T.; Perry III, M.H.; Morley, J.E. Comparison of the Saint Louis University mental status examination and the mini-mental state examination for detecting dementia and mild neurocognitive disorder-a pilot study. Am. J. Geriatr. Psych 2006, 14, 900–910. [Google Scholar] [CrossRef] [PubMed]
- Thiese, M.S. Observational and interventional study design types; an overview. Biochem. Med. 2014, 24, 199–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, S.R. Clinical trial structures. J. Exp. Stroke Transl. Med. 2010, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Chaudhry, B.; Dasgupta, D.; Mohamed, M.; Chawla, N. Teaching Tablet Technology to Older Adults. In Proceedings of the International Conference on Human-Computer Interaction, Yokohama, Japan, 8–13 May 2021; Springer: Cham, Switzerland, 2021; pp. 168–182. [Google Scholar]
- King, A.C. Theory’s role in shaping behavioral health research for population health. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Prestwich, A.; Sniehotta, F.F.; Whittington, C.; Dombrowski, S.U.; Rogers, L.; Michie, S. Does theory influence the effectiveness of health behavior interventions? Meta-analysis. Health Psychol. 2014, 33, 465. [Google Scholar] [CrossRef]
- Strecher, V.J.; Seijts, G.H.; Kok, G.J.; Latham, G.P.; Glasgow, R.; DeVellis, B.; Meertens, R.M.; Bulger, D.W. Goal setting as a strategy for health behavior change. Health Educ. Q. 1995, 22, 190–200. [Google Scholar] [CrossRef]
- Shilts, M.K.; Horowitz, M.; Townsend, M.S. Goal setting as a strategy for dietary and physical activity behavior change: A review of the literature. Am. J. Health Promot. 2004, 19, 81–93. [Google Scholar] [CrossRef]
- Munson, S.A.; Consolvo, S. Exploring goal-setting, rewards, self-monitoring, and sharing to motivate physical activity. In Proceedings of the 2012 6th International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth), San Diego, CA, USA, 21–24 May 2012; pp. 25–32. [Google Scholar]
- Fissler, P.; Küster, O.C.; Laptinskaya, D.; Loy, L.S.; von Arnim, C.A.F.; Kolassa, I.T. Jigsaw Puzzling Taps Multiple Cognitive Abilities and Is a Potential Protective Factor for Cognitive Aging. Front. Aging Neurosci. 2018, 10, 299. [Google Scholar] [CrossRef] [PubMed]
- Thompson, O.; Barrett, S.; Patterson, C.; Craig, D. Examining the neurocognitive validity of commercially available, smartphone-based puzzle games. Psychology 2012, 3, 525–526. [Google Scholar] [CrossRef] [Green Version]
- Altschul, D.M.; Deary, I.J. Playing analog games is associated with reduced declines in cognitive function: A 68-year longitudinal cohort study. J. Gerontol. Ser. B 2020, 75, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.Y.; Huang, Y.M.; Yeh, Y.Y. Let’s play cards: Multi-component cognitive training with social engagement enhances executive control in older adults. Front. Psychol. 2018, 9, 2482. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, N.; Owen, A.; Mohan, A.; Corbett, A.; Ballard, C. Associations between cognitively stimulating leisure activities, cognitive function and age-related cognitive decline. Int. J. Geriatr. Psychiatry 2015, 30, 422–430. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [Green Version]
- Wong, G. SF-12 and SF-36 Health Survey. In Encyclopedia of Gerontology and Population Aging; Springer: Cham, Switzerland, 2022; pp. 4490–4493. [Google Scholar]
- van der Meulen, M.; Zamanipoor Najafabadi, A.H.; Lobatto, D.J.; Andela, C.D.; Vliet Vlieland, T.P.; Pereira, A.M.; van Furth, W.R.; Biermasz, N.R. SF-12 or SF-36 in pituitary disease? Toward concise and comprehensive patient-reported outcomes measurements. Endocrine 2020, 70, 123–133. [Google Scholar] [CrossRef]
- Frieling, M.A.; Davis, W.R.; Chiang, G. The SF-36v2 and SF-12v2 health surveys in New Zealand: Norms, scoring coefficients and cross-country comparisons. Aust. N. Z. J. Public Health 2013, 37, 24–31. [Google Scholar] [CrossRef]
- Fitzsimmons, D.; Johnson, C.; George, S.; Payne, S.; Sandberg, A.A.; Bassi, C.; Beger, H.; Birk, D.; Büchler, M.; Dervenis, C.; et al. Development of a disease specific quality of life (QoL) questionnaire module to supplement the EORTC core cancer QoL questionnaire, the QLQ-C30 in patients with pancreatic cancer. Eur. J. Cancer 1999, 35, 939–941. [Google Scholar] [CrossRef]
- Broadhead, W.; Gehlbach, S.H.; De Gruy, F.V.; Kaplan, B.H. The Duke-UNC Functional Social Support Questionnaire: Measurement of social support in family medicine patients. Med. Care 1988, 26, 709–723. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A.; Gabriel, Z. Lay theories of quality of life in older age. Ageing Soc. 2007, 27, 827–848. [Google Scholar] [CrossRef] [Green Version]
- Milte, C.M.; Walker, R.; Luszcz, M.A.; Lancsar, E.; Kaambwa, B.; Ratcliffe, J. How important is health status in defining quality of life for older people? An exploratory study of the views of older South Australians. Appl. Health Econ. Health Policy 2014, 12, 73–84. [Google Scholar] [CrossRef]
- Liu, H.; Hays, R.D.; Adams, J.L.; Chen, W.P.; Tisnado, D.; Mangione, C.M.; Damberg, C.L.; Kahn, K.L. Imputation of SF-12 health scores for respondents with partially missing data. Health Serv. Res. 2005, 40, 905–922. [Google Scholar] [CrossRef]
- Lam, F.; Longnecker, M. A modified Wilcoxon rank sum test for paired data. Biometrika 1983, 70, 510–513. [Google Scholar] [CrossRef]
- Ware, J.; Kosinski, M.; Keller, S. SF-12: How to Score the SF-12 Physical and Mental Summary Scales; New England Medical Center, The Health Institute: Boston, MA, USA, 1995. [Google Scholar]
- Silveira, P.; van Het Reve, E.; Daniel, F.; Casati, F.; de Bruin, E.D. Motivating and assisting physical exercise in independently living older adults: A pilot study. Int. J. Med Inform. 2013, 82, 325–334. [Google Scholar] [CrossRef] [Green Version]
- Crandall, K.; Shake, M. A Mobile Application for Improving Functional Performance and Health Education in Older Adults: A Pilot Study. Aging Sci. 2016, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Bickmore, T.W.; Silliman, R.A.; Nelson, K.; Cheng, D.M.; Winter, M.; Henault, L.; Paasche-Orlow, M.K. A randomized controlled trial of an automated exercise coach for older adults. J. Am. Geriatr. Soc. 2013, 61, 1676–1683. [Google Scholar] [CrossRef]
- Ware, J.; Turner-Bowker, D.; Kosinski, M.; Gandek, B. SF12v2 Health Survey User’s Manual; QualityMetric, Inc.: Lincoln, RI, USA, 2002. [Google Scholar]
- Choi, M.; Kong, S.; Jung, D. Computer and internet interventions for loneliness and depression in older adults: A meta-analysis. Healthc. Inform. Res. 2012, 18, 191–198. [Google Scholar] [CrossRef]
- Elliot, A.J.; Mooney, C.J.; Douthit, K.Z.; Lynch, M.F. Predictors of older adults’ technology use and its relationship to depressive symptoms and well-being. J. Gerontol. Ser. Psychol. Sci. Soc. Sci. 2014, 69, 667–677. [Google Scholar] [CrossRef]
- Kobayashi, M.; Hiyama, A.; Miura, T.; Asakawa, C.; Hirose, M.; Ifukube, T. Elderly user evaluation of mobile touchscreen interactions. In Human-Computer Interaction–INTERACT 2011; Springer: Berlin/Heidelberg, Germany, 2011; pp. 83–99. [Google Scholar]
- Yerrakalva, D.; Yerrakalva, D.; Hajna, S.; Griffin, S. Effects of mobile health app interventions on sedentary time, physical activity, and fitness in older adults: Systematic review and meta-analysis. J. Med. Internet Res. 2019, 21, e14343. [Google Scholar] [CrossRef] [PubMed]
- Ramprasad, C.; Tamariz, L.; Garcia-Barcena, J.; Nemeth, Z.; Palacio, A. The use of tablet technology by older adults in health care settings—Is it effective and satisfying? a systematic review and meta analysis. Clin. Gerontol. 2019, 42, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Van Der Heide, I.; Wang, J.; Droomers, M.; Spreeuwenberg, P.; Rademakers, J.; Uiters, E. The relationship between health, education, and health literacy: Results from the Dutch Adult Literacy and Life Skills Survey. J. Health Commun. 2013, 18, 172–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakshminarayana, R.; Wang, D.; Burn, D.; Chaudhuri, K.R.; Galtrey, C.; Guzman, N.V.; Hellman, B.; James, B.; Pal, S.; Stamford, J.; et al. Using a smartphone-based self-management platform to support medication adherence and clinical consultation in Parkinson’s disease. NPJ Parkinson’s Dis. 2017, 3, 1–10. [Google Scholar]
- Marcum, Z.A.; Hanlon, J.T.; Murray, M.D. Improving medication adherence and health outcomes in older adults: An evidence-based review of randomized controlled trials. Drugs Aging 2017, 34, 191–201. [Google Scholar] [CrossRef]
- Fox, S.; Duggan, M. Tracking for Health; Pew Research Center’s Internet & American Life Project: Washington, DC, USA, 2013. [Google Scholar]
- Hopkins, R.O.; Suchyta, M.R.; Kamdar, B.B.; Darowski, E.; Jackson, J.C.; Needham, D.M. Instrumental activities of daily living after critical illness: A systematic review. Ann. Am. Thorac. Soc. 2017, 14, 1332–1343. [Google Scholar] [CrossRef]
- Chan, M.; Haber, S.; Drew, L.; Park, D. Training Older Adults to Use Tablet Computers: Does It Enhance Cognitive Function? Gerontology 2016, 56, 475–484. [Google Scholar] [CrossRef] [Green Version]
- Vaportzis, E.; Martin, M.; Gow, A.J. A tablet for healthy ageing: The effect of a tablet computer training intervention on cognitive abilities in older adults. Am. J. Geriatr. Psychiatry 2017, 25, 841–851. [Google Scholar] [CrossRef] [Green Version]
- Kolotkin, R.L.; Crosby, R.D.; and Williams, G.R. Integrating anchor-based and distribution-based methods to determine clinically meaningful change in obesity-specific quality of life. Qual. Life Res. 2002, 11, 670. [Google Scholar]
- Czaja, S.; Charness, N.; Fisk, A.; Hertzog, C.; Nair, S.; Rogers, W.; Sharit, J. Factors predicting the use of technology: Findings from the Center for Research and Education on Aging and Technology Enhancement (CREATE). Psychol. Aging 2006, 21, 333. [Google Scholar] [CrossRef] [Green Version]
- Linde, L.; Sørensen, J.; stergaard, M.; Hørslev-Petersen, K.; Rasmussen, C.; Jensen, D.V.; Hetland, M.L. What factors influence the health status of patients with rheumatoid arthritis measured by the SF-12v2 Health Survey and the Health Assessment Questionnaire? J. Rheumatol. 2009, 36, 2183–2189. [Google Scholar] [CrossRef] [PubMed]
- Shah, C.H.; Brown, J.D. Reliability and validity of the short-form 12 item version 2 (SF- 12v2) health-related quality of life survey and disutilities associated with relevant conditions in the US older adult population. J. Clin. Med. 2020, 9, 661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, M. Resilience in older adults living in rural, suburban, and urban areas. Online J. Rural. Nurs. Health Care 2010, 10, 45–54. [Google Scholar] [CrossRef]
- Joly, F.; Kosinski, M.; Shafer, F.; Wardecki, M.; Karaouni, A.; Hill, Q. Clinically important change in SF-12v2 physical (PCS) and mental (MCS) component summary scores for patients with cold agglutinin disease: An analysis using the phase 3 CARDINAL and CADENZA studies. Blood 2021, 138, 2002. [Google Scholar] [CrossRef]
- D’Haeseleer, I.; Gerling, K.; Schreurs, D.; Vanrumste, B.; Vanden Abeele, V. Ageing is Not a Disease: Pitfalls for the Acceptance of Self-Management Health Systems Supporting Healthy Ageing. In Proceedings of the 21st International ACM SIGACCESS Conference on Computers and Accessibility, Pittsburgh, PA, USA, 28–30 October 2019; pp. 286–298. [Google Scholar]
- Madjaroff, G.; Mentis, H.; Ronch, J. Differences in Perceived Impact of Person-Centered Technology on Older Adults’ Quality of Life. In Proceedings of the 2016 CHI Conference Extended Abstracts on Human Factors in Computing Systems, San Jose, CA, USA, 7–12 May 2016; pp. 2200–2208. [Google Scholar]
- Boniface, M. The CrowdHEALTH project and the holistic health records: Collective wisdom driving public health policies. Acta Inform. Medica 2019, 27, 369–373. [Google Scholar]
- Mavrogiorgou, A.; Kleftakis, S.; Mavrogiorgos, K.; Zafeiropoulos, N.; Menychtas, A.; Kiourtis, A.; Maglogiannis, I.; Kyriazis, D. beHEALTHIER: A microservices platform for analyzing and exploiting healthcare data. In Proceedings of the 2021 IEEE 34th International Symposium on Computer-Based Medical Systems (CBMS), Aveiro, Portugal, 7–9 June 2021; pp. 283–288. [Google Scholar]
- James, D. Factors influencing food choices, dietary intake, and nutrition-related attitudes among African Americans: Application of a culturally sensitive model. Ethn. Health 2004, 9, 349–367. [Google Scholar] [CrossRef]
- Baptiste-Roberts, K.; Gary, T.L.; Beckles, G.L.; Gregg, E.W.; Owens, M.; Porterfield, D.; Engelgau, M.M. Family history of diabetes, awareness of risk factors, and health behaviors among African Americans. Am. J. Public Health 2007, 97, 907–912. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Workshop No. | Workshop Topic | Total Times |
|---|---|---|
| 1 | Tablet basics (hardware buttons, tablet settings, etc.) | 2 |
| 2 | Tablet apps (calendar, reminders, weather, etc.) | 2 |
| 3 | eSeniorCare App | 2 |
| 4 | Communication apps (Gmail, Skype, Facebook) | 2 |
| 5 | Gaming apps (shape, image and word puzzles) | 4 |
| PID | Age (Years) | Gender | Education (Years) | Race | Income | Alone? |
|---|---|---|---|---|---|---|
| P74 | 65 | Female | 12 | AA | 0–$10 K | Yes |
| P76 | 62 | Female | 14 | AA | 10–$20 K | Yes |
| P80 | 72 | Female | 12 | AA | 10–$20 K | No |
| P82 | 58 | Female | 14 | AA | 0–$10 K | Yes |
| P83 | 69 | Male | 8 | AA | 0–$10 K | Yes |
| P85 | 64 | Female | 14 | AA | 10–$20 K | Yes |
| P88 | 72 | Male | 12 | AA | 0–$10 K | No |
| P89 | 61 | Male | 14 | AA | 10–$20 K | Yes |
| P91 | 66 | Male | 8 | WC | 20–$30 K | Yes |
| P93 | 60 | Male | 14 | AA | 0–$10 K | Yes |
| P94 | 59 | Female | 16 | AA | 0–$10 K | Yes |
| P95 | 56 | Female | 14 | AA | 0–$10 K | Yes |
| P96 | 64 | Male | 14 | AA | 10–$20 K | Yes |
| P98 | 66 | Female | 14 | AA | 0–$10 K | Yes |
| P99 | 72 | Female | 14 | AA | 0–$10 K | No |
| P100 | 64 | Female | 14.5 | AA | 0–$10 K | No |
| P101 | 57 | Female | 13 | AA | 0–$10 K | Yes |
| P102 | 79 | Male | 12 | AA | 0–$10 K | Yes |
| P107 | 75 | Female | 8 | AA | 0–$10 K | Yes |
| P108 | 83 | Female | 10 | AA | 0–$10 K | Yes |
| P110 | 65 | Male | 13.5 | ME | 0–$10 K | No |
| P115 | 73 | Male | 8 | AA | 0–$10 K | Yes |
| P131 | 61 | Male | 14 | AA | 0–$10 K | Yes |
| P133 | 59 | Female | 13 | WC | 0–$10 K | Yes |
| P189 | 61 | Male | 11 | AA | 0–$10 K | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaudhry, B.M.; Dasgupta, D.; Chawla, N.V. Successful Aging for Community-Dwelling Older Adults: An Experimental Study with a Tablet App. Int. J. Environ. Res. Public Health 2022, 19, 13148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192013148
Chaudhry BM, Dasgupta D, Chawla NV. Successful Aging for Community-Dwelling Older Adults: An Experimental Study with a Tablet App. International Journal of Environmental Research and Public Health. 2022; 19(20):13148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192013148
Chicago/Turabian StyleChaudhry, Beenish Moalla, Dipanwita Dasgupta, and Nitesh V. Chawla. 2022. "Successful Aging for Community-Dwelling Older Adults: An Experimental Study with a Tablet App" International Journal of Environmental Research and Public Health 19, no. 20: 13148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192013148