
Maternal Serum α-Fetoprotein Levels during Pregnancy and Testicular Cancer in Male Offspring: A Cohort Study within a Danish Pregnancy Screening Registry
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
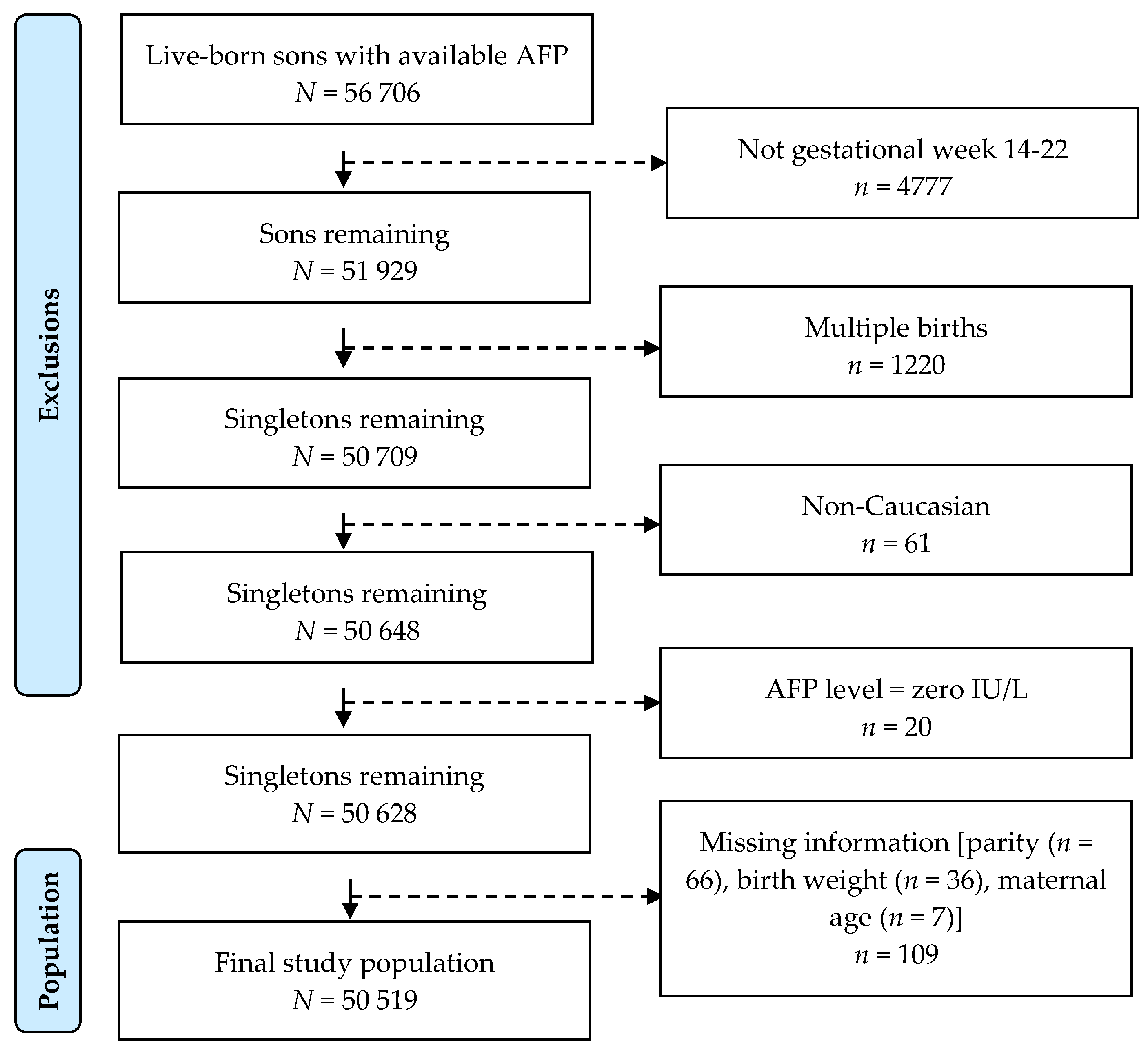
2.2. Study Population
2.3. Testicular Cancer
2.4. α-Fetoprotein (AFP)
2.5. Covariates
2.6. Statistical Analyses
2.7. Ethical Considerations and Data Protection
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ulbright, T.; Amin, M.; Balzer, B.; Berney, D.; Epstein, J.; Guo, C.; MT, I.; Looijenga, L.; Paner, G.; Rajpert-De Meyts, E.; et al. Germ Cell Tumours. In WHO Classification of Tumours of the Urinary System and Male Genital Organs; Moch, H., Humphrey, P.A., Ulbright, T.M., Reuter, V.E., Eds.; International Agency for Research on Cancer (IARC): Lyon, France, 2016; pp. 189–226. [Google Scholar]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, G.K.; Barlebo, H.; Olsen, J.; Schultz, H.P.; Starklint, H.; Søgaard, H.; Væth, M.; Group, D.S. Testicular Germ Cell Tumours in Denmark 1976–1980. Pathology of 1058 Consecutive Cases. Acta Radiol. Oncol. 1984, 23, 239–247. [Google Scholar] [CrossRef]
- Meyts, E.R.-D.; Skakkebaek, N.E.; Toppari, J. Testicular Cancer Pathogenesis, Diagnosis and Endocrine Aspects. In Endotext; MDText.com, Inc.: South Darthmouth, MA, USA, 2018. [Google Scholar]
- Skakkebaek, N.E.; Berthelsen, J.G.; Giwercman, A.; Muller, J. Carcinoma-in-Situ of the Testis: Possible Origin from Gonocytes and Precursor of All Types of Germ Cell Tumours except Spermatocytoma. Int. J. Androl. 1987, 10, 19–28. [Google Scholar] [CrossRef]
- Oosterhuis, J.W.; Looijenga, L.H.J. Testicular Germ-Cell Tumours in a Broader Perspective. Nat. Rev. Cancer 2005, 5, 210–222. [Google Scholar] [CrossRef]
- Juul, A.; Almstrup, K.; Andersson, A.; Jensen, T.; Jørgensen, N.; Main, K.; Rajpert-De Meyts, E.; Toppari, J.; Skakkebæk, N. Possible Fetal Determinants of Male Infertility. Nat. Rev. Endocrinol. 2014, 10, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Bay, K.; Asklund, C.; Skakkebaek, N.; Andersson, A. Testicular Dysgenesis Syndrome: Possible Role of Endocrine Disrupters. Best Pract. Res. Clin. Endocrinol. Metab. 2006, 20, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Skakkebaek, N.; Rajpert-De Meyts, E.; Main, K. Testicular Dysgenesis Syndrome: An Increasingly Common Developmental Disorder with Environmental Aspects. Hum. Reprod. 2001, 16, 972–978. [Google Scholar] [CrossRef] [Green Version]
- Skakkebaek, N.; Jørgensen, N. Testicular Dysgenesis and Fertility. Andrologia 2005, 37, 217–218. [Google Scholar] [CrossRef]
- McGlynn, K.A.; Cook, M.B. Etiologic Factors in Testicular Germ-Cell Tumors. Future Oncol. 2009, 5, 1389–1402. [Google Scholar] [CrossRef] [Green Version]
- Cook, M.B.; Akre, O.; Forman, D.; Patricia Madigan, M.; Richiardi, L.; McGlynn, K.A. A Systematic Review and Meta-Analysis of Perinatal Variables in Relation to the Risk of Testicular Cancer--Experiences of the Son. Int. J. Epidemiol. 2010, 39, 1605–1618. [Google Scholar] [CrossRef]
- Mizejewski, G.J. Levels of Alpha-Fetoprotein during Pregnancy and Early Infancy in Normal and Disease States. Obstet. Gynecol. Surv. 2003, 58, 804–826. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, D.; Boesman, M. Sites of Serum Alpha-Fetoprotein Synthesis in the Human and in the Rat. J. Clin. Investig. 1967, 46, 1010–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizejewski, G.J. Biological Roles of Alpha-Fetoprotein during Pregnancy and Perinatal Development. Exp. Biol. Med. 2004, 229, 439–463. [Google Scholar] [CrossRef] [PubMed]
- Norgaard-Pedersen, B. A Review of Recent Methodological and Clinical Studies. Scand. J. Immunol. 1976, 5, 7–45. [Google Scholar]
- Mizejewski, G.; Smith, G.; Butterstein, G. Review and Proposed Action of Alpha-Fetoprotein Growth Inhibitory Peptides as Estrogen and Cytoskeleton-Associated Factors. Cell Biol. Int. 2004, 28, 913–933. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, H.I.; Bennett, J.A.; Mizejewski, G.J. Inhibition of Estrogen-Dependent Breast Cancer Growth by a Reaction Product of Alpha-Fetoprotein and Estradiol. Cancer Res. 1990, 50, 415–420. [Google Scholar] [PubMed]
- Allen, S.H.G.; Bennett, J.A.; Mizejewski, G.J.; Andersen, T.T.; Ferraris, S.; Jacobson, H.I. Purification of Alpha-Fetoprotein from Human Cord Serum with Demonstration of Its Antiestrogenic Activity. Biochim. Biophys. Acta 1993, 1202, 135–142. [Google Scholar] [CrossRef]
- Mizejewski, G.J. A Compendium of Ligands Reported to Bind Alpha-Fetoprotein: A Comprehensive Review and Meta-Analysis. Cancer Ther. Oncol. Int. J. 2022, 20. [Google Scholar]
- Schmidt, M.; Pedersen, L.; Sørensen, H. The Danish Civil Registration System as a Tool in Epidemiology. Eur. J. Epidemiol. 2014, 29, 541–549. [Google Scholar] [CrossRef]
- Pedersen, C.B. The Danish Civil Registration System. Scand. J. Public Health 2011, 39, 22–25. [Google Scholar] [CrossRef]
- Gjerstorff, M.L. The Danish Cancer Registry. Scand. J. Public Health 2011, 39, 42–45. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; Fritz, A.; Percy, C.; Jack, A.; Shanmugaratnam, K.; Sobin, L.; Parkin, M.; Whelan, S. International Classification of Diseases for Oncology, 3rd ed.; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Bredaki, F.E.; Sciorio, C.; Wright, A.; Wright, D.; Nicolaides, K.H. Serum Alpha-Fetoprotein in the Three Trimesters of Pregnancy: Effects of Maternal Characteristics and Medical History. Ultrasound Obstet. Gynecol. 2015, 46, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Blettner, M.; et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Graubard, B.I.; Klebanoff, M.A.; Ronckers, C.; Stanczyk, F.Z.; Longnecker, M.P.; McGlynn, K.A. Maternal Hormone Levels among Populations at High and Low Risk of Testicular Germ Cell Cancer. Br. J. Cancer 2005, 92, 1787–1793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, W.B.; Rovito, M.J.; Craycraft, M. The Connection Between Testicular Cancer, Minority Males, and Planned Parenthood. Am. J. Mens. Health 2018, 12, 1774. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Lu, Q.; Wang, Y.; Ma, S. Racial Differences in Testicular Cancer in the United States: Descriptive Epidemiology. BMC Cancer 2020, 20, 284. [Google Scholar] [CrossRef]
- Sharpe, R.M.; Skakkebaek, N.E. Testicular Dysgenesis Syndrome: Mechanistic Insights and Potential New Downstream Effects. Fertil. Steril. 2008, 89, e33–e38. [Google Scholar] [CrossRef]
- Boyd, H.A.; Myrup, C.; Wohlfahrt, J.; Westergaard, T.; Nørgaard-Pedersen, B.; Melbye, M. Maternal Serum Alpha-Fetoprotein Level during Pregnancy and Isolated Cryptorchidism in Male Offspring. Am. J. Epidemiol. 2006, 164, 478–486. [Google Scholar] [CrossRef] [Green Version]
- Mead, G.M. International Germ Cell Consensus Classification: A Prognostic Factor-Based Staging System for Metastatic Germ Cell Cancers. International Germ Cell Cancer Collaborative Group. J. Clin. Oncol. 1997, 15, 594–603. [Google Scholar] [CrossRef]
- Milose, J.C.; Filson, C.P.; Weizer, A.Z.; Hafez, K.S.; Montgomery, J.S. Role of Biochemical Markers in Testicular Cancer: Diagnosis, Staging, and Surveillance. Open Access J. Urol. 2011, 4, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Wald, N.; Barker, S.; Peto, R.; Brock, D.J.H.; Bonnar, J. Maternal Serum Alpha-Fetoprotein Levels in Multiple Pregnancy. Br. Med. J. 1975, 1, 651–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trabert, B.; Chen, J.; Devesa, S.S.; Bray, F.; Mcglynn, K.A. International Patterns and Trends in Testicular Cancer Incidence, Overall and by Histologic Subtype, 1973–2007. Andrology 2015, 3, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, M.S.; Lauritsen, J.; Gundgaard, M.G.; Agerbæk, M.; Holm, N.V.; Christensen, I.J.; Von Der Maase, H.; Daugaard, G. A Nationwide Cohort Study of Stage I Seminoma Patients Followed on a Surveillance Program. Eur. Urol. 2014, 66, 1172–1178. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.N.; Devesa, S.S.; Zhu, K.; McGlynn, K.A. Trends in Testicular Germ Cell Tumours by Ethnic Group in the United States. Int. J. Androl. 2007, 30, 206–214. [Google Scholar] [CrossRef]
- Leveridge, M.J.; Siemens, D.R.; Brennan, K.; Izard, J.P.; Karim, S.; An, H.; Mackillop, W.J.; Booth, C.M. Temporal Trends in Management and Outcomes of Testicular Cancer: A Population-Based Study. Cancer 2018, 124, 2724–2732. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Non-Cases, n (%) | Testicular Cancer Cases, n (%) | ||
|---|---|---|---|---|
| (n = 50,354) | All (n = 163) # | Seminoma (n = 73) ‡ | Nonseminoma (n = 89) ‡,* | |
| Son’s age at testicular cancer diagnosis, median (25th–75th percentile) | ||||
| - | 26.5 (23.6–31.6) | 28.7 (25.4–32.1) | 24.9 (22.4–29.9) | |
| Gestational age (weeks) at birth | ||||
| ≤39 | 18,994 (37.7) | 69 (42.3) | 24 (32.9) | 44 (49.4) |
| 40 | 17,855 (35.5) | 55 (33.7) | 25 (34.2) | 30 (33.7) |
| ≥41 | 13,505 (26.8) | 39 (23.9) | 24 (32.9) | 15 (16.9) |
| Preterm (<37 weeks) | ||||
| Yes | 2473 (4.9) | 9 (5.5) | 3 (4.0) | 6 (6.4) |
| Birth weight (g) | ||||
| ≤2999 | 7519 (14.9) | 24 (14.7) | 10 (13.7) | 13 (14.6) |
| 3000–3499 | 15,832 (31.4) | 52 (31.9) | 24 (32.9) | 28 (31.5) |
| 3500–3999 | 17,421 (34.6) | 56 (34.4) | 26 (35.6) | 30 (33.7) |
| 4000–4499 | 7825 (15.5) | 27 (16.6) | 11 (15.1) | 16 (18.0) |
| ≥4500 | 1757 (3.5) | 4 (2.5) | 2 (2.7) | 2 (2.3) |
| Birth weight for gestational age | ||||
| SGA a | 5005 (9.9) | 19 (11.7) | 9 (12.3) | 9 (10.1) |
| Normal b | 39,094 (77.6) | 125 (76.7) | 59 (80.8) | 66 (74.2) |
| LGA c | 6285 (12.5) | 19 (11.7) | 5 (6.9) | 14 (15.7) |
| Birth year of son | ||||
| 1980–1984 | 11,205 (22.3) | 51 (31.3) | 26 (35.6) | 24 (27.0) |
| 1985–1989 | 21,082 (41.9) | 82 (50.3) | 34 (46.6) | 48 (53.9) |
| 1990–1996 | 18,067 (35.9) | 30 (18.4) | 13 (17.8) | 17 (19.1) |
| Maternal parity (no. of births prior to index birth) | ||||
| 0 | 24,373 (48.4) | 78 (47.9) | 33 (45.2) | 44 (49.4) |
| 1 | 17,179 (34.1) | 56 (34.4) | 28 (38.4) | 28 (31.5) |
| ≥2 | 8802 (17.5) | 29 (17.8) | 12 (16.4) | 17 (19.1) |
| Maternal age (years) at birth | ||||
| <25 | 11,637 (23.1) | 41 (25.2) | 15 (20.5) | 26 (29.2) |
| 25–29 | 19,003 (37.7) | 56 (34.4) | 29 (39.7) | 26 (29.2) |
| 30–34 | 11,881 (23.6) | 41 (25.2) | 18 (24.7) | 23 (25.8) |
| 35–39 | 6801 (13.5) | 20 (12.3) | 10 (13.7) | 10 (11.2) |
| ≥40 | 1032 (2.1) | 5 (3.1) | 1 (1.4) | 4 (4.5) |
| Cryptorchidism in sons | ||||
| Yes | 1874 (3.7) | 12 (7.4) | 6 (8.2) | 6 (6.7) |
| Paternal testicular cancer | ||||
| Yes | 52 (0.1) | 1 (0.6) | 1 (1.4) | 0 (0.0) |
| Testicular Cancer | AFP MoM a | Ncases/Person Years b | Relative Risk (95% CI) | ||
|---|---|---|---|---|---|
| Model 1 c | Model 2 (Main) d | Model 3 e | |||
| All | <1.00 | 73/749957 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥1.00 | 90/863418 | 1.06 (0.78; 1.44) | 1.04 (0.76; 1.41) | 1.03 (0.76; 1.41) | |
| Seminoma | <1.00 | 38/749063 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥1.00 | 35/861942 | 0.79 (0.50; 1.24) | 0.81 (0.51; 1.29) | 0.81 (0.51; 1.29) | |
| Nonseminoma * | <1.00 | 34/748839 | 1 (reference) | 1 (reference) | 1 (reference) |
| ≥1.00 | 55/862408 | 1.40 (0.91; 2.15) | 1.31 (0.85; 2.02) | 1.31 (0.85; 2.01) | |
| Overall | Seminoma | Nonseminoma * | ||||
|---|---|---|---|---|---|---|
| Stratification Variable | RR for AFP MoM ≥ 1 vs. AFP MoM < 1 (95% CI) ‡ | P for Trend | RR for AFP MoM ≥ 1 vs. AFP MoM < 1 (95% CI) ‡ | P for Trend | RR for AFP MoM ≥ 1 vs. AFP MoM < 1 (95% CI) ‡ | P for Trend |
| Gestational age (weeks) at birth | ||||||
| ≤39 | 1.16 (0.71; 1.90) | 0.420 | 1.09 (0.48; 2.50) | 0.120 | 1.28 (0.69; 2.40) | 0.992 |
| 40 | 0.78 (0.46; 1.32) | 0.41 (0.18; 0.94) | 1.31 (0.63; 2.72) | |||
| ≥41 | 1.27 (0.68; 2.39) | 1.21 (0.54; 2.70) | 1.38 (0.50; 3.82) | |||
| Preterm (<37 weeks) | ||||||
| Yes | 0.42 (0.11; 1.55) | 0.377 | 0.26 (0.02; 2.85) | 0.612 | 0.52 (0.11; 2.59) | 0.513 |
| No | 1.09 (0.79; 1.50) | 0.85 (0.53; 1.37) | 1.40 (0.89; 2.19) | |||
| Birth weight (g) | ||||||
| <2500 | 0.48 (0.10; 2.36) | 0.773 | 0.48 (0.03; 7.68) | 0.924 | na | 0.557 |
| 2500–2999 | 0.63 (0.25; 1.60) | 0.39 (0.09; 1.64) | 0.94 (0.26; 3.33) | |||
| 3000–3499 | 1.23 (0.70; 2.15) | 0.94 (0.42; 2.11) | 1.58 (0.71; 3.49) | |||
| 3500–3999 | 0.86 (0.51; 1.46) | 0.83 (0.38; 1.80) | 0.89 (0.43; 1.83) | |||
| 4000–4499 | 1.84 (0.84; 4.02) | 1.35 (0.41; 4.44) | 2.29 (0.80; 6.61) | |||
| ≥4500 | 1.29 (0.18; 9.13) | na | na | |||
| Birth weight for gestational age | ||||||
| SGA a | 0.47 (0.19; 1.17) | 0.478 | 0.54 (0.14; 2.00) | 0.350 | 0.50 (0.14; 1.88) | 0.318 |
| Normal b | 1.14 (0.80; 1.63) | 0.92 (0.55; 1.54) | 1.41 (0.85; 2.33) | |||
| LGA c | 1.20 (0.49; 2.94) | 0.28 (0.03; 2.51) | 1.86 (0.62; 5.57) | |||
| Birth year of son | ||||||
| 1980–1984 | 1.59 (0.89; 2.82) | 0.129 | 1.25 (0.57; 2.72) | 0.692 | 2.49 (0.99; 6.29) | 0.060 |
| 1985–1989 | 0.87 (0.56; 1.34) | 0.58 (0.29; 1.15) | 1.16 (0.65; 2.08) | |||
| 1990–1996 | 0.79 (0.39; 1.62) | 0.81 (0.27; 2.43) | 0.77 (0.30; 2.01) | |||
| Maternal parity (no. of births prior to index birth) | ||||||
| 0 | 0.85 (0.54; 1.33) | 0.491 | 0.67 (0.34; 1.33) | 0.740 | 1.07 (0.59; 1.96) | 0.600 |
| 1 | 1.25 (0.73; 2.13) | 0.91 (0.43; 1.92) | 1.78 (0.80; 3.93) | |||
| ≥2 | 1.22 (0.59; 2.55) | 1.06 (0.34; 3.28) | 1.36 (0.52; 3.59) | |||
| Maternal age (years) at birth | ||||||
| <25 | 1.07 (0.58; 2.00) | 0.730 | 0.91 (0.33; 2.52) | 0.759 | 1.18 (0.53; 2.60) | 0.447 |
| 25–29 | 0.83 (0.49; 1.40) | 0.70 (0.34; 1.46) | 1.09 (0.50; 2.39) | |||
| 30–34 | 1.23 (0.66; 2.30) | 0.73 (0.29; 1.86) | 1.93 (0.79; 4.70) | |||
| 35–39 | 1.47 (0.60; 3.60) | 1.03 (0.30; 3.56) | 2.21 (0.57; 8.56) | |||
| ≥40 | 0.58 (0.10; 3.48) | na | 0.29 (0.03; 2.75) | |||
| Cryptorchidism in sons | ||||||
| Yes | 1.00 (0.32; 3.15) | 0.151 | 0.74 (0.15; 3.67) | 0.251 | 1.39 (0.26; 7.62) | 0.514 |
| No | 1.03 (0.75; 1.43) | 0.81 (0.50; 1.32) | 1.30 (0.83; 2.03) | |||
| Paternal testicular cancer | ||||||
| Yes | na | na | na | na | na | na |
| No | 1.02 (0.75; 1.40) | 0.79 (0.49; 1.26) | 1.31 (0.85; 2.02) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uldbjerg, C.S.; Lim, Y.-H.; Glazer, C.H.; Hauser, R.; Juul, A.; Bräuner, E.V. Maternal Serum α-Fetoprotein Levels during Pregnancy and Testicular Cancer in Male Offspring: A Cohort Study within a Danish Pregnancy Screening Registry. Int. J. Environ. Res. Public Health 2022, 19, 14112. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192114112
Uldbjerg CS, Lim Y-H, Glazer CH, Hauser R, Juul A, Bräuner EV. Maternal Serum α-Fetoprotein Levels during Pregnancy and Testicular Cancer in Male Offspring: A Cohort Study within a Danish Pregnancy Screening Registry. International Journal of Environmental Research and Public Health. 2022; 19(21):14112. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192114112
Chicago/Turabian StyleUldbjerg, Cecilie S., Youn-Hee Lim, Clara H. Glazer, Russ Hauser, Anders Juul, and Elvira V. Bräuner. 2022. "Maternal Serum α-Fetoprotein Levels during Pregnancy and Testicular Cancer in Male Offspring: A Cohort Study within a Danish Pregnancy Screening Registry" International Journal of Environmental Research and Public Health 19, no. 21: 14112. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192114112