
Severity of Placental Abruption in Restrained Pregnant Vehicle Drivers: Correct Seat Belt Use Confirmed by Finite Element Model Analysis

Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. FE Model of Pregnant Woman
2.2. FE Model of Driver’s Seat
2.3. Sled Impact Test Simulation
2.3.1. Placental Abruption Area Analysis in Typical Safety Equipment Settings
2.3.2. Mitigating Placental Abruption by Reconfiguring Safety Equipment
3. Results
3.1. Validation of Sled Impact Test FE Model
3.2. Determining Placental Abruption Areas with Typical Safety Equipment Settings
3.3. Determining Placental Abruption Areas with Reconfigured Safety Equipment
4. Discussion
5. Conclusions
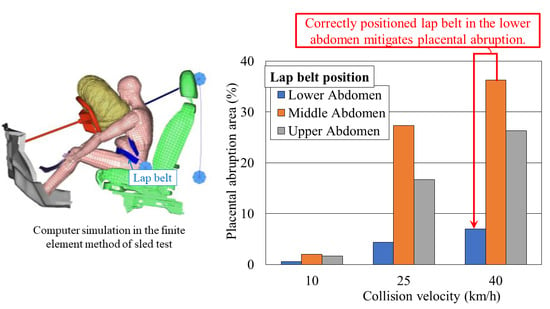
- According to our results, a correctly positioned lap belt could prevent negative fetal outcomes by minimizing the area of placental abruption to 7.0% at 40 km/h.
- Our findings also suggest that a wider lap belt could mitigate placental abruption. A force limiter setting of 2.5 kN may be adequate with respect to both forward movement and placental abruption area.
- We confirmed the safety factors related to correct seat belt use among pregnant drivers.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Fact sheet: Road Traffic Injuries. Available online: https://www.who.int/news-room/fact-sheets/detail/road-traffic-injuries (accessed on 15 August 2022).
- Bose, D.; Segui-Gomez, M.; Crandall, J.R. Vulnerability of female drivers involved in motor vehicle crashes: An analysis of US population at risk. Am. J. Public Health 2011, 101, 2368–2373. [Google Scholar] [CrossRef] [PubMed]
- Connolly, A.M.; Katz, V.L.; Bash, K.L.; McMahon, M.J.; Hansen, W.F. Trauma and pregnancy. Am. J. Perinatol. 1997, 14, 331–336. [Google Scholar] [CrossRef]
- Van Mieghem, T.; Whittle, W.L.; Farine, D.; Seaward, G.; D’Souza, R. Motor vehicle accidents in pregnancy: Implications and management. J. Obstet. Gynaecol. Can. 2013, 35, 303–304. [Google Scholar] [CrossRef]
- Morikawa, M.; Yamada, T.; Kato-Hirayama, E.; Nishikawa, A.; Watari, M.; Maeda, N.; Kogo, H.; Minakami, H. Seatbelt use and seat preference among pregnant women in Sapporo, Japan, in 2013. J. Obstet. Gynaecol. Res. 2016, 42, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Pearlman, M.D.; Tintinalli, J.E.; Lorenz, R.P. A prospective controlled study of outcome after trauma during pregnancy. Am. J. Obstet. Gynecol. 1990, 162, 1502–1510. [Google Scholar] [CrossRef]
- Page, E.W.; King, E.B.; A Merrill, J. Abruptio placentae; dangers of delay in delivery. Obstet. Gynecol. 1954, 3, 385–393. [Google Scholar] [PubMed]
- Tanaka, K.; Motozawa, Y.; Takahashi, K.; Maki, T.; Hitosugi, M. Factors affecting the severity of placental abruption in pregnant vehicle drivers: Analysis with a novel finite element model. Healthcare 2021, 10, 27. [Google Scholar] [CrossRef]
- Valckx, K.; Iida, T.; Motozawa, Y.; Hitosugi, M. Trend of seatbelt use in pregnant women drivers. J. Jpn. Soc. Perinat. Neonatal Med. 2010, 46, 49–53, (in Japanese with English abstract). [Google Scholar]
- Klinich, K.; Flannagan, C.A.; Rupp, J.; Sochor, M.; Schneider, L.W.; Pearlman, M.D. Fetal outcome in motor-vehicle crashes: Effects of crash characteristics and maternal restraint. Am. J. Obstet. Gynecol. 2008, 198, 450.e1–450.e9. [Google Scholar] [CrossRef]
- Hanahara, K.; Hitosugi, M.; Tateoka, Y. Education for appropriate seatbelt use required for early-phase pregnant women drivers. Sci. Rep. 2020, 10, 17609. [Google Scholar] [CrossRef]
- Koh, S.; Hitosugi, M.; Moriguchi, S.; Baba, M.; Tsujimura, S.; Takeda, A.; Takaso, M.; Nakamura, M. Comparison of Motor Vehicle Collision Injuries between Pregnant and Non-Pregnant Women: A Nationwide Collision Data-Based Study. Healthcare 2021, 9, 1414. [Google Scholar] [CrossRef]
- Manoogian, S. Comparison of pregnant and non-pregnant occupant crash and injury characteristics based on national crash data. Accid. Anal. Prev. 2015, 74, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Ghasedi, M.; Sarfjoo, M.; Bargegol, I. Prediction and Analysis of the Severity and Number of Suburban Accidents Using Logit Model, Factor Analysis and Machine Learning: A case study in a developing country. SN Appl. Sci. 2021, 3, 13. [Google Scholar] [CrossRef]
- Martin, P.L.; Audet, T.; Corriveau, H.; Hamel, M.; D’Amours, M.; Smeesters, C. Comparison between younger and older drivers of the effect of obstacle direction on the minimum obstacle distance to brake and avoid a motor vehicle accident. Accid. Anal. Prev. 2010, 42, 1144–1150. [Google Scholar] [CrossRef] [PubMed]
- Najafi Moghaddam Gilani, V.; Hosseinian, S.M.; Ghasedi, M.; Nikookar, M. Data-Driven Urban Traffic Accident Analysis and Prediction Using Logit and Machine Learning-Based Pattern Recognition Models. Math. Probl. Eng. 2021, 2021, 9974219. [Google Scholar] [CrossRef]
- Dave, D.D.; Jha, B.K. 3D mathematical modeling of calcium signaling in Alzheimer’s disease. Netw. Model. Anal. Health Inform. Bioinform. 2019, 9, 1. [Google Scholar] [CrossRef]
- Dave, D.D.; Jha, B.K. On finite element estimation of calcium advection diffusion in a multipolar neuron. J. Eng. Math. 2021, 128, 11. [Google Scholar] [CrossRef]
- Naik, P.A. Modeling the mechanics of calcium regulation in T lymphocyte: A finite element method approach. Int. J. Biomath. 2020, 13, 2050038. [Google Scholar] [CrossRef]
- Kumar, H.; Naik, P.A.; Pardasani, K.R. Finite element model to study calcium distribution in T lymphocyte involving buffers and ryanodine receptors. Proc. Natl. Acad. Sci. India Sect. A Phys. Sci. 2018, 88, 585–590. [Google Scholar] [CrossRef]
- Motozawa, Y.; Hitosugi, M.; Abe, T.; Tokudome, S. Effects of seatbelts worn by pregnant drivers during low-impact collisions. Am. J. Obstet. Gynecol. 2010, 203, 62.e1–62.e8. [Google Scholar] [CrossRef]
- Motozawa, Y.; Hitosugi, M.; Abe, T.; Tokudome, S. Analysis of the kinematics of pregnant drivers during low-speed frontal vehicle collisions. Int. J. Crashworthiness 2010, 15, 235–239. [Google Scholar] [CrossRef]
- Takeda, A.; Motozawa, Y.; Takaso, M.; Nakamura, M.; Hattori, S.; Hitosugi, M. Mechanisms of Negative Fetal Outcome in Frontal Vehicle Colli-Sions Involving Unbelted Pregnant Drivers. Healthcare 2020, 9, 25. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, K.; Yoshida, R.; Nakajima, Y.; Tanaka, Y.; Ishigaki, R.; Hosokawa, N.; Tanaka, Y.; Hitosugi, M. The effects of inboard shoulder belt and lap belt loadings on chest deflection. Stapp Car Crash J. 2018, 62, 67–91. [Google Scholar]
- Rupp, J.D.; Schneider, L.W.; Klinich, K.D. Design, Development and Testing of a New Pregnant Abdomen for the Hybrid III Small Female Crash Test Dummy; University of Michigan Transportation Research Institute: Ann Arbor, MI, USA, 2001. [Google Scholar]
- Hitosugi, M.; Motozawa, Y.; Kido, M.; Yokoyama, T.; Kawato, H.; Kuroda, K.; Tokudome, S. Traffic injuries of the pregnant women and fetal or neonatal outcomes. Forensic Sci. Int. 2006, 159, 51–54. [Google Scholar] [CrossRef]
- Hitosugi, M.; Koseki, T.; Hariya, T.; Maeda, G.; Moriguchi, S.; Hiraizumi, S. Shorter pregnant women restrained in the rear seat of a car are at risk for serious neck injuries: Biomechanical analysis using a pregnant crash test dummy. Forensic Sci. Int. 2018, 291, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Ishiko, A.; Hitosugi, M.; Takaso, M.; Mizuno, K.; Tsuji, S.; Ono, T.; Kimura, F.; Murakami, T. Chest compression of a pregnant woman by a seatbelt might affect fetal outcome, even in minor to moderate frontal vehicle collisions. Forensic Sci. Int. 2019, 302, 109888. [Google Scholar] [CrossRef]
- Motozawa, Y.; Hitosugi, M.; Tokudome, S. Analysis of seating position and anthropometric parameters of pregnant Japanese drivers. Traffic Inj. Prev. 2008, 9, 77–82. [Google Scholar] [CrossRef]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, K.; Motozawa, Y.; Takahashi, K.; Maki, T.; Nakamura, M.; Hitosugi, M. Severity of Placental Abruption in Restrained Pregnant Vehicle Drivers: Correct Seat Belt Use Confirmed by Finite Element Model Analysis. Int. J. Environ. Res. Public Health 2022, 19, 13905. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192113905
Tanaka K, Motozawa Y, Takahashi K, Maki T, Nakamura M, Hitosugi M. Severity of Placental Abruption in Restrained Pregnant Vehicle Drivers: Correct Seat Belt Use Confirmed by Finite Element Model Analysis. International Journal of Environmental Research and Public Health. 2022; 19(21):13905. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192113905
Chicago/Turabian StyleTanaka, Katsunori, Yasuki Motozawa, Kentaro Takahashi, Tetsuo Maki, Mami Nakamura, and Masahito Hitosugi. 2022. "Severity of Placental Abruption in Restrained Pregnant Vehicle Drivers: Correct Seat Belt Use Confirmed by Finite Element Model Analysis" International Journal of Environmental Research and Public Health 19, no. 21: 13905. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192113905