
The Impact of Oral Health Behaviors, Health Belief Model, and Absolute Risk Aversion on the Willingness of Japanese University Students to Undergo Regular Dental Check-Ups: A Cross-Sectional Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
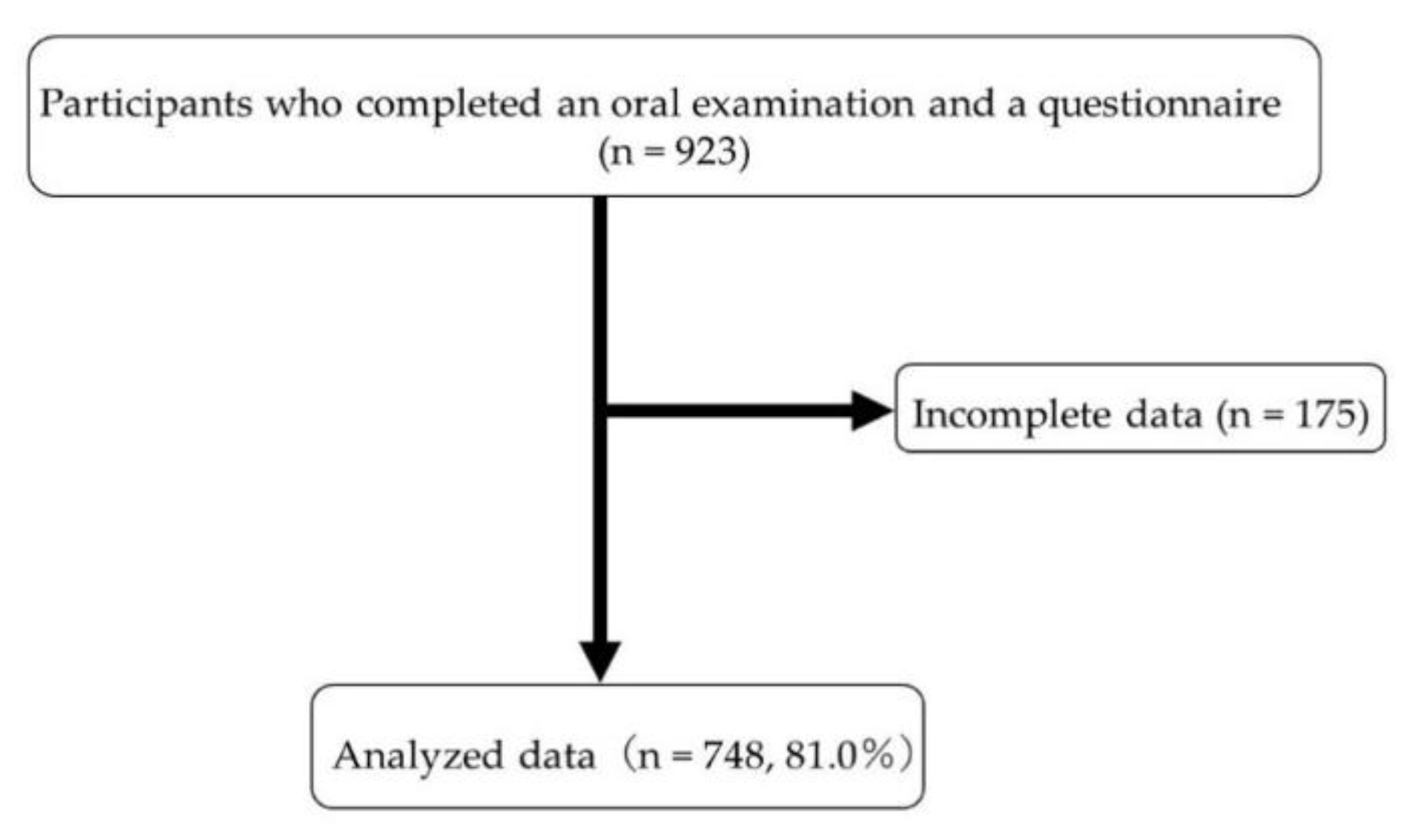
2.1. Study Population
2.2. Ethical Procedures and Informed Consent
2.3. Questionnaire
2.3.1. Oral Health Behaviors
2.3.2. Self-Stated Oral Health Status and Self-Rated Health Status
2.3.3. Health Belief Model
2.3.4. Absolute Risk Aversion
2.3.5. Willingness to Undergo Regular Dental Check-Ups
2.4. Oral Examination
2.5. Sample Size
2.6. Bias
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Mizutani, S.; Ekuni, D.; Furuta, M.; Tomofuji, T.; Irie, K.; Azuma, T.; Kojima, A.; Nagase, J.; Iwasaki, Y.; Morita, M. Effects of Self-Efficacy on Oral Health Behaviours and Gingival Health in University Students Aged 18- or 19-Years-Old. J. Clin. Periodontol. 2012, 39, 844–849. [Google Scholar] [CrossRef]
- Furuta, M.; Ekuni, D.; Irie, K.; Azuma, T.; Tomofuji, T.; Ogura, T.; Morita, M. Sex Differences in Gingivitis Relate to Interaction of Oral Health Behaviors in Young People. J. Periodontol. 2011, 82, 558–565. [Google Scholar] [CrossRef]
- Nakahara, M.; Ekuni, D.; Kataoka, K.; Yokoi, A.; Uchida-Fukuhara, Y.; Fukuhara, D.; Kobayashi, T.; Toyama, N.; Saho, H.; Islam, M.M.; et al. Living with Family Is Directly Associated with Regular Dental Checkup and Indirectly Associated with Gingival Status among Japanese University Students: A 3-Year Cohort Study. IJERPH 2021, 18, 324. [Google Scholar] [CrossRef]
- The National Health and Nutrition Survey in Japan. 2016. Available online: https://www.mhlw.go.jp/content/000681180.pdf (accessed on 26 September 2022).
- Rosenstock, I.M. Why People Use Health Services. Milbank Mem. Fund Q. 1966, 44, 94–127. [Google Scholar] [CrossRef]
- Lee, C.-Y.; Ting, C.-C.; Wu, J.-H.; Lee, K.-T.; Chen, H.-S.; Chang, Y.-Y. Dental Visiting Behaviours among Primary Schoolchildren: Application of the Health Belief Model. Int. J. Dent. Hyg. 2018, 16, e88–e95. [Google Scholar] [CrossRef]
- Ritchie, D.; Van den Broucke, S.; Van Hal, G. The Health Belief Model and Theory of Planned Behavior Applied to Mammography Screening: A Systematic Review and Meta-Analysis. Public Health Nurs. 2021, 38, 482–492. [Google Scholar] [CrossRef]
- Rahmati-Najarkolaei, F.; Rahnama, P.; Gholami Fesharaki, M.; Behnood, V. Predictors of Oral Health Behaviors in Female Students: An Application of the Health Belief Model. Iran. Red Crescent Med. J. 2016, 18, e24747. [Google Scholar] [CrossRef]
- Boyle, P.A.; Yu, L.; Buchman, A.S.; Bennett, D.A. Risk Aversion Is Associated with Decision Making among Community-Based Older Persons. Front. Psychol. 2012, 3, 205. [Google Scholar] [CrossRef]
- Riddel, M.; Hales, D. Predicting Cancer-Prevention Behavior: Disentangling the Effects of Risk Aversion and Risk Perceptions. Risk Anal. 2018, 38, 2161–2177. [Google Scholar] [CrossRef]
- Picone, G.; Sloan, F.; Taylor, D., Jr. Effects of Risk and Time Preference and Expected Longevity on Demand for Medical Tests. J. Risk Uncertain. 2004, 28, 39–53. [Google Scholar] [CrossRef]
- Cramer, J.S.; Hartog, J.; Jonker, N.; Van Praag, C.M. Low Risk Aversion Encourages the Choice for Entrepreneurship: An Empirical Test of a Truism. J. Econ. Behav. Organ. 2002, 48, 29–36. [Google Scholar] [CrossRef]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric Assessment of Subjective Sleep Quality Using the Japanese Version of the Pittsburgh Sleep Quality Index (PSQI-J) in Psychiatric Disordered and Control Subjects. Psychiatry Res. 2000, 97, 165–172. [Google Scholar] [CrossRef]
- Wee, J.H.; Yoo, D.M.; Byun, S.H.; Lee, H.-J.; Park, B.; Park, M.W.; Choi, H.G. Subjective Oral Health Status in an Adult Korean Population with Asthma or Allergic Rhinitis. Medicine 2020, 99, e22967. [Google Scholar] [CrossRef]
- Hakeberg, M.; Wide Boman, U. Self-Reported Oral and General Health in Relation to Socioeconomic Position. BMC Public Health 2018, 18, 63. [Google Scholar] [CrossRef]
- Vozza, I.; Capasso, F.; Calcagnile, F. School-age Dental Screening: Oral Health and Eating Habits. La Clin. Ter. 2019, 170, e36–e40. [Google Scholar] [CrossRef]
- Zahid, N.; Khadka, N.; Ganguly, M.; Varimezova, T.; Turton, B.; Spero, L.; Sokal-Gutierrez, K. Associations between Child Snack and Beverage Consumption, Severe Dental Caries, and Malnutrition in Nepal. IJERPH 2020, 17, 7911. [Google Scholar] [CrossRef]
- Cott, C.A.; Gignac, M.A.; Badley, E.M. Determinants of Self Rated Health for Canadians with Chronic Disease and Disability. J. Epidemiol. Commu. Health 1999, 53, 731–736. [Google Scholar] [CrossRef]
- Tsunematsu, M.; Kawasaki, H.; Masuoka, Y.; Kakehashi, M. Factors Affecting Breast Cancer Screening Behavior in Japan—Assessment Using the Health Belief Model and Conjoint Analysis. Asian Pac. J. Cancer Prev. 2013, 14, 6041–6048. [Google Scholar] [CrossRef]
- Kahneman, D.; Tversky, A. Prospect Theory: An Analysis of Decision under Risk. Econometrica 1979, 47, 263. [Google Scholar] [CrossRef]
- Eeckhoudt, L.; Fiori, A.; Rosazza Gianin, E. Risk Aversion, Loss Aversion, and the Demand for Insurance. Risks 2018, 6, 60. [Google Scholar] [CrossRef]
- Hanaoka, C.; Shigeoka, H.; Watanabe, Y. Do Risk Preferences Change? Evidence from Panel Data Before and after the Great East Japan Earthquake. SSRN J. 2014, 10, 298–330. [Google Scholar] [CrossRef]
- Oral Health Survey Basics Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997; Available online: https://apps.who.int/iris/bitstream/handle/10665/41905/9241544937.pdf?sequence=1&isAllowed=y (accessed on 26 September 2022).
- Greene, J.C.; Vermillion, J.R. The Simplified Oral Hygiene Index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, G.; Greenland, S. Simulation Study of Confounder-Selection Strategies. Am. J. Epidemiol. 1993, 138, 923–936. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, Y.; Nonoyama, T.; Miyano, Y.; Miyata, Y.; Hisada, K.; Nagasawa, T. Association between Dental Consultation and Oral Health Status among Male Japanese Employees. Jrnl. Occup. Health 2020, 62, e12104. [Google Scholar] [CrossRef] [PubMed]
- Setiawan, A.S.; Zubaedah, C. Application of Health Belief Model on Child’s Dental Visit Postponement during the COVID-19 Pandemic. Eur. J. Dent. 2020, 14, S7–S13. [Google Scholar] [CrossRef]
- Frank, D.; Swedmark, J.; Grubbs, L. Colon Cancer Screening in African American Women. ABNF J. 2004, 15, 67–70. [Google Scholar]
- Ghobadi Dashdebi, K.; Noroozi, A.; Tahmasebi, R. Factors Predicting Fecal Occult Blood Testing among Residents of Bushehr, Iran, Based on the Health Belief Model. Asian Pac. J. Cancer Prev. 2016, 17, 17–22. [Google Scholar] [CrossRef]
- Lau, J.; Lim, T.-Z.; Jianlin Wong, G.; Tan, K.-K. The Health Belief Model and Colorectal Cancer Screening in the General Population: A Systematic Review. Prev. Med. Rep. 2020, 20, 101223. [Google Scholar] [CrossRef]
- Didarloo, A.; Nabilou, B.; Khalkhali, H.R. Psychosocial Predictors of Breast Self-Examination Behavior among Female Students: An Application of the Health Belief Model Using Logistic Regression. BMC Public Health 2017, 17, 861. [Google Scholar] [CrossRef]
- Shirazi Zadeh Mehraban, S.; Namdar, A.; Naghizadeh, M.M. Assessment of Preventive Behavior for Cervical Cancer with the Health Belief Model. Asian Pac. J. Cancer Prev. 2018, 19, 2155–2163. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K.; Auladi, S. Health Belief Model and Practice of Breast Self-Examination and Breast Cancer Screening in Iranian Women. Breast Cancer 2014, 21, 429–434. [Google Scholar] [CrossRef]
- Kara, B.; Acikel, C.H. Health Beliefs and Breast Self-Examination in a Sample of Turkish Nursing Students and Their Mothers. J. Clin. Nurs. 2009, 18, 1412–1421. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-Efficacy: Toward a Unifying Theory of Behavioral Change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.E.; Strack, S.; Graves, P. Development of Oral Hygiene Self-Efficacy and Outcome Expectancy Questionnaires. Commun. Dent. Oral Epidemiol. 1997, 25, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Kamalikhah, T.; Abad, S.M.M.; Khalighinejad, N.; Rahmati-Najarkolaei, F. Dental Flossing Behaviour and Its Determinants among Students in a Suburb Area of Tehran-Iran: Using Transtheoretical Model. Int. J. Dent. Hyg. 2017, 15, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Deakin, J.; Aitken, M.; Robbins, T.; Sahakian, B.J. Risk Taking during Decision-Making in Normal Volunteers Changes with Age. J. Int. Neuropsychol. Soc. 2004, 10, 590–598. [Google Scholar] [CrossRef]
- Albert, S.M.; Duffy, J. Differences in Risk Aversion between Young and Older Adults. NAN 2012, 3, 10.2147/NAN.S27184. [Google Scholar] [CrossRef]
- Rosen, A.B.; Tsai, J.S.; Downs, S.M. Variations in Risk Attitude across Race, Gender, and Education. Med. Decis. Mak. 2003, 23, 511–517. [Google Scholar] [CrossRef]
- Ekuni, D.; Toyama, N.; Iwasaki, Y.; Morita, M. New Method of Avoiding Underestimation of Caries Incidence and Its Association with Possible Risk Factors in Japanese University Students: A Prospective Cohort Study. IJERPH 2022, 19, 2490. [Google Scholar] [CrossRef]


{kind=link}
| Factors | Willingness | p ‡ | ||
|---|---|---|---|---|
| (+) (n = 285) | (−) (n = 463) | |||
| Age | 18.0 (18.0, 19.0) * | 18.0 (18.0, 18.0) | 0.489 | |
| Male | 123 (33.3) † | 246 (66.7) | 0.008 | |
| Oral health behaviors | ||||
| Use of the interdental brush or the dental floss | No | 198 (34.3) | 380 (65.7) | <0.001 |
| Yes | 87 (51.2) | 83 (48.8) | ||
| Dental consultation within the past year | No | 111 (31.3) | 244 (68.7) | <0.001 |
| Yes | 174 (44.3) | 219 (55.7) | ||
| Snack and soft drink intake regularly | No | 79 (42.5) | 107 (57.5) | 0.091 |
| Once a day | 164 (37.8) | 270 (62.2) | ||
| Twice a day | 31 (31.0) | 69 (69.0) | ||
| Three times or more a day | 11 (39.3) | 17 (60.7) | ||
| Tooth brushing frequency (times/day) | One time or less | 14 (26.9) | 38 (73.1) | 0.015 |
| Twice | 186 (36.9) | 318 (63.1) | ||
| Three times or more | 85 (44.3) | 107 (55.7) | ||
| Self-rated oral health status | Very poor | 7 (38.9) | 11 (61.1) | 0.013 |
| Poor | 37 (34.6) | 70 (65.4) | ||
| Fair | 114 (33.6) | 225 (66.4) | ||
| Good | 95 (44.6) | 118 (55.4) | ||
| Very good | 32 (45.1) | 39 (54.9) | ||
| Self-rated health status | Very poor | 4 (57.1) | 3 (42.9) | 0.020 |
| Poor | 7 (24.1) | 22 (75.9) | ||
| Fair | 47 (32.2) | 99 (67.8) | ||
| Good | 133 (38.1) | 216 (61.9) | ||
| Very good | 94 (43.3) | 123 (56.7) | ||
| Health belief model | ||||
| Perceived susceptibility | 3.0 (2.0, 3.0) | 3.0 (2.0, 3.0) | 0.084 | |
| Perceived benefits—1 | 5.0 (4.0, 5.0) | 5.0 (4.0, 5.0) | 0.001 | |
| Perceived benefits—2 | 5.0 (4.0, 5.0) | 4.0 (4.0, 5.0) | <0.001 | |
| Perceived benefits—3 | 5.0 (4.0, 5.0) | 5.0 (4.0, 5.0) | <0.001 | |
| Perceived severity—1 | 4.0 (3.0, 5.0) | 3.0 (3.0, 4.0) | 0.001 | |
| Perceived severity—2 | 3.0 (2.0, 4.0) | 3.0 (3.0, 4.0) | 0.005 | |
| Perceived barrier | 2.0 (1.0, 3.0) | 2.0 (1.0, 3.0) | <0.001 | |
| Absolute risk aversion (×10−5) | 2.0 (1.8, 2.0) | 2.0 (1.8, 2.0) | 0.253 | |
| Oral health status | ||||
| Decayed, missing, and filled teeth | 0.000 (0.000, 0.003) | 0.000 (0.000, 0.003) | 0.698 | |
| Percentage of bleeding on probing | 10.0 (0.0, 30.0) | 10.0 (0.0, 30.0) | 0.135 | |
| Oral Hygiene Index-Simplified | 0.2 (0.0, 0.7) | 0.3 (0.0, 0.7) | 0.093 | |
| OR * | 95% CI | p | ||
|---|---|---|---|---|
| Gender | Male | 1 | 0.865–1.655 | 0.279 |
| Female | 1.196 | |||
| Oral health behaviors | ||||
| Use of the interdental brush or the dental floss | No | 1 | ||
| Yes | 1.616 | 1.104–2.365 | 0.014 | |
| Dental consultation within the past year | No | 1 | ||
| Yes | 1.371 | 0.985–1.909 | 0.061 | |
| Tooth brushing (times/day) | One time or less | 1 | ||
| Twice | 0.923 | 0.639–1.333 | 0.669 | |
| Three times or more | 0.663 | 0.319–1.376 | 0.270 | |
| Snack and soft drink intake regularly | No | 1 | ||
| Once a day | 0.834 | 0.332–2.099 | 0.700 | |
| Twice a day | 0.978 | 0.425–2.248 | 0.958 | |
| Three times or more a day | 1.225 | 0.515–2.915 | 0.646 | |
| Self-rated oral health status | 1.007 | 0.805–1.260 | 0.948 | |
| Self-rated health status | 1.083 | 0.885–1.341 | 0.417 | |
| Health belief model | ||||
| Perceived susceptibility | 0.942 | 0.784–1.131 | 0.519 | |
| Perceived benefits—1 | 1.175 | 0.906–1.522 | 0.224 | |
| Perceived benefits—2 | 1.683 | 1.254–2.260 | <0.001 | |
| Perceived benefits—3 | 1.044 | 0.740–1.474 | 0.806 | |
| Perceived severity—1 | 1.167 | 0.975–1.397 | 0.092 | |
| Perceived severity—2 | 0.917 | 0.774–1.068 | 0.316 | |
| Perceived barrier | 0.922 | 0.796–1.068 | 0.279 | |
| Oral Hygiene Index-Simplified | 0.817 | 0.562–1.187 | 0.288 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumita, I.; Toyama, N.; Ekuni, D.; Maruyama, T.; Yokoi, A.; Fukuhara, D.; Uchida-Fukuhara, Y.; Nakahara, M.; Morita, M. The Impact of Oral Health Behaviors, Health Belief Model, and Absolute Risk Aversion on the Willingness of Japanese University Students to Undergo Regular Dental Check-Ups: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 13920. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192113920
Sumita I, Toyama N, Ekuni D, Maruyama T, Yokoi A, Fukuhara D, Uchida-Fukuhara Y, Nakahara M, Morita M. The Impact of Oral Health Behaviors, Health Belief Model, and Absolute Risk Aversion on the Willingness of Japanese University Students to Undergo Regular Dental Check-Ups: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(21):13920. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192113920
Chicago/Turabian StyleSumita, Ichiro, Naoki Toyama, Daisuke Ekuni, Takayuki Maruyama, Aya Yokoi, Daiki Fukuhara, Yoko Uchida-Fukuhara, Momoko Nakahara, and Manabu Morita. 2022. "The Impact of Oral Health Behaviors, Health Belief Model, and Absolute Risk Aversion on the Willingness of Japanese University Students to Undergo Regular Dental Check-Ups: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 21: 13920. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192113920