
Can Nutritional Status in Adults Be Influenced by Health Locus of Control?
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Health Locus of Control and BMI
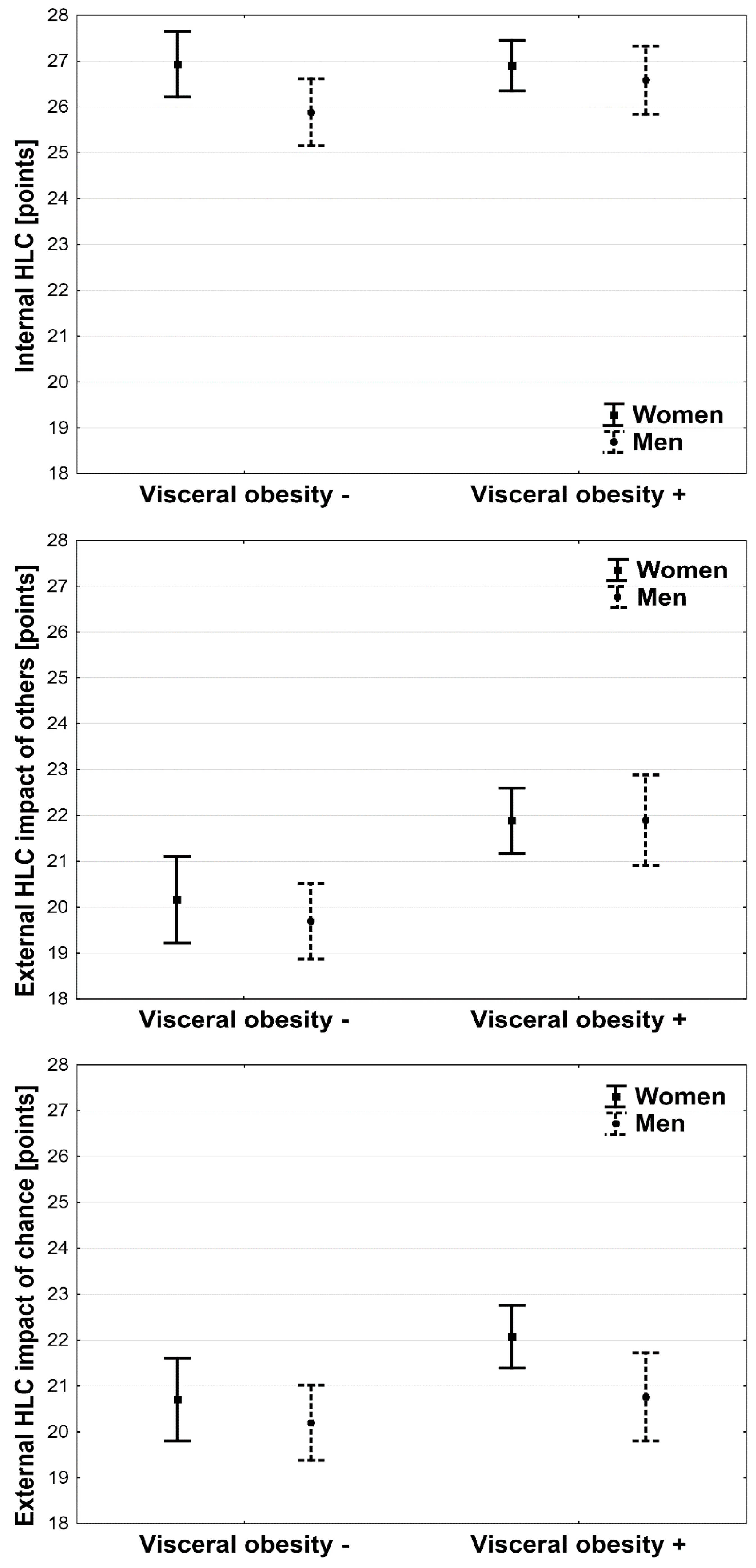
3.2. Health Locus of Control and Visceral Obesity
3.3. Univariable and Multivariable Ordinal Logistic Regression for Overweight and Obesity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnson, N.B.; Hayes, L.D.; Brown, K.; Hoo, E.C.; Ethier, K.A.; Centers for Disease Control and Prevention (CDC). CDC National Health Report: Leading causes of morbidity and mortality and associated behavioral risk and protective factors—United States, 2005–2013. MMWR Suppl. 2004, 63, 327. [Google Scholar]
- Shiozawa, M.; Kaneko, H.; Itoh, H.; Morita, K.; Okada, A.; Matsuoka, S.; Kiriyama, H.; Kamon, T.; Fujiu, K.; Michihata, N.; et al. Association of Body Mass Index with Ischemic and Hemorrhagic Stroke. Nutrients 2021, 13, 2343. [Google Scholar] [CrossRef]
- Linaker, C.H.; D’Angelo, S.; Syddall, H.E.; Harris, E.C.; Cooper, C.; Walker-Bone, K. Body Mass Index (BMI) and Work Ability in Older Workers: Results from the Health and Employment after Fifty (HEAF) Prospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 1647. [Google Scholar] [CrossRef] [Green Version]
- Flegal, K.M.; Carroll, M.D.; Ogden, C.L.; Curtin, L.R. Prevalence and trends in obesity among US adults, 1999–2008. JAMA 2010, 303, 235–241. [Google Scholar] [CrossRef] [Green Version]
- James, W.P.T. The epidemiology of obesity: The size of the problem. J. Intern. Med. 2008, 263, 336–352. [Google Scholar] [CrossRef]
- Rotter, J.B. Generalized expectancies for internal versus external control of reinforcement. Psychol. Monogr. 1966, 80, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Wallston, B.S.; Wallston, K.A.; Kaplan, G.D.; Maides, A. The development and validation of the health related locus of control (HLC) scale. J. Consul. Clin. Psychol. 1976, 44, 580–585. [Google Scholar] [CrossRef]
- Levenson, H. Activism and powerful others: Distinctions within the concept of internal-external control. J. Pers. Assess. 1974, 38, 377–383. [Google Scholar] [CrossRef]
- Norman, P.; Bennett, P.; Smith, C.; Murphy, S. Health locus of control and leisure-time exercise. Pers. Individ. Dif. 1997, 23, 769–774. [Google Scholar] [CrossRef]
- Kudo, Y.; Satoh, T.; Kido, S.; Ishibashi, M.; Miyajima, E.; Watanabe, M.; Miki, T.; Tsunoda, M.; Aizawa, Y. The degree of workers’ use of annual health checkups results among Japanese workers. Ind. Health 2008, 46, 223–232. [Google Scholar] [CrossRef] [Green Version]
- AbuSabha, R.; Achterberg, C. Review of self-efficacy and locus of control for nutrition and health-related behavior. J. Am. Diet. Assoc. 1997, 97, 1122–1132. [Google Scholar] [CrossRef]
- Von Ah, D.; Ebert, S.; Ngamvitroj, A.; Park, N.; Kang, D.H. Predictors of health behaviours in college students. J. Adv. Nurs. 2004, 48, 463–474. [Google Scholar] [CrossRef]
- Nuccitelli, C.; Valentini, A.; Caletti, M.T.; Caselli, C.; Mazzella, N.; Forlani, G.; Marchesini, G. Sense of coherence, self-esteem, and health locus of control in subjects with type 1 diabetes mellitus with/without satisfactory metabolic control. J. Endocrinol. Investig. 2017, 41, 307–314. [Google Scholar] [CrossRef]
- Náfrádi, L.; Nakamoto, K.; Schulz, P.J. Is patient empowerment the key to promote adherence? A systematic review of the relationship between self-efficacy, health locus of control and medication adherence. PLoS ONE 2017, 12, e0186458. [Google Scholar] [CrossRef] [Green Version]
- Anastasiou, C.A.; Fappa, E.; Karfopoulou, E.; Gkza, A.; Yannakoulia, M. Weight loss maintenance in relation to locus of control: The MedWeight study. Behav. Res. Ther. 2015, 71, 40–44. [Google Scholar] [CrossRef]
- Cobb-Clark, D.A.; Kassenboehmer, S.C.; Schurer, S. Healthy habits: The connection between diet, exercise, and locus of control. J. Econ. Behav. Organ. 2014, 98, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Wallston, B.S.; Wallston, K.A. Locus of control and health: A review of the literature. Health Educ. Monogr. 1978, 6, 107–117. [Google Scholar] [CrossRef]
- Allison, K.R. Theoretical issues concerning the relationship between perceived control and preventive health behavior. Health Educ. Res. 1991, 6, 141–151. [Google Scholar] [CrossRef]
- Sandler, I.N.; Lakey, B. Locus of control as a stress moderator: The role of control perceptions and social support. Am. J. Community Psychol. 1982, 10, 65–80. [Google Scholar] [CrossRef]
- Benassi, V.A.; Sweeney, P.D.; Dufour, C. Is there a relation between locus of control orientation and depression? J. Abnorm. Psychol. 1988, 97, 357–367. [Google Scholar] [CrossRef]
- Yeoh, S.H.; Tam, C.L.; Wong, C.P.; Bonn, G. Examining Depressive Symptoms and Their Predictors in Malaysia: Stress, Locus of Control, and Occupation. Front. Psychol. 2017, 8, 1411. [Google Scholar] [CrossRef]
- Holt, C.L.; Clark, E.M.; Kreuter, M.W. Weight locus of control and weight-related attitudes and behaviors in an over-weight population. Addict. Behav. 2001, 26, 329–340. [Google Scholar] [CrossRef]
- Gale, C.R.; Batty, G.D.; Deary, I.J. Locus of control at age 10 years and health outcomes and behaviors at age 30 years: The 1970 British cohort study. Psychosom. Med. 2008, 70, 397–403. [Google Scholar] [CrossRef]
- Galanos, A.N.; Strauss, R.P.; Pieper, C.F. Sociodemographic correlates of health beliefs among black and white community dwelling elderly individuals. Int. J. Aging Hum. Dev. 1994, 38, 339–350. [Google Scholar] [CrossRef]
- Cebolla, A.; Botella, C.; Galiana, L.; Fernández-Aranda, F.; Toledo, E.; Corella, D.; Salas-Salvadó, J.; Fitó, M.; Romaguera, D.; Wärnberg, J.; et al. Psychometric properties of the Weight Locus of Control Scale (MWLCS): Study with Spanish individuals of different anthropometric nutritional status. Eat. Weight Disord. 2020, 25, 1533–1542. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation on Obesity. 1997. Available online: https://apps.who.int/iris/handle/10665/63854 (accessed on 24 August 2022).
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome. 2005. Available online: https://www.idf.org/e-library/consensus-statements/60-idfconsensus-worldwide-definitionof-the-metabolic-syndrome (accessed on 24 August 2022).
- Wallston, K.A.; Wallston, B.S.; DeVellis, R. Development of the Multidimensional Health Locus of Control (MHLC) scales. Health Educ. Monogr. 1978, 6, 160–170. [Google Scholar] [CrossRef]
- Juczyński, Z. Narzędzia Pomiaru w Promocji i Psychologii Zdrowia. Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego; Practest: Warszawa, Poland, 2001; pp. 36–40. [Google Scholar]
- Wallston, K.A. The validity of the Multidimensional Health Locus of Control Scales. J. Health Psychol. 2005, 10, 623–631. [Google Scholar] [CrossRef] [Green Version]
- Torres, S.J.; Nowson, C.A. Relationship between stress, eating behavior, and obesity. Nutrition 2007, 23, 887–894. [Google Scholar] [CrossRef] [Green Version]
- Duplaga, M.; Grysztar, M. Nutritional Behaviors, Health Literacy, and Health Locus of Control of Secondary Schoolers in Southern Poland: A Cross-Sectional Study. Nutrients 2021, 13, 4323. [Google Scholar] [CrossRef]
- Chavez, E.L.; Michaels, A.C. Evaluation of the health locus of control for obesity treatment. Psychol. Rep. 1980, 47, 709–710. [Google Scholar] [CrossRef]
- Radcliff, Z.; Al Ghriwati, N.; Derlan, C.L.; Velazquez, E.; Halfond, R.; Corona, R. The relationship between Latina/o youth’s internal health locus of control, cultural factors, and body mass index. J. Lat. Psychol. 2018, 6, 190–203. [Google Scholar] [CrossRef]
- Walls, H.L.; Stevenson, C.E.; Mannan, H.R.; Abdullah, A.; Reid, C.M.; McNeil, J.J.; Peeters, A. Comparing trends in BMI and waist circumference. Obesity 2011, 19, 216–219. [Google Scholar] [CrossRef]
- Dalton, M.; Cameron, A.J.; Zimmet, P.Z.; Shaw, J.E.; Jolley, D.; Dunstan, D.W.; Welborn, T.A.; AusDiab Steering Committee. Waist circumference, waist-hip ratio and body mass index and their correlation with cardiovascular disease risk factors in Australian adults. J. Intern. Med. 2003, 254, 555–563. [Google Scholar] [CrossRef]
- Perdue, T.O.; Schreier, A.; Swanson, M.; Neil, J.; Carels, R. Majority of female bariatric patients retain an obese identity 18–30 months after surgery. Eat. Weight Disord. 2018, 25, 357–364. [Google Scholar] [CrossRef]
- Bernier, M.; Avard, J. Self-efficacy, outcome, and attrition in weight-reduction program. Cogn. Ther. Res. 1986, 10, 319–338. [Google Scholar] [CrossRef]
- Nir, Z.; Neumann, L. Relationship among self-esteem, internal-external locus of control, and weight change after participation in a weight reduction program. J. Clin. Psychol. 1995, 51, 482–490. [Google Scholar] [CrossRef]
- Saltzer, E.B. The Weight locus of control (WLOC) scale: A specific measure for obesity research. J. Pers. Assess. 1982, 46, 620–628. [Google Scholar] [CrossRef]
- Tobias, L.L.; MacDonald, M.L. Internal locus of control and weight loss: An insufficient condition. J. Consult. Clin. Psychol. 1977, 45, 647–653. [Google Scholar] [CrossRef]
- Nir, Z.; Neumann, L. Self-esteem and internal-external locus of control, and their relationship to weight reduction. J. Clin. Pers. 1991, 47, 568–575. [Google Scholar] [CrossRef]
- van de Putte, E.M.; Engelbert, R.H.; Kuis, W.; Sinnema, G.; Kimpen, J.L.; Uiterwaal, C.S. Chronic fatigue syndrome and health control in adolescents and parents. Arch. Dis. Child. 2005, 90, 1020–1024. [Google Scholar] [CrossRef] [Green Version]
- Asadi-Pooya, A.A.; Schilling, C.A.; Glosser, D.; Tracy, J.I.; Sperling, M.R. Health locus of control in patients with epilepsy and its relationship to anxiety, depression, and seizure control. Epilepsy Behav. 2007, 11, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.C.; Preveza, E.; Papandreou, K.; Prevezas, N. Locus of control among spinal cord injury patients with different levels of posttraumatic stress disorder. Psychiatry Res. 2007, 152, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Neymotin, F.; Nemzer, L.R. Locus of Control and Obesity. Front. Endocrinol. 2014, 5, 159. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.M.; Mack, D.E.; Grattan, K.P. Understanding motivation for exercise: A self-determination theory perspective. Can. Psychol. 2008, 49, 250–256. [Google Scholar] [CrossRef]
- Tucker, C.M.; Marsiske, M.; Rice, K.G.; Nielson, J.J.; Herman, K. Patient-centered culturally sensitive health care: Model testing and refinement. Health Psychol. 2011, 30, 342–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallston, K.A.; Stein, M.J.; Smith, K.A. Form C of the MHLC Scales: A condition-specific measure of locus of control. J. Pers. Assess. 1994, 63, 534–553. [Google Scholar] [CrossRef]
- Wallston, K.A.; Malcarne, V.L.; Flores, L.; Hansdottir, I.; Smith, C.A.; Stein, M.J.; Weisman, M.H.; Clements, P.J. Does god deter-mine your health? The god locus of health control scale. Cognit. Ther. Res. 1999, 23, 131–142. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [Green Version]
- Pasick, R.J.; D’onofrio, C.N.; Otero-Sabogal, R. Similarities and differences across cultures: Questions to inform a third generation for health promotion research. Health Educ. Q. 1996, 23, 142–161. [Google Scholar] [CrossRef]
- Lee, Y.-S.; Chia, M.; Komar, J. A Systematic Review of Physical Activity Intervention Programs in ASEAN Countries: Efficacy and Future Directions. Int. J. Environ. Res. Public Health 2022, 19, 5357. [Google Scholar] [CrossRef]
- Liuccio, M.; Caciolli, A. Campaigns against smoking: A review of the last ten years in Italy. Ann. Ig. Med. Prev. Comunita 2015, 27, 657–664. [Google Scholar] [CrossRef]
- Dorgeat, E.; Adeleye, A.; Lifford, K.J.; Edwards, A. Effectiveness of technological interventions to improve healthcare communication with children with long-term conditions: A systematic review and meta-analysis of randomised controlled trials. Patient Educ. Couns. 2022, 105, 1411–1426. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Normal Weight N = 347 | Overweight N = 221 | Obesity N = 176 | p for Trend | |
|---|---|---|---|---|
| Age [years] | 32 ± 10 | 36 ± 17 | 43 ± 13 | <0.001 |
| • Women | 33 ± 11 | 40 ± 11 | 45 ± 12 | <0.001 |
| • Men | 29 ± 9 | 33 ± 12 | 41 ± 14 | <0.001 |
| Higher education [N; %] | 142; 41.2 | 49; 22.3 | 30; 17.3 | <0.001 |
| • Women | 97; 41.1 | 22; 20.4 | 16; 15.1 | <0.001 |
| • Men | 45; 41.3 | 27; 24.1 | 14; 20.9 | <0.01 |
| Marital status—living alone [N; %] | 203; 60.2 | 89; 42.2 | 57; 34.1 | <0.001 |
| • Women | 119; 52.2 | 33; 32.3 | 32; 31.4 | <0.001 |
| • Men | 84; 77.1 | 56; 51.4 | 25; 38.5 | <0.001 |
| Alcohol consumption [N; %] | 248; 71.5 | 160; 72.4 | 113; 64.2 | 0.13 |
| • Women | 151; 64.0 | 61; 56.5 | 58; 53.7 | 0.06 |
| • Men | 97; 87.4 | 99; 87.6 | 55; 80.9 | 0.27 |
| Smoking [N; %] | 157; 45.2 | 125; 56.6 | 107; 60.8 | <0.001 |
| • Women | 98; 41.5 | 55; 50.9 | 62; 57.4 | <0.01 |
| • Men | 59; 53.1 | 70; 62.0 | 45; 66.2 | 0.07 |
| Active in sport [N; %] | 114; 32.8 | 64; 29.0 | 47; 26.7 | 0.13 |
| • Women | 67; 28.4 | 22; 20.4 | 25; 23.1 | 0.20 |
| • Men | 47; 42.3 | 42; 37.2 | 22; 32.4 | 0.22 |
| Women | Men | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Univariable | OR | −95% CI | +95% CI | z | p | OR | −95% CI | +95% CI | z | p |
| Age [each 5 years] | 1.42 | 1.31 | 1.54 | 8.39 | <0.001 | 1.33 | 1.21 | 1.46 | 5.99 | <0.001 |
| Higher education | 1.40 | 0.94 | 2.08 | 1.67 | 0.10 | 1.19 | 0.75 | 1.88 | 0.75 | 0.46 |
| Marital status—living alone | 0.91 | 0.64 | 1.31 | −0.49 | 0.62 | 0.84 | 0.55 | 1.29 | −0.79 | 0.43 |
| Smoking | 0.84 | 0.59 | 1.19 | −0.99 | 0.32 | 1.32 | 0.86 | 2.03 | 1.28 | 0.20 |
| Alcohol consumption | 0.70 | 0.49 | 1.00 | −1.96 | 0.05 | 0.71 | 0.38 | 1.33 | −1.07 | 0.29 |
| Active in sport | 0.74 | 0.49 | 1.12 | −1.40 | 0.16 | 0.74 | 0.47 | 1.14 | −1.35 | 0.18 |
| Internal HLC [high] | 0.91 | 0.64 | 1.30 | −0.50 | 0.62 | 1.11 | 0.72 | 1.72 | 0.47 | 0.64 |
| External HLC with the impact of others [high] | 1.80 | 1.26 | 2.56 | 3.25 | <0.01 | 1.86 | 1.20 | 2.88 | 2.80 | <0.01 |
| External HLC with the impact of chance [high] | 1.59 | 1.10 | 2.22 | 2.47 | <0.05 | 1.01 | 0.65 | 1.57 | 0.05 | 0.96 |
| Multivariable | OR | −95% CI | +95% CI | z | p | OR | −95% CI | +95% CI | z | P |
| Age [each 5 years] | 1.40 | 1.29 | 1.52 | 8.02 | <0.001 | 1.32 | 1.20 | 1.46 | 5.78 | <0.001 |
| External HLC with the impact of others [high] | 1.53 | 1.06 | 2.22 | 2.26 | 0.05 | 1.61 | 1.02 | 2.53 | 2.05 | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gruszka, W.; Owczarek, A.J.; Glinianowicz, M.; Bąk-Sosnowska, M.; Chudek, J.; Olszanecka-Glinianowicz, M. Can Nutritional Status in Adults Be Influenced by Health Locus of Control? Int. J. Environ. Res. Public Health 2022, 19, 15513. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192315513
Gruszka W, Owczarek AJ, Glinianowicz M, Bąk-Sosnowska M, Chudek J, Olszanecka-Glinianowicz M. Can Nutritional Status in Adults Be Influenced by Health Locus of Control? International Journal of Environmental Research and Public Health. 2022; 19(23):15513. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192315513
Chicago/Turabian StyleGruszka, Wojciech, Aleksander J. Owczarek, Mateusz Glinianowicz, Monika Bąk-Sosnowska, Jerzy Chudek, and Magdalena Olszanecka-Glinianowicz. 2022. "Can Nutritional Status in Adults Be Influenced by Health Locus of Control?" International Journal of Environmental Research and Public Health 19, no. 23: 15513. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192315513