
Tegumentary Leishmaniasis in Northeastern Italy from 2017 to 2020: A Neglected Public Health Issue
 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
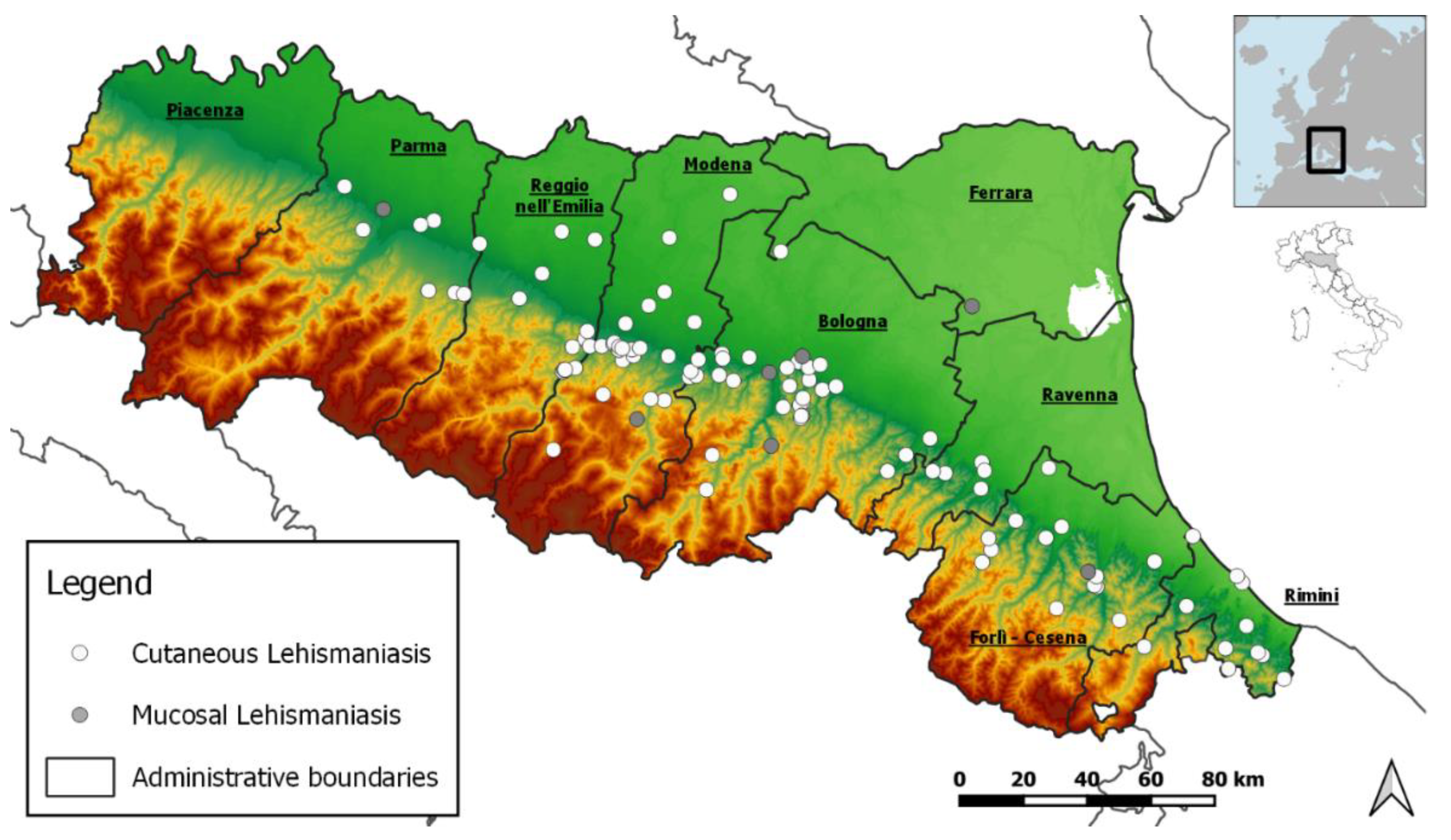
2.1. Study Area
2.2. Case Definition
2.3. Surveillance of Tegumentary Leishmaniasis in Italy and in RER
2.4. Skin_Leish_RER Network
2.5. Diagnosis of Tegumentary Leishmaniasis
2.6. Data Collection
2.7. Statistical Analysis
3. Results
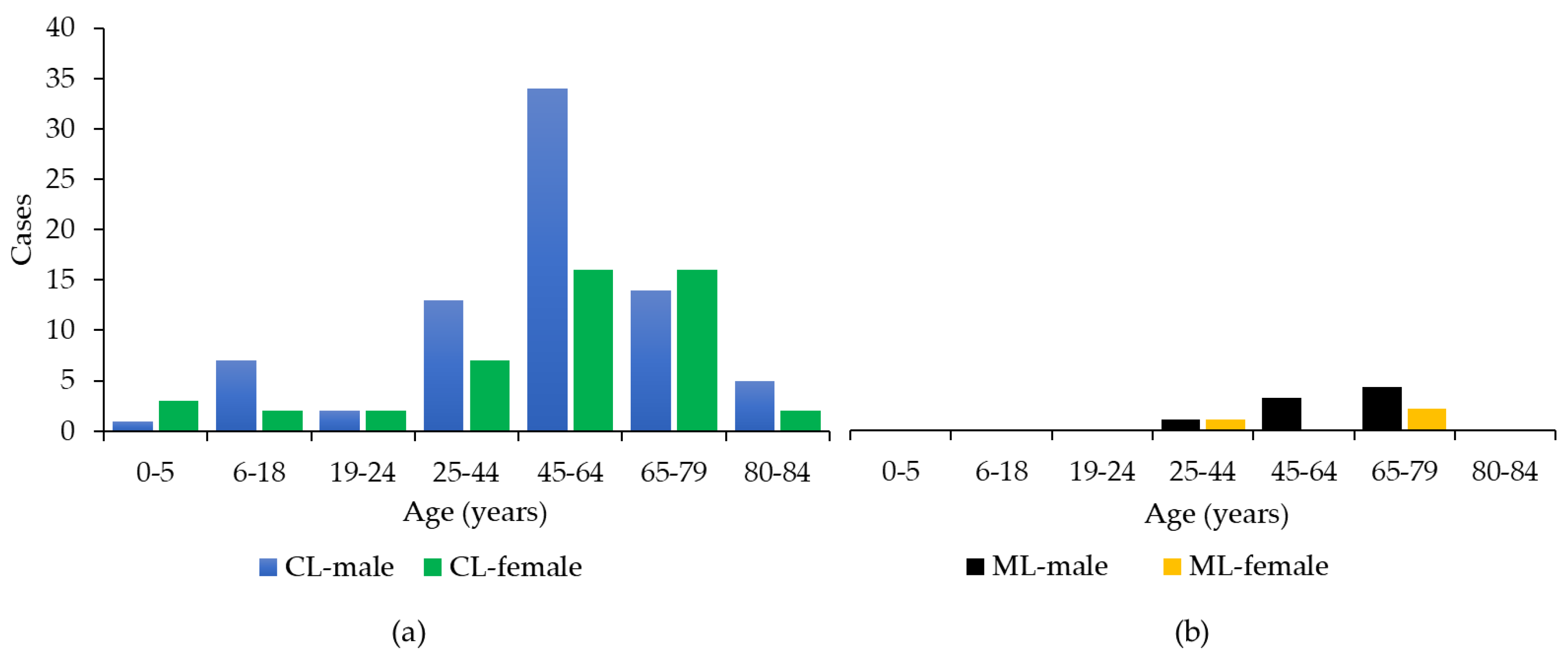
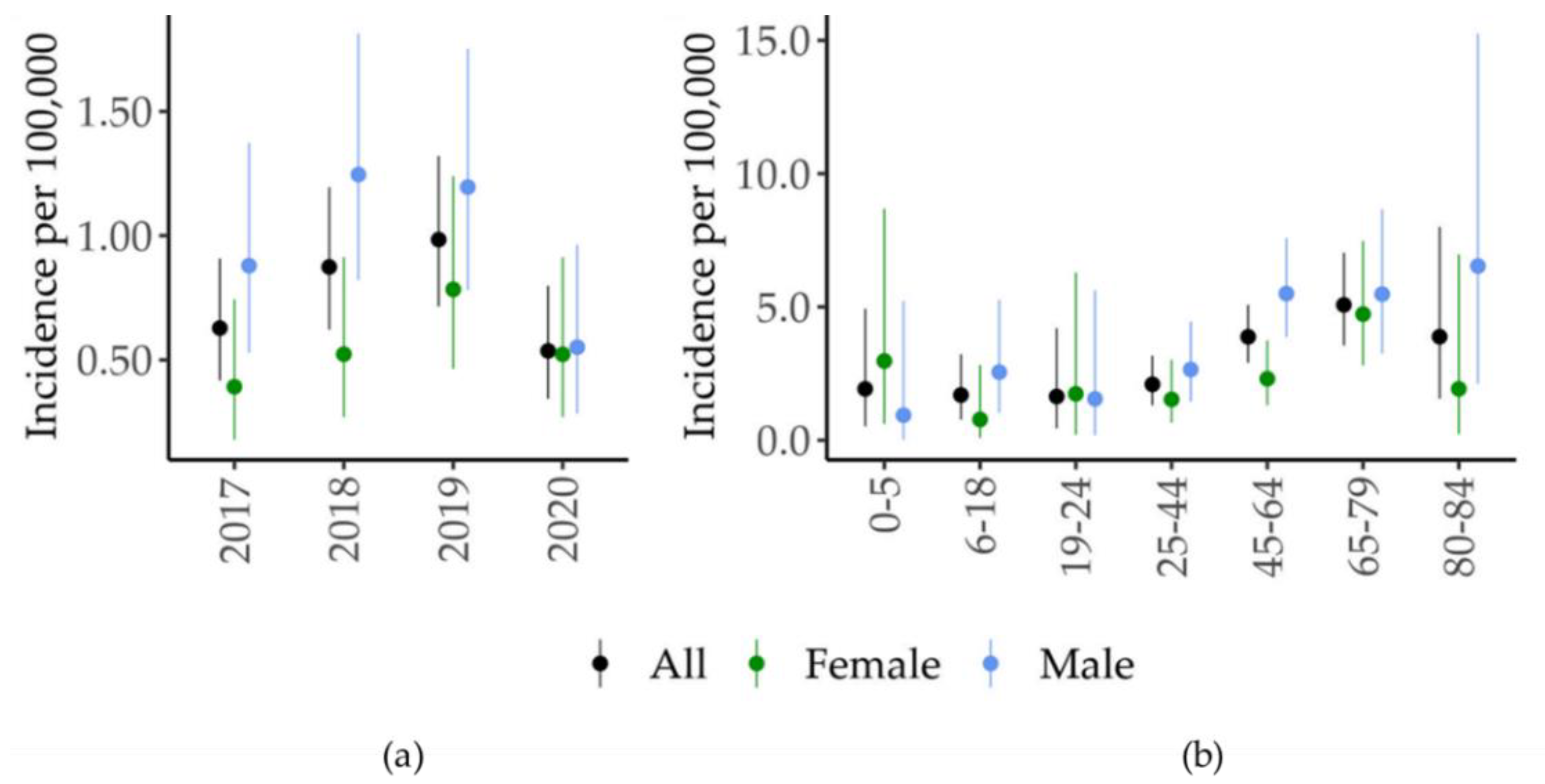
3.1. Case Surveillance
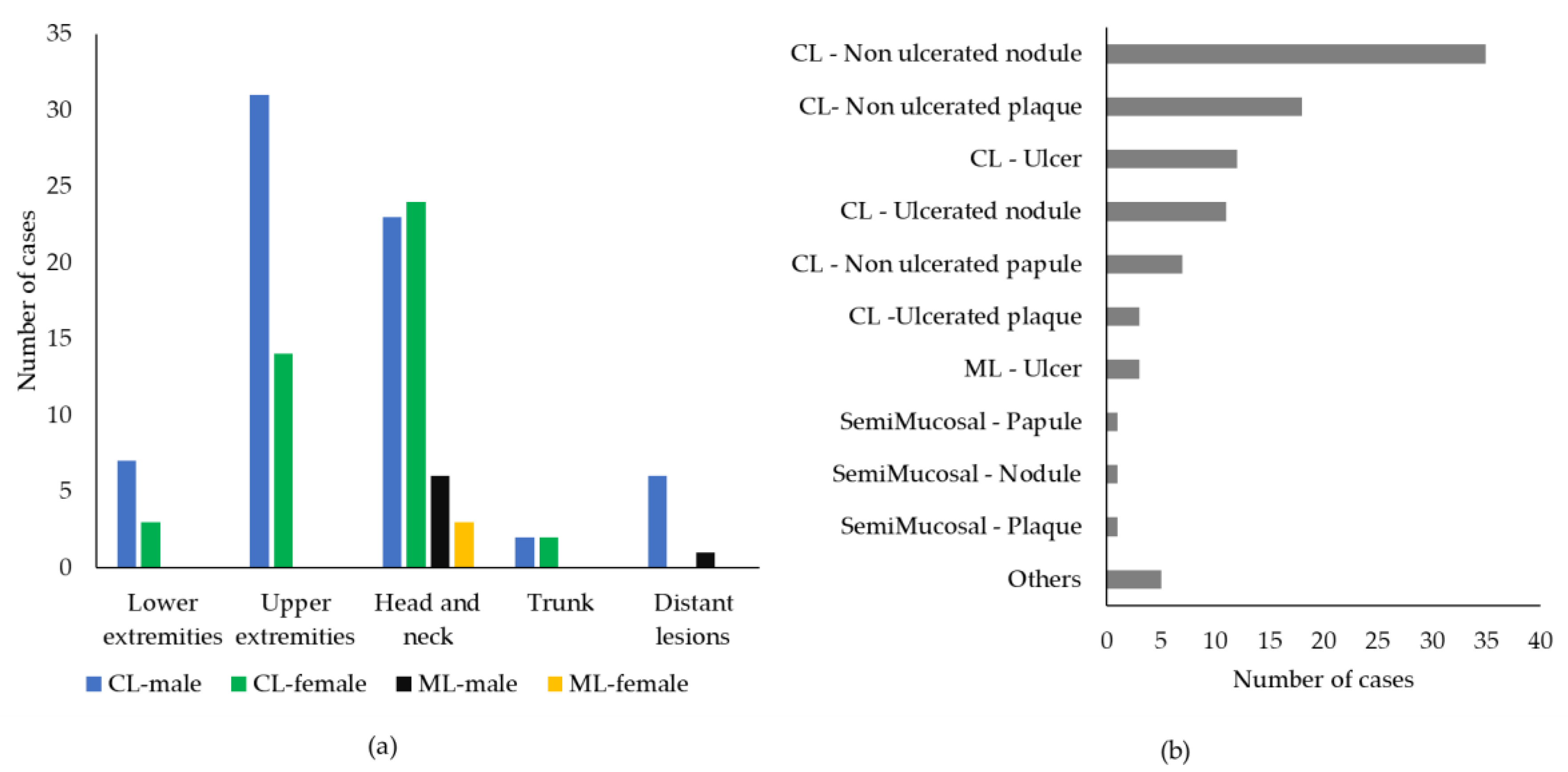
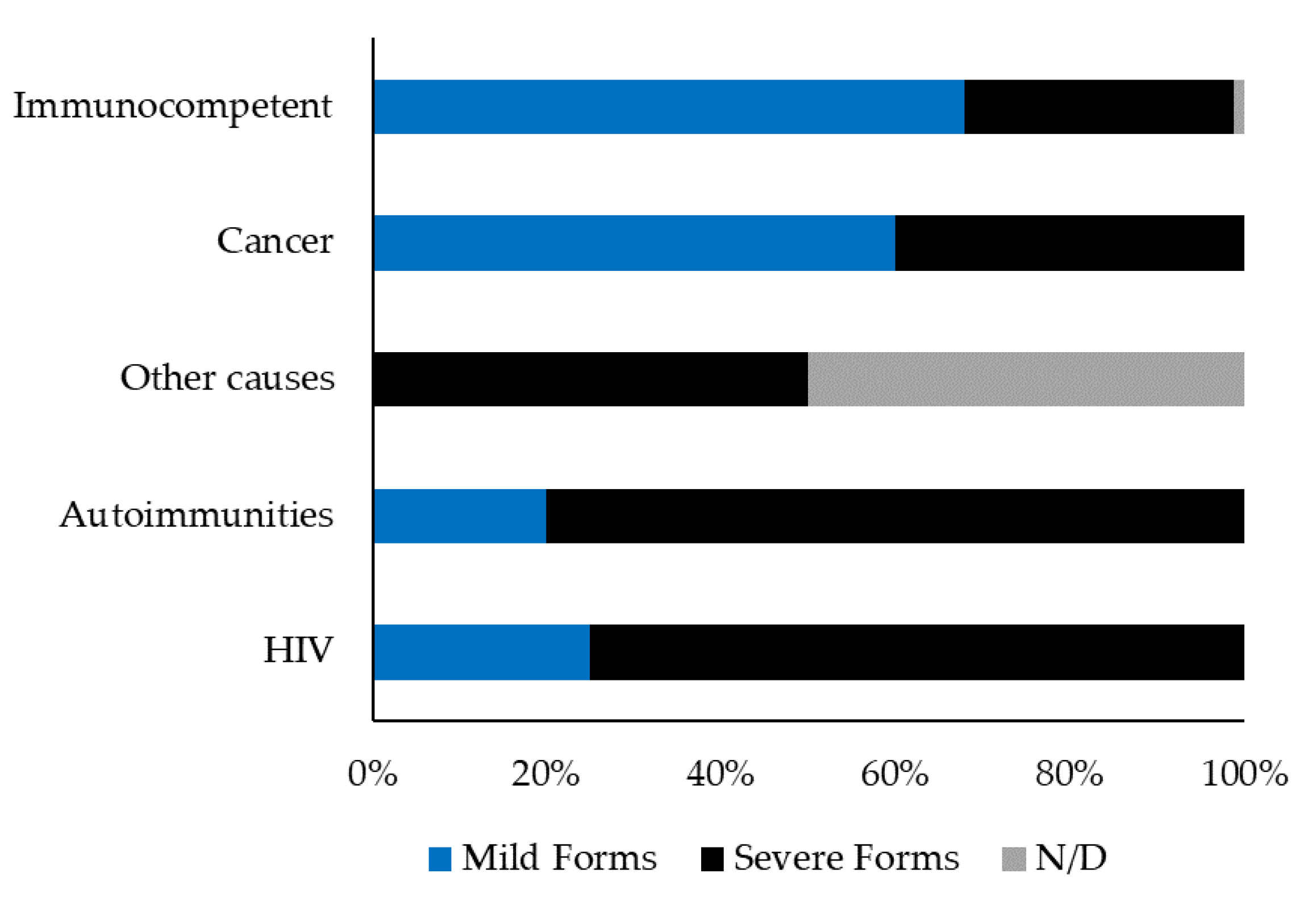
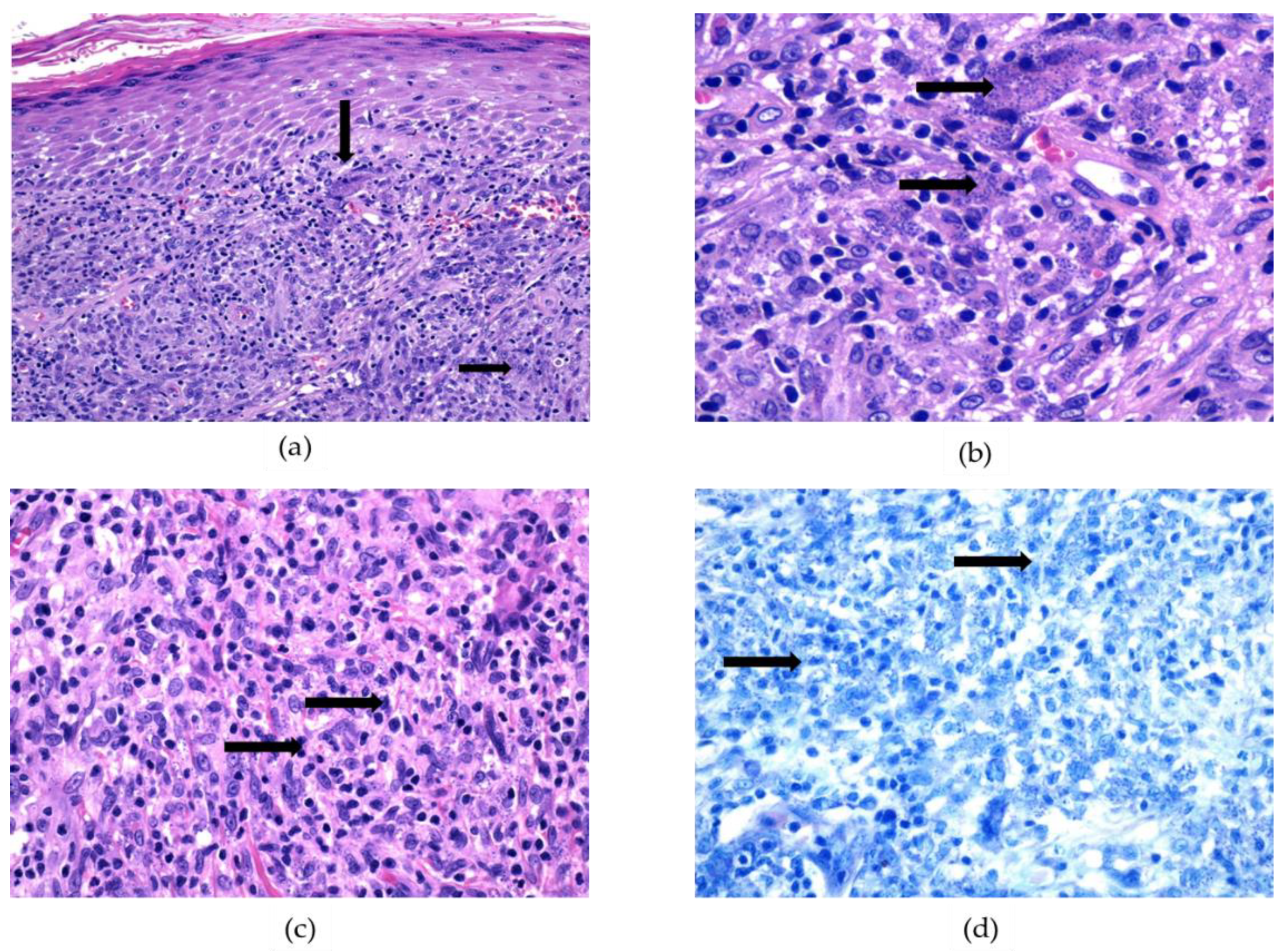
3.2. Clinicopathological Features
3.3. Diagnosis of Tegumentary Leishmaniasis
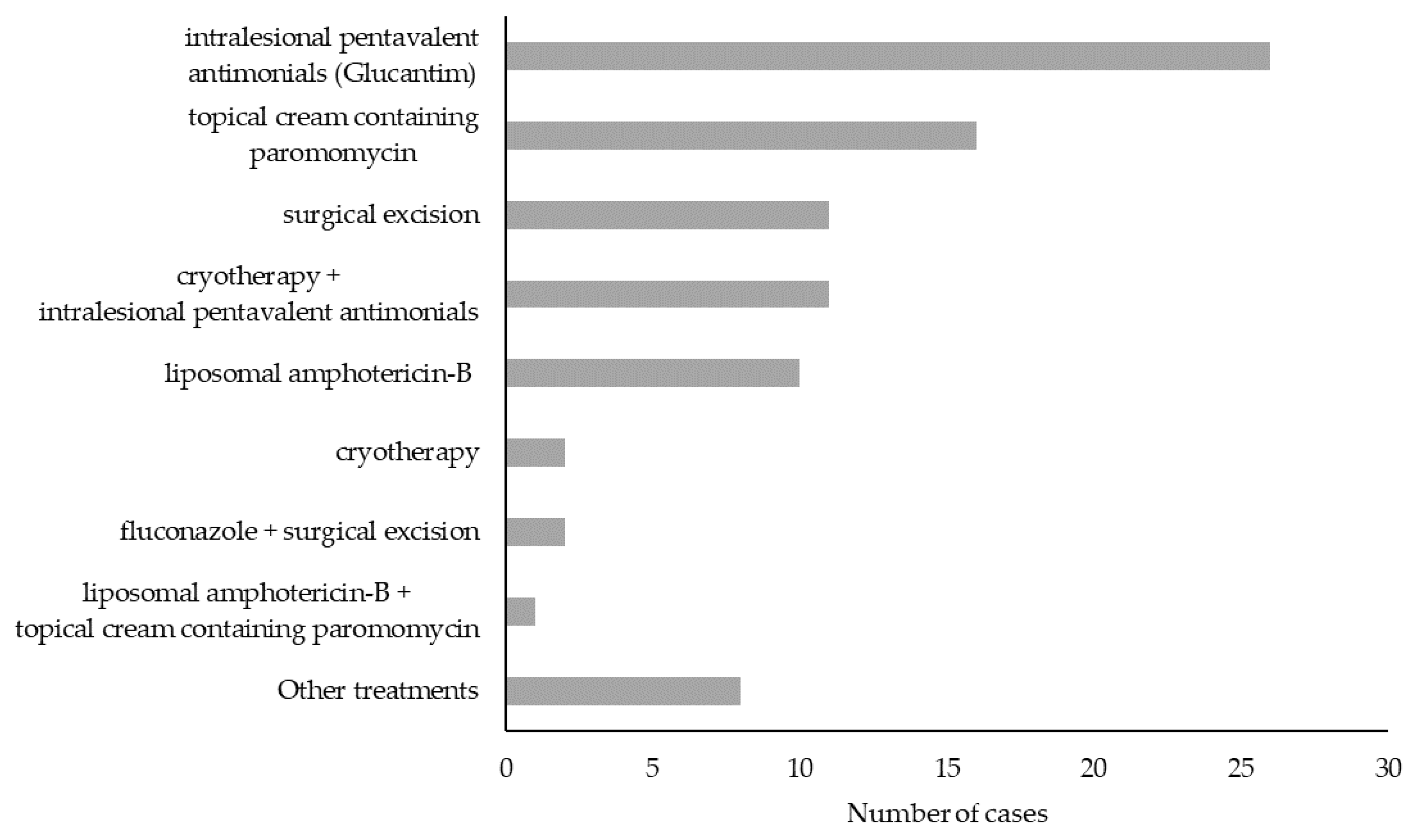
3.4. TL Treatment and Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gradoni, L. Epidemiological surveillance of leishmaniasis in the European Union: Operational and research challenges. Euro Surveill 2013, 18, 20539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guery, R.; Walker, S.L.; Harms, G.; Neumayr, A.; Van Thiel, P.; Gangneux, J.P.; Clerinx, J.; Söbirk, S.K.; Visser, L.; Lachaud, L.; et al. Clinical diversity and treatment results in Tegumentary Leishmaniasis: A European clinical report in 459 patients. PLoS Negl. Trop. Dis. 2021, 15, e0009863. [Google Scholar] [CrossRef] [PubMed]
- Grifferty, G.; Shirley, H.; McGloin, J.; Kahn, J.; Orriols, A.; Wamai, R. Vulnerabilities to and the Socioeconomic and Psychosocial Impacts of the Leishmaniases: A Review. Res. Rep. Trop Med. 2021, 12, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Gianchecchi, E.; Montomoli, E. The enemy at home: Leishmaniasis in the Mediterranean basin, Italy on the focus. Expert Rev. Anti-Infect. Ther. Aims Scope 2020, 18, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Postigo, J.A.; Grout, L.; Jain, S. Global Leishmaniasis Surveillance, 2017–2018, and First Report on 5 Additional Indicators; World Health Organization: Geneva, Switzerland, 2020; pp. 265–280. Available online: https://www.who.int/publications/i/item/who-wer9525 (accessed on 31 October 2022).
- Ruiz-Postigo, R.-P.; Saurabh, J.; Alexei, M.; Maia-Elkhoury, M.-E.A.N.; Samantha, V.; Supriya, W.; Mona, O.; Zaw, L.; Abate, B.; Aya, Y.; et al. Global Leishmaniasis Surveillance: 2019–2020, A Baseline for the 2030 Roadmap; World Health Organization: Geneva, Switzerland, 2021; pp. 401–419. Available online: https://www.who.int/publications/i/item/who-wer9635-401-419 (accessed on 31 October 2022).
- Berriatua, E.; Maia, C.; Conceição, C.; Özbel, Y.; Töz, S.; Baneth, G.; Pérez-Cutillas, P.; Ortuño, M.; Muñoz, C.; Jumakanova, Z.; et al. Leishmaniases in the European Union and Neighboring Countries. Emerg. Infect. Dis. 2021, 27, 1723–1727. [Google Scholar] [CrossRef]
- Alvar, J.; Vélez, I.D.; Bern, C.; Herrero, M.; Desjeux, P.; Cano, J.; Jannin, J.; den Boer, M.; Team, W.L.C. Leishmaniasis worldwide and global estimates of its incidence. PLoS ONE 2012, 7, e35671. [Google Scholar] [CrossRef]
- Gaspari, V.; Zaghi, I.; Macrì, G.; Patrizi, A.; Salfi, N.; Locatelli, F.; Carra, E.; Re, M.C.; Varani, S. Autochthonous Cases of Mucosal Leishmaniasis in Northeastern Italy: Clinical Management and Novel Treatment Approaches. Microorganisms 2020, 8, 588. [Google Scholar] [CrossRef] [Green Version]
- Santi, A.; Renzi, M.; Baldelli, R.; Calzolari, M.; Caminiti, A.; Dell’Anna, S.; Galletti, G.; Lombardini, A.; Paternoster, G.; Tamba, M. A surveillance program on canine leishmaniasis in the public kennels of Emilia-Romagna Region, Northern Italy. Vector-Borne Zoonotic Dis. 2014, 14, 206–211. [Google Scholar] [CrossRef] [Green Version]
- Faucher, B.; Pomares, C.; Fourcade, S.; Benyamine, A.; Marty, P.; Pratlong, L.; Faraut, F.; Mary, C.; Piarroux, R.; Dedet, J.P.; et al. Mucosal Leishmania infantum leishmaniasis: Specific pattern in a multicentre survey and historical cases. J. Infect. 2011, 63, 76–82. [Google Scholar] [CrossRef]
- WHO. Italy. Available online: http://who-dev.essi.upc.edu/who/leishmaniasis.html (accessed on 31 October 2022).
- Maroli, M.; Rossi, L.; Baldelli, R.; Capelli, G.; Ferroglio, E.; Genchi, C.; Gramiccia, M.; Mortarino, M.; Pietrobelli, M.; Gradoni, L. The northward spread of leishmaniasis in Italy: Evidence from retrospective and ongoing studies on the canine reservoir and phlebotomine vectors. Trop. Med. Int. Health 2008, 13, 256–264. [Google Scholar] [CrossRef]
- Mattivi, A.; Massimiliani, E.; Cagarelli, R.; Albieri, A. LEISHMANIOSI IN EMILIA-ROMAGNA, Aggiornamento Epidemiologico 1999–2015. Available online: https://salute.regione.emilia-romagna.it/normativa-e-documentazione/rapporti/malattie-infettive/leishmaniosi-er-epidemiologia-1999-2015 (accessed on 31 October 2022).
- Gaspari, V.; Ortalli, M.; Foschini, M.P.; Baldovini, C.; Lanzoni, A.; Cagarelli, R.; Gaibani, P.; Rossini, G.; Vocale, C.; Tigani, R.; et al. New evidence of cutaneous leishmaniasis in north-eastern Italy. J. Eur. Acad Dermatol. Venereol. 2017, 31, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Cesinaro, A.M.; Nosseir, S.; Mataca, E.; Mengoli, M.C.; Cavatorta, C.; Gennari, W. An outbreak of cutaneous leishmaniasis in Modena province (Northern Italy): Report of 35 cases. Pathologica 2017, 109, 363–367. [Google Scholar]
- Varani, S.; Cagarelli, R.; Melchionda, F.; Attard, L.; Salvadori, C.; Finarelli, A.C.; Gentilomi, G.A.; Tigani, R.; Rangoni, R.; Todeschini, R.; et al. Ongoing outbreak of visceral leishmaniasis in Bologna Province, Italy, November 2012 to May 2013. Euro Surveill 2013, 18, 20530. [Google Scholar] [CrossRef] [Green Version]
- Franceschini, E.; Puzzolante, C.; Menozzi, M.; Rossi, L.; Bedini, A.; Orlando, G.; Gennari, W.; Meacci, M.; Rugna, G.; Carra, E.; et al. Clinical and Microbiological Characteristics of Visceral Leishmaniasis Outbreak in a Northern Italian Nonendemic Area: A Retrospective Observational Study. Biomed Res. Int. 2016, 2016, 6481028. [Google Scholar] [CrossRef] [PubMed]
- Regione Emilia-Romagna. Individuazione Del Laboratorio di Riferimento Regionale Per la Diagnosi di Leishmaniosi Viscerale e Cutanea Umana. Doc nr. PG_2014_276720, 28/07/2014. Available online: https://salute.regione.emilia-romagna.it/sanita-pubblica/malattie-infettive/nota-regionale-luglio-2014.pdf/@@download/file/nota%20regionale%20luglio%202014.pdf (accessed on 24 November 2022).
- Regione Emilia-Romagna. Individuazione del Laboratorio di Riferimento Regionale Per la Diagnosi di Leishmaniosi Viscerale e Cutanea Umana. Precisazioni e Integrazioni Alla Nota PG_2014_276720. Doc. nr. PG_2014_373414, 14/10/2014. Available online: https://salute.regione.emilia-romagna.it/sanita-pubblica/malattie-infettive/pg_2014_373414-completo_.pdf/@@download/file/PG_2014_373414%20completo_.pdf (accessed on 24 November 2022).
- ISTAT. Superfici Territoriali. Available online: http://dati.istat.it/Index.aspx?DataSetCode=DCCV_CARGEOMOR_ST_COM (accessed on 31 October 2022).
- ISTAT. Popolazione Residente al 1° Gennaio 2021: Emilia-Romagna. Available online: http://dati.istat.it/index.aspx?queryid=18560 (accessed on 31 October 2022).
- Gradoni, L.; López-Vélez, R.; Mokni, M. Manual on Case Management and Surveillance of the Leishmaniases in the WHO European Region; World Health Organization: København, Danemark, 2017. [Google Scholar]
- Italian Ministry of Health. Prevenzione e Controllo Della Leishmaniosi in Italia. Doc nr. 0033122-14/10/2020-DGPRE-DGPRE-P. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=77839&parte=1%20&serie=null (accessed on 31 October 2022).
- Wortmann, G.; Sweeney, C.; Houng, H.S.; Aronson, N.; Stiteler, J.; Jackson, J.; Ockenhouse, C. Rapid diagnosis of leishmaniasis by fluorogenic polymerase chain reaction. Am. J. Trop. Med. Hyg. 2001, 65, 583–587. [Google Scholar] [CrossRef] [Green Version]
- Mary, C.; Faraut, F.; Lascombe, L.; Dumon, H. Quantification of Leishmania infantum DNA by a real-time PCR assay with high sensitivity. J. Clin. Microbiol. 2004, 42, 5249–5255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 31 October 2022).
- Spadea, T.; Di Girolamo, C.; Landriscina, T.; Leoni, O.; Forni, S.; Colais, P.; Fanizza, C.; Allotta, A.; Onorati, R.; Gnavi, R.; et al. Indirect impact of Covid-19 on hospital care pathways in Italy. Sci. Rep. 2021, 11, 21526. [Google Scholar] [CrossRef]
- Calzolari, M.; Romeo, G.; Munari, M.; Bonilauri, P.; Taddei, R.; Sampieri, M.; Bariselli, S.; Rugna, G.; Dottori, M. Sand Flies and Pathogens in the Lowlands of Emilia-Romagna (Northern Italy). Viruses 2022, 14, 2209. [Google Scholar] [CrossRef]
- Calzolari, M.; Angelini, P.; Finarelli, A.C.; Cagarelli, R.; Bellini, R.; Albieri, A.; Bonilauri, P.; Cavrini, F.; Tamba, M.; Dottori, M.; et al. Human and entomological surveillance of Toscana virus in the Emilia-Romagna region, Italy, 2010 to 2012. Euro Surveill 2014, 19, 20978. [Google Scholar] [CrossRef] [Green Version]
- Calzolari, M.; Carra, E.; Rugna, G.; Bonilauri, P.; Bergamini, F.; Bellini, R.; Varani, S.; Dottori, M. Isolation and Molecular Typing of of Leishmania infantum from Phlebotomus perfiliewi in a Re-Emerging Focus of Leishmaniasis, Northeastern Italy. Microorganisms 2019, 7, 644. [Google Scholar] [CrossRef] [Green Version]
- Calzolari, M.; Romeo, G.; Callegari, E.; Bonilauri, P.; Chiapponi, C.; Carra, E.; Rugna, G.; Taddei, R.; Lelli, D.; Dottori, M. Co-Circulation of Phleboviruses and Leishmania Parasites in Sand Flies from a Single Site in Italy Monitored between 2017 and 2020. Viruses 2021, 13, 1660. [Google Scholar] [CrossRef] [PubMed]
- Rugna, G.; Carra, E.; Bergamini, F.; Calzolari, M.; Salvatore, D.; Corpus, F.; Gennari, W.; Baldelli, R.; Fabbi, M.; Natalini, S.; et al. Multilocus microsatellite typing (MLMT) reveals host-related population structure in Leishmania infantum from northeastern Italy. PLoS Negl. Trop. Dis. 2018, 12, e0006595. [Google Scholar] [CrossRef] [Green Version]
- Ait Maatallah, I.; Akarid, K.; Lemrani, M. Tissue tropism: Is it an intrinsic characteristic of Leishmania species? Acta Trop. 2022, 232, 106512. [Google Scholar] [CrossRef] [PubMed]
- Chargui, N.; Amro, A.; Haouas, N.; Schönian, G.; Babba, H.; Schmidt, S.; Ravel, C.; Lefebvre, M.; Bastien, P.; Chaker, E.; et al. Population structure of Tunisian Leishmania infantum and evidence for the existence of hybrids and gene flow between genetically different populations. Int. J. Parasitol. 2009, 39, 801–811. [Google Scholar] [CrossRef] [PubMed]
- van Griensven, J.; Carrillo, E.; López-Vélez, R.; Lynen, L.; Moreno, J. Leishmaniasis in immunosuppressed individuals. Clin. Microbiol. Infect. 2014, 20, 286–299. [Google Scholar] [CrossRef] [Green Version]
- de Vries, H.J.; Reedijk, S.H.; Schallig, H.D. Cutaneous leishmaniasis: Recent developments in diagnosis and management. Am. J. Clin. Dermatol. 2015, 16, 99–109. [Google Scholar] [CrossRef] [Green Version]
- Tordini, G.; Giaccherini, R.; Pacenti, L.; Miracco, C.; Zazzi, M.; Zanelli, G. Cutaneous leishmaniasis: Usefulness of PCR on paraffin-embedded skin biopsies as part of routine investigation. Ann. Trop. Med. Parasitol. 2007, 101, 745–749. [Google Scholar] [CrossRef]
- Martín-Ezquerra, G.; Fisa, R.; Riera, C.; Rocamora, V.; Fernández-Casado, A.; Barranco, C.; Serra, T.; Baró, T.; Pujol, R.M. Role of Leishmania spp. infestation in nondiagnostic cutaneous granulomatous lesions: Report of a series of patients from a Western Mediterranean area. Br. J. Dermatol. 2009, 161, 320–325. [Google Scholar] [CrossRef]
- Silgado, A.; Armas, M.; Sánchez-Montalvá, A.; Goterris, L.; Ubals, M.; Temprana-Salvador, J.; Aparicio, G.; Chicharro, C.; Serre-Delcor, N.; Ferrer, B.; et al. Changes in the microbiological diagnosis and epidemiology of cutaneous leishmaniasis in real-time PCR era: A six-year experience in a referral center in Barcelona. PLoS Negl. Trop. Dis. 2021, 15, e0009884. [Google Scholar] [CrossRef]
- Morizot, G.; Kendjo, E.; Mouri, O.; Thellier, M.; Pérignon, A.; Foulet, F.; Cordoliani, F.; Bourrat, E.; Laffitte, E.; Alcaraz, I.; et al. Travelers with cutaneous leishmaniasis cured without systemic therapy. Clin. Infect. Dis. 2013, 57, 370–380. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | TL Cases (n.) | Notified to LHU n. (%) | Autochthonous Cases n. (%) | CL Cases n. (%) | ML Cases n. (%) |
|---|---|---|---|---|---|
| 2017 | 28 | 21 (75%) | 21 (75%) | 23 (82%) | 5 (18%) |
| 2018 | 39 | 36 (92%) | 34 (87%) | 38 (97%) | 1 (3%) |
| 2019 | 44 | 38 (86%) | 40 (91%) | 41 (93%) | 3 (7%) |
| 2020 | 24 | 18 (75%) | 18 (75%) | 22 (92%) | 2 (8%) |
| Total | 135 | 113 (84%) | 113 (84%) | 124 (92%) | 11 * (8%) |
| Case Notification | |||
|---|---|---|---|
| Yes | No | ||
| PCR Confirmation | Yes | 92 (68%) | 11 (8%) |
| No | 21 (15%) | 11 (8%) | |
| Total | 113 (84%) | 22 (16%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaspari, V.; Gritti, T.; Ortalli, M.; Santi, A.; Galletti, G.; Rossi, A.; Rugna, G.; Mattivi, A.; Matteo, G.; Belloli, G.L.; et al. Tegumentary Leishmaniasis in Northeastern Italy from 2017 to 2020: A Neglected Public Health Issue. Int. J. Environ. Res. Public Health 2022, 19, 16047. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192316047
Gaspari V, Gritti T, Ortalli M, Santi A, Galletti G, Rossi A, Rugna G, Mattivi A, Matteo G, Belloli GL, et al. Tegumentary Leishmaniasis in Northeastern Italy from 2017 to 2020: A Neglected Public Health Issue. International Journal of Environmental Research and Public Health. 2022; 19(23):16047. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192316047
Chicago/Turabian StyleGaspari, Valeria, Tommaso Gritti, Margherita Ortalli, Annalisa Santi, Giorgio Galletti, Arianna Rossi, Gianluca Rugna, Andrea Mattivi, Giulio Matteo, Gian L. Belloli, and et al. 2022. "Tegumentary Leishmaniasis in Northeastern Italy from 2017 to 2020: A Neglected Public Health Issue" International Journal of Environmental Research and Public Health 19, no. 23: 16047. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192316047