


Expression of Matrix Metalloproteinase-2,-7,-9 in Serum during Pregnancy in Patients with Pre-Eclampsia: A Prospective Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
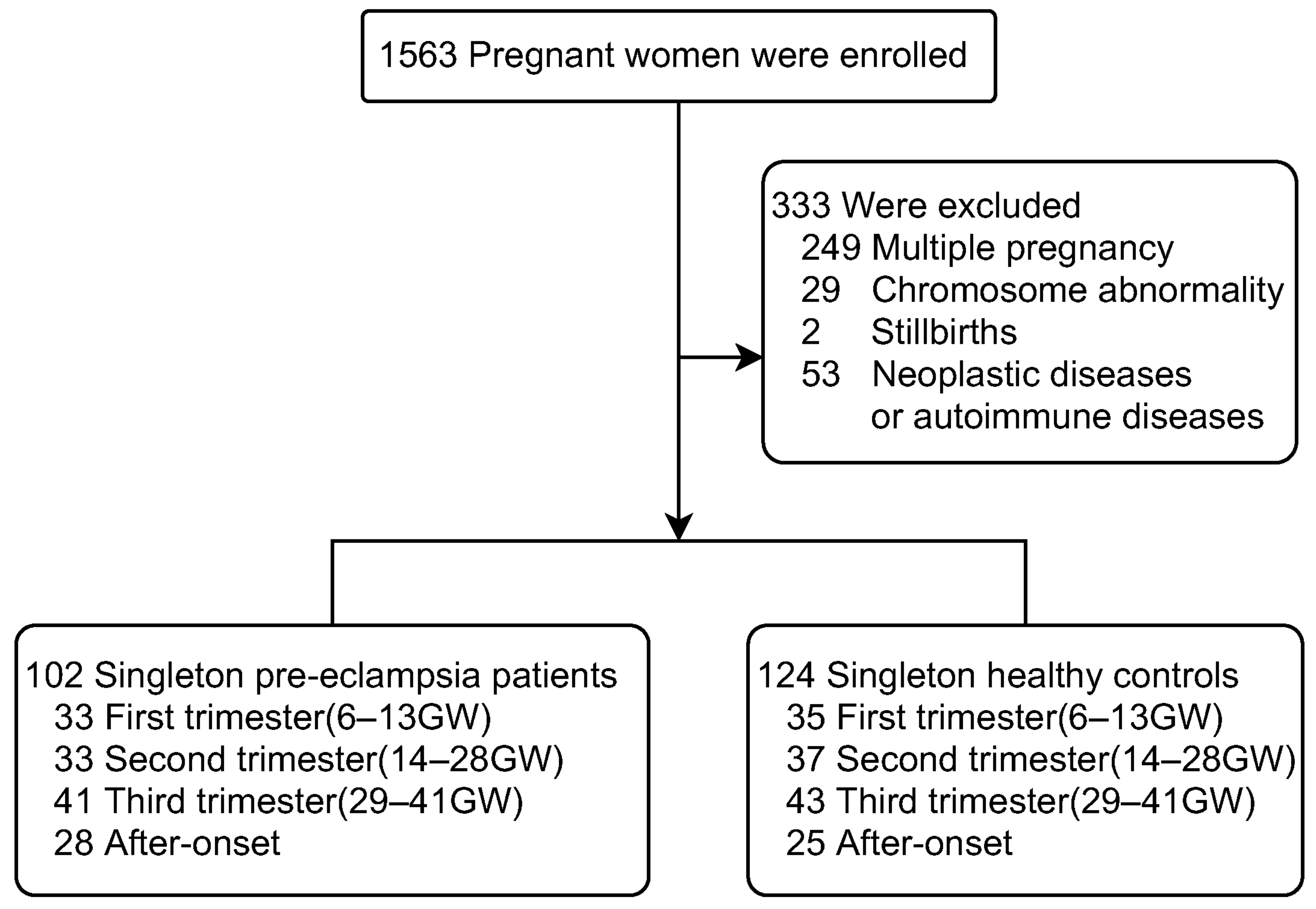
2.1. Study Population
2.2. Inclusion and Exclusion Criteria
- Pre-eclampsia group: A singleton pregnancy that developed pre-eclampsia. The diagnosis of pre-eclampsia was based on the diagnostic criteria of ACOG practice bulletin No. 222 [19];
- Control group: singleton pregnancy, normal conception, normal blood pressure, no diabetes, nephropathy and/or other medical and surgical diseases and no autoimmune diseases.
2.3. Sample Collection
2.4. ELISA
2.5. Statistical Analysis
3. Results
- 1.
- Clinical Characteristics analysis of the study groups.
- 2.
- Serum levels of MMP-2, MMP-7 and MMP-9 in pre-eclampsia and control groups during pregnancy
- 3.
- Analysis of the ROC curve for MMP-2, MMP-7 and MMP-9
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Khan, K.S.; Wojdyla, D.; Say, L.; Gulmezoglu, A.M.; Van Look, P.F.A. WHO analysis of causes of maternal death: A systematic review. Lancet 2006, 367, 1066–1074. [Google Scholar] [CrossRef]
- Ke, L.I.; Zhu, D.W.; Chen, J.K.; Jian, H.A.N.; Zheng, X.H.; Guo, J.X.; Li, L.I. Research progress on pathogenesis and clinical treatment of preeclampsia. Chin. PLA Med. J. 2019, 44, 423–429. [Google Scholar]
- Espino, Y.S.S.; Flores-Pliego, A.; Espejel-Nuñez, A.; Medina-Bastidas, D.; Vadillo-Ortega, F.; Zaga-Clavellina, V.; Estrada-Gutierrez, G. New Insights into the Role of Matrix Metalloproteinases in Preeclampsia. Int. J. Mol. Sci. 2017, 18, 1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redman, C. The six stages of pre-eclampsia. Pregnancy Hypertens. 2014, 4, 246. [Google Scholar] [CrossRef] [PubMed]
- Redman, C.W.; Sargent, I.L. Placental stress and pre-eclampsia: A revised view. Placenta 2009, 30 (Suppl. A), S38–S42. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Khalil, R.A. Matrix Metalloproteinases, Vascular Remodeling, and Vascular Disease. Adv. Pharmacol. 2018, 81, 241–330. [Google Scholar]
- Cabral-Pacheco, G.A.; Garza-Veloz, I.; Castruita-De la Rosa, C.; Ramirez-Acuña, J.M.; Perez-Romero, B.A.; Guerrero-Rodriguez, J.F.; Martinez-Avila, N.; Martinez-Fierro, M.L. The Roles of Matrix Metalloproteinases and Their Inhibitors in Human Diseases. Int. J. Mol. Sci. 2020, 21, 9739. [Google Scholar] [CrossRef]
- Gutiérrez, J.A.; Gómez, I.; Chiarello, D.I.; Salsoso, R.; Klein, A.D.; Guzmán-Gutiérrez, E.; Toledo, F.; Sobrevia, L. Role of proteases in dysfunctional placental vascular remodelling in preeclampsia. Biochim. Biophys. Acta. Mol. Basis Dis. 2020, 1866, 165448. [Google Scholar] [CrossRef]
- Lin, C.; He, H.; Cui, N.; Ren, Z.; Zhu, M.; Khalil, R.A. Decreased uterine vascularization and uterine arterial expansive remodeling with reduced matrix metalloproteinase-2 and -9 in hypertensive pregnancy. Am. J. Physiol. Heart Circ. Physiol. 2020, 318, H165–H180. [Google Scholar] [CrossRef]
- Chen, J.; Khalil, R.A. Matrix Metalloproteinases in Normal Pregnancy and Preeclampsia. Prog. Mol. Biol. Transl. Sci. 2017, 148, 87–165. [Google Scholar]
- Verslegers, M.; Lemmens, K.; Van Hove, I.; Moons, L. Matrix metalloproteinase-2 and -9 as promising benefactors in development, plasticity and repair of the nervous system. Prog. Neurobiol. 2013, 105, 60–78. [Google Scholar] [CrossRef]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef] [Green Version]
- Sahay, A.S.; Jadhav, A.T.; Sundrani, D.P.; Wagh, G.N.; Mehendale, S.S.; Joshi, S.R. Matrix metalloproteinases-2 (MMP-2) and matrix metalloproteinases-9 (MMP-9) are differentially expressed in different regions of normal and preeclampsia placentae. J. Cell. Biochem. 2018, 119, 6657–6664. [Google Scholar] [CrossRef]
- Erez, O.; Romero, R.; Maymon, E.; Chaemsaithong, P.; Done, B.; Pacora, P.; Panaitescu, B.; Chaiworapongsa, T.; Hassan, S.S.; Tarca, A.L. The prediction of late-onset preeclampsia: Results from a longitudinal proteomics study. PLoS ONE 2017, 12, e0181468. [Google Scholar] [CrossRef] [Green Version]
- Staun-Ram, E.; Goldman, S.; Gabarin, D.; Shalev, E. Expression and importance of matrix metalloproteinase 2 and 9 (MMP-2 and -9) in human trophoblast invasion. Reprod. Biol. Endocrinol. 2004, 2, 59. [Google Scholar] [CrossRef] [Green Version]
- Ravn, J.D.; Bendix, E.J.; Sperling, L.; Overgaard, M. First trimester serum matrix metalloproteinase-7 is a poor predictor of late-onset preeclampsia. Pregnancy Hypertens. 2022, 28, 94–99. [Google Scholar] [CrossRef]
- Timokhina, E.; Zinin, V.; Ignatko, I.; Ibragimova, S.; Belotserkovtseva, L.; Strizhakov, A. Matrix metalloproteinases MMP-2 and MMP-9 as markers for the prediction of preeclampsia in the first trimester. Ceska Gynekol. 2021, 86, 228–235. [Google Scholar] [CrossRef]
- Yakovleva, N.; Saprykina, D.; Vasiljeva, E.; Bettikher, O.; Godzoeva, A.; Kazantseva, T.; Zazerskaya, I. Matrix metalloproteinase -12: A marker of preeclampsia? Placenta 2022, 129, 36–42. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin Summary, Number 222. Obstet. Gynecol. 2020, 135, 1492–1495. [Google Scholar] [CrossRef]
- Turbeville, H.R.; Sasser, J.M. Preeclampsia beyond pregnancy: Long-term consequences for mother and child. Am. J. Physiology. Ren. Physiol. 2020, 318, F1315–F1326. [Google Scholar] [CrossRef]
- Lalu, M.M.; Xu, H.; Davidge, S.T. Matrix metalloproteinases: Control of vascular function and their potential role in preeclampsia. Front. Biosci. 2007, 12, 2484–2493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montagnana, M.; Lippi, G.; Albiero, A.; Scevarolli, S.; Salvagno, G.L.; Franchi, M.; Guidi, G.C. Evaluation of metalloproteinases 2 and 9 and their inhibitors in physiologic and pre-eclamptic pregnancy. J. Clin. Lab. Anal. 2009, 23, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Do, N.C.; Vestgaard, M.; Ásbjörnsdóttir, B.; Andersen, L.L.T.; Jensen, D.M.; Ringholm, L.; Damm, P.; Mathiesen, E.R. Home Blood Pressure for the Prediction of Preeclampsia in Women With Preexisting Diabetes. J. Clin. Endocrinol. Metab. 2022, 107, e3670–e3678. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wu, N. Gestational Diabetes Mellitus and Preeclampsia: Correlation and Influencing Factors. Front. Cardiovasc. Med. 2022, 9, 831297. [Google Scholar] [CrossRef] [PubMed]
- Feng, H.; Wang, L.; Zhang, M.; Zhang, Z.; Guo, W.; Wang, X. Ratio of matrix metalloproteinase-2 to -9 is a more accurate predictive biomarker in women with suspected pre-eclampsia. Biosci. Rep. 2017, 37, BSR20160508. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.M.; Li, L.; Zeng, Y.P.; Yao, C.P. Expression of advanced glycation end products, its receptor and matrix metalloproteinase-9 in hypertensive disorders complicating pregnancy. Chin. J. Evid.-Based Cardiovasc. Med. 2019, 11, 90–93. [Google Scholar]
- He, H.; Cai, Y.Q.; Zhou, D.M.; Zheng, C.; Yang, R. Serum levels of matrix metalloproteinase-2, 9 and their inhibitors in patients with preeclampsia. J. Nanjing Med. Univ. (Nat. Sci. Ed.) 2015, 35, 246–248. [Google Scholar]
- Timokhina, E.; Strizhakov, A.; Ibragimova, S.; Gitel, E.; Ignatko, I.; Belousova, V.; Zafiridi, N. Matrix Metalloproteinases MMP-2 and MMP-9 Occupy a New Role in Severe Preeclampsia. J. Pregnancy 2020, 2020, 8369645. [Google Scholar] [CrossRef]
- Nikolov, A.; Popovski, N. Role of Gelatinases MMP-2 and MMP-9 in Healthy and Complicated Pregnancy and Their Future Potential as Preeclampsia Biomarkers. Diagnostics 2021, 11, 480. [Google Scholar] [CrossRef]
- Myers, J.E.; Merchant, S.J.; Macleod, M.; Mires, G.J.; Baker, P.N.; Davidge, S.T. MMP-2 levels are elevated in the plasma of women who subsequently develop preeclampsia. Hypertens. Pregnancy 2005, 24, 103–115. [Google Scholar] [CrossRef]
- Foote, C.A.; Martinez-Lemus, L.A. Uncovering novel roles for matrix metalloproteinases in preeclampsia. Am. J. Physiology. Heart Circ. Physiol. 2017, 313, H687–H689. [Google Scholar] [CrossRef]
- Anacker, J.; Segerer, S.E.; Hagemann, C.; Feix, S.; Kapp, M.; Bausch, R.; Kämmerer, U. Human decidua and invasive trophoblasts are rich sources of nearly all human matrix metalloproteinases. Mol. Hum. Reprod. 2011, 17, 637–652. [Google Scholar] [CrossRef] [Green Version]
- Murray, A.J. Oxygen delivery and fetal-placental growth: Beyond a question of supply and demand? Placenta 2012, 33 (Suppl. S2), e16–e22. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Pre-Eclampsia Group (n = 135) | Control Group (n = 140) | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameters | First Trimester (n = 33) | Second Trimester (n = 33) | Third Trimester (n = 41) | After-Onset (n = 28) | First Trimester (n = 35) | Second Trimester (n = 37) | Third Trimester (n = 43) | After-Onset (n = 25) |
| Age (years) | 34 (32, 38) | 32 (31, 34) | 33 (31, 36) | 33 (31, 35) | 33 (31, 36.5) | 33 (31, 35) | 33 (30, 35.5) | 34 (31, 37) |
| BMI (Kg/m2) | 23.83 (22.66, 27.79) | 23.14 (21.77, 25.71) | 23.44 (22.04, 24.92) | 23.14 (20.83, 24.22) | 23.31 (20.85, 26.67) | 22.94 (20.03, 26.95) | 23.11 (21.09, 23.84) | 22.49 (20.96, 23.79) |
| Nulliparity (n (%)) | 27 (81.8%) | 27 (81.8%) | 34 (82.9%) | 20 (71.4%) | 24 (68.6%) | 27 (73%) | 26 (60.5%) | 12 (48%) |
| Blood Pressure (mmHg) | ||||||||
| SBP | 127 (119, 129) | 126.5 (123, 134.25) | 143 (140, 153.75) | 140 (136.5, 154) | 122 (114, 128) | 121 (116, 126) | 126 (123, 133.5 | 125 (124, 131) |
| DBP | 74 (68, 82) | 74.5 (68, 79.25) | 90 (85.25, 96.75) | 90 (85.5, 98.5) | 70 (66, 76) | 67 (63, 74) | 72 (67, 79) | 76 (71, 83) |
| MAP | 92.67 (84.67, 97.67) | 91.17 (87.5, 96.08) | 106.67 (104.83, 115.17) | 107.33 (101, 117.7) | 87.33 (83, 94.67) | 86 (80.33, 90) | 90 (86.17, 97.17) | 92.33 (87, 97.53) |
| p values of blood pressure | ||||||||
| Ps | 0.329 | 0.002 | 0.000 | 0.000 | ||||
| Pd | 0.163 | 0.004 | 0.000 | 0.000 | ||||
| Pm | 0.154 | 0.001 | 0.000 | 0.000 | ||||
| History (n (%)) | ||||||||
| eclampsia | 0 | 5 (15.2%) | 2 (4.9%) | 3 (10.7%) | 0 | 0 | 0 | 0 |
| GDM | 11 (33.3%) | 13 (39.4%) | 18 (43.9%) | 10 (35.7%) | 0 | 0 | 0 | 0 |
| kidney disease | 1 (3.0%) | 2 (6.1%) | 2 (4.9%) | 1 (3.6%) | 0 | 0 | 0 | 0 |
| Number of cases in subgroups (n (%)) | ||||||||
| Sever | 11 (33.33%) | 13 (39.40%) | 18 (43.90%) | 12 (42.86%) | 0 | 0 | 0 | 0 |
| Mild | 22 (66.67%) | 20 (60.60%) | 23 (56.10%) | 16 (57.14%) | 0 | 0 | 0 | 0 |
| Preterm | 2 (6.06%) | 4 (12.12%) | 10 (24.39) | 12 (42.86%) | 7 (20%) | 4 (10.81%) | 5 (11.63%) | 8 (32%) |
| Term | 31 (93.94%) | 29 (87.88%) | 31 (75.61%) | 16 (57.14%) | 28 (80%) | 33 (89.19%) | 38 (88.37%) | 17 (68%) |
| Indicators | Gestation | Pre-Eclampsia Group (n = 111) | Control Group (n = 144) | Z | P0 | P1 | P2 |
|---|---|---|---|---|---|---|---|
| MMP-2 (ng/mL) | First Trimester | 314.44 (229.6, 346.35) | 332.8 (304.41, 356.98) | −1.154 | 0.249 | 0.146 | 0.000 a 0.795 b 0.001 c 0.011 d 1.000 e 0.138 f |
| Second Trimester | 302.43 (177.69, 351.33) | 228.64 (213.12, 254.7) | 2.053 | 0.040 | |||
| Third Trimester | 337.2 (279.12, 376.4) | 282.52 (236.4, 344.01) | 2.272 | 0.023 | |||
| After-onset | 302.85 (232, 342) | 242 (217.8, 281.2) | 2.585 | 0.010 | |||
| MMP-7 (ng/mL) | First Trimester | 2.35 (1.94, 2.88) | 2.48 (2.13, 2.62) | −0.045 | 0.964 | 1.000 a 0.009 b 0.000 c 0.014 d 0.000 e 0.553 f | 0.000 a 0.795 b 0.001 c 0.011 d 1.000 e 0.138 f |
| Second Trimester | 2.38 (1.87, 2.85) | 1.84 (1.38, 2.74) | 2.001 | 0.045 | |||
| Third Trimester | 3.43 (2.39, 5.82) | 2.56 (1.65, 3.38) | 2.345 | 0.019 | |||
| After-onset | 4.14 (3.37, 6.32) | 3.48 (1.91, 4.16) | 2.350 | 0.019 | |||
| MMP-9 (ng/mL) | First Trimester | 991.88 (841.81, 1075.35) | 845.64 (747.24, 972.36) | 3.148 | 0.002 | 0.979 | 0.000 a 0.000 b 1.000 c 1.000 d 0.002 e 0.000 f |
| Second Trimester | 968.15 (841.81, 1185) | 1220.06 (909.19, 1285.15) | −2.194 | 0.028 | |||
| Third Trimester | 1020.7 (880.71, 1170.25) | 1263 (951.29, 2618.22) | −2.156 | 0.031 | |||
| After-onset | 1066.92 (829.73, 1305.75) | 806 (581.47, 1051) | 2.227 | 0.026 |
| Indicators | AUC | 95% CI | Cut-Off (ng/mL) | Sensitivity (%) | Specificity (%) | PPV (%) | 95% PPV | NPV (%) | 95% NPV | Youden Index | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| First Trimester | |||||||||||
| MMP-2 | 0.583 | 0.444–0.722 | 329.832 | 60.6 | 62.9 | 60.6 | 44–77 | 62.9 | 47–79 | 0.235 | 0.241 |
| MMP-7 | 0.508 | 0.362–0.653 | 2.01 | 68.4 | 82.9 | 68.4 | 53–84 | 59.2 | 43–75 | 0.223 | 0.912 |
| MMP-9 | 0.722 | 0.601–0.843 | 1003.752 | 80.0 | 88.6 | 80.0 | 66–94 | 64.6 | 49–80 | 0.371 | 0.002 |
| Second Trimester | |||||||||||
| MMP-2 | 0.663 | 0.507–0.819 | 294.987 | 60.6 | 97.3 | 95.2 | 78–99 | 73.5 | 59–88 | 0.579 | 0.019 |
| MMP-7 | 0.616 | 0.483–0.749 | 1.53 | 93.9 | 35.1 | 56.4 | 39–73 | 86.7 | 76–98 | 0.291 | 0.096 |
| MMP-9 | 0.653 | 0.521–0.785 | 1078.844 | 72.7 | 64.9 | 64.9 | 49–81 | 72.7 | 58–87 | 0.376 | 0.028 |
| Third Trimester | |||||||||||
| MMP-2 | 0.669 | 0.531–0.808 | 298.673 | 70.0 | 67.7 | 67.7 | 53–82 | 70.0 | 56–84 | 0.377 | 0.023 |
| MMP-7 | 0.675 | 0.538–0.811 | 3.53 | 50.0 | 80.6 | 71.4 | 58–85 | 62.5 | 48–77 | 0.306 | 0.019 |
| MMP-9 | 0.667 | 0.526–0.807 | 1315.878 | 90.0 | 48.4 | 62.8 | 48–78 | 83.3 | 72–94 | 0.384 | 0.025 |
| After-onset | |||||||||||
| MMP-2 | 0.686 | 0.538–0.833 | 289.2 | 62.1 | 86.7 | 81.8 | 68–96 | 70.3 | 52–88 | 0.487 | 0.014 |
| MMP-7 | 0.711 | 0.579–0.843 | 4.07 | 58.6 | 76.7 | 70.8 | 54–88 | 65.7 | 47–84 | 0.353 | 0.005 |
| MMP-9 | 0.678 | 0.538–0.817 | 881.5 | 72.4 | 63.3 | 65.6 | 48–83 | 70.4 | 53–88 | 0.357 | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bahabayi, A.; Yang, N.; Xu, T.; Xue, Y.; Ma, L.; Gu, X.; Wang, Y.; Jia, K. Expression of Matrix Metalloproteinase-2,-7,-9 in Serum during Pregnancy in Patients with Pre-Eclampsia: A Prospective Study. Int. J. Environ. Res. Public Health 2022, 19, 14500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192114500
Bahabayi A, Yang N, Xu T, Xue Y, Ma L, Gu X, Wang Y, Jia K. Expression of Matrix Metalloproteinase-2,-7,-9 in Serum during Pregnancy in Patients with Pre-Eclampsia: A Prospective Study. International Journal of Environmental Research and Public Health. 2022; 19(21):14500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192114500
Chicago/Turabian StyleBahabayi, Ayibaota, Nan Yang, Tong Xu, Yuting Xue, Lijuan Ma, Xunke Gu, Yongqing Wang, and Keke Jia. 2022. "Expression of Matrix Metalloproteinase-2,-7,-9 in Serum during Pregnancy in Patients with Pre-Eclampsia: A Prospective Study" International Journal of Environmental Research and Public Health 19, no. 21: 14500. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192114500