
Impacts of an Intervention to Improve the Identification, Referral and Safety of Those Experiencing Domestic Violence: A Mixed Methods Study in the UK
Abstract
:1. Introduction
- What impacts does IRIS have on recorded health conditions as captured in GP and IRIS data?
- How do survivors of DV who have accessed IRIS support describe its impacts on their health and well-being?
- What is the relationship between IRIS support, its outcomes, who survivors are and deprivation profile?
- How do the quantitative and qualitative strands of the study interact to inform future research and practice?
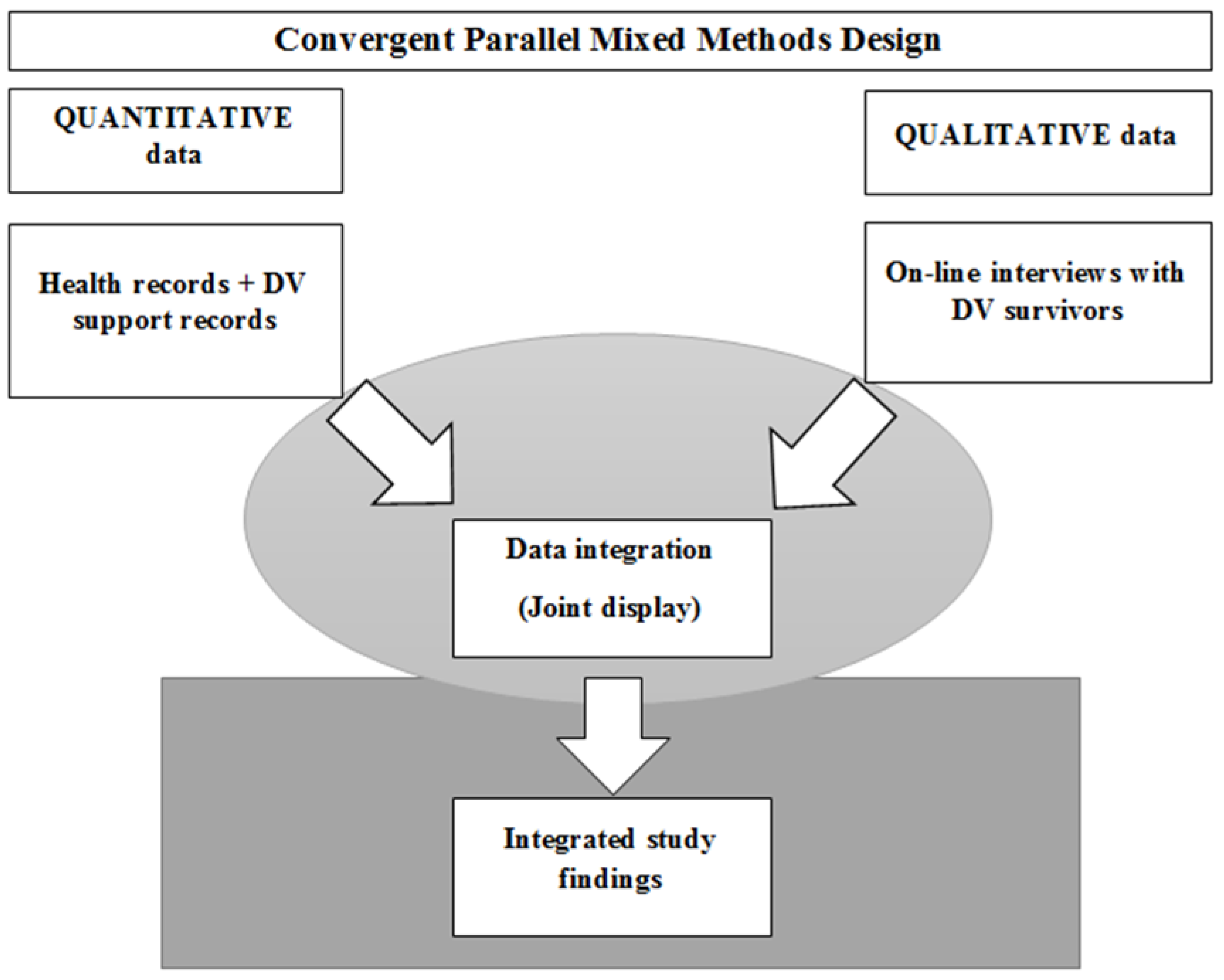
2. Methods and Materials
2.1. Quantitative Phase
2.1.1. Data Collection
2.1.2. Sampling Procedure
- The IRIS support agencies sent the researcher team a list of referrals from each GP practice and the training dates of GP practices from each area.
- The research team identified GP practices for inclusion in the study and provided the IRIS support agencies with a list of GP practices and numbers of referrals from each.
- The agencies added the anonymisation codes and referral dates of each patient from each of the GP practices and sent to the research team.
- Agencies sent names of the patients to GP practices. In doing so, this kept the names of the patients blind to the research team.
- The research team used agency anonymisation codes for each patient and created customised blank spreadsheets for each patient and sent to each GP practice for data collection across the study area.
- The research team created a customised blank spreadsheet for each patient/referral for data collection on the support provided and sent to all IRIS support agencies.
- GPs returned to the research team the collected data by return of spreadsheets (from Step 5) on health information for each patient/referral.
- Agencies sent the research team the data on IRIS support provided to each patient/referral by return of spreadsheets (in Step 6).
2.1.3. Data Analysis
2.2. Qualitative Phase
2.2.1. Recruitment
2.2.2. Data Collection
2.2.3. Data Analysis
3. Results
3.1. Quantitative Results
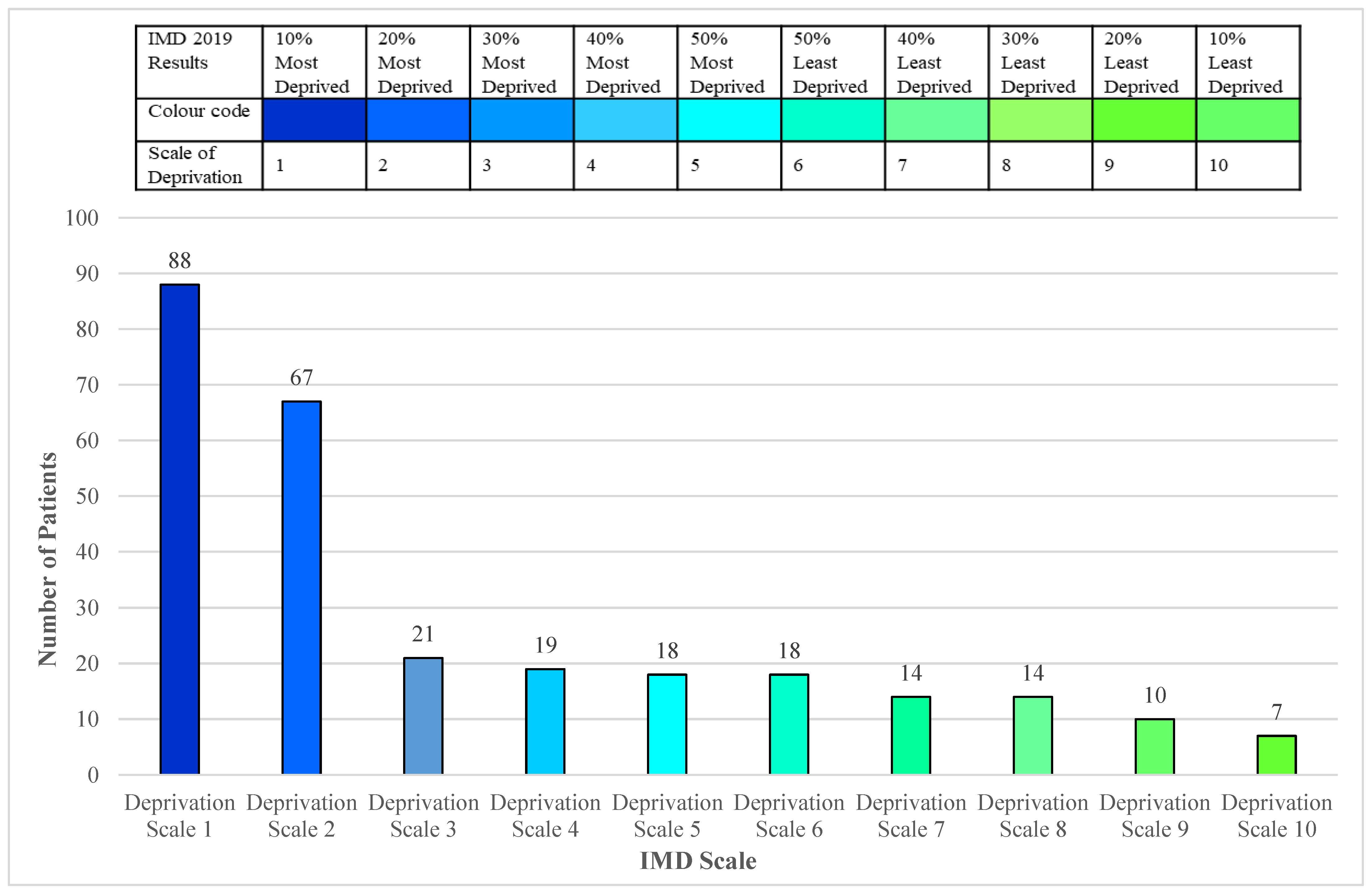
3.1.1. Mapping Deprivation
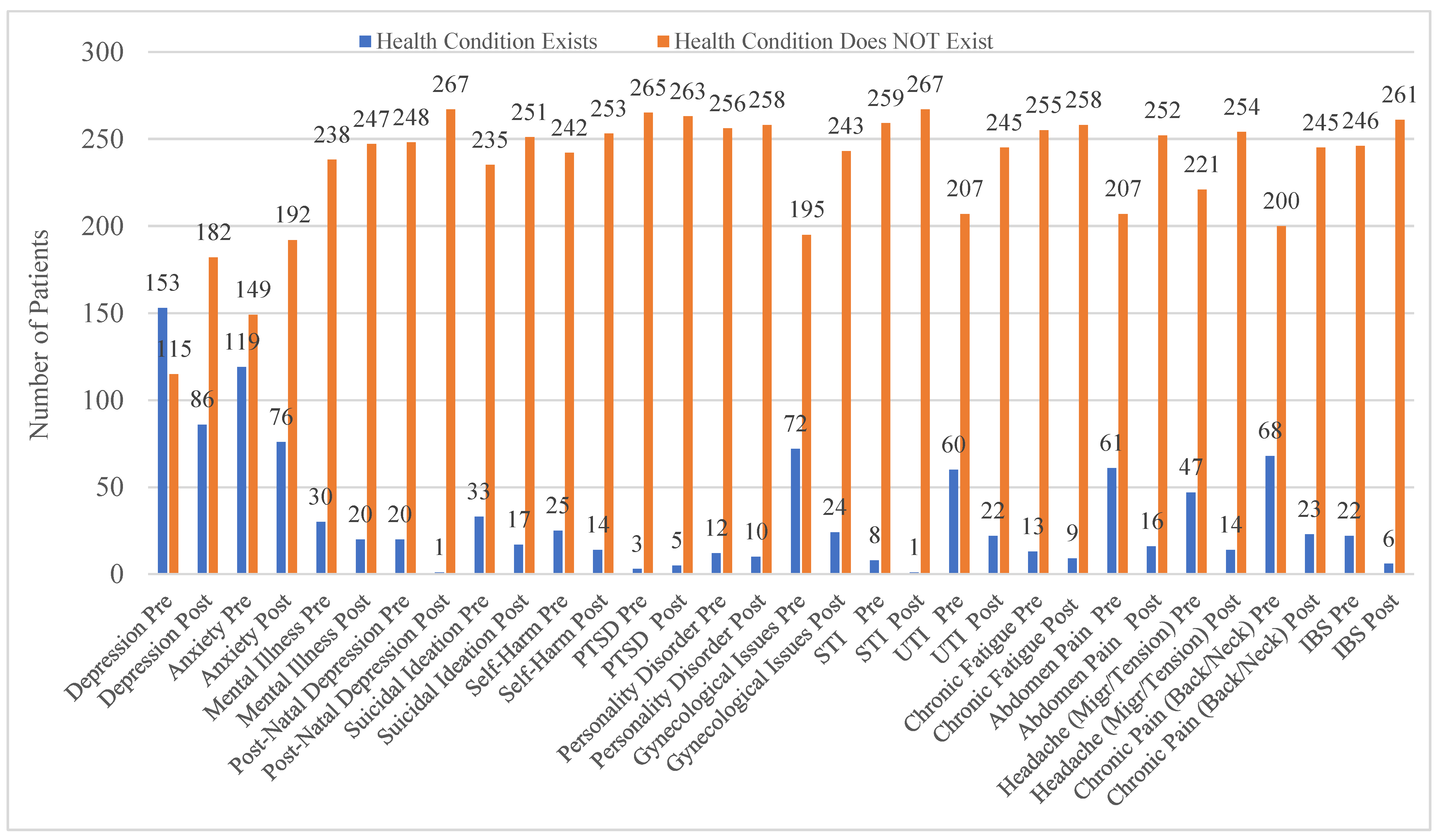
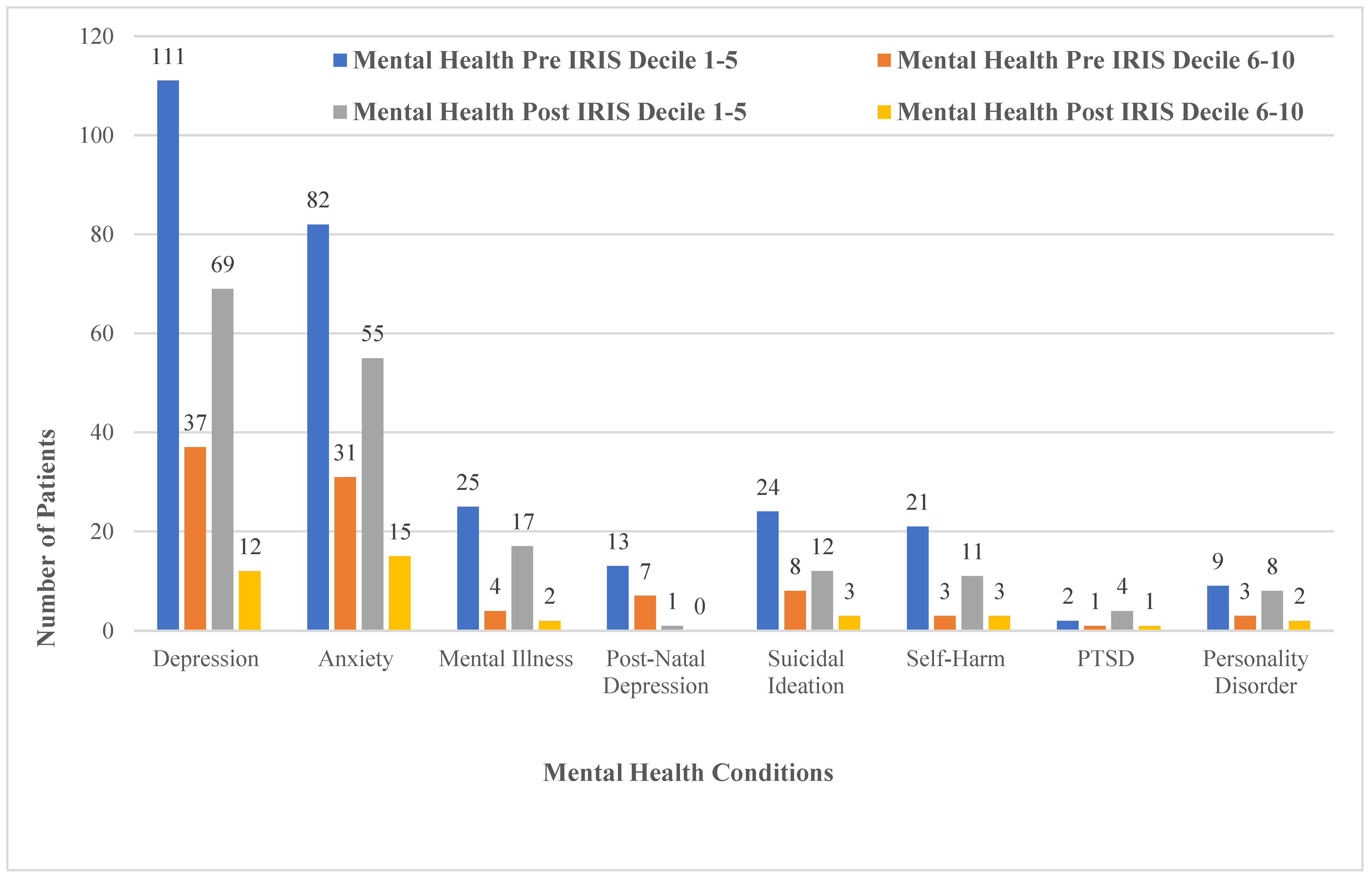
3.1.2. Health Conditions and Deprivation Analysis
3.2. Qualitative Findings
3.2.1. Life Before
I almost lost emotion, but I also lost the ability to be able to control emotion… I’d feel more anger than I’ve ever noticed I’ve ever felt before… I struggled quite a lot with that and there was a lot of emotions that I was unable to control, almost.(W5)
Yeah, I just felt really low like and, to be honest, I think I was just ground down by it all. You know, police intervention, child services, I mean I was a bit embarrassed. You know the last thing you want as a parent is child services—you feel like you’ve failed a little bit, do you know what I mean?(D2)
3.2.2. Driving Forces for Help-Seeking
Things got really bad for me and I needed some support and didn’t understand a lot of things. Some things had happened which was really hard for me to understand and I needed the right medication and I needed the right support and help and I think that’s when [AE] kind of came in a supported me in my hospital appointments and anything else that I needed really.(W8)
I told the doctor, and I just explained the situation, how it was at home, because how I was living with him. And it was the doctor who diagnosed it as coercive control.(D7)
Once I knew that it was only down the road, for example—there was lots of things that helped me make that decision, so the fact that it was local, that I could do it, it was term time only, they had child care… so in a way… it got to the point that I couldn’t not go! Because there were no barriers, you know? So, all the barriers that, you know, would stop me from going were sorted out.(B4)
3.2.3. Experiences of Support
She’s just sat there and allowed me to speak, allowed me to cry, allowed me to express. And she’s given me all… support and advice.(D6)
She was very good with just speaking to me about gaining control because I felt that I’d lost all control… She gave me all the right help at that time so I think it was a really good outcome… I don’t know which place I would be in if I hadn’t met [AE]. I probably would have been in a lot of a worst place.(B5)
Yeah, it was really good, because I think when you’re in a domestic violence situation and you’re clouded by a lot of factors, it’s kind of, you know, someone shedding that bit of light on it for you so you kind of look at it in a different way, if that makes sense?(D2)
And I think it’s very important that you are validated by professionals. Not that other women can’t validate you, that’s also important. But I think that it’s really, really important that you can get to an understanding yourself that what was done to you was wrong, and that you’re in no way responsible for it.(B4)
And I think, I just needed that validation I think, and to believe myself. Because there was lot of things that I didn’t say out loud, there was a lot of things that I didn’t act on, because if I said it out loud it was real. I think saying it out loud and realising it’s real is one of the most important things because otherwise it just gets hidden away and ignored.(W5)
She [AE] told me, ‘don’t worry if you can’t speak English, just call me and if you can’t speak, just ring and say “call me”’. She said she would call back with an interpreter. I would message her ‘call me’ and she would call back with an interpreter who could speak Urdu… then without fail I would receive a call from her. So that’s why I say that even my soul prays for her. I received a lot of help from [AE].(B1)
3.2.4. Perceived Impacts
I think to be honest with you in that aspect, it’s… everyone’s aware of antidepressants. Nobody is aware of anti-abuse workers. Forget the antidepressants, no one is aware that we have support workers out there who can do a lot better than those antidepressants can.(D6)
My diabetes, well, that is much, much better and my physical health, I’m getting fitter, I’m walking more, I’m exercising more. I’m taking more care of me. That’s the thing, I never took care of me and now I am. So, it’s had a massive, massive impact on every aspect of my health.(D1)
Well, I was in a wheelchair… and now, the wheelchair is there if I need it, but I’m—I’m trying to make myself…I push myself to go down for a walk to the garden.(W6)
I started reading books because he wouldn’t let me read books… do you know what I mean?(W6)
I feel, I’m beginning to feel freer than I ever felt, I’m not looking over my shoulder as much (although I am looking over my shoulder), but it’s definitely not the way I did it before when it first happened.(S4)
3.2.5. Recovery as a Journey
I haven’t come to the end of my journey in terms of dealing with what happened to me, but I’m a lot further forward than I would have been, had I not been able to get outside support. It’s taken a long time for me to recognise and understand that my mission in life is to be the best version of me.(B4)
I mean, don’t get me wrong, I do still have my down days, and I’ve had moments where I’ve been on the antidepressants but then I put my children first and think, well if I’m teaching my children that they need to battle to succeed in their life, me as being their role model and being on antidepressants—what am I actually teaching them? I’m totally going against my own teachings.(D6)
I think my outlook is completely different and can actually say that I’m happy. Don’t get me wrong, I have my worries and… about the future, you know, it is daunting being a single parent, you know, it is hard work but I do have good support network and my boys are really happy, you know, because I’m happy they’re happy you know?(D2)
I’ve enrolled into college to start in September... I’ve got my goals, in place, where I want to get to. You know I want to study, I want to further my career, I want a secure future for my children.(D2)
I’ve got my life back on track and I’m feeling a lot better about myself.(D6)
3.3. Data Integration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization & Pan American Health Organization. Understanding and Addressing Violence against Women: Intimate Partner Violence. 2012. Available online: https://apps.who.int/iris/handle/10665/77432 (accessed on 2 November 2021).
- World Health Organization. The Public Health Approach. 2021. Available online: http://www.who.int/violenceprevention/approach/public_health/en/ (accessed on 2 November 2021).
- World Health Organization. Violence against Women. 9 Match 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/violence-against-women (accessed on 2 November 2021).
- United Nations. Neglect, Abuse and Violence against Older Women. 2013. Available online: https://www.un.org/esa/socdev/documents/ageing/neglect-abuse-violence-older-women.pdf (accessed on 11 November 2022).
- Office for National Statistics. Domestic Abuse Victim Characteristics, England and Wales. Ons.Gov.UK. 25 November 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/crimeandjustice/articles/domesticabusevictimcharacteristicsenglanDVndwales/yearendingmarch2020 (accessed on 2 October 2020).
- Ferrari, G.; Agnew-Davies, R.; Bailey, J.; Howard, L.; Howarth, E.; Peters, T.J.; Sardinha, L.; Feder, G.S. Domestic violence and mental health: A cross sectional survey of women seeking help from domestic violence support services. Glob. Health Action 2016, 9, 29890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandan, J.S.; Thomas, T.; Bradbury-Jones, C.; Russell, R.; Bandyopadhyay, S.; Nirantharakumar, K.; Taylor, J. Female Survivors of Intimate Partner Violence and Risk of Depression, Anxiety and Serious Mental Illness. Br. J. Psychiatry 2019, 217, 562–567. [Google Scholar] [CrossRef] [PubMed]
- Sauber, E.W.; O’Brien, K.M. Multiple Losses: The Psychological and Economic Well-Being of Survivors of Intimate Partner Violence. J. Interpers. Violence 2017, 35, 3054–3078. [Google Scholar] [CrossRef] [PubMed]
- Lin-Roark, I.H.; Church, A.T.; McCubbin, L.D. Battered Women’s Evaluations of Their Intimate Partners as a Possible Mediator between Abuse and Self-Esteem. J. Fam. Violence 2015, 30, 201–214. [Google Scholar] [CrossRef]
- Lima, L.A.A.; Monteiro, C.F.S.; Nunes, B.M.V.T.; Junior, F.J.G.S.; Fernandes, M.A.; Zafar SSantos, M.A.; Wagstaff, C.; Diehl, A.; Pillon, S.C. Factors associated with violence against women by an intimate partner in Northeast Brazil. Arch. Psychiatr. Nurs. 2021, 35, 669–677. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Domestic Violence and Abuse, (QS116) Quality Standard. 2016. Available online: https://www.nice.org.uk/guidance/qs116/resources/domestic-violence-and-abuse-pdf-75545301469381 (accessed on 2 November 2021).
- Keynejad, R.; Baker, N.; Lindenberg, U.; Pitt, K.; Boyle, A.; Hawcroft, C. Identifying and responding to domestic violence and abuse in healthcare settings. BMJ 2021, 373, n1047. [Google Scholar] [CrossRef] [PubMed]
- Chandan, J.S.; Gokhale, K.M.; Bradbury-Jones, C.; Nirantharakumar, K.; Bandyopadhyay, S.; Taylor, J. Exploration of trends in the incidence and prevalence of childhood maltreatment and domestic abuse recording in UK primary care: A retrospective cohort study using ‘the health improvement network’ database. BMJ Open 2020, 10, e036949. [Google Scholar] [CrossRef] [PubMed]
- Heron, R.L.; Eisma, M.C. Barriers and facilitators of disclosing domestic violence to the healthcare service: A systematic review of qualitative research. Health Soc. Care Community 2021, 29, 612–630. [Google Scholar] [CrossRef] [PubMed]
- Feder, G.; Davies, R.A.; Baird, K.; Dunne, D.; Eldridge, S.; Griffiths, C.; Gregory, A.; Howell, A.; Johnson, M.; Ramsay, J.; et al. Identification and Referral to Improve Safety (IRIS) of women experiencing domestic violence with a primary care training and support programme: A cluster randomised controlled trial. Lancet 2011, 378, 1788–1795. [Google Scholar] [CrossRef] [PubMed]
- IRISi. About the IRIS Programme. 2021. Available online: https://irisi.org/about-the-iris-programme/ (accessed on 16 November 2021).
- Bradbury-Jones, C.; Clark, M.T.; Taylor, J. Abused women’s experiences of a primary care identification and referral intervention: A case study analysis. J. Adv. Nurs. 2017, 73, 3189–3199. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, E.; D’avo, G.; Howell, A.; Johnson, M. IRIS Improving the General Practice Response to Domestic Violence and Abuse. 2020. Available online: https://irisi.org/wp-content/uploads/2020/10/IRIS-National-Report-2020.pdf (accessed on 2 November 2021).
- Creswell, J.W.; Plano-Clark, V.L. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Index of Multiple Deprivation, Government UK, English Indices of Deprivation. 2019. Available online: https://www.gov.uk/guidance/english-indices-of-deprivation-2019-mapping-resources (accessed on 3 October 2020).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Dillon, G.; Hussain, R.; Loxton, D.; Rahman, S. Mental and physical health and intimate partner violence against women: A review of the literature. Int. J. Fam. Med. 2013, 2013, 313909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandan, J.S.; Thomas, T.; Bradbury-Jones, C.; Taylor, J.; Bandyopadhyay, S.; Nirantharakumar, K. Intimate partner violence and the risk of developing fibromyalgia and chronic fatigue syndrome. J. Interpers. Violence 2019, 36, 12279–12298. [Google Scholar] [CrossRef] [PubMed]
- Zlotnick, C.; Johnson, D.M.; Kohn, R. Intimate partner violence and long-term psychosocial functioning in a national sample of American women. J. Interpers. Violence 2006, 21, 262–275. [Google Scholar] [CrossRef] [PubMed]
- Devries, K.; Mak, J.Y.; Bacchus, L.J.; Child, J.C.; Falder, G.; Petzold, M.; Astbury, J.; Watts, C.H. Intimate partner violence and incident depressive symptoms and suicide attempts: A systematic review of longitudinal studies. PLoS Med. 2013, 10, e1001439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raphael, E.; Van Den Eeden, S.K.; Gibson, C.J.; Tonner, C.; Thom, D.H.; Subak, L.; Huang, A.J. Interpersonal violence and painful bladder symptoms in community-dwelling midlife to older women. Am. J. Obstet. Gynecol. 2022, 226, e1–e11. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/pii/S0002937821010450 (accessed on 24 January 2022). [CrossRef] [PubMed]
- Sharps, P.W.; Njie-Carr, V.P.S.; Alexander, K. The Syndemic Interaction of Intimate Partner Violence, Sexually Transmitted Infections, and HIV Infection among African American Women: Best Practices and Strategies. J. Aggress. Maltreatment Trauma 2021, 30, 811–827. [Google Scholar] [CrossRef]
- Hegarty, K.L.; O’Doherty, L.J.; Chondros, P.; Valpied, J.; Taft, A.J.; Astbury, J.; Brown, S.J.; Gold, L.; Taket, A.; Feder, G.S.; et al. Effect of type and severity of intimate partner violence on women’s health and service use: Findings from a primary care trial of women afraid of their partners. J. Interpers. Violence 2013, 28, 273–294. [Google Scholar] [CrossRef] [PubMed]
- Keeling, J.; Fisher, C. Health professionals’ responses to women’s disclosure of domestic violence. J. Interpers. Violence 2015, 30, 2363–2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsay, J.; Rutterford, C.; Gregory, A.; Dunne, D.; Eldridge, S.; Sharp, D.; Feder, G. Domestic violence: Knowledge, attitudes, and clinical practice of selected UK primary healthcare clinicians. Br. J. Gen. Pract. 2012, 62, e647–e655. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Recorded Ethnicity | Participants (n = 294) |
|---|---|
| White British | 163 |
| British Pakistani | 32 |
| British Indian | 15 |
| British Asian | 13 |
| British Other | 11 |
| European | 8 |
| White Other | 7 |
| British Bangladeshi | 6 |
| British African | 2 |
| British Caribbean | 2 |
| White and Black African | 3 |
| White and Black Caribbean | 1 |
| White Irish | 1 |
| Other Mixed Background | 1 |
| Other | 18 |
| Blank | 11 |
| Age (years) | |
| 18–29 | 57 |
| 30–39 | 80 |
| 40–49 | 59 |
| 50–59 | 34 |
| 60–69 | 17 |
| 70–79 | 16 |
| 80–89 | 2 |
| 90–100 | 1 |
| Gender | |
| Female | 264 |
| Male | 30 |
| Domain | Quantitative Results | Qualitative Findings | Inferences | Implications |
|---|---|---|---|---|
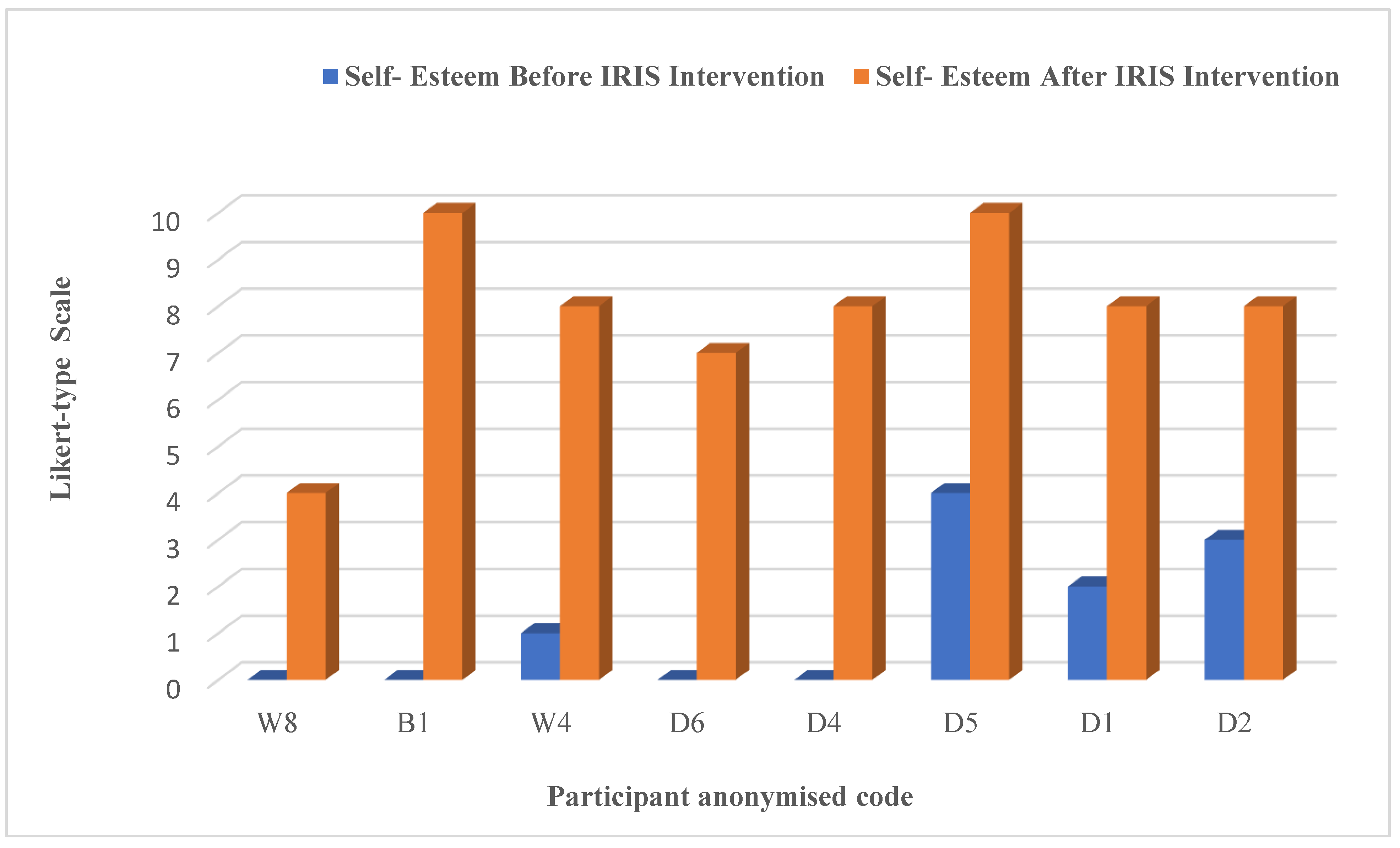
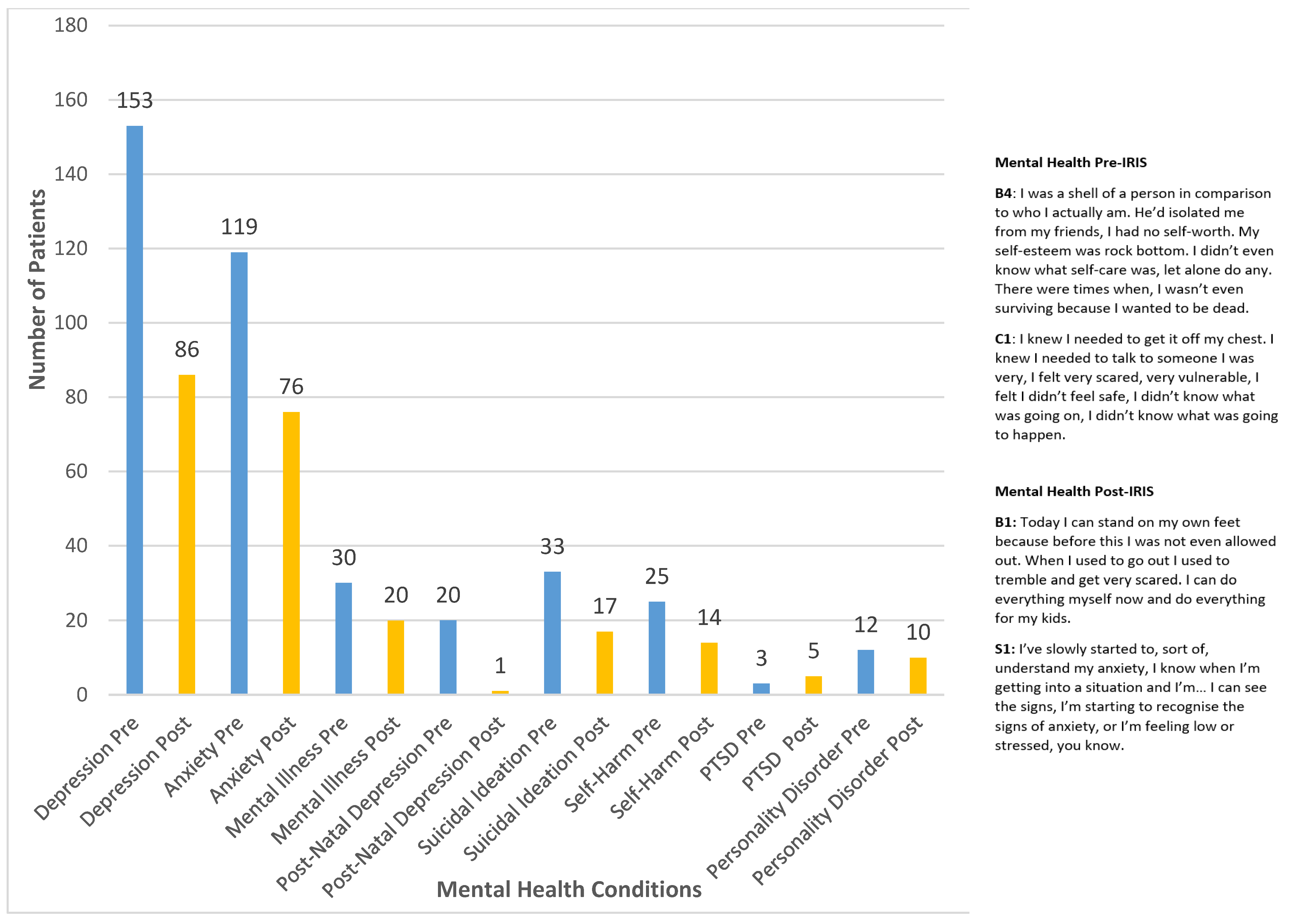
| Mental health conditions | Pre-IRIS, 57% (n = 153) of the sample had depression recorded, and 44% (n = 119) had anxiety recorded. Post-IRIS, depression and anxiety were recorded at 32% (n = 86) and 28% (n = 76), respectively. | All participants reported an improved sense of self-esteem, and for those who had experienced anxiety and depression prior to IRIS, most stated that this was reduced following the support. | The quantitative and qualitative findings indicate that IRIS support has a positive impact on mental health. | IRIS should be regarded as an effective intervention in promoting positive mental health, and its commissioning should be regarded as a justifiable return on investment. |
| Genitourinary conditions | Pre-IRIS, 27% (n = 72) of the sample had gynaecological problems recorded, 3% (n = 8) had STI recorded and 22% (n = 60) had UTI recorded. Post-IRIS, gynaecological problems, STI and UTI were recorded at 9% (n = 24) 0.4% (n = 1) and 8% (n = 22), respectively. | No participants in the qualitative phase talked of this aspect of physical health. | The quantitative results showed an improvement in recorded genitourinary conditions post-IRIS support, but this was not supported by the qualitative findings. | Qualitative studies that explore the potential impacts of IRIS on genitourinary health are recommended. |
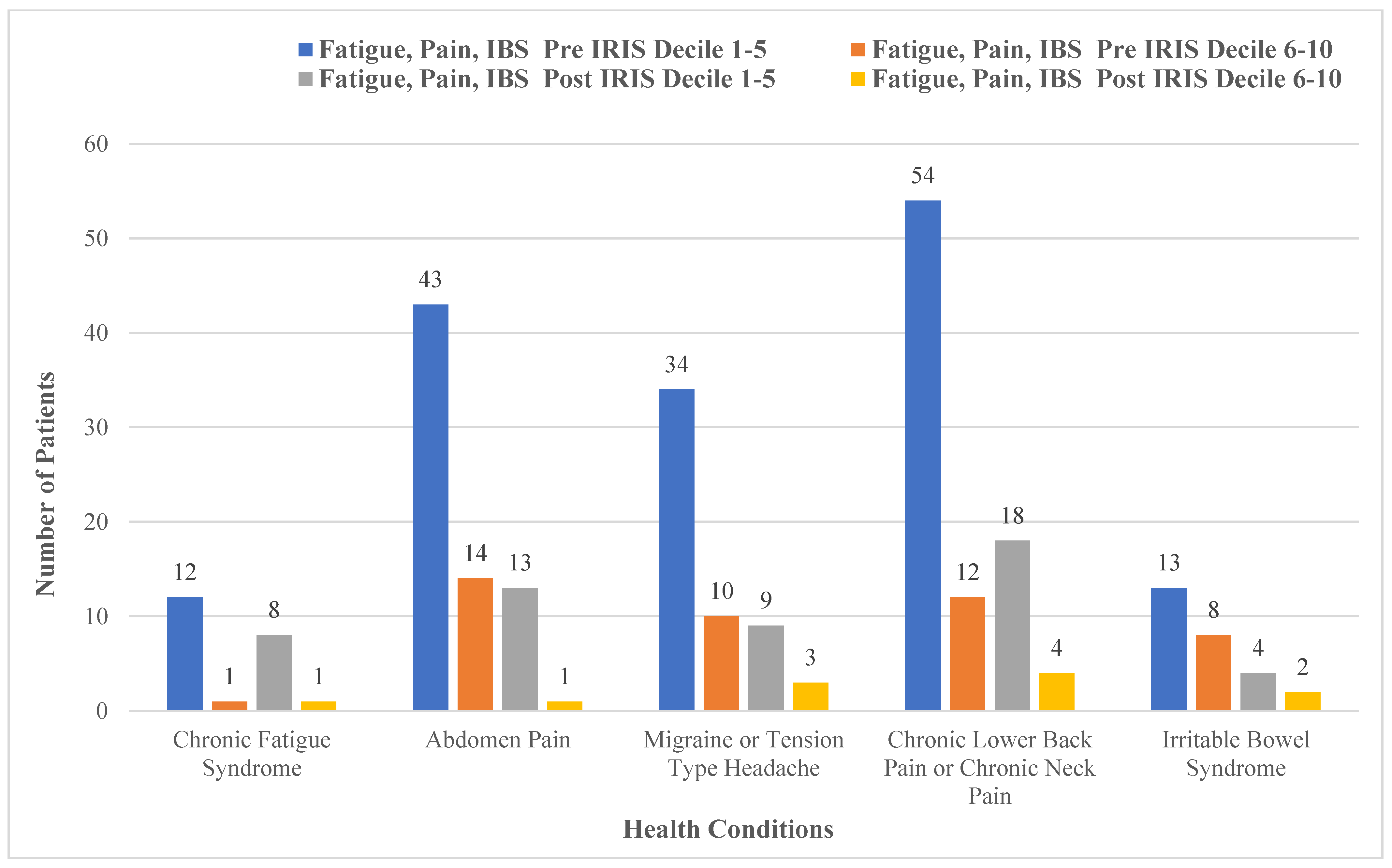
| Fatigue, pain and IBS | Pre-IRIS, 5% (n = 13) had chronic fatigue recorded, 66% (n = 176) had pain recorded and 8% (n = 22) had IBS recorded. Post-IRIS, chronic fatigue, pain and IBS were recorded at 3% (n = 9) 20% (n = 53) and 2% (n = 6), respectively. | Some participants in the qualitative phase reported improved mobility and improvements in overall health, but not specifically in relation to fatigue, pain and IBS. | The quantitative results showed an improvement in recorded fatigue, pain and IBS post-IRIS support, but we were unable to verify this through the qualitative findings. | Qualitative studies that explore the potential impacts of IRIS on fatigue, pain and IBS health are recommended. |
| Deprivation | 77% of sample cohort were from the most deprived areas of West Midlands, and 23% were living in the least deprived areas. There was a range of ethnicities within the sample cohort who had received IRIS support, with the highest number of participants (55%) identifying as white British and the next highest number (11%) identifying as British Pakistani. | We did not collect demographic data pertaining to participants’ socio-economic status, and our processes of anonymisation meant that we did not know their postcodes. | Although a broad range of ethnicities were acknowledged, the number of participants who identified as non-white were far lower than expected due to population in West Midlands containing a very cosmopolitan mix of ethnicities. More work needs to be performed to reach those communities. | DV interventions that target the most deprived communities are useful, but this must not overshadow the experiences of DV among all societal strata. |
| Overall health | The overall health was recorded as a drop post-IRIS intervention indication improvement. | Recovery is a process | The results from the quantitative phase were seen especially in mental health improving in the qualitative phase. | Intervention when provided timely and continued ongoing post-intervention has proven to show benefits to an individual’s overall health. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zafar, S.; Bradbury-Jones, C.; Bandyopadhyay, S. Impacts of an Intervention to Improve the Identification, Referral and Safety of Those Experiencing Domestic Violence: A Mixed Methods Study in the UK. Int. J. Environ. Res. Public Health 2022, 19, 16181. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192316181
Zafar S, Bradbury-Jones C, Bandyopadhyay S. Impacts of an Intervention to Improve the Identification, Referral and Safety of Those Experiencing Domestic Violence: A Mixed Methods Study in the UK. International Journal of Environmental Research and Public Health. 2022; 19(23):16181. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192316181
Chicago/Turabian StyleZafar, Shazia, Caroline Bradbury-Jones, and Siddhartha Bandyopadhyay. 2022. "Impacts of an Intervention to Improve the Identification, Referral and Safety of Those Experiencing Domestic Violence: A Mixed Methods Study in the UK" International Journal of Environmental Research and Public Health 19, no. 23: 16181. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192316181