

“Dignity as a Small Candle Flame That Doesn’t Go Out!”: An Interpretative Phenomenological Study with Patients Living with Advanced Chronic Obstructive Pulmonary Disease

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Recruitment
2.3. Data Collection
2.4. Data Analysis
2.5. Trustworthiness
2.6. Ethical Considerations
3. Results
3.1. Sample Description
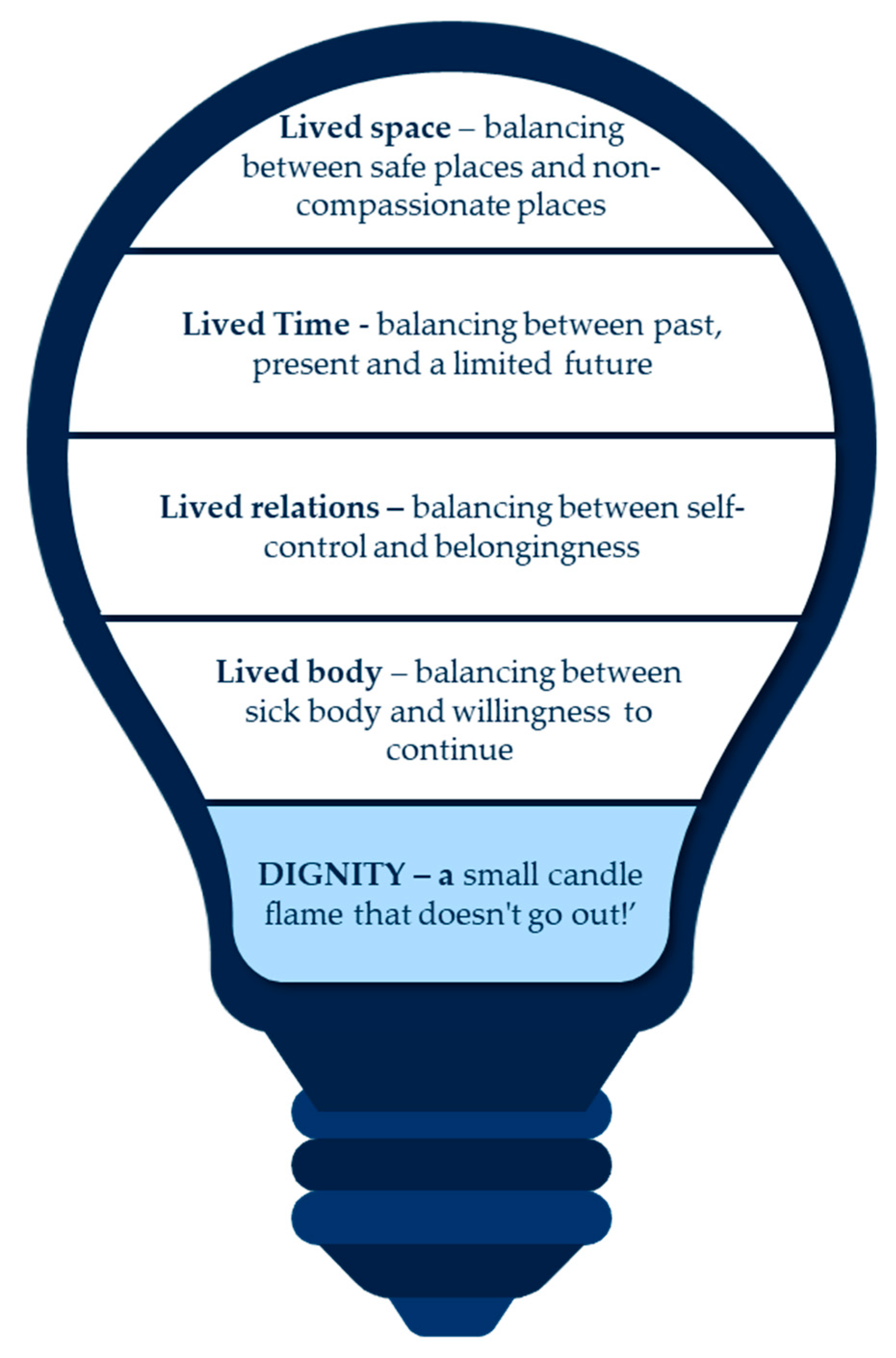
3.2. Findings from Interviews
3.2.1. Lived Body—Balancing between Sick Body and Willingness to Continue
P3: “Shortness of breath is unpredictable, it appears every three or four weeks–it feels like I’m drowning, it’s horrible. The tiredness and anxiety are terrible… my body is exhausted, and in those moments, I think I’m going to die.”
P1: “The despair of being able to breathe and not being able to, generates a frustration that limits me. I think about what I was, the energetic person who did everything independently. And now [pause]… I feel trapped in my body, it doesn’t obey my will!”
P4: “My legs hurt; my muscles are stuck. Again and again, my body limits me. But I stay active until I can’t do anything else. Because if I don’t, my life will lose its meaning.”
P8: “Currently I have difficulty doing activities that I used to do without any problem… I feel a slowdown in all my activities, and this affects me a lot.”
3.2.2. Lived Relations—Balancing between Self-Control and Belongingness
P16: ”the disease allowed me to strengthen ties in my family! I had an older brother with whom I didn’t have much connection, in fact, we had been apart for years, and since he found out I was worse he came to see me! I’m very happy…”
P20: “there is one thing that the disease brought, it was family unity, my grandchildren see my condition and are always available for whatever I need. Just last week they took me for a walk, I went to see the sea… (crying), I couldn’t remember that feeling anymore.”
3.2.3. Lived Time—Balancing between Past, Present and a Limited Future
P2: “I feel like a matryoshka, as time passes, I feel smaller, more compressed with the clear certainty that many of my desires will not be possible to come true… in the most difficult moments I resort to prayer to find some strength to carry on!”
P10: “If I die today, I will have the opportunity to live again… I have the impression that God is around me… I know I may confess my transgressions to him, and that he will forgive me. I can tell you everything since he’s a terrific buddy I can rely on.”
P18: “God… give me strength… I have no fears.”
P10: “I’m never alone, I have faith and hope… I think that tomorrow I’ll be a little better.”
3.2.4. Lived Space—Balancing between Safe Places and Non-Compassionate Places
P6: “My house is all I have, I helped build it and that makes it a part of me. So, when I die, I want to be here… surrounded by those who love me; P9: When I get up in the morning, I look out my window and I see my backyard, the trees I’ve planted, and I think how good it is to be here.”
4. Discussion
4.1. Study Limitations
4.2. Implications for Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Viegi, G.; Maio, S.; Fasola, S.; Baldacci, S. Global Burden of Chronic Respiratory Diseases. J. Aerosol. Med. Pulm. Drug Deliv. 2020, 33, 171–177. [Google Scholar] [CrossRef]
- Iheanacho, I.; Zhang, S.; King, D.; Rizzo, M.; Ismaila, A.S. Economic Burden of Chronic Obstructive Pulmonary Disease (COPD): A Systematic Literature Review. Int. J. Chron. Obs. Pulmon. Dis. 2020, 15, 439–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2020 Report. 2020. Available online: https://goldcopd.org/wp-content/uploads/2019/11/GOLD-2020-REPORT-ver1.0wms.pdf (accessed on 11 August 2022).
- Hurst, J.R.; Winders, T.; Worth, H.; Bhutani, M.; Gruffydd-Jones, K.; Stolz, D.; Dransfield, M.T. A Patient Charter for Chronic Obstructive Pulmonary Disease. Adv. Ther. 2021, 38, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Butorac-Petanjek, B.; Chilosi, M.; Cosío, B.G.; Flezar, M.; Koulouris, N.; Marin, J.; Miculinic, N.; Polese, G.; Samaržija, M.; et al. Chronic obstructive pulmonary disease with mild airflow limitation: Current knowledge and proposal for future research-a consensus document from six scientific societies. Int. J. Chron. Obs. Pulmon. Dis. 2017, 12, 2593–2610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lecheler, L.; Richter, M.; Franzen, D.P.; Rampini, S.K.; Cheetham, M.; Jenewein, J.; Battegay, E.; Nowak, A. The frequent and underrecognised co-occurrence of acute exacerbated COPD and depression warrants screening: A systematic review. Eur. Respir. Rev. 2017, 26, 170026. [Google Scholar] [CrossRef] [Green Version]
- Henoch, I.; Ekberg-Jansson, A.; Löfdahl, C.G.; Strang, P. Benefits, for patients with late stage chronic obstructive pulmonary disease, of being cared for in specialized palliative care compared to hospital. A nationwide register study. BMC Palliat. Care 2021, 20, 130. [Google Scholar] [CrossRef]
- Noppe, D.; Veen, H.; Mooren, K. COPD patients in need of palliative care: Identification after hospitalization through the surprise question. Chron. Respir. Dis. 2019, 16, 1479972318796219. [Google Scholar] [CrossRef]
- Braço Forte, C.; Sousa, S. End of life in COPD patients: Time for a change. Breathe 2017, 13, e84–e86. [Google Scholar] [CrossRef]
- Bolton, L.E.; Seymour, J.; Gardiner, C. Existential suffering in the day to day lives of those living with palliative care needs arising from chronic obstructive pulmonary disease (COPD): A systematic integrative literature review. Palliat. Med. 2022, 36, 567–580. [Google Scholar] [CrossRef]
- Rosa, F.; Bagnasco, A.; Ghirotto, L.; Rocco, G.; Catania, G.; Aleo, G.; Zanini, M.; Dasso, N.; Hayter, M.; Sasso, L. Experiences of older people following an acute exacerbation of chronic obstructive pulmonary disease: A phenomenological study. J. Clin. Nurs. 2018, 27, e1110–e1119. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Universal Declaration of Human Rights, 2022. Available online: https://www.un.org/en/about-us/universal-declaration-of-human-rights (accessed on 14 August 2022).
- Edlund, M.; Lindwall, L.; von Post, I.; Lindström, U.Å. Concept determination of human dignity. Nurs. Ethics 2013, 20, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Gysels, M.; Reilly, C.C.; Jolley, C.J.; Pannell, C.; Spoorendonk, F.; Moxham, J.; Bausewein, C.; Higginson, I.J. Dignity Through Integrated Symptom Management: Lessons from the Breathlessness Support Service. J. Pain Symptom Manag. 2016, 52, 515–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellver Capella, V. Vigencia del concepto de dignidad humana en los cuidados de salud: Una perspectiva literaria [Validity of the concept of human dignity in health care: A literary perspective]. Cuad. Bioet. 2019, 30, 237–252. [Google Scholar] [PubMed]
- Tranvåg, O.; Petersen, K.A.; Nåden, D. Relational interactions preserving dignity experience: Perceptions of persons living with dementia. Nurs. Ethics 2015, 22, 577–593. [Google Scholar] [CrossRef]
- Nordenfelt, L.; Edgar, A. The four notions of dignity. Qual. Ageing 2005, 6, 17–21. [Google Scholar] [CrossRef]
- Stephen Ekpenyong, M.; Nyashanu, M.; Ossey-Nweze, C.; Serrant, L. Exploring the perceptions of dignity among patients and nurses in hospital and community settings: An integrative review. J. Res. Nurs. 2021, 26, 517–537. [Google Scholar] [CrossRef]
- Lindwall, L.; Lohne, V. Human dignity research in clinical practice-a systematic literature review. Scand. J. Caring Sci. 2021, 35, 1038–1049. [Google Scholar] [CrossRef]
- Chochinov, H.M.; Hack, T.; McClement, S.; Kristjanson, L.; Harlos, M. Dignity in the terminally ill: A developing empirical model. Soc. Sci. Med. 2002, 54, 433–443. [Google Scholar] [CrossRef]
- Harstäde, C.W.; Blomberg, K.; Benzein, E.; Östlund, U. Dignity-conserving care actions in palliative care: An integrative review of Swedish research. Scand. J. Caring Sci. 2017, 32, 8–23. [Google Scholar] [CrossRef]
- Sæteren, B.; Nåden, D. Dignity: An Essential Foundation for Promoting Health and Well-Being. In Health Promotion in Health Care–Vital Theories and Research; Haugan, G., Eriksson, M., Eds.; Springer: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Chang, Y.Y.; Dai, Y.T.; Chien, N.H.; Chan, H.Y. The Lived Experiences of People with Chronic Obstructive Pulmonary Disease: A Phenomenological Study. J. Nurs. Scholarsh. 2016, 48, 466–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Disler, R.T.; Green, A.; Luckett, T.; Newton, P.J.; Inglis, S.; Currow, D.C.; Davidson, P.M. Experience of advanced chronic obstructive pulmonary disease: Metasynthesis of qualitative research. J. Pain Symptom. Manag. 2014, 48, 1182–1199. [Google Scholar] [CrossRef] [PubMed]
- Barken, T.L.; Thygesen, E.; Söderhamn, U. Unlocking the limitations: Living with chronic obstructive pulmonary disease and receiving care through telemedicine-A phenomenological study. J. Clin. Nurs. 2018, 27, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Galvin, K. ‘Getting back to the matters’: Why the existential matters in care. Scand. J. Caring Sci. 2021, 35, 679–684. [Google Scholar] [CrossRef] [PubMed]
- van Manen, M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy, 2nd ed.; Routledge: London, UK, 1997. [Google Scholar]
- Van Manen, M. Phenomenology of Practice: Meaning-Giving Methods in Phenomenological Research and Writing, 1st ed.; Routledge: London, UK, 2014. [Google Scholar] [CrossRef]
- O'Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Laverty, S.M. Hermeneutic phenomenology and phenomenology: A comparison of historical and methodological considerations. Int. J. Qual. Methods 2003, 2, 21–35. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lund Disease (GOLD). Global Strategy for Prevention, Diagnosis and Management of COPD. 2022. Available online: https://goldcopd.org/2021-gold-reports/ (accessed on 14 August 2022).
- Bakthavatsalu, B.; Walshe, C.; Simpson, J. The experience of hospitalization in people with advanced chronic obstructive pulmonary disease: A qualitative, phenomenological study. Chronic Illn. 2022, 17423953211073580. [Google Scholar] [CrossRef]
- Apóstolo, J. Geriatric Instruments, 1st ed.; ESEnfC: Coimbra, Portugal, 2012. [Google Scholar]
- McPherson, P.J. “A metamorphosis of the educator”: A hermeneutic phenomenology study of the perceptions and lived experiences of the 6–12 educator in transitioning from teacher-centered to student-centered learning. Competency-Based Educ. 2021, 6, e01230. [Google Scholar] [CrossRef]
- Creswell, J.W. Educational Research: Planning, Conducting, and Evaluating Quantitative and Qualitative Research, 5th ed.; Pearson: London, UK, 2015. [Google Scholar]
- Saldaña, J. The coding Manual for Qualitative Researchers, 3rd ed.; Sage Publications: London, UK, 2016. [Google Scholar]
- Korstjens, I.; Moser, A. Series: Practical guidance to qualitative research. Part 4: Trustworthiness and publishing. Eur. J. Gen. Pract. 2018, 24, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Pooler, C. Living with Chronic Lower Pulmonary Disease: Disruptions of the Embodied Phenomenological Self. Glob. Qual. Nurs. Res. 2014, 1, 2333393614548762. [Google Scholar] [CrossRef]
- van der Meide, H.; Teunissen, T.; Visser, L.H.; Visse, M. Trapped in my lungs and fighting a losing battle. A phenomenological study of patients living with chronic obstructive and pulmonary disease. Scand. J. Caring Sci. 2020, 34, 118–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Prat, A.; Escribano, X. A Philosophical View on the Experience of Dignity and Autonomy through the Phenomenology of Illness. J. Med. Philos. 2019, 44, 279–298. [Google Scholar] [CrossRef] [PubMed]
- Bruun Lorentsen, V.; Nåden, D.; Sæteren, B. The meaning of dignity when the patients' bodies are falling apart. Nurs. Open 2019, 6, 1163–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laranjeira, C.A.; Leão, P.P.; Leal, I. The "silenced" voices of women cancer survivors: Bodily experiences from an existential perspective. Res. Theory Nurs. Pract. 2013, 27, 173–192. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.M.; Zhang, M.R.; Yang, C.H.; Li, Y. The meaning of life according to patients with advanced lung cancer: A qualitative study. Int. J. Qual. Stud. Health Well-Being 2022, 17, 2028348. [Google Scholar] [CrossRef]
- Almeida, S.N.; Elliott, R.; Silva, E.R.; Sales, C.M. Fear of cancer recurrence: A qualitative systematic review and meta-synthesis of patients’ experiences. Clin. Psychol. Rev. 2019, 68, 13–24. [Google Scholar] [CrossRef] [Green Version]
- Grassi, L.; Nanni, M.G. Demoralization syndrome: New insights in psychosocial cancer care. Cancer 2016, 122, 2130–2133. [Google Scholar] [CrossRef] [Green Version]
- Robinson, S.; Kissane, D.W.; Brooker, J.; Burney, S. A systematic review of the demoralization syndrome in individuals with progressive disease and cancer: A decade of research. J. Pain Symptom Manag. 2015, 49, 595–610. [Google Scholar] [CrossRef]
- Gómez-Vírseda, C.; de Maeseneer, Y.; Gastmans, C. Relational autonomy: What does it mean and how is it used in end-of-life care? A systematic review of argument-based ethics literature. BMC Med. Ethics 2019, 20, 76. [Google Scholar] [CrossRef] [Green Version]
- Ho, A.H.; Leung, P.P.; Tse, D.M.; Pang, S.M.; Chochinov, H.M.; Neimeyer, R.A.; Chan, C.L. Dignity amidst liminality: Healing within suffering among Chinese terminal cancer patients. Death Stud. 2013, 37, 953–970. [Google Scholar] [CrossRef] [Green Version]
- Leget, C. Forgiveness and Reconciliation in Palliative Care: The Gap between the Psychological and Moral Approaches. Religions 2020, 11, 440. [Google Scholar] [CrossRef]
- Breitbart, W. Legacy in palliative care: Legacy that is lived. Palliat. Support. Care 2016, 14, 453–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.E.; Haupt, E.C.; Nau, C.; Werch, H.; McMullen, C.; Lynn, J.; Shen, E.; Mularski, R.A.; Nguyen, H.Q.; HomePal Research Group. Association between Financial Distress with Patient and Caregiver Outcomes in Home-Based Palliative Care: A Secondary Analysis of a Clinical Trial. J. Gen. Intern. Med. 2022, 37, 3029–3037. [Google Scholar] [CrossRef]
- Benson, J.J.; Parker Oliver, D.; Demiris, G.; Washington, K. Accounts of Family Conflict in Home Hospice Care: The Central Role of Autonomy for Informal Caregiver Resilience. J. Fam. Nurs. 2019, 25, 190–218. [Google Scholar] [CrossRef]
- Rodríguez-Prat, A.; Monforte-Royo, C.; Porta-Sales, J.; Escribano, X.; Balaguer, A. Patient Perspectives of Dignity, Autonomy and Control at the End of Life: Systematic Review and Meta-Ethnography. PLoS ONE 2016, 11, e0151435. [Google Scholar] [CrossRef] [PubMed]
- Alm Andreassen, T. Service user involvement and repositioning of health care professionals: A framework for examining implications of different forms of involvement. Nordic Welfare Res. 2018, 3, 58–69. [Google Scholar] [CrossRef] [Green Version]
- Holmen, H.; Larsen, M.H.; Sallinen, M.H.; Thoresen, L.; Ahlsen, B.; Andersen, M.H.; Borge, C.R.; Eik, H.; Wahl, A.K.; Mengshoel, A.M. Working with patients suffering from chronic diseases can be a balancing act for health care professionals-a meta-synthesis of qualitative studies. BMC Health Serv. Res. 2020, 20, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bragadottir, G.H.; Halldorsdottir, B.S.; Ingadottir, T.S.; Jonsdottir, H. Patients and families realising their future with chronic obstructive pulmonary disease—A qualitative study. J. Clin. Nurs. 2018, 27, 57–64. [Google Scholar] [CrossRef]
- Jerpseth, H.; Knutsen, I.R.; Jensen, K.T.; Halvorsen, K. Mirror of shame: Patients experiences of late-stage COPD. A qualitative study. J. Clin. Nurs. 2021, 30, 2854–2862. [Google Scholar] [CrossRef]
- Pinnock, H.; Kendall, M.; Murray, S.A.; Worth, A.; Levack, P.; Porter, M.; MacNee, W.; Sheikh, A. Living and dying with severe chronic obstructive pulmonary disease: Multi-perspective longitudinal qualitative study. BMJ 2011, 342, d142. [Google Scholar] [CrossRef] [Green Version]
- Jowsey, T.; Yen, L.E.; Bagheri, N.; McRae, I.S. Time spent by people managing chronic obstructive pulmonary disease indicates biographical disruption. Int. J. Chron. Obs. Pulmon. Dis. 2014, 9, 87–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jowsey, T. Time and chronic illness: A narrative review. Qual. Life Res. 2016, 25, 1093–1102. [Google Scholar] [CrossRef] [PubMed]
- Fitch, M.I.; Bartlett, R. Patient Perspectives about Spirituality and Spiritual Care. Asia Pac. J. Oncol. Nurs. 2019, 6, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Hemati, Z.; Ashouri, E.; AllahBakhshian, M.; Pourfarzad, Z.; Shirani, F.; Safazadeh, S.; Ziyaei, M.; Varzeshnejad, M.; Hashemi, M.; Taleghani, F. Dying with dignity: A concept analysis. J. Clin. Nurs. 2016, 25, 1218–1228. [Google Scholar] [CrossRef] [PubMed]
- Sagha Zadeh, R.; Eshelman, P.; Setla, J.; Kennedy, L.; Hon, E.; Basara, A. Environmental Design for End-of-Life Care: An Integrative Review on Improving the Quality of Life and Managing Symptoms for Patients in Institutional Settings. J. Pain Symptom Manag. 2018, 55, 1018–1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendelboe-Nelson, C.; Kelly, S.; Kennedy, M.; Cherrie, J.W. A Scoping Review Mapping Research on Green Space and Associated Mental Health Benefits. Int. J. Environ. Res. Public Health 2019, 16, 2081. [Google Scholar] [CrossRef] [Green Version]
- Pearson, D.G.; Craig, T. The great outdoors? Exploring the mental health benefits of natural environments. Front. Psychol. 2014, 5, 1178. [Google Scholar] [CrossRef]
- Seymour, V. The Human-Nature Relationship and Its Impact on Health: A Critical Review. Front. Public Health 2016, 4, 260. [Google Scholar] [CrossRef]
- Pollock, K. Is home always the best and preferred place of death? BMJ 2015, 351, h4855. [Google Scholar] [CrossRef]
- Driessen, A.; Borgstrom, E.; Cohn, S. Placing death and dying: Making place at the end of life. Soc. Sci. Med. 2021, 291, 113974. [Google Scholar] [CrossRef]
- Sinclair, S.; Kondejewski, J.; Jaggi, P.; Dennett, L.; Roze des Ordons, A.L.; Hack, T.F. What is the state of compassion education? A systematic review of compassion training in health care. Acad. Med. 2021, 96, 1057–1070. [Google Scholar] [CrossRef] [PubMed]
- Malenfant, S.; Jaggi, P.; Hayden, K.A.; Sinclair, S. Compassion in healthcare: An updated scoping review of the literature. BMC Palliat. Care 2022, 21, 80. [Google Scholar] [CrossRef]
- Fusi-Schmidhauser, T.; Riglietti, A.; Froggatt, K.; Preston, N. Palliative care provision for patients with advanced chronic obstructive pulmonary disease: A systematic integrative literature review. COPD 2018, 15, 600–611. [Google Scholar] [CrossRef] [PubMed]
- da Cruz, M.B.; Nunes, R. Palliative care and the Portuguese health system. Porto Biomed. J. 2016, 1, 72–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacomini, M.; DeJean, D.; Simeonov, D.; Smith, A. Experiences of living and dying with COPD: A systematic review and synthesis of the qualitative empirical literature. Ont. Health Technol. Assess. Ser. 2012, 12, 1–47. [Google Scholar] [PubMed]
- Clari, M.; Ivziku, D.; Casciaro, R.; Matarese, M. The Unmet Needs of People with Chronic Obstructive Pulmonary Disease: A Systematic Review of Qualitative Findings. COPD 2018, 15, 79–88. [Google Scholar] [CrossRef]
- Fusi-Schmidhauser, T.; Froggatt, K.; Preston, N. Living with Advanced Chronic Obstructive Pulmonary Disease: A Qualitative Interview Study with Patients and Informal Carers. COPD 2020, 17, 410–418. [Google Scholar] [CrossRef]
- Lévinas, E. Totalidade e Infinito, [Totality and Infinity], 3rd ed.; Edições 70: Lisboa, Portugal, 2008. [Google Scholar]
- Neubauer, B.E.; Witkop, C.T.; Varpio, L. How phenomenology can help us learn from the experiences of others. Perspect. Med. Educ. 2019, 8, 90–97. [Google Scholar] [CrossRef]


{kind=link}
| Participant | Age (Years) | Sex | Marital Status | Educational Level | Job Status | Time Since Diagnosis (Years) | GOLD Class * |
|---|---|---|---|---|---|---|---|
| P1 | 63 | Male | Married | Secondary education | Retired | 4 | Stage III |
| P2 | 59 | Male | Divorced | Secondary education | Unemployed | 8 | Stage IV |
| P3 | 66 | Female | Married | Secondary education | Retired | 4.5 | Stage III |
| P4 | 63 | Male | Married | Secondary education | Unemployed | 4 | Stage III |
| P5 | 59 | Male | Widowed | Higher education | Unemployed | 4 | Stage III |
| P6 | 71 | Male | Divorced | Secondary education | Retired | 5 | Stage III |
| P7 | 74 | Male | Married | Basic education | Retired | 6 | Stage III |
| P8 | 70 | Female | Married | Secondary education | Retired | 4.5 | Stage III |
| P9 | 68 | Male | Married | Higher education | Retired | 7 | Stage III |
| P10 | 58 | Male | Single | Secondary education | Unemployed | 4.5 | Stage III |
| P11 | 65 | Male | Married | Secondary education | Retired | 5 | Stage III |
| P12 | 58 | Male | Married | Higher education | Unemployed | 8 | Stage IV |
| P13 | 62 | Male | Married | Secondary education | Retired | 5.5 | Stage IV |
| P14 | 70 | Male | Married | Secondary education | Retired | 8 | Stage IV |
| P15 | 73 | Female | Married | Basic education | Retired | 3.5 | Stage III |
| P16 | 62 | Female | Married | Higher education | Retired | 9 | Stage IV |
| P17 | 82 | Male | Widowed | Basic education | Retired | 6 | Stage III |
| P18 | 74 | Male | Married | Basic education | Retired | 4 | Stage III |
| P19 | 60 | Male | Married | Secondary education | Retired | 7 | Stage III |
| P20 | 80 | Female | Married | Secondary education | Retired | 11 | Stage IV |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laranjeira, C.; Dourado, M. “Dignity as a Small Candle Flame That Doesn’t Go Out!”: An Interpretative Phenomenological Study with Patients Living with Advanced Chronic Obstructive Pulmonary Disease. Int. J. Environ. Res. Public Health 2022, 19, 17029. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192417029
Laranjeira C, Dourado M. “Dignity as a Small Candle Flame That Doesn’t Go Out!”: An Interpretative Phenomenological Study with Patients Living with Advanced Chronic Obstructive Pulmonary Disease. International Journal of Environmental Research and Public Health. 2022; 19(24):17029. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192417029
Chicago/Turabian StyleLaranjeira, Carlos, and Marília Dourado. 2022. "“Dignity as a Small Candle Flame That Doesn’t Go Out!”: An Interpretative Phenomenological Study with Patients Living with Advanced Chronic Obstructive Pulmonary Disease" International Journal of Environmental Research and Public Health 19, no. 24: 17029. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192417029