
Inspiratory Muscle Training Improves Aerobic Fitness in Active Children

1
Division of Rehabilitation Technology, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Hualien 970473, Taiwan
2
Department of Physical Therapy, Tzu Chi University, Hualien 970374, Taiwan
*
Author to whom correspondence should be addressed.
Int. J. Environ. Res. Public Health 2022, 19(22), 14722; https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192214722
Submission received: 30 September 2022
/
Revised: 2 November 2022
/
Accepted: 7 November 2022
/
Published: 9 November 2022
(This article belongs to the Special Issue Exercise and Physical Fitness)
Abstract
:Research on the effect of inspiratory muscle training (IMT) on exercise performance is inconsistent. IMT has not been applied to fit child athletes, who are more likely to develop inspiratory muscle fatigue, and, consequently, to benefit from IMT. Methods: Thirty children (mean age: 10.7 ± 1.2 years) were recruited and randomly assigned to a high-intensity (HG), a low-intensity (LG), or a control group (CG). For both training groups, a double-blind procedure was applied. In the HG, 80% of maximal inspiratory pressure (MIP) was used as the level of training intensity. The LG used 30% MIP. Training groups were trained at 6 breaths a set, 4 sets a day, totaling 24 breaths a day for 6 weeks. Exercise capacity outcomes include maximal and submaximal aerobic capacity, as measured as VO2max and distance from six-minute walk test (6MWD). Results show improvement in MIP, VO2max, and 6MWD only in the HG. MIP in the HG significantly increases from 108.7 (100.8–143.3) to 144.4 (130.0–175.6) cmH2O. VO2max in the HG increases from 43.0 (40.5–45) to 53.0 (46–63) mL·kg−1·min−1. The 6MWD increases from 792.0 (737.5–818.0) to 862.0 (798.5–953.5) m. Data are presented as median (interquartile range). No difference is found in the LG or CG. Conclusion: high-intensity IMT increases MIP, maximal, and submaximal exercise capacity in the HG, but no difference is found in the LG or CG. Therefore, high-intensity type of IMT improves aerobic fitness in fit children by appropriately applying inspiratory muscle strength training.
1. Introduction
Ventilation systems are not considered a limiting factor to maximal exercise at sea level because arterial oxygen pressure is generally well-maintained, even during high-level exercise [1]. However, most relevant studies demonstrate that the diaphragm fatigues following high-level exercise [2]. Athletes who have to train at a higher intensity for longer period of time are likely to suffer from diaphragm fatigue. Research shows that diaphragm fatigue induces sympathetically mediated reductions in limb blood flow and can further diminish endurance performance [3].
Inspiratory muscle training has been applied to different populations, ranging from low-fitness groups, such as patients with cardiopulmonary disorders, to high-fitness groups, such as elite athletes. The purpose of inspiratory muscle training is mostly to increase exercise performance, but the effects are inconsistent due to the variant outcomes measured, the task required, and subjects from different levels of breathing fitness. Respiratory muscle fatigue is found during high-intensity exercise (>85% VO2max) and would further limit exercise performance by increased sympathetic vasoconstrictor outflow to limb muscles and the sensation of dyspnea [4]. Diaphragm fatigue is considered present if there is a ≥15% reduction in maximal pressure ability, and is a result of the combination of pressure generating during inspiration and the ratio of inspiration time to total breathing cycle duration [5]. The rationale for a strength type of inspiratory muscle training (IMT) is based on ventilatory demand requiring higher pressure-generating capability during incremental to maximal exercise to produce increased volume and airflow. The strength type of IMT was specifically developed to increase inspiratory strength, and was found to increase diaphragm thickness [6] and aerobic performance [7], as well as relieving the sensation of dyspnea [8]. However, data on the effects of IMT on exercise performance, especially for athletes, are equivocal. The difference in outcomes probably depends on how well the principles of training are applied, the specific type of training, and the nature of subjects that receive the training.
Children have smaller lungs than adults, and women have smaller lungs and airways compared to men. Research on breathing in children is scarce, but evidence shows that work of breathing in females increases more rapidly than males and females present a greater O2 cost of breathing when matched for a relative amount of ventilation [9]. For the same reason, children can suffer more from inspiratory muscle fatigue during high intensity exercise.
Nowadays, young athletes are achieving higher performances in many sports and they probably respond differently to training than adults. If IMT is necessary to prevent or delay inspiratory muscle fatigue, children and athletes would benefit from it most because of their smaller lungs and having to exercise at high intensity, respectively. IMT can prevent or delay fatigue, which provides an athlete with a competitive advantage. Our review of the literature of respiratory muscle training and exercise performance revealed that no single study coupled IMT with maximal aerobic capacity exercise performance for fit child athletes. Therefore, the purpose of this study was to investigate the effect of a strength type of IMT on maximal oxygen uptake (VO2max) in extremely fit child athletes.
2. Materials and Methods
The study was designed to evaluate the effect of a 6 week IMT program on inspiratory muscle strength and exercise performance in fit young boys. To explore the difference in training effects between high- and low-intensity types of IMT, random assignment and double-blind control design were applied. All of the participants were randomly assigned to a high-intensity training group (HG), a low-intensity training group (LG), or a no-training control group (CG). The HG and LG each received 6 weeks of IMT. The CG did not receive any inspiratory training. For both training groups, double-blind control was applied so that the group decision was unknown to the participants and experiment operator. Subjects in both training groups received a personal inspiratory trainer with pressure threshold set at a pre-determined intensity. The intensity setting on the inspiratory trainer was occluded with tape and the intensity was not seen by the subjects.
2.1. Participants
Boys from local elementary sports teams were recruited. The inclusion criteria were as follows: (1) at least 2 years of training experience with the team; and (2) the ongoing minimal sports training amount that the participants received was 90 min/d, for at least 5 days a week.
Thirty regularly trained, non-smoking boy volunteers with normal lung function were studied (FEV1 > 80% of age predicted, FVC > 80% of age predicted, and FEV1/FVC > 70%) [10]. The study was approved by the Institutional Review Board in Tzu Chi Medical Center. Informed consent was obtained from each subject and their guardian.
All subjects assessed for eligibility met the inclusion criteria of the study. The inclusion criteria of a two-year training background and sufficient ongoing training were confirmed by the coaches. Thirty children were randomized before initiating the study protocol. A prior study evaluated the effect of IMT on MIP for healthy subjects in our laboratory, and demonstrated the significant difference of the mean MIP of 20 cmH2O [11]. Based on this difference, and the study objective to realize 80% power with type I error of 0.05, the present study required twenty-one children for the three study groups when using analysis of variance (ANOVA). Hence, the study included thirty boys to account for possible a 30% dropout.
Weight and height were measured, and the body mass index (BMI) was calculated. Body composition was assessed using bioelectrical impedance (Biospace Inbody 3.0 Body Composition Analyzer, Singapore) to determine body fat percentage.
2.2. Outcome Measurements-Inspiratory Muscle Strength
Maximal inspiratory pressure (MIP) was measured at the mouth by a pressure manometer (RPM, Micro, Cardinal Health, Basingstoke, UK). Subjects were seated in a comfortable chair upright with nose clips on. After exhaling to residual volume, subjects placed their lips around a mouthpiece and inspired as forcefully as possible. Repeated measurements were taken at least five times, with a 60 to 120 s rest between trials, until three measurements within 10% variation were obtained. The average of these three measurements was recorded as the subjects’ MIP. MIP is the highest pressure that subjects can generate and represented inspiratory strength.
2.3. Outcome Measurements-Maximal Exercise Capacity
Maximal exercise capacity was assessed using maximal oxygen uptake (VO2max) by having the participants run on an electromechanical treadmill (HP-Cosmos, Quasar Med 4.0, Nussdorf–Traunstein, Germany). The treadmill was programmed for increases in angle of inclination and speed according to the original Bruce protocol. The boys were instructed to avoid vigorous exercise within 2 h of the beginning the test, and not to hold the guardrail during the test. Breath-by-breath gas samples were collected using a fitted facemask and were analyzed throughout the test using open-circuit calorimetry. A two-way breathing valve was attached to the mask, which covered their nose and mouth, and was used to collect the expired air. The air was analyzed continuously for ventilatory and metabolic variables. During the maximal exercise test, physiologic responses were measured using a heart rate (HR) monitor (Polar, Polar Electro, Finland) and a calibrated mobile gas analysis system (Cortex Metamax 3B, Cortex Medical GmbH, Leipzig, Germany). The Cortex Metamax 3B is a valid and reliable system for measuring ventilatory parameters during exercise [12]. VO2max was determined when 2 of the following 3 conditions were reached: (1) respiratory exchange ratio > 1.0; (2) heart rate > 85% of the age-predicted maximum; and (3) the child was exhausted and refused to continue, despite strong verbal encouragement [13]. VO2max was defined as the highest value achieved during the last 30 s before peak or levelling. During the test all subjects were highly motivated and strongly encouraged to continue to run to the maximum workload.
2.4. Outcome Measurements-Submaximal Exercise Capacity
Submaximal exercise capacity was assessed by the six-minute walk test (6MWT), which was conducted according to guidelines recommended in an official ATS statement [14]. Dyspnea, as measured with the visual analogue scale (VAS), peripheral oxygen saturation (SpO2), and pulse rate were measured using pulse oximetry at the start and end of the 6MWT. VAS was measured using a horizontal line, 100 mm in length, anchored by the word descriptors “no dyspnea at all” and “very severe dyspnea” at each end. Subjects were asked to mark on the line the point that represented their perception of their state. The VAS score was determined by measuring in millimeters from the left-hand end of the line to the point that the patient marked. The distance that the subjects covered in 6 min was recorded as the 6MWD. The 6MWD is a functional measurement and represented a submaximal aerobic exercise capacity.
2.5. Inspiratory Muscle Training (IMT) Protocol
Training for both the HG and LG was conducted 5 days per week for 6 weeks. Each daily inspiratory training session consisted of 4 sets of 6 training breaths. Each participant used a personal custom-designed pressure threshold inspiratory muscle trainer, which was a device that provided a pressure threshold load to inspiration so that the participant must generate pressure greater than the load to open the valve for air to enter. Pressure threshold inspiratory trainer with individualized inspiratory training load was pre-set according to the group decision before giving it to the subjects. In the HG, training intensity was 80% of MIP, whereas in the LG, training intensity was 30%. The two training groups performed inspiratory training daily at the beginning of their daily routine sports team practice, completing 4 sets of training required for approximately 10 min. During the first week, the same researcher in this study supervised the training to ensure that there was no difficulty in learning or practicing. After the participants successfully learned the skill to breath against the pressure-loaded trainer, the team coach assumed the supervision. At the end of the third week and in the remaining weeks, every week the researcher remeasured the participants’ MIP and adjusted the pressure threshold to 80% or 30% of the current MIP.
2.6. Statistical Analysis
Our subjects were active children of a similar age and the sample size was small (n = 30). Not all data in this study passed the Shapiro–Wilk test for normality assumptions, therefore, non-parametric statistics were adopted for the following analysis. All data are presented as the median (interquartile range), unless otherwise explained. Anthropometric data (body mass, height, weight, body mass index (BMI), and body fat percentage), inspiratory muscle strength data (MIP), maximal exercise capacity (VO2max), and submaximal exercise capacity (6MWD) were compared using Kruskal–Wallis one-way analysis of variance (ANOVA) on ranks. When significant differences are found, Dunn’s test was used for pairwise comparison. Within-group change between pre- and post-IMT was evaluated using the Wilcoxon signed-rank test. Significance levels for all tests were established as two-tailed p values less than 0.05.
3. Results
Study Group Characteristics
Thirty boys were randomly assigned into three groups (HG: n = 9, mean ± SD age 12.1 ± 0.3 y, height 149.2 ± 9.3 cm, weight 44.1 ± 9.5 kg; LG: n = 10, age 10.3 ± 1.3 y, height 140.4 ± 12.5 cm, weight 34.9 ± 9.7 kg; and CG: n = 11, age 10.0 ± 0.6 y, height 138.9 ± 8.2 cm, weight 36.4 ± 9.1 kg). The participants completed 6 weeks of inspiratory muscle training (from both training groups) and all participants finished both pre- and post-training measurements. All participants were highly motivated and maintained their original daily sports training routine during our experiment period. The sports training was twice a day, one hour before and one hour after school. Subjects were preparing for a national middle school contest when the experiment was conducted. The randomization procedure results in significant differences in age among groups, and the following Dunn’s test shows that the age in the HG is significantly greater than both the LG and CG (Table 1). For height and weight, differences are found in the Kruskal–Wallis ANOVA test, but the following Dunn’s test shows that there is no difference in any pairwise comparison. There are no differences in other physiological characteristics such as BMI or body fat percentage.
For the pre-IMT outcome variables, results from the Kruskal–Wallis test show that there is significant group difference in VO2max and 6MWD (p < 0.05). A post hoc Dunn’s test was used for pairwise comparison. VO2max is significantly greater in the LG when compared to the HG. The 6MWD is found to be smaller in the CG when compared to both the HG and LG (Table 2).
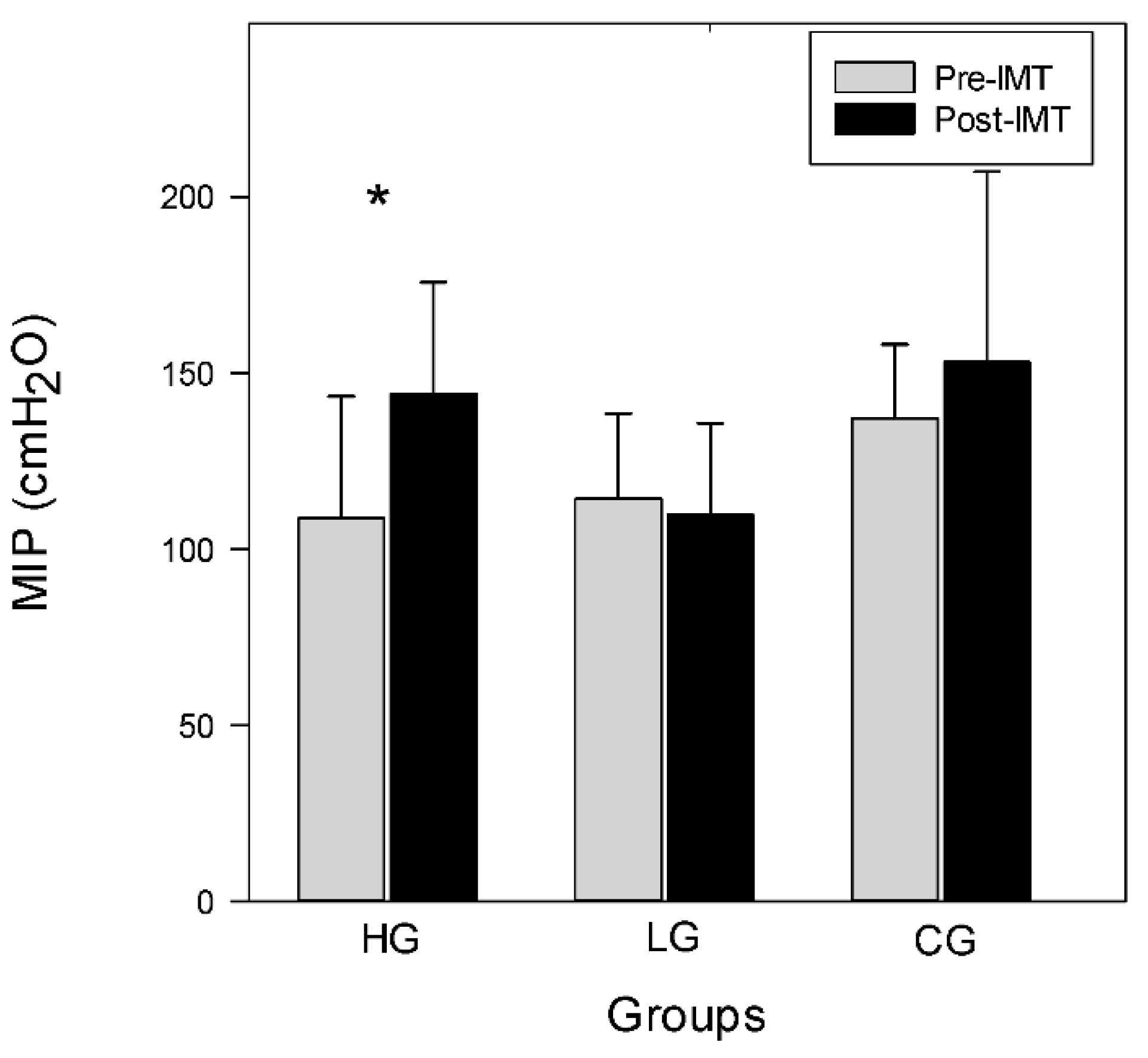
For the within group post-IMT outcome variables, results from the Wilcoxon signed-rank test show significant improvement in MIP, VO2max, and 6MWD in the HG (p < 0.05). MIP, VO2max, and 6MWD do not change in the LG or CG. The detailed outcome data are presented in Table 2. MIP in the HG increases from 108.7 pre-training (100.8–143.3) to 144.4 (130.3–175.6) cmH2O post-training (p < 0.05). MIP in the LG and CG does not change, ranging from 114.4 (83.8–138.5) and 137.0 (95.0–158.0) pre-training to 109.7 (96.3–135.7) and 153.0 (105.0–207.0) cmH2O post-training, respectively, as shown in Figure 1. This suggests that 6 weeks of high-intensity IMT results in an increase in MIP, and low-intensity IMT does not result in any change in MIP.
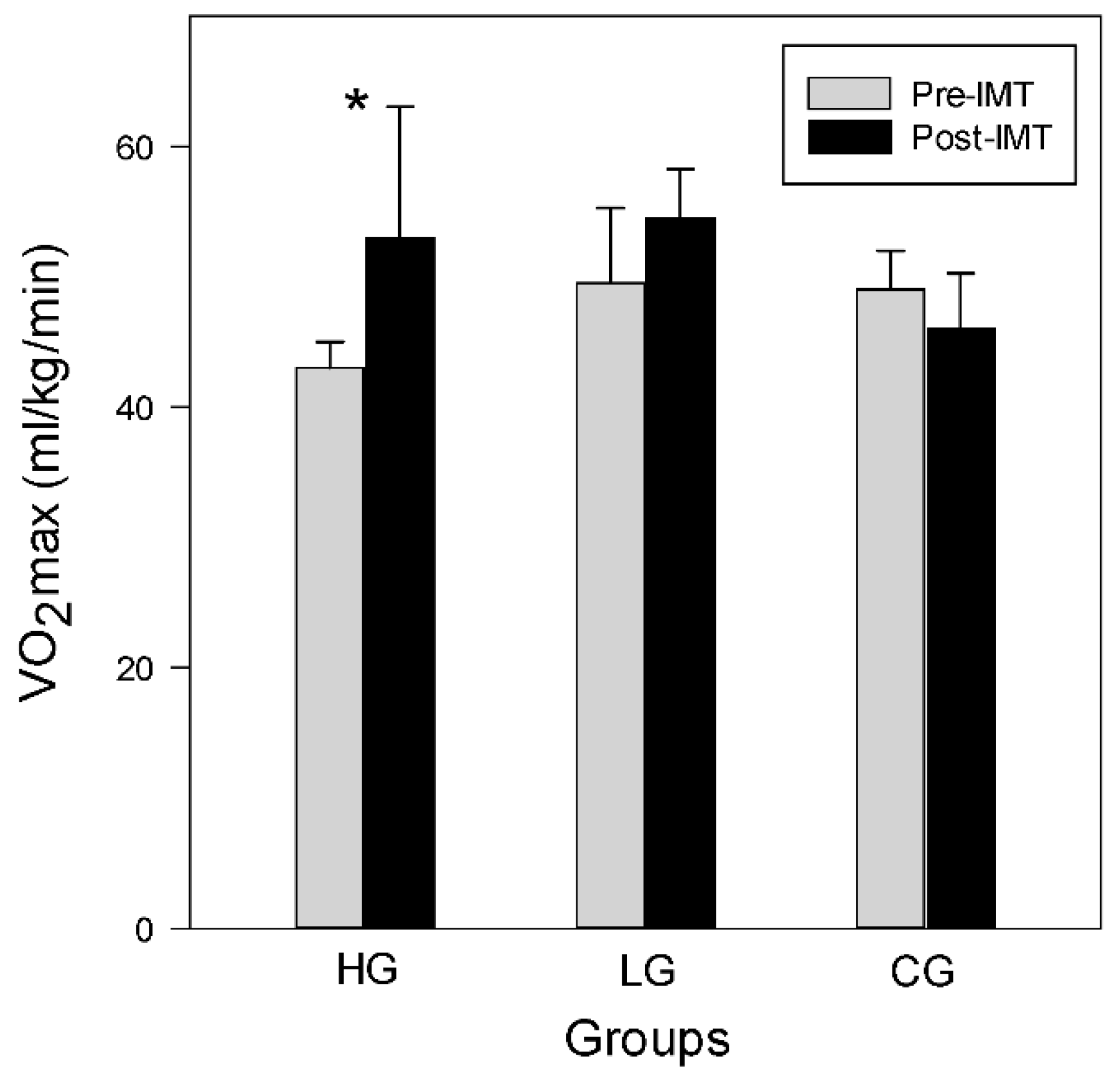
VO2max, expressed as mL·kg−1·min−1, increases only in the HG after 6 weeks of training and remains unchanged in both the LG and CG. The Wilcoxon signed-rank test shows that the HG significantly improves VO2max, which in the HG ranges from 43.0 (40.5–45.0) pre-training to 53.0 (46.0–63.0) mL·kg−1·min−1 post-training (p < 0.05). VO2max in the LG and CG do not change, ranging from 49.5 (45.7–55.3) pre-training to 54.5 (49.7–58.3) mL·kg−1·min−1 post-training in the LG, and 49.0 (45.0–52.0) pre-training to 46.0 (42.8–50.3) mL·kg−1·min−1 post-training in the CG, as shown in Figure 2.
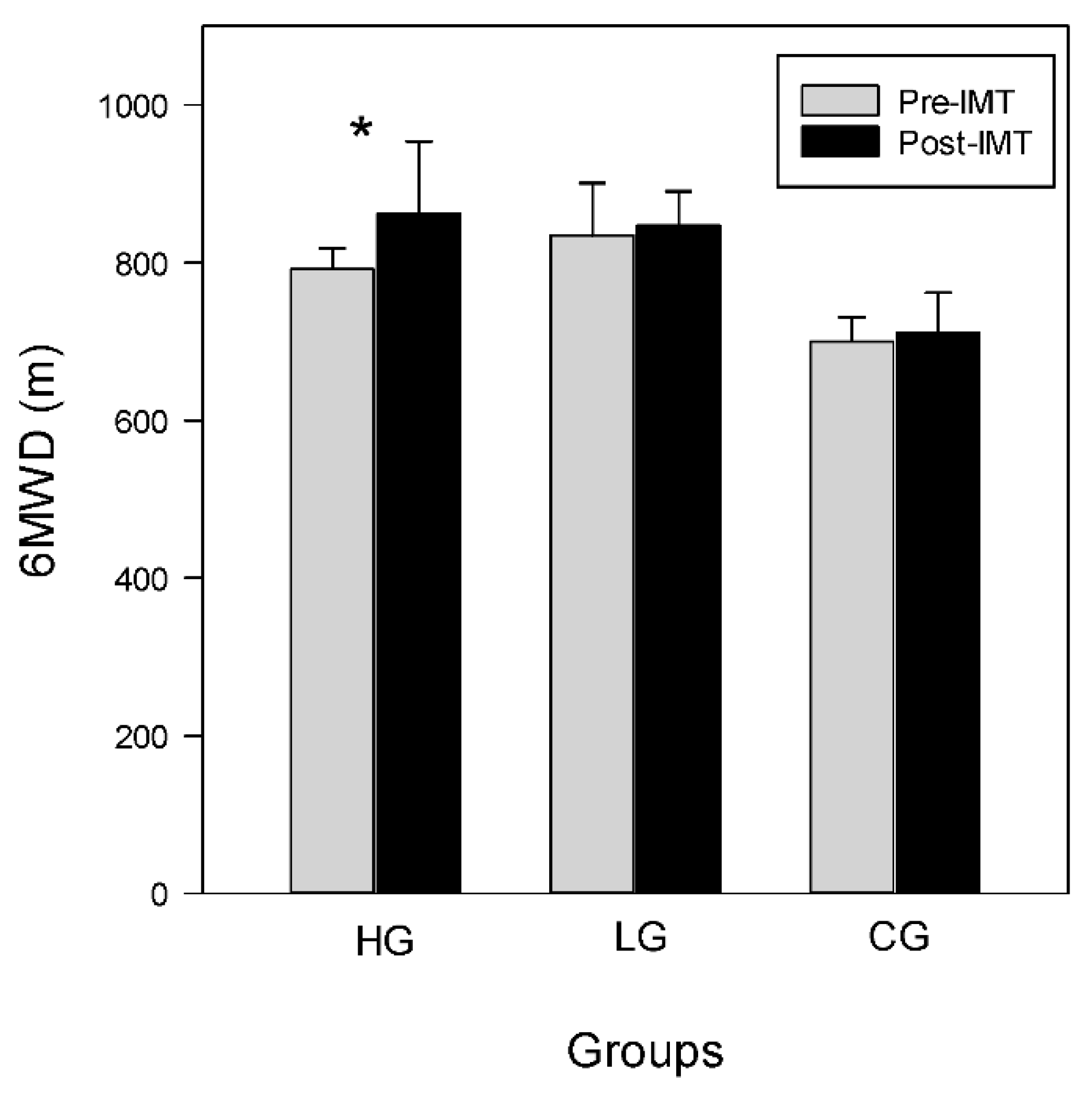
Wilcoxon signed-rank test shows that the 6MWD improves significantly in the HG. The 6MWD in the HG improves from 792.0 (737.5–818.0) pre-training to 862.0 (798.5–953.5) m post-training (p < 0.05). However, the 6MWD in the LG and CG remain unchanged, which range from 834.5 (797.5–900.8) pre-training to 847.5 (812.8–890.5) m post-training, and from 726.0 (626.0–750.0) pre-training to 713.0 (688.0–751.0) m post-training, respectively, as shown in Figure 3. There is no difference in HR, SpO2, and VAS after training among groups during the 6MWT (Table 3).
The results suggest high-intensity IMT improves inspiratory muscle strength, maximal, and submaximal aerobic exercise capacity, as seen in the MIP, VO2max, and 6MWD values, respectively. In contrast, low-intensity IMT does not show any effects on MIP, VO2max, or 6MWD.
4. Discussion
This study aimed at evaluating the impacts of IMT on inspiratory strength, maximal, and submaximal exercise capacity, hypothesizing that high-intensity, but not low-intensity, IMT could produce improvement. Random assignment and double-blind control design were applied to compare the effect. The findings verify our hypotheses and show that high-intensity IMT improves inspiratory strength, and maximal and submaximal exercise capacity among physically fit child athletes. Low-intensity IMT does not improve inspiratory strength, and no difference in exercise capacity is found.
4.1. Effects of Inspiratory Muscle Training on MIP
Maximal inspiratory pressure is used for the assessment of inspiratory muscle strength. However, one difficulty is that this test requires subjects to understand and follow the instructions and to perform with maximum effort. The normative data for children are limited, and for youth athletes are unavailable. The MIP values found in the current study are greater than children of a similar age [15]. The possible reason could be that our subjects are physically fit child athletes. Tests of MIP require understanding, cooperation, and patience, and we carefully instructed and monitored the performance. The requirement was that each subject had to perform the tests multiple times with enough rest in between and the highest three scores of tests had to be within 10% variation. This was to avoid inconsistent high outlier data due to accidental biting of the mouthpiece. We have not found studies that compare the MIP between healthy subjects and athletes at this young age.
Our high intensity IMT results in an average of a 35% increase in MIP in the HG; low-intensity training does not affect MIP. The training outcome confirms training specificity theory, because inspiratory muscles are morphologically and functionally skeletal muscles and would respond to appropriate physiological stimuli. Training received in the HG is a model of strength training, which is high intensity (80% of MIP), low repetition (six breaths a set), aiming at an increase in maximal strength (MIP). The amount of training effect is similar to reports on healthy adult athletes [16], suggesting that children at this age respond to inspiratory training stimuli as effectively as adults. This positive finding is also consistent with previous studies about weight training for youths [17].
4.2. Effects of Inspiratory Muscle Training on Maximal Exercise Capacity VO2max
Normally trained young athletes have higher VO2max than their untrained peers, and VO2max increases in boys through childhood and adolescence; VO2max values of >60 mL/kg/min have been observed [18]. Compared to the above review, our participants (mean age 10.7 y; median age 10.4 y) are relatively younger and present an average pre-training VO2max of 48.1 mL/kg/min. However, if compared to the data from the literature on VO2max in Chinese boys [19], which show the average VO2max of 30 mL/kg/min from boys aged 8–12 years, we believe that VO2max of 48.1 mL/kg/min pre-training from our participants is able to represent a group of trained boy athletes appropriate to their age.
The finding in which an increase in VO2max improves after IMT in the HG suggests an improvement in maximal aerobic exercise capacity. The VO2max in the HG is 44.9 ± 8.2 (mean ± SD) pre-IMT and 53.4 ± 9.5 post-IMT, which represents a 21% increase. There is considerable evidence that inspiratory muscles develop fatigue during intense exercise, considering the significant demand for O2 and the high work of breathing that occurs during heavy endurance exercise [20]. It has been established that respiratory muscle fatigue occurs during exercise at an intensity of at least 85% of maximal oxygen consumption [21]. The outcome of inspiratory muscle fatigue is that fatigue causes a sympathetically mediated vasoconstriction of the lower limbs and further results in peripheral muscle fatigue, known as inspiratory muscle metaboreflex [22]. The mechanism involves neural and cardiovascular change, which impairs exercise performance. IMT induces the delay in activating this mechanism, decreasing the onset of peripheral muscle fatigue [20] and the sensation of dyspnea [11]. The improvement in our study is in agreement with a previous finding by Holm et al. [23], which demonstrates that IMT improves VO2max in a group of fit cyclists. Training builds stronger inspiratory muscles, which helps delay the onset of inspiratory muscle fatigue; the possible sympathetic reflex, which may lead to reduced blood flow in the peripheral muscle, is, thus, prevented. Hajghabari et al. [24] published a systemic review of the effects of respiratory muscle training on the performance of athletes and concluded that respiratory muscle training improved performance. In their conclusion, the authors offered the important explanation for inconsistent outcomes in IMT studies: not enough progression in training intensity. The present training protocol uses 80% of MIP as the training intensity, 24 breaths per day over 6 weeks of training, and with weekly adjustment for training intensity. To delay possible inspiratory muscle fatigue, and to prevent further metabolic reflex, it is necessary to apply overload and specificity training principles for improving strength.
4.3. Effects of Inspiratory Muscle Training on Submaximal Exercise Capacity
The 6MWD test is a reliable and valid functional test for assessing exercise tolerance and endurance in healthy children [13]. We chose it because it represents the most suitable and convenient method for assessing the submaximal level of functional exercise capacity. Our results show that IMT improves the 6MWD in the HG, without a significant difference in the change of VAS or SpO2, meaning that our participants in the HG are able to walk longer distances with the same level of breathlessness and oxygen saturation. Our 6WMD is greater than published data on “healthy children” with comparable age [25], confirming the greater fitness of our participants. After IMT, the 6MWD even improves 10% (786 ± 63 m pre-training to 863 ± 97 m post-training, data presented as mean ± SD) in the HG, while there is no change in the LG (847 ± 63 m pre-training to 852 ± 63 m post-training, data presented as mean ± SD).
4.4. Limitations
The first limitation of this study is an insufficient number of subjects, which causes several variables to not pass the Shapiro–Wilk normality Test. We chose to run non-parametric statistical analysis instead for all the dependent variables. It is found that parametric tests are more powerful than non-parametric tests only if all of the assumptions underlying the parametric test are met [26]. Not passing the normality test and small sample sizes both are appropriate conditions in which to use a non-parametric analysis [27]. Second, randomization with small sample results in difference in age among groups. Therefore, the influence of development needs to be considered. Post-puberty boys show greater maximal isometric force than pre-puberty boys [28], and we recognize that this may have influenced our results. Third, we do not differentiate the type of sport team among participants. For a study with small subject number, background endurance type sports, i.e., running, or intermittent type sports, i.e., tennis, could possibly lead to different responses to IMT and affect our results of exercise performance. Thus, larger studies on subgroups representing children with certain sports backgrounds are needed.
4.5. Practical Applications
Alongside regular athletic training, researchers and coaches can use additional high-intensity IMT to improve VO2max for already fit athletes. This research shows that a strength-type of inspiratory muscle training results in significant increases in both maximal and submaximal exercise capacity. However, an endurance-type of inspiratory muscle training does not have the same effects.
5. Conclusions
This study demonstrates that in addition to regular sports training, additional high-intensity IMT improves inspiratory muscle function, accompanied by enhanced exercise capacity, in fit child athletes. At ten minutes per day, this protocol is feasible and efficient. This study is the first to provide evidence that child athletes can respond to IMT. Child athletes benefit from high-intensity IMT. Maximal inspiratory muscle pressure and both maximal and submaximal exercise capacity improve in response to high-intensity IMT. However, low-intensity IMT does not cause changes in MIP or exercise capacity.
Author Contributions
C.-H.L. and C.-W.L.: experiment and methodology. C.-H.H.: funding, analysis, and writing. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Taiwan Ministry of Science and Technology (NSC 96-2413-H-320-003-MY3).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Tzu Chi Medical Center (IRB095-18, issued on 18 January 2006).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Powers, S.K.; Martin, D.; Dodd, S. Exercise-Induced Hypoxaemia in Elite Endurance Athletes. Sport. Med. 1993, 16, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Katayama, K.; Iwamoto, E.; Ishida, K.; Koike, T.; Saito, M. Inspiratory muscle fatigue increases sympathetic vasomotor outflow and blood pressure during submaximal exercise. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2012, 302, R1167–R1175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harms, C.A.; Wetter, T.J.; Croix, C.M.S.; Pegelow, D.F.; Dempsey, J.A. Effects of respiratory muscle work on exercise performance. J. Appl. Physiol. 2000, 89, 131–138. [Google Scholar] [CrossRef]
- Wells, G.D.; Norris, S.R. Assessment of physiological capacities of elite athletes & respiratory limitations to exercise performance. Paediatr. Respir. Rev. 2009, 10, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Bellemare, F.; Grassino, A. Effect of pressure and timing of contraction on human diaphragm fatigue. J. Appl. Physiol. 1982, 53, 1190–1195. [Google Scholar] [CrossRef] [PubMed]
- Enright, S.J.; Unnithan, V.B.; Heward, C.; Withnall, L.; Davies, D.H. Effect of High-Intensity Inspiratory Muscle Training on Lung Volumes, Diaphragm Thickness, and Exercise Capacity in Subjects Who Are Healthy. Phys. Ther. 2006, 86, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Hartz, C.S.; Sindorf, M.A.; Lopes, C.R.; Batista, J.; Moreno, M.A. Effect of inspiratory muscle training on performance of handball athletes. J. Hum. Kinet. 2018, 63, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.H.; Martin, A.D.; Davenport, P.W. Effects of Inspiratory Strength Training on the Detection of Inspiratory Loads. Appl. Psychophysiol. Biofeedback 2009, 34, 17–26. [Google Scholar] [CrossRef]
- Archiza, B.; Leahy, M.G.; Kipp, S.; Sheel, A.W. An integrative approach to the pulmonary physiology of exercise: When does biological sex matter? Eur. J. Appl. Physiol. 2021, 121, 2377–2391. [Google Scholar] [CrossRef]
- Murray, C.; Foden, P.; Lowe, L.; Durrington, H.; Custovic, A.; Simpson, A. Diagnosis of asthma in symptomatic children based on measures of lung function: An analysis of data from a population-based birth cohort study. Lancet Child Adolesc. Health 2017, 1, 114–123. [Google Scholar] [CrossRef]
- Huang, C.-H.; Yang, G.-G.; Wu, Y.-T.; Lee, C.-W. Comparison of Inspiratory Muscle Strength Training Effects Between Older Subjects With and Without Chronic Obstructive Pulmonary Disease. J. Formos. Med. Assoc. 2011, 110, 518–526. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, D.J.; Wong, P. Validity, reliability and stability of the portable Cortex Metamax 3B gas analysis system. Eur. J. Appl. Physiol. 2012, 112, 2539–2547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, A.M.; Yin, J.; Yu, C.C.W.; Tsang, T.; So, H.K.; Wong, E.; Chan, D.; Hon, E.K.L.; Sung, R. The six-minute walk test in healthy children: Reliability and validity. Eur. Respir. J. 2005, 25, 1057–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Mellies, U.; Stehling, F.; Dohna-Schwake, C. Normal values for inspiratory muscle function in children. Physiol. Meas. 2014, 35, 1975. [Google Scholar] [CrossRef] [Green Version]
- Karsten, M.; Ribeiro, G.S.; Esquivel, M.S.; Matte, D.L. The effects of inspiratory muscle training with linear workload devices on the sports performance and cardiopulmonary function of athletes: A systematic review and meta-analysis. Phys. Ther. Sport 2018, 34, 92–104. [Google Scholar] [CrossRef]
- Faigenbaum, A. State of the art reviews: Resistance training for children and adolescents: Are there health outcomes? Am. J. Lifestyle Med. 2007, 1, 190–200. [Google Scholar] [CrossRef]
- Rowland, T.W. Evolution of maximal oxygen uptake in children. Pediatr. Fit. 2007, 50, 200–209. [Google Scholar] [CrossRef]
- Wong, T.W.; Yu, T.S.; Wang, X.R.; Robinson, P. Predicted maximal oxygen uptake in normal Hong Kong Chinese schoolchildren and those with respiratory diseases. Pediatr. Pulmonol. 2001, 31, 126–132. [Google Scholar] [CrossRef]
- Perlovitch, R.; Gefen, A.; Elad, D.; Ratnovsky, A.; Kramer, M.R.; Halpern, P. Inspiratory muscles experience fatigue faster than the calf muscles during treadmill marching. Respir. Physiol. Neurobiol. 2007, 156, 61–68. [Google Scholar] [CrossRef]
- Johnson, B.D.; Babcock, M.A.; Suman, O.E.; Dempsey, J.A. Exercise-induced diaphragmatic fatigue in healthy humans. J. Physiol. 1993, 460, 385–405. [Google Scholar] [CrossRef] [PubMed]
- Wetter, T.J.; Harms, C.A.; Nelson, W.B.; Pegelow, D.F.; Dempsey, J.A. Influence of respiratory muscle work on VO(2) and leg blood flow during submaximal exercise. J. Appl. Physiol. 1999, 87, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Holm, P.; Sattler, A.; Fregosi, R.F. Endurance training of respiratory muscles improves cycling performance in fit young cyclists. BMC Physiol. 2004, 4, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- HajGhanbari, B.; Yamabayashi, C.; Buna, T.R.; Coelho, J.D.; Freedman, K.D.; Morton, T.A.; Palmer, S.A.; Toy, M.A.; Walsh, C.; Sheel, A.W.; et al. Effects of respiratory muscle training on performance in athletes: A systematic review with meta-analyses. J. Strength Cond. Res. 2013, 27, 1643–1663. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, S.; Hildenbrand, F.F.; Treder, U.; Fischler, M.; Keusch, S.; Speich, R.; Fasnacht, M. Reference values for the 6-minute walk test in healthy children and adolescents in Switzerland. BMC Pulm. Med. 2013, 13, 49. [Google Scholar] [CrossRef] [Green Version]
- Tomkins, C.; Hall, C. An introduction to non-parametric statistics for health scientists. Univ. Alta. Health Sci. J. 2006, 3, 20–26. [Google Scholar]
- Mishra, P.; Pandey, C.M.; Singh, U.; Keshri, A.; Sabaretnam, M. Selection of appropriate statistical methods for data analysis. Ann. Card. Anaesth. 2019, 22, 297. [Google Scholar] [CrossRef]
- Sadres, E.; Eliakim, A.; Constantini, N.; Lidor, R.; Falk, B. The Effect of Long-Term Resistance Training on Anthropometric Measures, Muscle Strength, and Self Concept in Pre-Pubertal Boys. Pediatr. Exerc. Sci. 2001, 13, 357–372. [Google Scholar] [CrossRef]
Figure 1.
Pre- and post-training MIP among groups. Data are shown as median+ 75th percentile. * p < 0.05.
Figure 1.
Pre- and post-training MIP among groups. Data are shown as median+ 75th percentile. * p < 0.05.

Figure 2.
Pre- and post-training VO2max among groups. Data are shown as median+ 75th percentile. * p < 0.05.
Figure 2.
Pre- and post-training VO2max among groups. Data are shown as median+ 75th percentile. * p < 0.05.

Figure 3.
Pre- and post-training 6MWD among groups. Data are shown as median+ 75th percentile. * p < 0.05.
Figure 3.
Pre- and post-training 6MWD among groups. Data are shown as median+ 75th percentile. * p < 0.05.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Comparisons of demographics and anthropometric characteristic among groups.
| Total | HG | LG | CG | p-Value | |
|---|---|---|---|---|---|
| N | 30 | 9 | 10 | 11 | |
| Age (years) | 10.4 (9.7–12.1) | 12.3 (11.7–12.2) | 9.7 (9.5–11.6) * | 9.8 (9.6–10.4) * | p < 0.05 |
| Height (cm) | 141.1 (135.4–150.0) | 149.0 (141.1–153.9) | 137.9 (130.5–147.9) | 137.8 (132.3–147.5) | p < 0.05 |
| Weight (kg) | 35.0 (30.2–44.6) | 43.2 (36.4–51.4) | 32.1 (29.3–39.2) | 30.9 (29.7–42.6) | p < 0.05 |
| BMI (kg/m2) | 18.3 (16.4–20.4) | 19.4 (17.7–21.4) | 16.9 (15.7–18.8) | 17.3 (16.2–20.9) | 0.19 |
| Body fat (%) | 16.7 (13.1–22.0) | 16.7 (13.6–23.7) | 14.4 (11.5–20.2) | 17.5 (14.7–26.3) | 0.42 |
Data are presented as median (interquartile range). BMI, body mass index. * p < 0.05 when compared to HG.
Table 2.
Inspiratory strength, maximal exercise capacity, and submaximal exercise capacity before and after IMT among groups.
Table 2.
Inspiratory strength, maximal exercise capacity, and submaximal exercise capacity before and after IMT among groups.
| Dependent Variables | HG | LG | CG | Between Group p Value |
|---|---|---|---|---|
| MIP, cmH2O | ||||
| Pre | 108.7 (100.8–143.3) | 114.3 (83.8–138.5) | 137.0 (95.0–158.0) | p = 0.49 |
| Post | 144.4 (130.0–175.6) | 109.7 (96.3–135.7) | 153.0 (105.0–207.0) | |
| Within group p value | p < 0.05 | p = 0.19 | p = 0.88 | |
| VO2max, mL/kg/min | ||||
| Pre | 43.0 (40.5–45.0) | 49.5 (45.8–55.3) * | 49.0 (45.0–52.0) | p < 0.05 |
| Post | 53.0 (46.0–63.0) | 54.5 (49.7–58.3) | 46.0 (42.8–50.3) | |
| Within group p value | p < 0.05 | p = 0.19 | p = 0.43 | |
| 6 MWD, m | ||||
| Pre | 792.0 (737.5–818.0) | 834.5 (797.5–900.8) | 726.0 (626.0–750.0) *# | p < 0.01 |
| Post | 862.0 (798.5–953.5) | 847.5 (812.8–890.5) | 713.0(688.0–751.0) | |
| Within group p value | p < 0.05 | p = 0.79 | p = 0.76 |
Data are presented as median (interquartile range). *: p < 0.05 when compared to HG. #: p< 0.05 when compared to LG.
Table 3.
Difference in HR, SpO2, and VAS during 6MWT before and after IMT among groups.
| Variables/Groups | HG | LG | CG | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Beginning of 6MWT | End of 6MWT | Difference | Beginning of 6MWT | End of 6MWT | Difference | Beginning of 6MWT | End of 6MWT | Difference | |
| Pre-IMT | |||||||||
| HR (beats) | 96 (84–100) | 134 (126–164) | 50 (35–64) | 89 (84–94) | 151 (134–158) | 56 (47–72) | 98 (90–113) | 123 (109–154) | 29 (24–57) |
| SpO2 (%) | 98 (98–99) | 98 (98–99) | −1 (−1–1) | 99 (98–99) | 98 (98–98) | 0 (−1–0) | 98 (98–100) | 98 (98–98) | 0 (−1–1) |
| VAS (mm) | 0 (0–0) | 20 (15–35) | 20 (15–35) | 0 (0–0) | 30 (18–45) | 30 (15–30) | 0 (0–0) | 40 (30–50) | 30 (23–50) |
| Post- IMT | |||||||||
| HR (beats) | 93 (90–97) | 146 (136–176) | 74 (46–84) | 82 (71–91) | 146 (137–166) | 69 (61–85) | 107 (105–115) | 153 (143–173) | 54 (37–57) |
| SpO2 (%) | 98 (98–98) | 98 (97–98) | 0 (−1–1) | 98 (98–99) | 99 (97–99) | 0 (−1–2) | 98 (98–98) | 98 (97–99) | 0 (−1–1) |
| VAS (mm) | 0 (0–0) | 35 (15–40) | 35 (15–40) | 0 (0–1.25) | 40 (21–40) | 35 (20–40) | 0 (0–0) | 40 (26–41) | 40 (25–43) |
Data are presented as median (interquartile range).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lin, C.-H.; Lee, C.-W.; Huang, C.-H. Inspiratory Muscle Training Improves Aerobic Fitness in Active Children. Int. J. Environ. Res. Public Health 2022, 19, 14722. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192214722
AMA Style
Lin C-H, Lee C-W, Huang C-H. Inspiratory Muscle Training Improves Aerobic Fitness in Active Children. International Journal of Environmental Research and Public Health. 2022; 19(22):14722. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192214722
Chicago/Turabian StyleLin, Ching-Hsin, Chih-Wei Lee, and Chien-Hui Huang. 2022. "Inspiratory Muscle Training Improves Aerobic Fitness in Active Children" International Journal of Environmental Research and Public Health 19, no. 22: 14722. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192214722
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.