
Age- and Gender-Specific Differences in the Seasonal Distribution of Diabetes Mortality in Shandong, China: A Spatial Analysis
Abstract
:1. Introduction
2. Materials and Methods
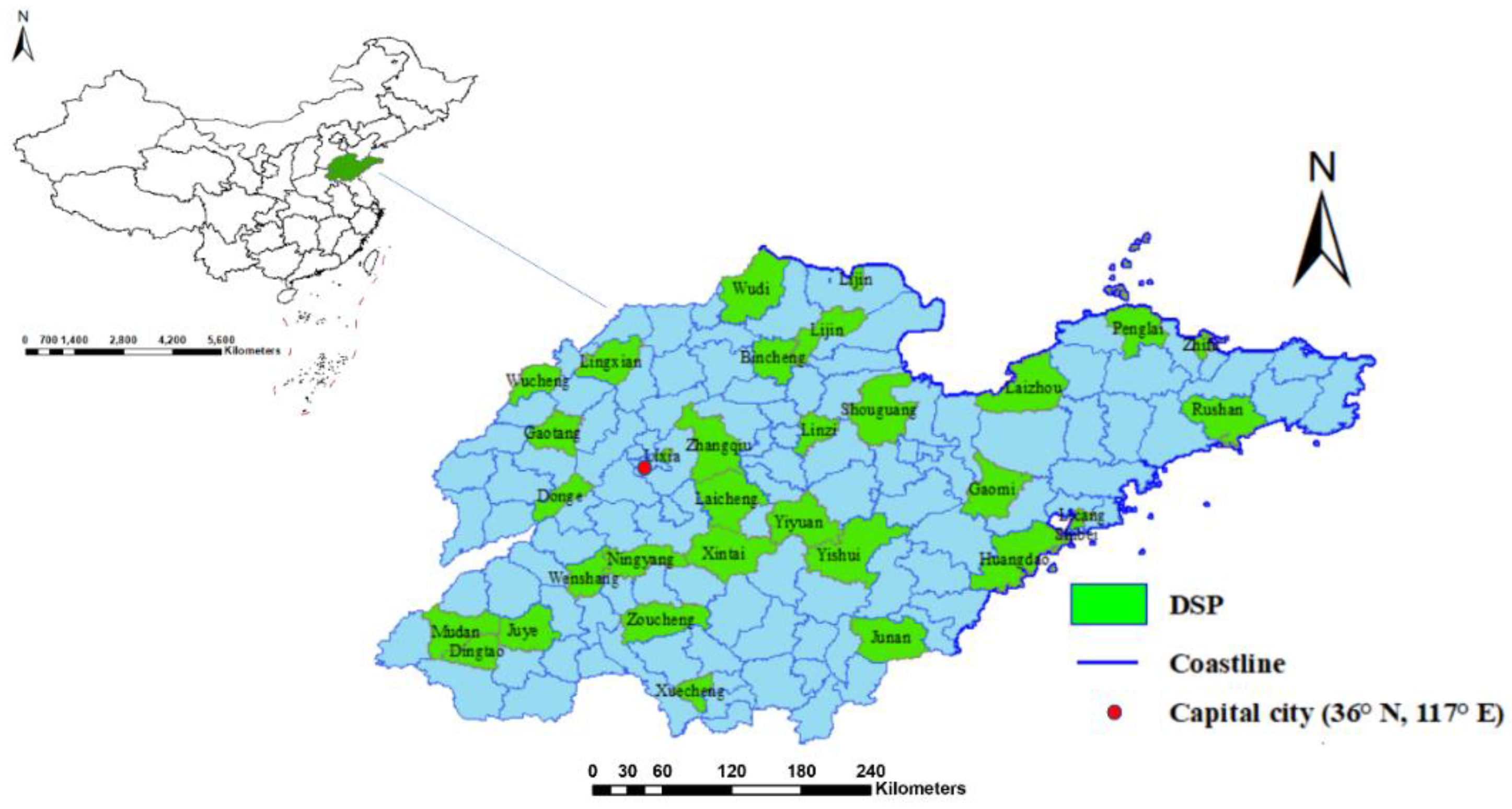
2.1. Data Source
2.2. Data Analysis
3. Results
3.1. Descriptive Analyses
3.2. Spatial Autocorrelation and Interpolation
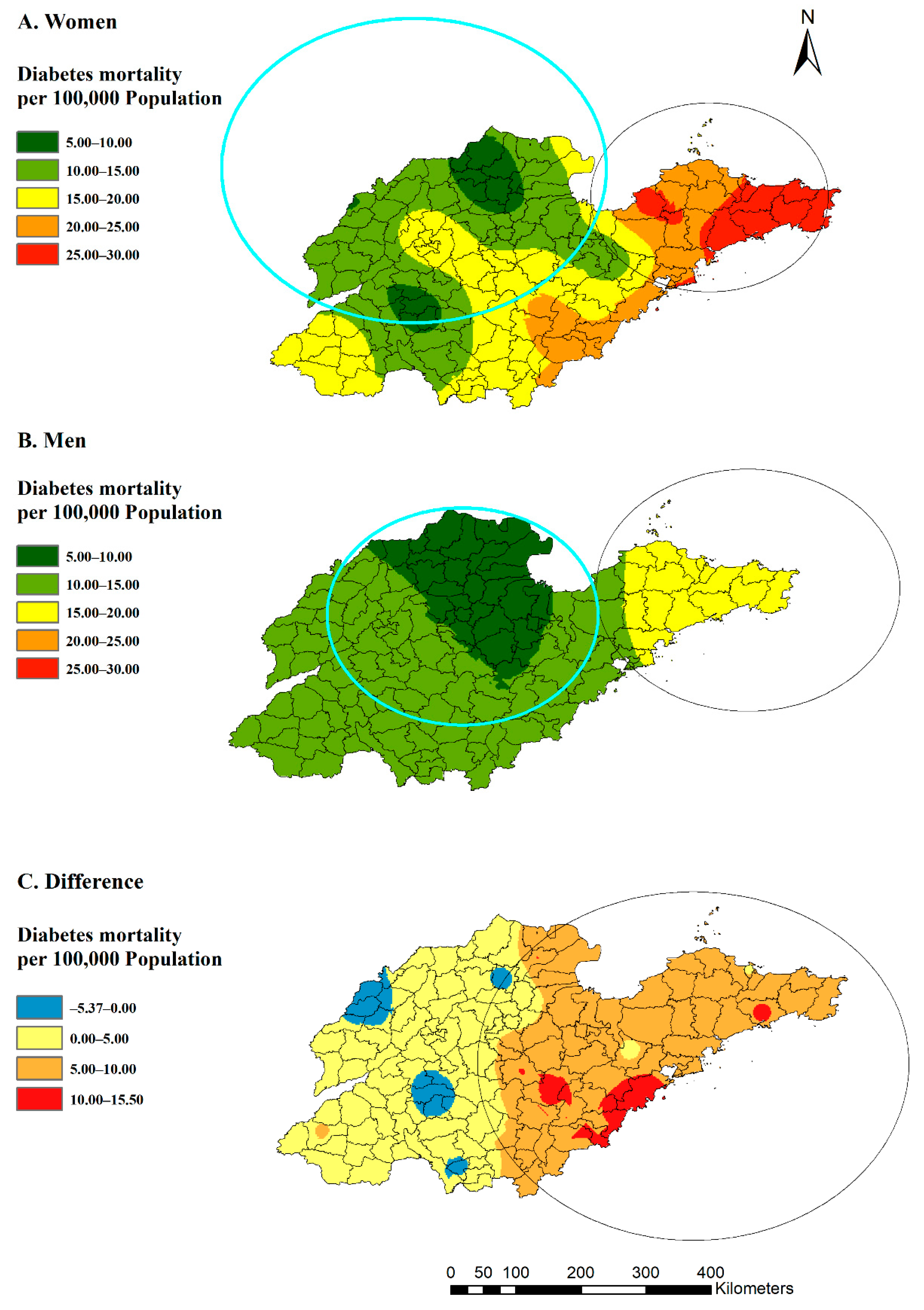
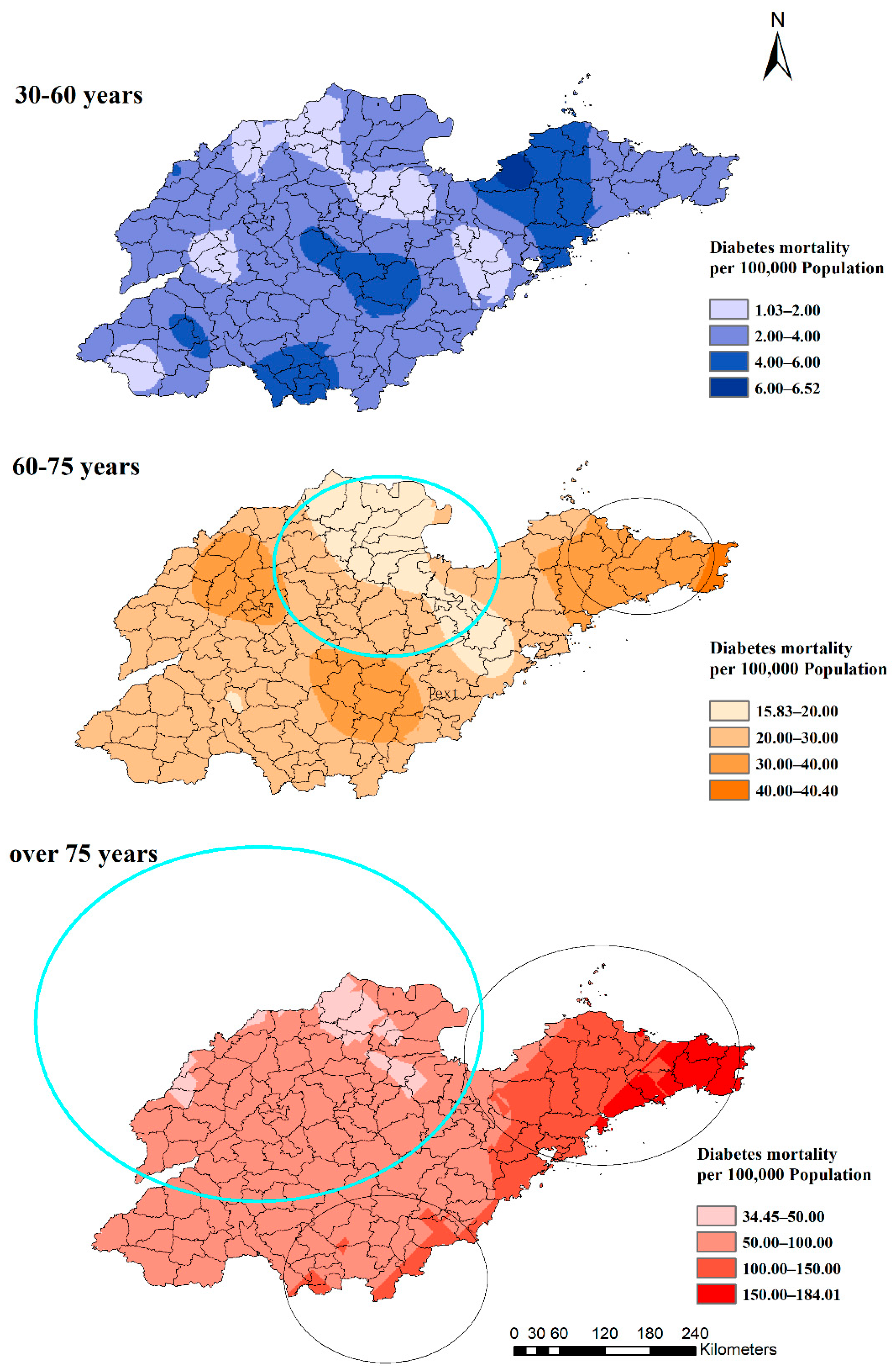
3.3. Spatial Clusters
3.4. Geographical Associations
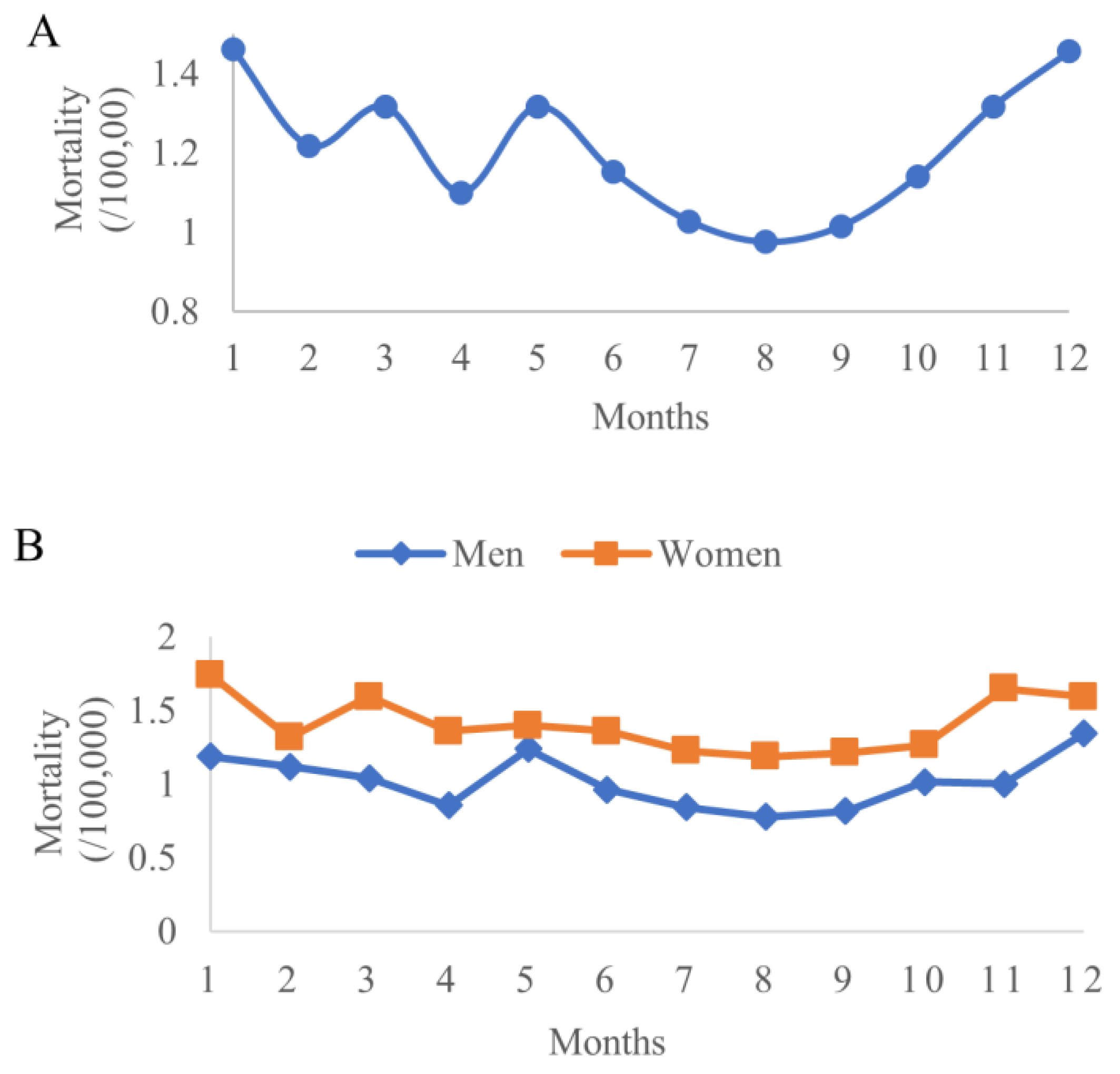
3.5. Seasonality Pattern in Subgroups
3.6. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Diabetes. Available online: https://www.who.int/health-topics/diabetes#tab=tab_1 (accessed on 9 October 2022).
- Whiting, D.R.; Guariguata, L.; Weil, C.; Shaw, J. IDF diabetes atlas: Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res. Clin. Pract. 2011, 94, 311–321. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care 2013, 36 (Suppl. S1), S11–S66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. World Health Statistics Report. Available online: https://www.who.int/publications/i/item/9789240051157 (accessed on 9 October 2022).
- Global Burden of Disease Collaborative Network. Global Health Data Exchange. Available online: https://ghdx.healthdata.org/ (accessed on 10 October 2022).
- Shandong Provincial Bureau of Statistics. Statistical Bulletin of National Economic and Social Development of Shandong Province; Shandong Provincial Bureau of Statistics: Shandong, China, 2015; p. 1.
- Disease and Health Status of Residents in Shandong Province in 2016. Jinan, China, 17 July 2017. Available online: http://www.scio.gov.cn/xwfbh/gssxwfbh/xwfbh/shandong/Document/1558954/1558954.htm (accessed on 11 October 2022).
- Zhang, J.Y.; Chu, J.; Lu, Z.L.; Guo, X.L.; Xu, A.Q. Analysis of mortality and probability of premature death caused by four main non-communicable diseases in Shandong Province, 2015. Chin. J. Prev. Med. 2019, 53, 316–318. [Google Scholar] [CrossRef]
- Liu, M.; Liu, S.W.; Wang, L.J.; Bai, Y.M.; Zeng, X.Y.; Guo, H.B.; Liu, Y.N.; Jiang, Y.Y.; Dong, W.L.; He, G.X.; et al. Burden of diabetes, hyperglycaemia in China from to 2016: Findings from the 1990 to 2016, global burden of disease study. Diabetes Metab. 2019, 45, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Guo, G.; Xu, J.; Yan, X.; Wang, H.; Zhang, L.; Dong, Y. Survey on the trend in the prevalence of Type 2 diabetes and various influence factors of diabetes mellitus among the Qingdao. Front. Med. 2014, 8, 66–68. [Google Scholar] [CrossRef]
- Zhang, G.; Hu, J.; Chen, X.; Xu, C.; Tang, J.; Lu, Z. Morbidity, awareness rate, treatment and control among residents with diabetes (≥18 years old) of Shandong Province in 2013. Chin. J. Prev. Contr. Chron. Dis. 2017, 12, 881–884. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, S.; Gong, S.; Zhou, L.; Zhang, J. Epidemiological characteristics of diabetes mortality in residents, Jinan, 2011–2015. Mod. Prev. Med. 2016, 43, 4337–4340. [Google Scholar]
- Yang, G.; Hu, J.; Rao, K.Q.; Ma, J.; Rao, C.; Lopez, A.D. Mortality registration and surveillance in China: History, current situation and challenges. Popul. Health Metr. 2005, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Wang, L.; Wang, Y.; Jin, S.; Wu, Z.; Chin, D.P.; Koplan, J.P.; Wilson, M.E. Emergence and control of infectious diseases in China. Lancet 2008, 372, 1598–1605. [Google Scholar] [CrossRef]
- Zhou, M.; Jiang, Y.; Huang, Z.; Wu, F. Adjustment and representativeness evaluation of national disease surveillance points system. Dis. Surveill. 2010, 25, 239–244. [Google Scholar] [CrossRef]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Cressie, N. Spatial prediction and kriging. Math. Geol. 1988, 20, 405–421. [Google Scholar] [CrossRef]
- Anselin, L. Local indicators of spatial association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Moran, P.A.P. Notes on continuous stochastic phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Kulldorff, M. SaTScan User Guide. Available online: https://www.satscan.org/cgi-bin/satscan/register.pl/SaTScan_Users_Guide.pdf?todo=process_userguide_download (accessed on 18 August 2022).
- Jarvis, A.; Reuter, H.I.; Nelson, A.; Guevara, E. Hole-Filled Seamless SRTM Data V4. Available online: http://srtm.csi.cgiar.org (accessed on 18 August 2022).
- Zhang, J.; Wang, J.; Xue, F.; Ma, J.; Wu, X. Trend-surface analysis of the geographical distribution of diabetes in Shandong Province. J. Shandong Univ. (Health Sci.) 2003, 41, 387–390. [Google Scholar] [CrossRef]
- Shandong Bureau of Statistics. Shandong Statistics Yearbook; Shandong Bureau of Statistics: Shandong, China, 2015; p. 28.
- Barik, A.; Mazumdar, S.; Chowdhury, A.; Rai, R.K. Physiological and behavioral risk factors of type 2 diabetes mellitus in rural India. BMJ Open Diabetes Res. Care 2016, 4, e000255. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.M.H.; Gruebner, O.; Kraemer, A. The geography of diabetes among the general adults aged 35 years and older in Bangladesh: Recent evidence from a cross-sectional survey. PLoS ONE 2014, 9, e110756. [Google Scholar] [CrossRef] [Green Version]
- Ramachandran, A.; Ma, R.C.W.; Snehalatha, C. Diabetes in Asia. Lancet 2010, 375, 408–418. [Google Scholar] [CrossRef]
- Li, Y.; Lan, L.; Wang, Y.; Yang, C.; Tang, W.; Cui, G.; Luo, S.; Cheng, Y.; Liu, Y.; Liu, J.; et al. Extremely cold and hot temperatures increase the risk of diabetes mortality in metropolitan areas of two Chinese cities. Environ. Res. 2014, 134, 91–97. [Google Scholar] [CrossRef]
- Wang, F.; Wang, W.; Yin, P.; Liu, Y.; Liu, J.; Wang, L.; Qi, J.; You, J.; Lin, L.; Zhou, M. Mortality and Years of Life Lost in Diabetes Mellitus and Its Subcategories in China and Its Provinces, 2005–2020. J. Diabetes Res. 2022, 2022, 1609267. [Google Scholar] [CrossRef]
- Landi, F.; Calvani, R.; Martone, A.M.; Salini, S.; Zazzara, M.B.; Candeloro, M.; Coelho-Junior, H.J.; Tosato, M.; Picca, A.; Marzetti, E. Normative values of muscle strength across ages in a ‘real world’ population: Results from the longevity check-up 7+ project. J. Cachexia Sarcopenia Muscle 2020, 11, 1562–1569. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.G.; Li, Y.C.; Wang, H.D.; Zeng, X.Y.; Wang, L.J.; Liu, S.W.; Liu, Y.N.; Liang, X.F. Analysis on life expectancy and healthy life expectancy in China, 1990–2015. Chin. J. Epidemiol. 2016, 37, 1439–1443. [Google Scholar] [CrossRef]
- Liu, X.; Yu, C.; Wang, Y.; Bi, Y.; Liu, Y.; Zhang, Z. Trends in the Incidence and Mortality of Diabetes in China from 1990 to 2017: A Joinpoint and Age-Period-Cohort Analysis. Int. J. Environ. Res. Public Health 2019, 16, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatling, W.; Guzder, R.N.; Turnbull, J.C.; Budd, S.; Mullee, M.A. The Poole Diabetes Study: How many cases of Type 2 diabetes are diagnosed each year during normal health care in a defined community? Diabetes Res. Clin. Pract. 2001, 53, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Amati, F.; Dubé, J.J.; Coen, P.M.; Stefanovic-Racic, M.; Toledo, F.G.; Goodpaster, B.H. Physical inactivity and obesity underlie the insulin resistance of aging. Diabetes Care 2009, 32, 1547–1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, A.M.; Halter, J.B. Aging and insulin secretion. Am. J. Physiol. Endocrinol. Metab. 2003, 284, E7–E12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, J.E. Diabetes and aging: Epidemiologic overview. Clin. Geriatr Med. 2008, 24, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Yin, P.; Zhou, M.; Ou, C.Q.; Li, M.; Liu, Y.; Gao, J.; Chen, B.; Liu, J.; Bai, L.; et al. The effect of ambient temperature on diabetes mortality in China: A multi-city time series study. Sci. Total Environ. 2016, 543, 75–82. [Google Scholar] [CrossRef]
- Xu, R.; Zhao, Q.; Coelho, M.; Saldiva, P.H.N.; Zoungas, S.; Huxley, R.R.; Abramson, M.J.; Guo, Y.; Li, S. Association between Heat Exposure and Hospitalization for Diabetes in Brazil during 2000–2015: A Nationwide Case-Crossover Study. Environ. Health Perspect. 2019, 127, 117005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Zhou, L.; Chen, K. Burden of cause-specific mortality attributable to heat and cold: A multicity time-series study in Jiangsu Province, China. Environ. Int. 2020, 144, 105994. [Google Scholar] [CrossRef]
- He, Y.; Cheng, L.; Bao, J.; Deng, S.; Liao, W.; Wang, Q.; Tawatsupa, B.; Hajat, S.; Huang, C. Geographical disparities in the impacts of heat on diabetes mortality and the protective role of greenness in Thailand: A nationwide case-crossover analysis. Sci. Total Environ. 2020, 711, 135098. [Google Scholar] [CrossRef] [PubMed]
- Abatzoglou, J.T.; Dobrowski, S.Z.; Parks, S.A.; Hegewisch, K.C. Terraclimate, a high-resolution global dataset of monthly climate and climatic water balance from 1958–2015. Sci. Data 2018, 5, 170191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, W.; Han, S.W.; Tsui, K.L.; Woodall, W.H. Spatiotemporal surveillance methods in the presence of spatial correlation. Stat. Med. 2011, 30, 569–583. [Google Scholar] [CrossRef]
- Lui, C.-W.; Wang, Z.; Wang, N.; Milinovich, G.; Ding, H.; Mengersen, K.; Bambrick, H.; Hu, W. A call for better understanding of social media in surveillance and management of noncommunicable diseases. Health Res. Policy Syst. 2021, 19, 18. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Fatehi, F.; Maiorana, A.; Bashi, N.; Hu, W.; Edwards, I. Digital health for COPD care: The current state of play. J. Thorac. Dis. 2019, 11, S2210–S2220. [Google Scholar] [CrossRef]
- Veazie, S.; Winchell, K.; Gilbert, J.; Paynter, R.; Ivlev, I.; Eden, K.B.; Nussbaum, K.; Weiskopf, N.; Guise, J.M.; Helfand, M. Rapid Evidence Review of Mobile Applications for Self-management of Diabetes. J. Gen. Intern. Med. 2018, 33, 1167–1176. [Google Scholar] [CrossRef] [Green Version]
- Herbert, L.J.; Mehta, P.; Monaghan, M.; Cogen, F.; Streisand, R. Feasibility of the SMART Project: A Text Message Program for Adolescents With Type 1 Diabetes. Diabetes Spectr. 2014, 27, 265–269. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. of Death (n, %) | Population | Rate (per 100,000) |
|---|---|---|---|
| Gender | |||
| Men | 923 | 7,595,650 | 12.15 |
| Spring | 237 (26%) | 3.12 | |
| Summer | 195 (21%) | 2.57 | |
| Autumn | 215 (23%) | 2.83 | |
| Winter | 276 (30%) | 3.63 | |
| Women | 1278 | 7,589,271 | 16.84 |
| Spring | 330 (26%) | 4.35 | |
| Summer | 284 (22%) | 3.74 | |
| Autumn | 312 (24%) | 4.11 | |
| Winter | 352 (28%) | 4.64 | |
| Age | |||
| 30–60 | 351 | 11,001,247 | 3.19 |
| Spring | 94 (27%) | 0.85 | |
| Summer | 78 (22%) | 0.71 | |
| Autumn | 72 (21%) | 0.65 | |
| Winter | 107 (30%) | 0.97 | |
| 60–75 | 812 | 3,078,369 | 26.38 |
| Spring | 217 (27%) | 7.05 | |
| Summer | 162 (20%) | 5.26 | |
| Autumn | 191 (24%) | 6.20 | |
| Winter | 242 (30%) | 7.86 | |
| 75– | 1038 | 1,105,305 | 93.91 |
| Spring | 256 (25%) | 23.16 | |
| Summer | 239 (23%) | 21.62 | |
| Autumn | 264 (25%) | 23.88 | |
| Winter | 279 (27%) | 25.24 | |
| Total (30–) | 2201 | 15,184,921 | 14.49 |
| Variables | Crude OR (95%CI) | Adjusted OR (95%CI) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | Gender | Age | All | Gender | Age | |||||||
| Men | Women | 30–60 | 60–75 | 75– | Men | Women | 30–60 | 60–75 | 75– | |||
| Longitude | 1.13 (1.10–1.16) | 1.12 (1.08–1.16) | 1.18 (1.15–1.21) | 1.18 (1.15–1.21) | 1.03 (1.01–1.05) | 1.14 (1.11–1.16) | 1.11 (1.01–1.23) | 1.08 (0.99–1.19) | 1.17 (1.09–1.25) | 1.04 (0.91–1.19) | 1.01 (0.94–1.07) | 1.21 (1.11–1.33) |
| Latitude | 1.00 (0.95–1.06) | 1.04 (0.97–1.11) | 1.02 (0.96–1.09) | 0.93 (0.83–1.04) | 1.02 (0.98–1.06) | 0.96 (0.91–1.02) | 0.79 (0.64–0.96) | 0.88 (0.73–1.06) | 0.85 (0.73–0.98) | 0.96 (0.73–1.26) | 1.02 (0.89–1.17) | 0.72 (0.59–0.87) |
| Elevation (100 m) | 1.06 (1.01–1.13) | 1.03 (0.98–1.08) | 1.06 (1.01–1.11) | 1.06 (0.99–1.13) | 1.04 (1.00–1.0) | 1.06 (0.99–1.13) | 1.04 (0.98–1.10) | 1.01 (0.96–1.06) | 1.02 (0.98–1.07) | 1.05 (0.98–1.13) | 1.04 (0.99–1.08) | 1.02 (0.97–1.08) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, W.; Chu, J.; Ren, J.; Dong, J.; Bambrick, H.; Wang, N.; Mengersen, K.; Guo, X.; Hu, W. Age- and Gender-Specific Differences in the Seasonal Distribution of Diabetes Mortality in Shandong, China: A Spatial Analysis. Int. J. Environ. Res. Public Health 2022, 19, 17024. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192417024
Zheng W, Chu J, Ren J, Dong J, Bambrick H, Wang N, Mengersen K, Guo X, Hu W. Age- and Gender-Specific Differences in the Seasonal Distribution of Diabetes Mortality in Shandong, China: A Spatial Analysis. International Journal of Environmental Research and Public Health. 2022; 19(24):17024. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192417024
Chicago/Turabian StyleZheng, Wenxiu, Jie Chu, Jie Ren, Jing Dong, Hilary Bambrick, Ning Wang, Kerrie Mengersen, Xiaolei Guo, and Wenbiao Hu. 2022. "Age- and Gender-Specific Differences in the Seasonal Distribution of Diabetes Mortality in Shandong, China: A Spatial Analysis" International Journal of Environmental Research and Public Health 19, no. 24: 17024. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192417024