
Canada First Nations Strengths in Community-Based Primary Healthcare
 ,
, {kind=link}
Abstract
:1. Introduction
Background
2. Methods
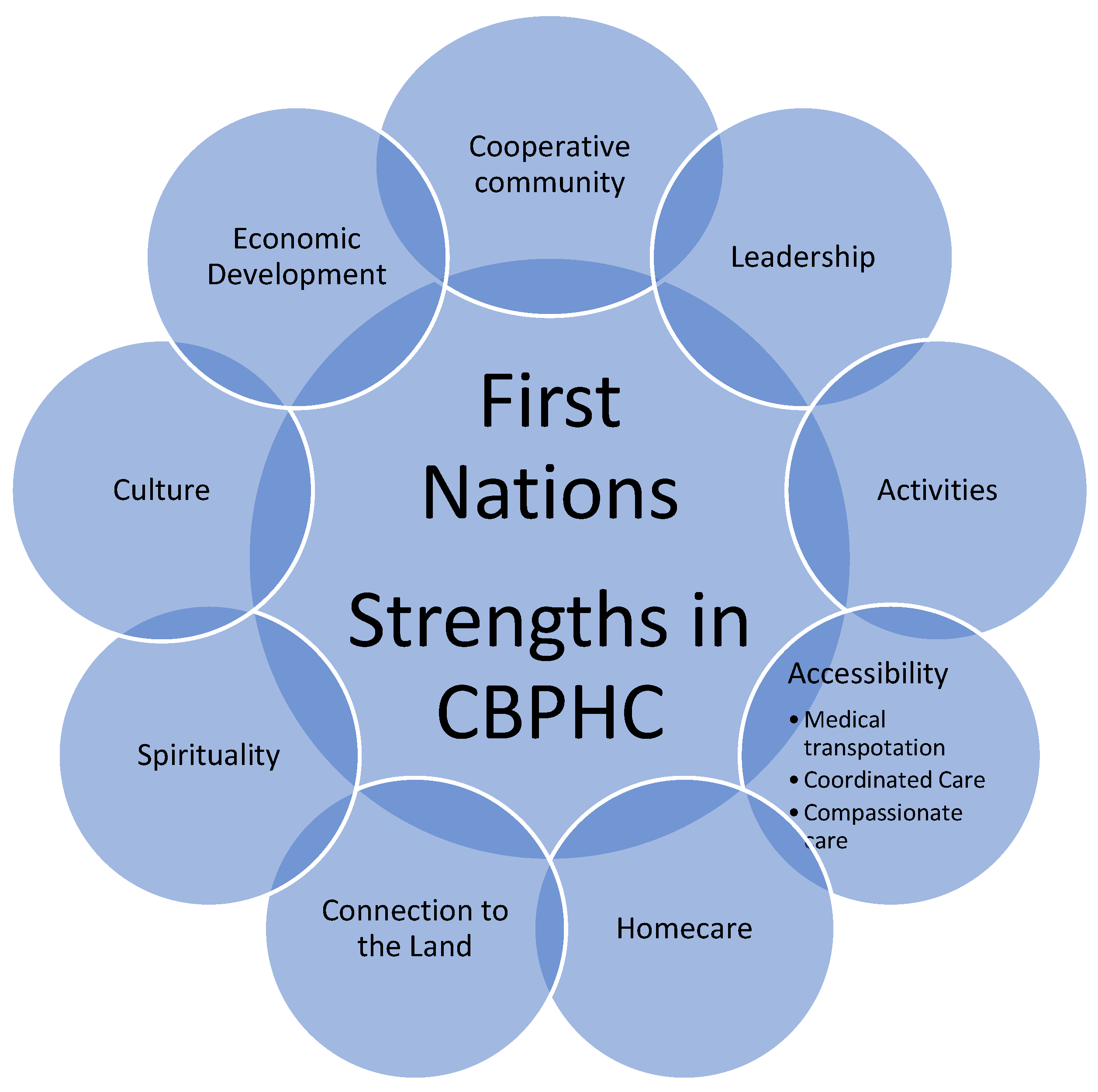
3. Findings
3.1. Cooperative Community
I think that the strengths of the community reside within the people themselves. There is this thing that they have—resilience. There is a resilience that people have in this community that no matter the circumstances they get back on their feet and they don’t let life’s circumstances take them way down…—I see that as a strength. And they see support for each other when the need is there.(F006)
I guess everybody sees this like our community is different from others. It seems that in our community there is always people that are willing to help each other. We have an abundance of help that comes from people. Like say if there’s a death, everybody wants to help. If somebody is in trouble, accidents, people come. People come together and they help.(C007)
[Our] community has a high population of youth and I think having the youth in the community that is a strength…we’re actually learning from the youth. And it goes hand in hand. Youth learn from Elders and Elders learn from youth. And by Elders and youth working together in the community that’s a strength. You know, coming together and sharing their knowledge and providing that support to one another. I find that’s a big strength.(D005)
3.2. Leadership
What I found is that the health leadership is trying very hard to help our First Nation. That’s what I find unique about our community. They’re trying to help First Nations [people] from 0 to 100 years old, in any possible way. The services are there; people aren’t scared to use them. That’s what I find unique.(B017)
3.3. Activities in the Community
You know, it’s unique to have a community like that that’s got lots of land, land to use, lots of water to use. I find that unique because a lot of [other] communities don’t have that. I lived [off reserve] for a long time there and a lot of people look for a place to go swim over there in other places. Like they look for places to go camping but there’s lots of rules, you know, when you go camping. But here you can go anywhere, anywhere in the bush here to go camp. You know, it’s unique like that that we can use the land pretty much and not ask anyone to use the land. We don’t have to go ask for a permit or things like that. I see that as unique and it’s good to have that.(C011)
Lots of events always taking place… this winter they were showing them [kids] ice fishing, how they hunt and trapping, how to make traps and …I know my uncle said that they asked him to do some teachings. Like that’s another thing too is he said he goes down there, and they gather, and some families want to know their history. So, he sits there and tells them who they’re related to and tells them their history. That’s another thing they do down there, it’s kind of like a gathering place for different events like I said…a community-gathering place for our people. And everybody camps and it’s really good and it’s growing. I know they have more things that are being added on. Like the big event they have is the country days, big country singers they bring out and that’s good. And then they have our radio station which is another good thing and that probably will even get bigger. Maybe they’ll even get a television station here. We have a lot of good things, I’m proud.(D002)
Our traditions are still alive. There’s still caribou hunting, they are still dry meat making, there’s still people fishing. Beadwork, you still see it. And we have a sense of pride when we see that. Even our language, when we talk and nobody else understands and there’s two of us speaking our language, there’s pride in that. That is a good strength.(FFG1-1)
3.4. Positive Experiences with Community-Based Healthcare System
3.4.1. Accessibility—Medical Transportation
The only difference [with off-reserve] would be that the medical, we have medical transportation, like, even for the young. I guess off the reserve just the old folks have it I guess. We got it for everybody. Even for guys that have vehicles, they still get on the bus, don’t they?(E009)
A lot of things are getting to be a better… now I’m older they come to my home, which is just nice, instead of us going to the nursing station. Then, at that time, we didn’t have no transportation to go to the nursing station, and we used to walk. Now we have a medical van transporting us to and from.(GFG004-3)
Providing rides for people that [don’t have any] so they can come see the doctor or the nurse or the dentist or anything is a good idea. And maybe increasing the number of vans so people can access our resources would be wonderful.(H005)
3.4.2. Coordinated Care
Well, I mean I think we’re lucky I would say because if you go to an emergency in Winnipeg how long do you sit there and this is nothing compared to being in the city. Like you have a nurse here or even have a doctor here sometimes, but I think we’re lucky. It’s just that what I said before about the nurses, they have more compassion for their job.(C014)
I would think just faster service… I would say on the reserve you get pretty good service too, yeah. Anytime I needed help or my daughter or any of my kids needed something, I phone here, they set it up, they let me know “Okay, we got you in this time for this time,” and all that. I don’t got to worry about it but off the reserve I would be worried. Oh, I appreciate it.(E006)
3.4.3. Compassionate Care
We have some really good workers here that are dedicated to their jobs, and they try to help as best they could to help take care of the person at the time of need, and refer on, if need be.(E016)
I think maybe that’s the difference. And they’re more, cause I think maybe too they know you here, they’re more, they have that caring, you know, caring part. But I think community D is actually up there, like they’re careful.(D002)
There again, they say we have to have certificates of all kinds in order to provide the good care we need. I think we have our own resources here for people-, caring people. I’ve seen one family provide palliative care very good to a relative of mine. Some people feel better with community people.(E010)
3.4.4. Homecare
Well, the services I guess would be, like if there had to be a difference to off reserve people, is probably homecare because we don’t offer homecare to off reserve provincial.(B003)
Well, I think that homecare is important for the benefit of the Elders and residents who need healthcare at home and get healthcare. It’s something that’s really important.(D003)
I think on a couple of occasions already I’ve had personal service provided to me from the health centre when I had an operation. I had a nurse come in and change the dressing on my surgery wound, also when I had an operation on my chest the second time. I had my foot and part of my leg amputated. I was looked after by the health nurse.(H020)
3.4.5. Connection to the Land
That would be it there, I think. More into the land, it’s the land that binds us. It’s the land that defines the Native person; it’s in our blood. Like I said, I don’t understand. I tried to look at it and say, “Why is this? Why is that?” I’ve missed so much growing up-, not really growing up here. The old people have come and gone, some of the old people I have talked… you sense that, you sense the attachment to the land. I raised my kids on the trap line, I taught them from the trap line. My Dad even told me that’s how we began. He was raised at the trap line. Blood was in the land and land was in his blood.(A007)
Nice looking lawns, families helping families, in general, like a good family relationship, a good healthy family relationship.(B017)
We’re proud of getting gardens and trying to go back to the old ways where it was—I know it was harder but it was actually better…I think too about the kids, they’re getting so obese you know and it’s because we wanted to make life easier like you know but easier ain’t always best.(CFG2-4)
Natural foods and I know when you think of the Elders, they kind of live like a long life because they lived off the land and they worked really hard and they had a lot of physical activity. Because like myself as a little girl, we went to pick berries, you know, according to the seasons. We still pick the berries. And I think like you’re canning, you’re preserving and there’s a lot of … there’s that cultural part of a way of life. Yeah and … whereas today we’re at a stage where we want to embrace that cultural life again because we know it was a good life and it was a healthy way of living within the community. That’s the best way to explain it but you know what I mean.(D005)
I think the uniqueness of the community here is the land we live in and how we use our environment…I believe your surroundings around you have a lot to do with the way you live and your health. [The] environment you put yourself in or how you take care of your environment. I believe that’s a big thing, keeping it clean, and healthy as well.(E016)
3.4.6. Spirituality
They have these people that seek traditional healing and traditional help and they know the history of it. Before I came into this community, it was more focused on Christians, but I can see now there is more open [traditional practice] now, they’ve accepted the people. They’ve begun to accept it and it’s starting to be open to people. The people who carry the traditional healing and light, they’re out there. You can find them if you need something from them. You know who to go to get advice but maybe 20, 30 years ago you weren’t, you couldn’t, you know? That’s something positive to me is that we have options. Yeah, their strength is that when the people seek for help, they’re able to get it; we have different options. We can see children following that too. They want to learn how to dance and how to make drums and that.(A014)
In this community, there is currently seven healing and sweat lodges present. And I think all the community members who follow this way of life would you know, live a balanced life. We call it the Red Road. Spiritual Elders take your inner child and work their way out toward an adult, to bring everything out that has happened in the past, so you can live a balanced life, whether it was abuse or alcohol or there’s a number of abuses that could be said. That’s my strength is when I go into a sweat lodge, is the same thing as a healing lodge for me. The Red Road… it’s you know trying to live that balanced life, the seven teachings that the creator had given us to follow. The [FN] communities that I’ve gone to, there is a healing lodge that exists in the community and there’s always a Spiritual Elder that comes from that community. And I guess that’s the strength of our communities.(B021)
3.4.7. Culture
Yeah, that would be one here because I know even when I had my own experience with a funeral, I had relatives come out of town. And they couldn’t believe how everybody helped out and how they have the and how they did that, and you know, and how they thought of that, and how everybody come and shook everybody’s hand, they thought that was really different. They’d never seen that. They liked that.(A008)
Workers here all practice their culture. They dance, they sing and [one of them] was a sweat lodge keeper. We have a lot of women that work in here… They’re all grandmothers and mothers and they all still speak their Ojibway language, which is an asset both to work with the older people and for the younger people. [Our] language is still here and I think that’s unique in our community because I know our younger generation don’t speak the language but all our older generations speak the language. They’re speaking to the community so we still have that in our health center and I think that makes us unique.(B005)
Our community has traditions. By traditions, I mean things that people did together. People, you know, fish together, the helping of one another; you need people to help each other. People help with raising their children. I know my grandmother and her sisters were like the people that could correct you. My dad’s sisters, my aunts, they could correct you and my dad wouldn’t say nothing, my mom wouldn’t say nothing. [They’d say] good, it’s good you corrected my children; go ahead, because if they’re doing something they shouldn’t be doing then good, you correct them. People took their kids to church in the morning, took them in the afternoon, whenever they went and it was good. The kid knew, the child knew to respect people and also how to pray. Also, when I’d see an old person like we’d pass an older person and my grandma would say, “Say hi to your grandma” and I’d look confused at first, then I got the hang of it. Oh, yes, okay. Every old person you met, whether it was a man or a woman, if it was a woman that was your grandma and grandpa the other one, you know? You have to call them that. You couldn’t call them by their name and same with your parents, you wouldn’t call them by their name. We were taught to respect all Elders in the community and then in the community it was fun. You’d meet somebody, you said hi, you talked to them and then my grandmother and I would stand there and never get tired but I knew I’d have to stand there while she chatted with somebody, you know? And stuff like that. That’s what made it unique for me, unique community.(C010)
The strength, I think, each different community has their own strengths within the people. We recently started a culture camp, which is a good thing to be starting, things where people could learn. Strengths, here there’s traditional medicines in the community that are being used and utilizing the western medications, as well.(E016)
3.4.8. Economic Development
Some of us are good at stuff you know what I mean. They just don’t give us a chance. I had a hard time finding a job in Winnipeg.(CFG102)
Right now I think it is work… a lot of jobs being provided… And our strength, our health is getting better. I think health is getting better. I see more guys working more people don’t have to leave the reserve for that. …Lots of housing… I’m kind of proud of that, that we’re doing this, doing it for ourselves this time around. For the first time, I find it unique right now is that we’re doing it ourselves, showing we can do it ourselves.(E006)
They’ve got the sewing program and they do arts and crafts, and they have that case displayed out there for them to sell crafts, I really like that.(GFG004-4)
4. Discussion
5. Strengths and Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freemantle, J.; Ring, I.; Solomon, T.G.A.; Gachupin, F.C.; Smylie, J.; Cutler, T.L.; Waldon, J.A. Indigenous Mortality (Revealed): The Invisible Illuminated. Am. J. Public Health 2015, 105, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Frohlich, K.L.; Ross, N.; Richmond, C. Health disparities in Canada today: Some evidence and a theoretical framework. Health Policy 2006, 79, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Gone, J.P.; Hartmann, W.E.; Pomerville, A.; Wendt, D.C.; Klem, S.H.; Burrage, R.L. The impact of historical trauma on health outcomes for indigenous populations in the USA and Canada: A systematic review. Am. Psychol. 2019, 74, 20–35. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, M.; de Leeuw, S.; Lindsay, N. Challenges in health equity for Indigenous peoples in Canada. Lancet 2018, 391, 1645–1648. [Google Scholar] [CrossRef]
- Hajizadeh, M.; Hu, M.; Bombay, A.; Asada, Y. Socioeconomic inequalities in health among Indigenous peoples living off-reserve in Canada: Trends and determinants. Health Policy 2018, 122, 854–865. [Google Scholar] [CrossRef]
- Katz, A.; Avery Kinew, K.; Star, L.; Taylor, C.; Koseva, I.; Lavoie, J.; Burchill, C.; Urquia, M.L.; Basham, A.; Rajotte, L.J.; et al. The Health Status of and Access to healthcare by Registered First Nation Peoples in Manitoba. In Manitoba Centre for Health Policy Report in Partnership with First Nations Health and Social Secretariat of Manitoba; Manitoba Centre for Health Policy, University of Manitoba, Rady Faculty of Health Sciences: Winnipeg, MB, Canada, 2019; Available online: http://mchp-appserv.cpe.umanitoba.ca/deliverablesList.html (accessed on 10 July 2022).
- National Collaborating Centre for Aboriginal Health. The State of Knowledge of Aboriginal Health: A Review of Aboriginal Public Health in Canada. 2012. Available online: https://www.ccnsa-nccah.ca/docs/context/RPT-StateKnowledgeReview-EN.pdf (accessed on 10 July 2022).
- Daschuk, J.W. Clearing the Plains: Disease, Politics of Starvation, and the Loss of Aboriginal Life; University of Regina Press: Regina, SK, Canada, 2013. [Google Scholar]
- Greenwood, M.; DeLeeuw, S.; Lindsay, N.M. Determinants of Indigenous Peoples’ Health in Canada: Beyond the Social; Canadian Scholars’ Press Inc.: Toronto, ON, Canada, 2018; ISBN 9781773380377. [Google Scholar]
- Hackett, C.; Feeny, D.; Tompa, E. Canada’s residential school system: Measuring the intergenerational impact of familial attendance on health and mental health outcomes. J. Epidemiol. Community Health 2016, 70, 1096–1105. [Google Scholar] [CrossRef] [Green Version]
- Lux, M.K. Separate Beds: A History of Indian Hospitals in Canada, 1920s–1980s; University of Toronto Press: Toronto, ON, Canada, 2016. [Google Scholar]
- Stote, K. An Act of Genocide: Colonialism and the Sterilization of Aboriginal Women; Fernwood Publishing: Black Point, NS, Canada, 2015; Available online: https://books.google.ca/books?id=ZKPjrQEACAAJ (accessed on 16 July 2022).
- Allan, B.; Smylie, J. First Peoples, Second Class Treatment: The Role of Racism in the Health and Well-Being of Indigenous Peoples in Canada. 2015. Available online: http://www.wellesleyinstitute.com/wp-content/uploads/2015/02/Summary-First-Peoples-Second-Class-Treatment-Final.pdf (accessed on 10 July 2022).
- Lux, M.K. Care for the ‘racially careless’: Indian hospitals in the Canadian West, 1920–1950s. Can. Hist. Rev. 2010, 91, 407–434. [Google Scholar] [CrossRef]
- Barnabe, C.; Jones, C.A.; Bernatsky, S.; Peschken, C.A.; Voaklander, D.; Homik, J.; Crowshoe, L.F.; Esdaile, J.M.; El-Gabalawy, H.; Hemmelgarn, B. Inflammatory Arthritis Prevalence and Health Services Use in the First Nations and Non–First Nations Populations of Alberta, Canada. Arthritis Care Res. 2017, 69, 467–474. [Google Scholar] [CrossRef] [Green Version]
- Brownell, M.; Enns, J.E.; Hanlon-Dearman, A.; Chateau, D.; Phillips-Beck, W.; Singal, D.; MacWilliam, L.; Longstaffe, S.; Chudley, A.; Elias, B.; et al. Health, Social, Education, and Justice Outcomes of Manitoba First Nations Children Diagnosed with Fetal Alcohol Spectrum Disorder: A Population-Based Cohort Study of Linked Administrative Data. Can. J. Psychiatry 2018, 64, 611–620. [Google Scholar] [CrossRef]
- Chen, L.; Wang, W.-J.; Auger, N.; Xiao, L.; Torrie, J.; McHugh, N.G.-L.; Luo, Z.-C. Diabetes in pregnancy in associations with perinatal and postneonatal mortality in First Nations and non-Indigenous populations in Quebec, Canada: Population-based linked birth cohort study. BMJ Open 2019, 9, e025084. [Google Scholar] [CrossRef]
- Luo, Z.-C.; Wilkins, R.; Heaman, M.; Martens, P.; Smylie, J.; Hart, L.; Simonet, F.; Wassimi, S.; Wu, Y.; Fraser, W.D. Birth Outcomes and Infant Mortality by the Degree of Rural Isolation Among First Nations and Non-First Nations in Manitoba, Canada. J. Rural Health 2010, 26, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Wahi, G.; Zorzi, A.; Macnab, A.; Panagiotopoulos, C. Prevalence of type 2 diabetes, obesity and the metabolic syndrome among Canadian First Nations children in a remote Pacific coast community. Paediatr. Child Health 2009, 14, 79–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenwood, M.L.; de Leeuw, S.N. Social determinants of health and the future well-being of Aboriginal children in Canada. Paediatr. Child Health 2012, 17, 381–384. [Google Scholar] [PubMed] [Green Version]
- MMIWG. Reclaiming Power and Place: The Final Report of the National Inquiry into Missing and Murdered Indigenous Women and Girls. 2019. Available online: https://www.mmiwg-ffada.ca/final-report/ (accessed on 28 June 2022).
- Harfield, S.; Davy, C.; Kite, E.; McArthur, A.; Munn, Z.; Brown, N.; Brown, A. Characteristics of Indigenous primary health care models of service delivery: A scoping review protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Harfield, S.G.; Davy, C.; McArthur, A.; Munn, Z.; Brown, A.; Brown, N. Characteristics of Indigenous primary health care service delivery models: A systematic scoping review. Glob. Health 2018, 14, 12. [Google Scholar] [CrossRef] [Green Version]
- Phillips-Beck, W.; Eni, R.; Lavoie, J.G.; Kinew, K.A.; Achan, G.K.; Katz, A. Confronting Racism within the Canadian Healthcare System: Systemic Exclusion of First Nations from Quality and Consistent Care. Int. J. Environ. Res. Public Health 2020, 17, 8343. [Google Scholar] [CrossRef]
- Gerald Taiaiake, A. Colonialism and State Dependency. J. Aborig. Health 2009, 5, 42. [Google Scholar]
- Mitchell, T. Colonial Trauma: Complex, continuous, collective, cumulative and compounding effects on the health of Indigenous Peoples in Canada and beyond. Int. J. Indig. Health 2019, 14, 74–94. [Google Scholar] [CrossRef]
- Davy, C.; Harfield, S.; McArthur, A.; Munn, Z.; Brown, A. Access to primary health care services for Indigenous peoples: A framework synthesis. Int. J. Equity Health 2016, 15, 163. [Google Scholar] [CrossRef] [Green Version]
- Kyoon-Achan, G.; Lavoie, J.; Kinew, K.A.; Ibrahim, N.; Sinclair, S.; Katz, S.S.A.A.; Phillips-Beck, W. What Changes Would Manitoba First Nations Like to See in the Primary Healthcare They Receive? A Qualitative Investigation. Healthc. Policy 2019, 15, 85–99. [Google Scholar] [CrossRef]
- Amsler, S. Cultural Colonialism. Wiley Online Libr. 2016, 20, 12. [Google Scholar] [CrossRef]
- Eni, R.; Phillips-Beck, W.; Achan, G.K.; Lavoie, J.G.; Kinew, K.A.; Katz, A. Decolonizing health in Canada: A Manitoba first nation perspective. Int. J. Equity Health 2021, 20, 206. [Google Scholar] [CrossRef] [PubMed]
- Aquash, M. First Nations in Canada: Decolonization and Self-Determination. Education 2013, 19, 120–137. [Google Scholar] [CrossRef]
- Murdock, R. Supporting Indigenous Self-Determination in Health: Lessons Learned from a Review of Best Practices in Health Governance in Canada and Internationally, National Collaborating Centre for Indigenous Health. 2020. Available online: https://policycommons.net/artifacts/1888207/supporting-indigenous-self-determination-in-health/2638188/ (accessed on 20 September 2022).
- Okazaki, S.; David, E.J.R.; Abelmann, N. Colonialism and Psychology of Culture. Soc. Pers. Psychol. Compass 2007, 2, 90–106. [Google Scholar] [CrossRef]
- Quinless, J.M. Decolonizing Bodies: A First Nation Perspective on the Determinants of Urban Indigenous Health and Wellness in Canada. Doctoral Dissertation, University of Victoria, Victoria, BC, Canada, 2017. [Google Scholar]
- Field, M. Decolonizing Healing Through Indigenous Ways of Knowing. In Reimagining Science Education in the Anthropocene; Palgrave Studies in Education and the Environment; Wallace, M.F.G., Bazzul, J., Higgins, M., Tolbert, S., Eds.; Palgrave Macmillan: Cham, Switzerland, 2022. [Google Scholar] [CrossRef]
- Lee, B. Colonialization and community: Implications for first nations development1. Community Dev. J. 1992, 27, 211–219. [Google Scholar] [CrossRef]
- Cardinal, S.; Pepler, D. Community Journey of Change Through Relational Determinants of Health. Int. Indig. Policy J. 2021, 12, 1–16. [Google Scholar] [CrossRef]
- Corrado, R.R.; Cohen, I.M. Mental Health Profiles for a Sample of British Columbia’s Aboriginal Survivors of the Canadian Residential School System; Report Prepared for the Aboriginal Healing Foundation; Aboriginal Healing Foundation: Ottawa, ON, Canada, 2003. [Google Scholar]
- Gauthier, M. The Impact of the Residential School, Child Welfare System and Intergenerational Trauma upon the Incarceration of Aboriginals. Master’s Thesis, Queen’s University, Kingston, ON, Canada, 2010. [Google Scholar]
- Ross, A.; Dion, J.; Cantinotti, M.; Collin-Vézina, D.; Paquette, L. Impact of residential schooling and of child abuse on substance use problem in Indigenous Peoples. Addict. Behav. 2015, 51, 184–192. [Google Scholar] [CrossRef] [Green Version]
- Wilk, P.; Maltby, A.; Cooke, M. Residential schools and the effects on Indigenous health and well-being in Canada-a scoping review. Public Health Rev. 2017, 38, 8. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.J. Putting an End to the Silence: Educating Society about the Canadian Residential School System. Bridges Undergrad. J. Contemp. Connect. 2017, 2. Available online: https://scholars.wlu.ca/bridges_contemporary_connections/vol2/iss1/1 (accessed on 10 July 2022).
- Bombay, A.; Matheson, K.; Anisman, H. The intergenerational effects of Indian Residential Schools: Implications for the concept of historical trauma. Transcult. Psychiatry 2014, 51, 320–338. [Google Scholar] [CrossRef] [Green Version]
- CBC News Saskatchewan. A Year of Pain and Healing since 751 Unmarked Graves Announced at Cowessess First Nation. Available online: https://www.cbc.ca/news/canada/saskatchewan/cowessess-graves-first-anniversary-1.6495126 (accessed on 24 June 2022).
- National Post. The Year of the Graves: How the World’s Media Got It Wrong on Residential School Graves. Available online: https://nationalpost.com/opinion/the-year-of-the-graves-how-the-worlds-media-got-it-wrong-on-residential-school-graves (accessed on 26 May 2022).
- Richmond, C.A.M.; Cook, C. Creating conditions for Canadian aboriginal health equity: The promise of healthy public policy. Public Health Rev. 2016, 37, 2. [Google Scholar] [CrossRef] [PubMed]
- Ladner, K.L. Understanding the Impact of Self-Determination on Communities in Crisis. Natl. Aborig. Health Organ. J. Aborig. Health 2009, 5, 88–101. Available online: https://journals.scholarsportal.info/pdf/22919368/v05i0002/88_utiosdocic.xml (accessed on 16 July 2022).
- Kirmayer, L.; Simpson, C.; Cargo, M. Healing Traditions: Culture, Community and Mental Health Promotion with Canadian Aboriginal Peoples. Australas. Psychiatry 2003, 11, S15–S23. [Google Scholar] [CrossRef]
- Kirmayer, L.J. The cultural diversity of healing: Meaning, metaphor and mechanism. Br. Med. Bull. 2004, 69, 33–48. [Google Scholar] [CrossRef] [Green Version]
- Laderman, C. The ambiguity of symbols in the structure of healing. Soc. Sci. Med. 1987, 24, 293–301. [Google Scholar] [CrossRef]
- Riegel, B.; Moser, D.K.; Buck, H.G.; Dickson, V.V.; Dunbar, S.B.; Lee, C.S.; Lennie, T.A.; Lindenfeld, J.; Mitchell, J.E.; Treat-Jacobson, D.J.; et al. Self-Care for the Prevention and Management of Cardiovascular Disease and Stroke. J. Am. Heart Assoc. 2017, 6, e006997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menéndez, E.L. Consecuencias, visibilizaciones y negaciones de una pandemia: Los procesos de autoatención. Salud Colect. 2020, 16, e3149. [Google Scholar] [CrossRef] [PubMed]
- Coté, C. “Indigenizing” Food Sovereignty. Revitalizing Indigenous Food Practices and Ecological Knowledges in Canada and the United States. Humanities 2016, 5, 57. [Google Scholar] [CrossRef] [Green Version]
- Wastesicoot, J. A Cultural Framework for Cree Self-Government: Retracing Our Steps Back. Master’s Thesis, University of Manitoba, Winnipeg, MB, Canada, 2004. [Google Scholar]
- Barnabe, C. Towards attainment of Indigenous health through empowerment: Resetting health systems, services and provider approaches. BMJ Glob. Health 2021, 6, e004052. [Google Scholar] [CrossRef]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis; SAGE Publications: Thousand Oaks, CA, USA, 2006. [Google Scholar]
- Engward, H. Understanding grounded theory. Nurs. Stand. 2013, 28, 37–41. [Google Scholar] [CrossRef]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory; Routledge: New York, NY, USA, 2017. [Google Scholar] [CrossRef]
- Brunger, F.; Wall, D. “What Do They Really Mean by Partnerships?” Questioning the Unquestionable Good in Ethics Guidelines Promoting Community Engagement in Indigenous Health Research. Qual. Health Res. 2016, 26, 1862–1877. [Google Scholar] [CrossRef] [PubMed]
- Canadian Institutes of Health Research. CIHR Guidelines for Health Research Involving Aboriginal People (2007–2010). 2010. Available online: http://www.cihr-irsc.gc.ca/e/29134.html (accessed on 10 July 2022).
- Boffa, J.; King, M.; McMullin, K.; Long, R. A process for the inclusion of Aboriginal People in health research: Lessons from the Determinants of TB Transmission project. Soc. Sci. Med. 2011, 72, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Flicker, S.; O’Campo, P.; Monchalin, R.; Thistle, J.; Worthington, C.; Masching, R.; Guta, A.; Pooyak, S.; Whitebird, W.; Thomas, C. Research Done in “A Good Way”: The Importance of Indigenous Elder Involvement in HIV Community-Based Research. Am. J. Public Health 2015, 105, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- Kyoon-Achan, G.; Lavoie, J.; Kinew, K.A.; Phillips-Beck, W.; Ibrahim, N.; Sinclair, S.; Katz, A. Innovating for Transformation in First Nations Health Using Community-Based Participatory Research. Qual. Health Res. 2018, 28, 1036–1049. [Google Scholar] [CrossRef] [PubMed]
- Phillips-Beck, W.; Kyoon-Achan, G.; Lavoie, J.G.; Krueger, N.; Kinew, K.A.; Sinclair, S.; Ibrahim, N.; Katz, A. Negotiation, Reciprocity, and Reality: The Experience of Collaboration in a Community-Based Primary Health Care (CBPHC) Program of Research with Eight Manitoba First Nations. Int. Indig. Policy J. 2020, 10. [Google Scholar] [CrossRef]
- Chilisa, B. Indigenous Research Methodologies; SAGE Publications: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Kovach, M. Conversational Method in Indigenous Research. First Peoples Child Fam. Rev. 2010, 5, 40–48. Available online: https://fncaringsociety.com/sites/default/files/online-journal/vol5num1/Kovach_pp40.pdf (accessed on 10 July 2022). [CrossRef]
- National Aboriginal Health Organization. OCAP: Ownership, Control, Access and Possession; First Nations Centre, National Aboriginal Health Organization: Ottawa, ON, Canada, 2007; ISBN 9780978078584. [Google Scholar]
- Miles, M.; Huberman, A.M. Qualitative Data Analysis: An Expanded Sourcebook, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Jernigan, V.B.B.; D’Amico, E.J.; Kaholokula, J.K. Prevention Research with Indigenous Communities to Expedite Dissemination and Implementation Efforts. Prev. Sci. 2018, 21, 74–82. [Google Scholar] [CrossRef]
- Haggerty, J.; Chin, M.H.; Katz, A.; Young, K.; Foley, J.; Groulx, A.; Pérez-Stable, E.J.; Turnbull, J.; DeVoe, J.E.; Uchendu, U.S. Proactive Strategies to Address Health Equity and Disparities: Recommendations from a Bi-National Symposium. J. Am. Board Fam. Med. 2018, 31, 479–483. [Google Scholar] [CrossRef] [Green Version]
- Cook, C.; MacKinnon, M.; Anderson, M.; Whetter, I. Structures last longer than intentions: Creation of Ongomiizwin—Indigenous Institute of Health and Healing at the University of Manitoba. Int. J. Circumpolar Health 2019, 78, 1571381. [Google Scholar] [CrossRef] [Green Version]
- Lavoie, J.G.; Kornelsen, D.; Wylie, L.; Mignone, J.; Dwyer, J.; Boyer, Y.; Boulton, A.; O’Donnell, K. Responding to health inequities: Indigenous health system innovations. Glob. Health Epidemiol. Genom. 2016, 1, e14. [Google Scholar] [CrossRef]
- Gallagher, J. Indigenous approaches to health and wellness leadership: A BC First Nations perspective. Health Manag. Forum 2019, 32, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Kenny, C. Liberating Leadership Theory; Kenny, C., Fraser, T.N., Eds.; Native Narratives on Building Strong Communities, UBC Press: Vancouver, BC, Canada, 2012; pp. 1–14. [Google Scholar]
- Gottlieb, K. The Nuka System of Care: Improving health through ownership and relationships. Int. J. Circumpolar Health 2013, 72, 21118. [Google Scholar] [CrossRef] [PubMed]
- Harris, S.B.; Tompkins, J.W.; TeHiwi, B. Call to action: A new path for improving diabetes care for Indigenous peoples, a global review. Diabetes Res. Clin. Pr. 2015, 123, 120–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavoie, J.G.; Kaufert, J.M.; Browne, A.J.; Mah, S.; O’Neil, J.D. Negotiating Barriers, Navigating the Maze: First Nation Peoples’ Experience of Medical Relocation; Canadian Public Administration: Ottawa, ON, Canada, 2015; Volume 58. [Google Scholar]
- Redvers, J. “The land is a healer”: Perspectives on land-based healing from Indigenous practitioners in northern Canada. Int. J. Indig. Health 2020, 15, 90–107. [Google Scholar] [CrossRef]
- Venugopal, J.; Ninomiya, M.E.M.; Green, N.T.; Peach, L.; Linklater, R.; George, P.N.; Wells, S. A scoping review of evaluated Indigenous community-based mental wellness initiatives. Rural Remote Health 2021, 21, 6203. [Google Scholar] [CrossRef]
- Lines, L.-A.; Yellowknives Dene First Nation Wellness Division; Jardine, C.G. Connection to the land as a youth-identified social determinant of Indigenous Peoples’ health. BMC Public Health 2019, 19, 176. [Google Scholar] [CrossRef]
- Brown, H.J.; McPherson, G.; Peterson, R.; Newman, V.; Cranmer, B. Our land, our language: Connecting dispossession and health equity in an indigenous context. Can. J. Nurs. Res. 2012, 44, 44–63. [Google Scholar]
- Kryzanowski, J.A.; McIntyre, L. A Holistic Model for the Selection of Environmental Assessment Indicators to Assess the Impact of Industrialization on Indigenous Health. Can. J. Public Health 2011, 102, 112–117. [Google Scholar] [CrossRef]
- Bethune, R.; Absher, N.; Obiagwu, M.; Qarmout, T.; Steeves, M.; Yaghoubi, M.; Tikoo, R.; Szafron, M.; Dell, C.; Farag, M. Social determinants of self-reported health for Canada’s indigenous peoples: A public health approach. Public Health 2018, 176, 172–180. [Google Scholar] [CrossRef]
- Wien, F.; Denis, J.; Dockstator, J.S.; Dockstator, M.S.; Duhaime, G.; Loppie, C.; Loxley, J.; Moore, C.; Newhouse, D.; Weir, W.; et al. First Nation paths to well-being: Lessons from the Poverty Action Research Project. Glob. Health Promot. 2019, 26, 6–16. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyoon Achan, G.; Eni, R.; Phillips-Beck, W.; Lavoie, J.G.; Kinew, K.A.; Katz, A. Canada First Nations Strengths in Community-Based Primary Healthcare. Int. J. Environ. Res. Public Health 2022, 19, 13532. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192013532
Kyoon Achan G, Eni R, Phillips-Beck W, Lavoie JG, Kinew KA, Katz A. Canada First Nations Strengths in Community-Based Primary Healthcare. International Journal of Environmental Research and Public Health. 2022; 19(20):13532. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192013532
Chicago/Turabian StyleKyoon Achan, Grace, Rachel Eni, Wanda Phillips-Beck, Josée G. Lavoie, Kathi Avery Kinew, and Alan Katz. 2022. "Canada First Nations Strengths in Community-Based Primary Healthcare" International Journal of Environmental Research and Public Health 19, no. 20: 13532. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192013532