
Public R&D Projects-Based Investment and Collaboration Framework for an Overarching South Korean National Strategy of Personalized Medicine

Abstract
:1. Introduction
1.1. Background Study through Literature Review
1.1.1. PM Initiative in South Korea
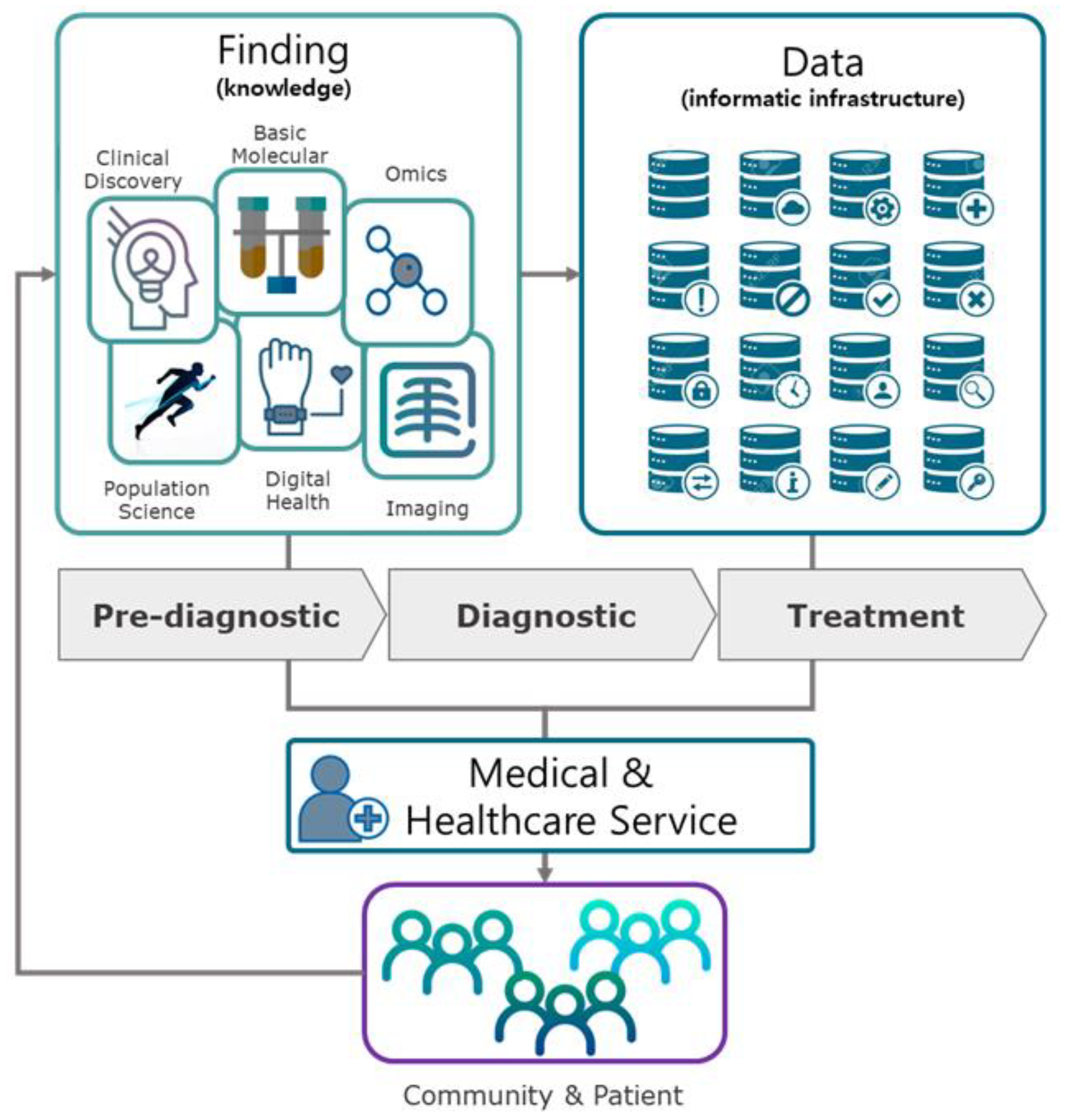
1.1.2. Main Elements in the Value Chain of Personalized Medicine
1.1.3. Theories and Empirical Review
1.2. Research Purpose and Questions
- Research Question 1-1: What are the expenditures of R&D projects in PM-related fields in which the South Korea government has invested over the past 5 years (2015–2020)?
- Research Question 1-2: What are the expenditures of R&D projects in PM-related fields in which the South Korea government has invested from a regional perspective?
- Research Question 2-1: What has been the trend of investment in PM-related fields in which the South Korea government has invested over the past 5 years (2015–2020)?
- Research Question 2-2: What were the regional portions of the government R&D funding in PM-related technologies?
- Research Question 3-1: What kinds of organizations (university, industry, research institutes, and hospital) have contributed to PM-related technologies from a viewpoint of regions?
- Research Question 3-2: From a regional perspective, which organizations may be served as overarching collaborative R&D partners in each PM-related technology?
2. Materials and Methods
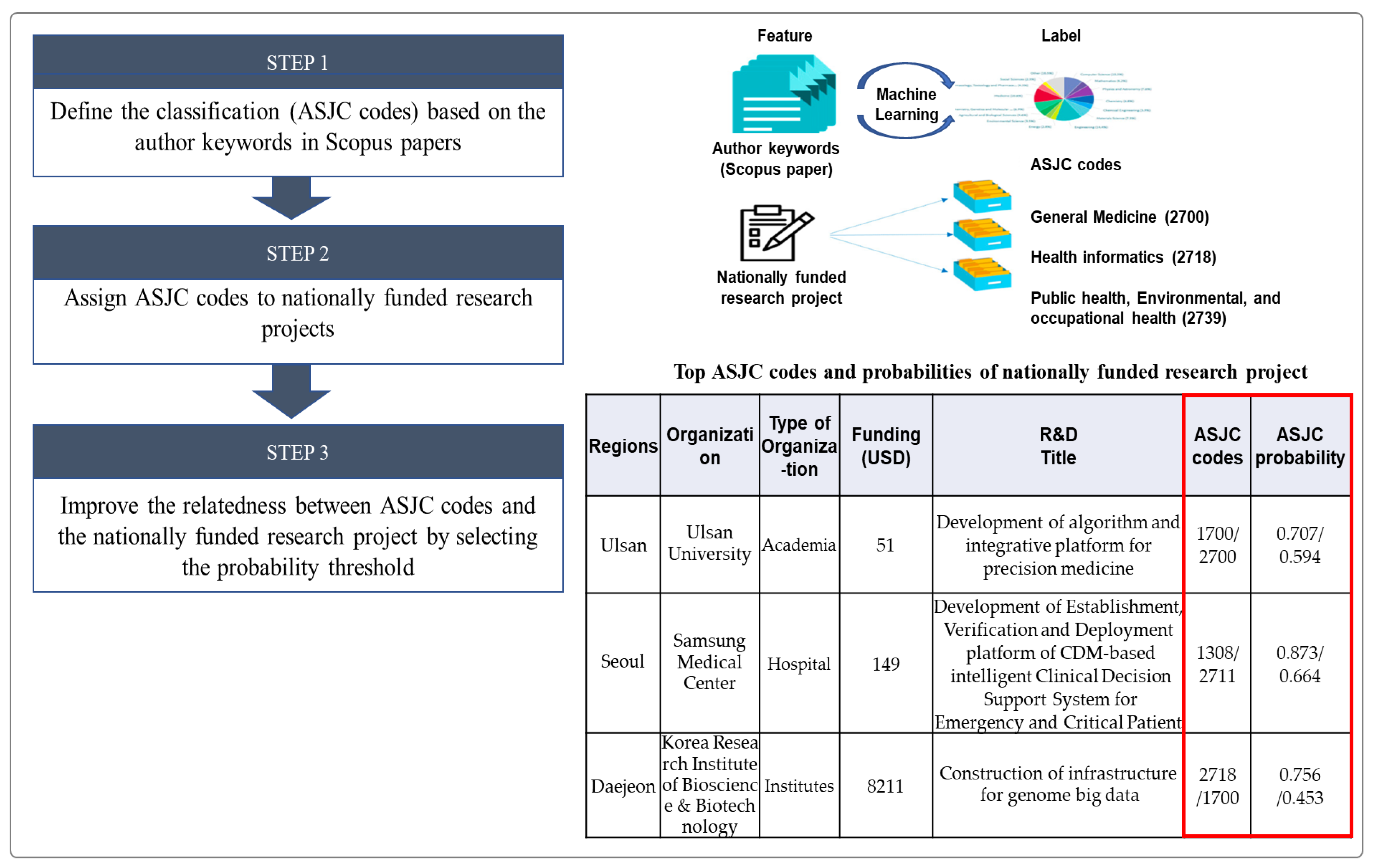
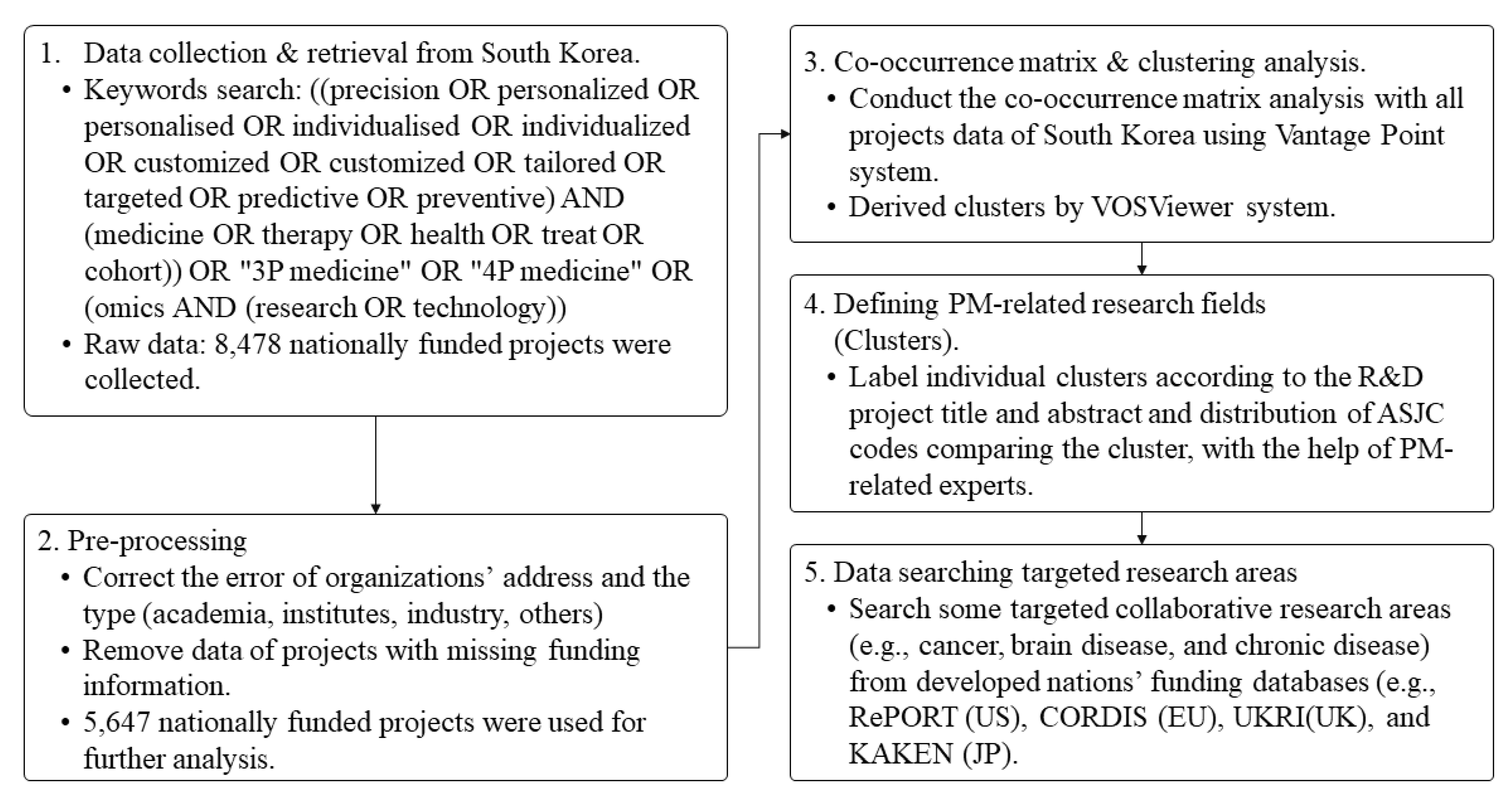
2.1. Data Collection and Preprocessing
2.2. Co-Occurrence Matrix
2.3. Clustering and Network Visualization
2.4. Defining the PM-Related Research Fields
3. Results
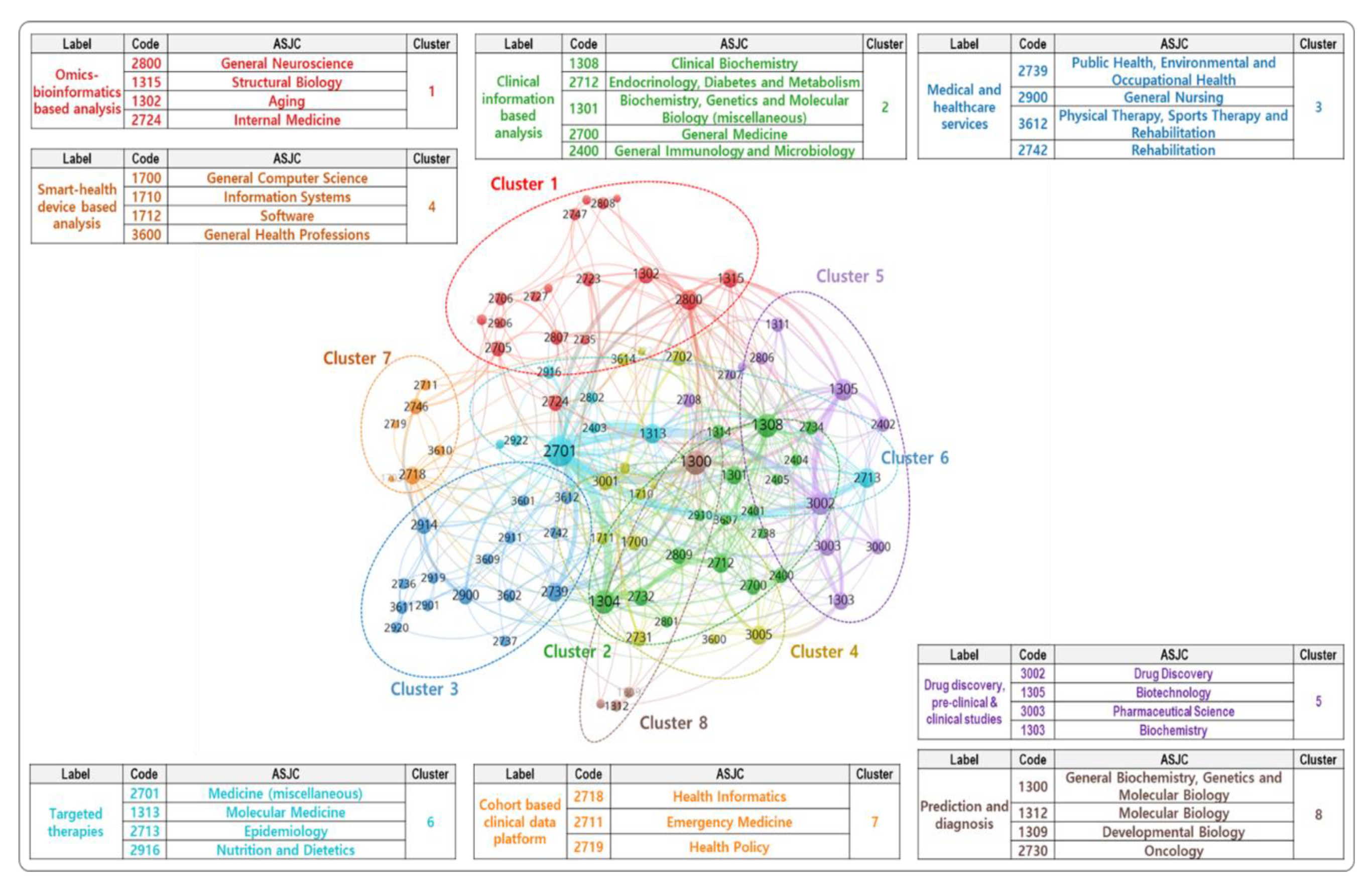
3.1. PM-Related Research Fields of Public R&D Projects
- Cluster 1. Bigdata infrastructure for PM (Omics: Omics-bioinformatics based analysis): Research on the establishment of a core infrastructure for PM based on human informatics, including genomics, transcriptomics, proteomics, and metabolomics.
- Cluster 2. Empirical and clinical studies for PM (Clinical information: Clinical information-based analysis): Research on the system that collects daily life health information, such as pulse and heartrate from wearable devices for personal health management.
- Cluster 3. Medical and healthcare services (Service: Medical and healthcare services): Research on data infrastructure that allows storing, processing, and analyzing various medical bigdata (genomic information, health and disease information, living environmental information), while collecting and integrating various medical and health sources such as personal, hospital, and government agencies.
- Cluster 4. Bigdata infrastructure for PM (Smart-health: Smart-health device-based analysis): Research on the development and verification of algorithms that use medical bigdata from various medical and health sources.
- Cluster 5. Empirical and clinical studies for PM (Drug: Drug discovery, pre-clinical, and clinical studies): Research on the companion diagnosis, molecular diagnosis, pharmacogenomic analysis, early diagnosis, liquid biopsy technology, and pre-clinical/clinical test.
- Cluster 6. Empirical and clinical studies for PM (Therapies: Targeted therapies): Research on biomarker analysis utilization, diagnostic kit (next-generation sequencing panel, single nucleotide polymorphisms chip, biochip), and AI-based decision-making support.
- Cluster 7. Bigdata infrastructure for PM (Cohort: Cohort-based clinical data platform): Clinical research on developing personalized treatments including drug prescriptions, medical devices, and treatment programs based on specific genes and environmental factors using medical and health bigdata.
- Cluster 8. Empirical and clinical studies for PM (Prediction: Prediction and diagnosis): Research on the public health service to promote PM industry through adopting disease genome analysis service, direct to consumer, and decision support system application in the current medical system.
3.2. Status of Government Investment in PM
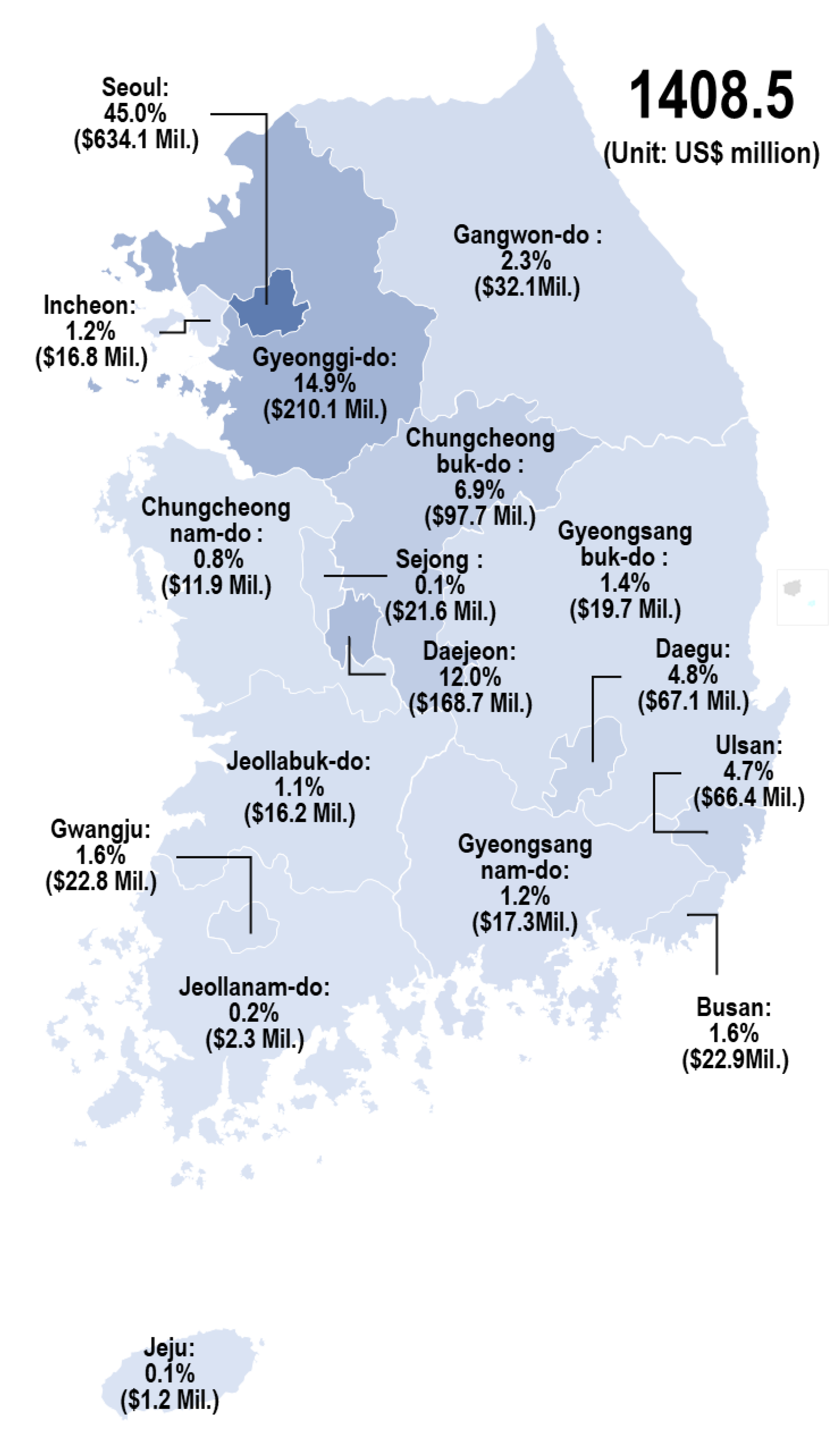
3.2.1. Status of Public R&D Projects from a Regional Perspective
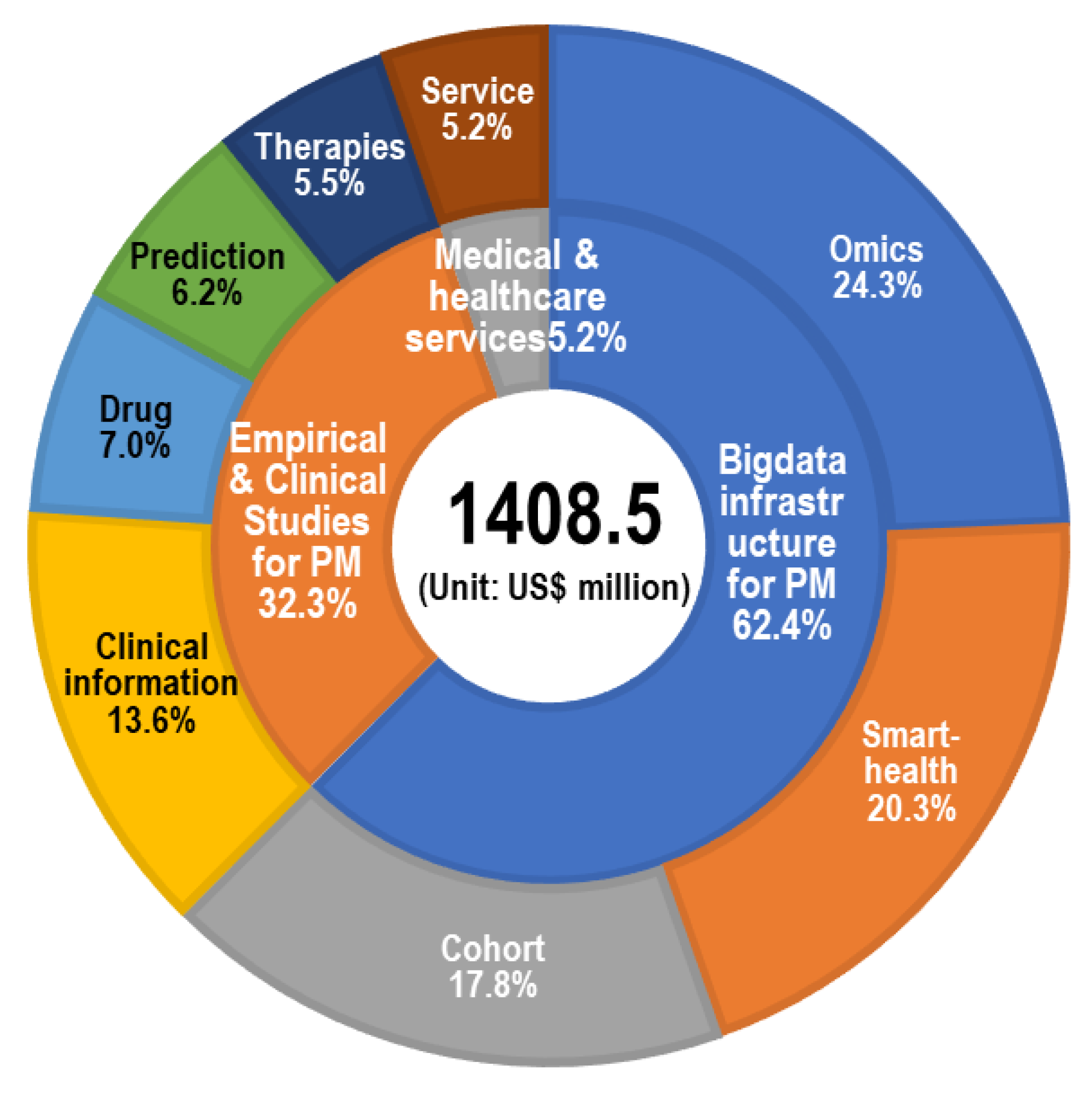
3.2.2. Status and Trend of Public R&D Projects by Technology Clusters
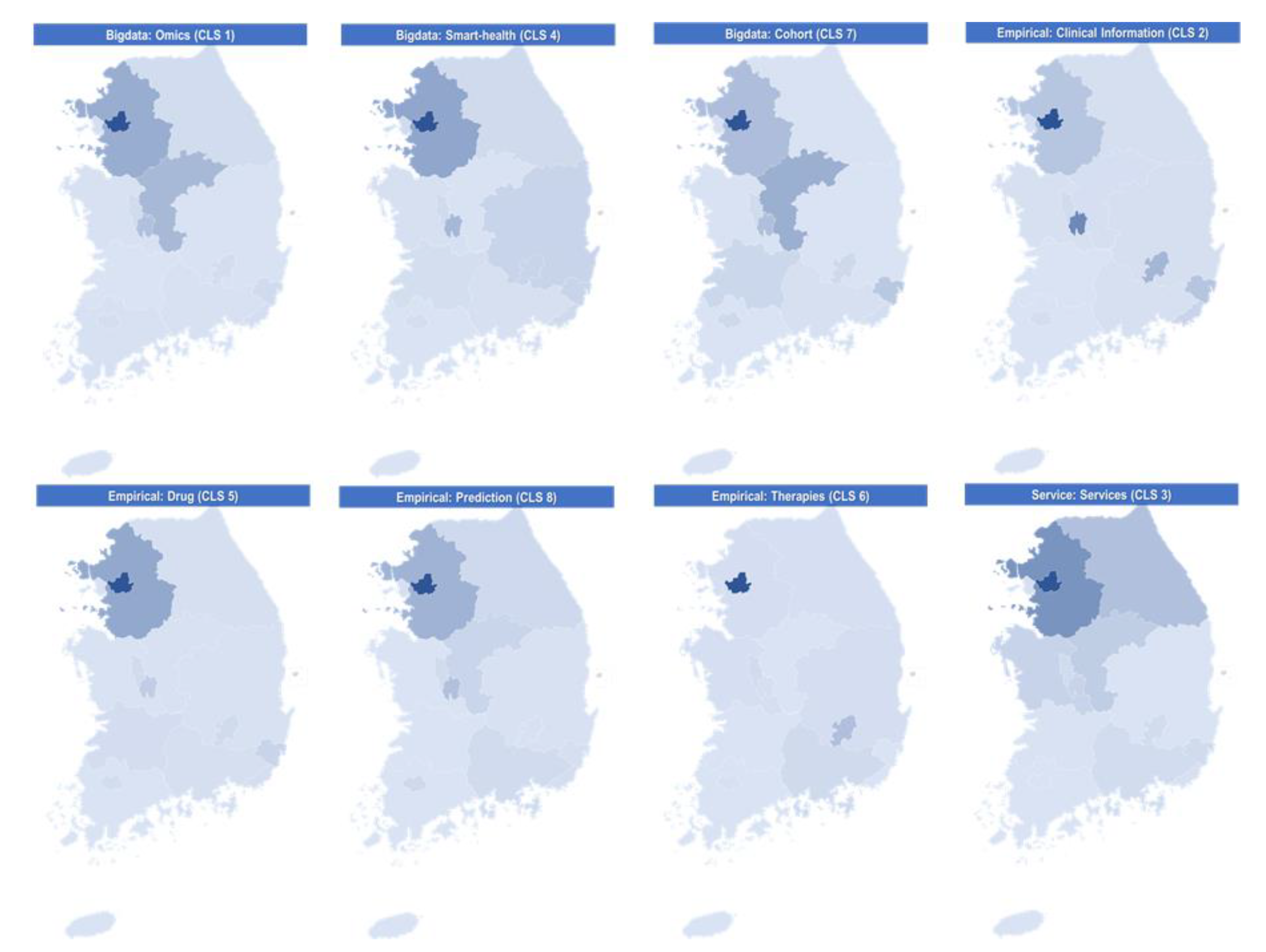
3.2.3. Status of Public R&D Projects According to Technology Clusters and Regions
3.2.4. Status of Public R&D Projects According to Technology Clusters, Regions, and Organization Types
3.2.5. Potential National Collaborative Partners in R&D Related to Three Targeted Diseases
4. Discussion
Discussion for Collaborative Overarching R&D Strategy on PM
5. Conclusions
Limitations and Further Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lippi, G.; Bassi, A.; Bovo, C. The future of laboratory medicine in the era of precision medicine. J. Lab. Precis. Med. 2016, 1, 1–5. [Google Scholar] [CrossRef]
- Joint Committee of the Nordic Medical Research Councils. Personalised Medicine in the Nordic Countries; NOS-M: Oslo, Norway, 2016. [Google Scholar]
- Ho, D.; Quake, S.R.; Mccabe, E.R.B.; Chng, W.J.; Chow, E.K.; Ding, X.; Gelb, B.D.; Ginsburg, G.S.; Hassenstab, J.; Ho, C. Enabling technologies for personalized and precision medicine. Trends Biotechnol. 2020, 38, 497–518. [Google Scholar] [CrossRef] [PubMed]
- Love-Koh, J.; Peel, A.; Rejon-Parrilla, J.C.; Ennis, K.; Lovett, R.; Manca, A.; Chalkidou, A.; Wood, H.; Taylor, M. The future of precision medicine: Potential impacts for health technology assessment. Pharmacoeconomics 2018, 36, 1439–1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, H.; Jung, E.Y. The impact of policy on the growth of precision medicine. Health Policy Technol. 2018, 7, 347–357. [Google Scholar] [CrossRef]
- Nimmesgern, E.; Norstedt, I.; Draghia-Akli, R. Enabling personalized medicine in Europe by the European Commission’s funding activities. Per. Med. 2017, 14, 355–365. [Google Scholar] [CrossRef] [Green Version]
- Ten Have, H.; Gordijn, B. Precision in health care. Med. Health Care Philos. 2018, 21, 441–442. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Health. Estimates of Funding for Various Research, Condition, and Disease Categories (RCDC); National Institute of Health: Bethesda, MD, USA, 2021.
- Cyranoski, D. China embraces precision medicine on a massive scale. Nature 2016, 529, 9–10. [Google Scholar] [CrossRef] [Green Version]
- Shigeoka, H. Personalized and Precision Medicine in Japan; Asia Health Policy Program: Stanford, CA, USA, 2017. [Google Scholar]
- MOTIE. Nine National Strategic Projects of South Korea; MOTIE: Sejong-si, Korea, 2016.
- Iriart, J.A.B. Precision medicine/personalized medicine: A critical analysis of movements in the transformation of biomedicine in the early 21st century. Cad. Saúde Publica 2019, 35, 1–13. [Google Scholar] [CrossRef]
- Chong, H.Y.; Allotey, P.A.; Chaiyakunapruk, N. Current landscape of personalized medicine adoption and implementation in Southeast Asia. BMC Med. Genom. 2018, 11, 1–15. [Google Scholar] [CrossRef]
- DeMerle, K.; Angus, D.C.; Seymour, C.W. Precision medicine for COVID-19. JAMA 2021, 325, 2041. [Google Scholar] [CrossRef]
- Kadakia, K.; Patel, B.; Shah, A. Advancing digital health: FDA innovation during COVID-19. NPJ Digit. Med. 2020, 3, 161. [Google Scholar] [CrossRef] [PubMed]
- Palanica, A.; Docktor, M.J.; Lieberman, M.; Fossat, Y. The need for artificial intelligence in digital therapeutics. Digit. Biomark. 2020, 4, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Horgan, D. From here to 2025: Personalised medicine and healthcare for an immediate future. J. Cancer Policy 2018, 16, 6–21. [Google Scholar] [CrossRef]
- Yiu, C.; Macon-Cooney, B.; Fingerhut, H. A research and policy agenda for the post-pandemic world. Futur. Health J. 2021, 8, e198–e203. [Google Scholar] [CrossRef] [PubMed]
- Vicente, A.M.; Ballensiefen, W.; Jönsson, J.I. How personalised medicine will transform healthcare by 2030: The ICPerMed vision. J. Transl. Med. 2020, 18, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Shotelersuk, V.; Tongsima, S.; Pithukpakorn, M.; Eu-ahsunthornwattana, J.; Mahasirimongkol, S. Precision medicine in Thailand. Am. J. Med. Genet. Part C Semin. Med. Genet. 2019, 181, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Nardini, C.; Osmani, V.; Cormio, P.G.; Frosini, A.; Turrini, M.; Lionis, C.; Neumuth, T.; Ballensiefen, W.; Borgonovi, E.; D’Errico, G. The evolution of personalized healthcare and the pivotal role of European regions in its implementation. Per. Med. 2021, 18, 283–294. [Google Scholar] [CrossRef]
- Njølstad, P.R.; Andreassen, O.A.; Brunak, S.; Børglum, A.D.; Dillner, J.; Esko, T.; Franks, P.W.; Freimer, N.; Groop, L.; Heimer, H.; et al. Roadmap for a precision-medicine initiative in the Nordic region. Nat. Genet. 2019, 51, 924–930. [Google Scholar] [CrossRef]
- Cash, D.; Clark, W.C.; Alcock, F.; Dickson, N.M.; Eckley, N.; Jäger, J. Salience, Credibility, Legitimacy and Boundaries: Linking Research, Assessment and Decision Making. Assessment and Decision Making; SSRN: Rochester, NY, USA, 2002. [Google Scholar]
- Parkhurst, J. The Politics of Evidence: From Evidence-Based Policy to the Good Governance of Evidence; Taylor & Francis: Abingdon, UK, 2017. [Google Scholar]
- Houser, K.A. Can AI solve the diversity problem in the tech industry: Mitigating noise and bias in employment decision-making. Stan. Tech. L Rev. 2019, 22, 290. [Google Scholar]
- Dror, I.E. Cognitive and human factors in expert decision making: Six fallacies and the eight sources of bias. Anal. Chem. 2020, 92, 7998–8004. [Google Scholar] [CrossRef]
- Lee, D.; Kim, K. A Collaborative trans-regional R&D strategy for the South Korea Green New Deal to achieve future mobility. Sustainability 2021, 13, 8637. [Google Scholar] [CrossRef]
- Lee, D.; Kim, K. Research and development investment and collaboration framework for the hydrogen economy in South Korea. Sustainability 2021, 13, 10686. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. Bio-Health Industry to Achieve People-Centered Innovative Growth. Available online: http://www.mohw.go.kr/eng/nw/nw0101vw.jsp?PAR_MENU_ID=1007&MENU_ID=100701&page=1&CONT_SEQ=349515 (accessed on 30 November 2021).
- OECD. OECD Economic Surveys: Korea 2020; OECD: Paris, France, 2020. [Google Scholar]
- OECD. OECD Reviews of Public Health: Korea: A Healthier Tomorrow; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Redekop, W.K.; Mladsi, D. The faces of personalized medicine: A framework for understanding its meaning and scope. Value Health 2013, 16 (Suppl. S6), S4–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raza, S.; Blackburn, L.; Moorthie, S.; Cook, S.; Johnson, E.; Gaynor, L.; Kroese, M. The Personalised Medicine Technology Landscape; PHG Foundation: Cambridge, UK, 2018. [Google Scholar]
- University of California San Francisco. The Elements of Precision Medicine. Available online: https://precisionmedicine.ucsf.edu/elements-precision-medicine (accessed on 10 November 2021).
- Roumbanis, L. Peer review or lottery? A critical analysis of two different forms of decision-making mechanisms for allocation of research grants. Sci. Technol. Hum. Values 2019, 44, 994–1019. [Google Scholar] [CrossRef]
- Meadmore, K.; Fackrell, K.; Recio-Saucedo, A.; Bull, A.; Fraser, S.D.S.; Blatch-Jones, A. Decision-making approaches used by UK and international health funding organisations for allocating research funds: A survey of current practice. PLoS ONE 2020, 15, e0239757. [Google Scholar] [CrossRef]
- Beresford, B.; Sloper, P. Understanding the Dynamics of Decision-making and Choice: A Scoping Study of Key Psychological Theories to Inform the Design and Analysis of the Panel Study; Social Policy Research Unit, University of York: York, UK, 2008. [Google Scholar]
- Simon, H.A. Administrative Behavior: A Study of Decision-making Processes in Administrative Organization. In The Oxford Handbook of Classics in Public Policy and Administration; Monash University: Melbourne, Australia, 1947. [Google Scholar]
- Turoff, M.; Linstone, H.A. The Delphi Method—Techniques and Applications; Addison-Wesley: Boston, MA, USA, 2002. [Google Scholar]
- Langfeldt, L. Expert panels evaluating research: Decision-making and sources of bias. Res. Eval. 2004, 13, 51–62. [Google Scholar] [CrossRef]
- Manual, F. Guidelines for Collecting and Reporting Data on Research and Experimental Development. Available online: http://www.oecd.org/sti/frascati-manual-2015-9789264239012-en.htm (accessed on 30 November 2021).
- OECD. Scientific Advice for Policy Making: The role and responsibility of expert bodies and individual scientists. In OECD Science, Technology and Industry Policy Papers, No. 21; OECD Publishing: Paris, France, 2015. [Google Scholar] [CrossRef]
- Galindo-Rueda, F.; Verger, F. OECD Taxonomy of Economic Activities Based on R&D Intensity; OECD: Paris, France, 2016. [Google Scholar]
- Aminullah, E. STI policy and R&D governance for the attainment of SDGs: Envisioning the Indonesia’s future. Asian J. Technol. Innovat. 2020, 28, 204–233. [Google Scholar]
- Mazzucato, M. Mission-oriented innovation policies: Challenges and opportunities. Ind. Corp. Change 2018, 27, 803–815. [Google Scholar] [CrossRef] [Green Version]
- Begg, I. Innovative directions for EU Cohesion Policy after 2020. In CESifo Forum; IFO Institut-Leibniz-Institut für Wirtschaftsforschung an der Universität München: München, Germany, 2018; Volume 19, pp. 3–9. [Google Scholar]
- Whitsel, L.P.; Wilbanks, J.; Huffman, M.D.; Hall, J.L. The role of government in precision medicine, precision public health and the intersection with healthy living. Prog. Cardiovasc. Dis. 2019, 62, 50–54. [Google Scholar] [CrossRef]
- Denicolai, S.; Previtali, P. Precision medicine: Implications for value chains and business models in life sciences. Technol. Forecast Soc. Change 2020, 151, 119767. [Google Scholar] [CrossRef]
- Chanfreau-Coffinier, C.; Peredo, J.; Russell, M.M.; Yano, E.M.; Hamilton, A.B.; Lerner, B.; Provenzale, D.; Knight, S.J.; Voils, C.I.; Scheuner, M.T. A logic model for precision medicine implementation informed by stakeholder views and implementation science. Genet. Med. 2019, 21, 1139–1154. [Google Scholar] [CrossRef] [PubMed]
- Maughan, T. The promise and the hype of ‘personalised medicine’. New Bioeth. 2017, 23, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.; Heo, Y.; Kim, K. A strategy for international cooperation in the COVID-19 pandemic era: Focusing on national scientific funding data. Healthcare 2020, 8, 204. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Kim, S.; Kim, K. International R&D collaboration for a global aging society: Focusing on aging-related national-funded projects. Int. J. Environ. Res. Public Health 2020, 17, 8545. [Google Scholar] [CrossRef]
- Shah, S.H.H.; Lei, S.; Ali, M.; Doronin, D.; Hussain, S.T. Prosumption: Bibliometric Analysis using HistCite and VOSviewer. Kybernetes 2019, 49, 1020–1045. [Google Scholar] [CrossRef]
- Waltman, L.; Van Eck, N.J.; Noyons, E.C.M. A unified approach to mapping and clustering of bibliometric networks. J. Informetr. 2010, 4, 629–635. [Google Scholar] [CrossRef] [Green Version]
- DOE. Hydrogen Program Plan; DOE: Washington, DC, USA, 2020. [Google Scholar]
- Chien, C. A Portfolio-evaluation framework for selecting R&D projects. R&D Manag. 2002, 32, 359–368. [Google Scholar] [CrossRef]
- Crawford, L.; Hobbs, B.; Turner, J.R. Aligning capability with strategy: Categorizing projects to do the right projects and to do them right. Proj. Manag. J. 2006, 37, 38–50. [Google Scholar] [CrossRef]
- Min, S.; Kim, J.; Sawng, Y.W. The effect of innovation network size and public R&D investment on regional innovation efficiency. Technol. Forecast. Soc. Change 2020, 155, 119998. [Google Scholar] [CrossRef]
- WHO. A Framework for National Health Policies, Strategies and Plans; WHO: Geneva, Switzerland, 2010. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Regions | Unique Identification Number (ID) | Organization | Type of Organization | Research Program | Funding (USD Thousand) | Project Period | Project Contents | ||
|---|---|---|---|---|---|---|---|---|---|
| Start Date | End Date | Title | Abstract | ||||||
| Ulsan | 1711117189 | Ulsan University | University | Omics-based precision medical technology development project | 51 | 9-1-2019 | 12-31-2024 | Development of algorithm and integrative platform for precision medicine | Through the treatment of current biologics available in severe asthma patients using such a treatment response and omics data a new phenotype and cluster through a disturbing effect and select such as to minimize the problem, statistical models developed: PRISM 1 Research. PRISM adaptive design can be applied based on the first results (adaptive design), developing and proposing guidelines for biological agents through clinical tests in the selection of patients with severe asthma: study PRISM 2. |
| Seoul | 1465030239 | Samsung Medical Center | Hospital | CDM-based precision medical data integration platform | 149 | 4-17-2019 | 12-31-2021 | Development of Establishment, Verification and Deployment platform of CDM-based intelligent Clinical Decision Support System for Emergency and Critical Patients | First Year (1) Development Goals: General: Consumer emergency center, intensive care CDM extended model development and standardization (based on research) 1 Details: First, Chinese characters CDM extended model standardization and deployment (2) research content and scope (using the system configuration figure, representing the structure, etc.). General (detail 1) research and development information, demand survey carried out in emergency, artificial intelligence algorithms intended for physicians and researchers in the intensive care unit; explore the variables required to build a CDM-based intelligent precision medical identification algorithm. |
| Daejeon | 1711119491 | Korea Research Institute of Bioscience and Biotechnology | Research institute | Bio Bigdata | 8211 | 5-29-2020 | 12-31-2021 | Construction of infrastructure for genome big data | (1) Rare, one of the leading business resources and data secure. Holds data of government business resources (leading to business) and a data connection to secure dielectric data (10,000) The dielectric holds leading business (5000) and clinical information (5000) selected by linking genomic data. Rare diseases dielectric secure data (10,000). (2) Creating a dielectric sequencing and analysis report. Leading business and genomic data production of new rare disease samples (15,000). |
| Search Terms | Time Period | Amount of Raw Data | Final Number of Data Utilized |
|---|---|---|---|
| ((precision OR personalized OR personalised OR individualised OR individualized OR customized OR customized OR tailored OR targeted OR predictive OR preventive) AND (medicine OR therapy OR health OR treat OR cohort)) OR “3P medicine” OR “4P medicine” OR (omics AND (research OR technology)) | 2015–2020 | 8478 | 5647 |
| Region | Funding (USD Thousand) | No. of Projects | Funding Per Project | Funding (%) |
|---|---|---|---|---|
| Gangwon-do | 32,145 | 138 | 233 | 2.3% |
| Gyeonggi-do | 210,138 | 1073 | 196 | 14.9% |
| Gyeongsangnam-do | 17,285 | 95 | 182 | 1.2% |
| Gyeongsangbuk-do | 19,722 | 91 | 217 | 1.4% |
| Gwangju | 22,779 | 131 | 174 | 1.6% |
| Daegu | 67,088 | 163 | 412 | 4.8% |
| Daejeon | 168,691 | 440 | 383 | 12.0% |
| Busan | 22,888 | 125 | 183 | 1.6% |
| Seoul | 634,143 | 2669 | 238 | 45.0% |
| Sejong | 1208 | 8 | 151 | 0.1% |
| Ulsan | 66,388 | 282 | 235 | 4.7% |
| Incheon | 16,825 | 82 | 205 | 1.2% |
| Jeollanam-do | 2257 | 10 | 226 | 0.2% |
| Jeollabuk-do | 16,153 | 64 | 252 | 1.1% |
| Jeju | 1199 | 9 | 133 | 0.1% |
| Chungcheongnam-do | 11,908 | 77 | 155 | 0.8% |
| Chungcheongbuk-do | 97,688 | 190 | 514 | 6.9% |
| Total/Average | 1,408,505 | 5647 | 249 | 100.0% |
| Value Chain Sector | Technology Cluster | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | Total | 2015–2020 CAGR |
|---|---|---|---|---|---|---|---|---|---|
| Bigdata | Omics (CLS 1) | 38.1 | 43.9 | 54.9 | 58.3 | 67.8 | 79.6 | 342.7 | 15.9% |
| Smart-health (CLS 4) | 21.4 | 28.6 | 51.0 | 71.3 | 57.6 | 55.9 | 285.7 | 21.2% | |
| Cohort (CLS 7) | 14.0 | 21.5 | 29.3 | 53.1 | 68.5 | 64.6 | 251.0 | 35.8% | |
| 73.5 | 94.0 | 135.2 | 182.7 | 193.9 | 200.1 | 879.4 | 22.2% | ||
| Empirical | Clinical Information (CLS 2) | 10.2 | 17.5 | 34.2 | 51.0 | 43.7 | 35.5 | 192.2 | 28.3% |
| Drug (CLS 5) | 8.4 | 14.6 | 20.5 | 21.0 | 19.8 | 14.1 | 98.4 | 11.1% | |
| Prediction (CLS 8) | 6.3 | 11.1 | 13.3 | 19.1 | 17.1 | 20.1 | 87.0 | 26.2% | |
| Therapies (CLS 6) | 11.8 | 15.1 | 14.2 | 15.9 | 11.4 | 9.6 | 78.0 | −4.1% | |
| 36.7 | 58.2 | 82.2 | 107.0 | 92.0 | 79.4 | 455.5 | 16.7% | ||
| Service | Services (CLS 3) | 4.6 | 8.2 | 11.9 | 16.5 | 16.4 | 15.9 | 73.6 | 28.2% |
| Total Sum (Unit: USD million) | 114.8 | 160.4 | 229.3 | 306.2 | 302.3 | 295.5 | 1408.5 | 20.8% | |
| (Unit: USD Million) | Bigdata | Empirical | Service | TOTAL | |||||
|---|---|---|---|---|---|---|---|---|---|
| Omics (CLS 1) | Smart-Health (CLS 4) | Cohort (CLS 7) | Clinical Information (CLS 2) | Drug (CLS 5) | Prediction (CLS 8) | Therapies (CLS 6) | Service (CLS 3) | ||
| Gangwon-do | 7.7 | 7.9 | 0.9 | 2.2 | 1.5 | 3.1 | 1.4 | 7.5 | 32.1 |
| Gyeonggi-do | 60.3 | 52.4 | 27.7 | 14.7 | 20.9 | 15.1 | 1.7 | 17.3 | 210.1 |
| Gyeongsangnam-do | 2.1 | 2.3 | 2.4 | 1.7 | 1.6 | 2.5 | 3.2 | 1.6 | 17.3 |
| Gyeongsangbuk-do | 1.5 | 12.6 | 0.2 | 2.3 | 0.7 | 0.5 | 1.9 | 0.1 | 19.7 |
| Gwangju | 5.0 | 2.2 | 7.7 | 1.9 | 2.2 | 3.1 | 0.6 | - | 22.8 |
| Daegu | 6.3 | 12.9 | 7.5 | 22.5 | 2.7 | 0.6 | 13.0 | 1.6 | 67.1 |
| Daejeon | 36.5 | 37.1 | 25.7 | 45.8 | 7.8 | 10.7 | 1.5 | 3.6 | 168.7 |
| Busan | 3.9 | 7.6 | 2.3 | 7.4 | 0.5 | 0.5 | 0.2 | 0.6 | 22.9 |
| Seoul | 158.1 | 122.4 | 104.3 | 72.5 | 50.4 | 44.3 | 51.3 | 30.9 | 634.1 |
| Sejong | - | - | 0.3 | - | 0.4 | 0.5 | - | - | 1.2 |
| Ulsan | 9.1 | 13.1 | 20.2 | 15.6 | 5.2 | 1.3 | 0.0 | 1.8 | 66.4 |
| Incheon | 1.0 | 7.2 | 4.0 | 1.9 | 0.7 | 0.3 | 1.6 | 0.1 | 16.8 |
| Jeollanam-do | 2.1 | 0.0 | 0.0 | - | - | - | 0.1 | - | 2.3 |
| Jeollabuk-do | 0.1 | 4.7 | 9.0 | 0.1 | 2.0 | - | - | 0.3 | 16.2 |
| Jeju | 0.3 | - | - | 0.2 | 0.7 | - | - | - | 1.2 |
| Chungcheongnam-do | 2.3 | 2.4 | 0.7 | 1.4 | 0.3 | 0.1 | 1.3 | 3.4 | 11.9 |
| Chungcheongbuk-do | 46.4 | 0.9 | 38.2 | 2.0 | 0.8 | 4.4 | 0.2 | 4.9 | 97.7 |
| Total | 342.7 | 285.7 | 251.0 | 192.2 | 98.4 | 87.0 | 78.0 | 73.6 | 1408.5 |
| (Unit: USD Thousand) | Organization | Gangwon-do | Gyeonggi-do | Gyeongsangnam-do | Gyeongsangbuk-do | Gwangju | Daegu | Daejeon | Busan | Seoul | Sejong | Ulsan | Incheon | Jeollanam-do | Jeollabuk-do | Jeju | Chungcheongnam-do | Chungcheongbuk-do |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Omics (CLS 1) | Industry | - | 7299 | - | - | - | 125 | 2435 | 1375 | 23,593 | - | 250 | 528 | - | 56 | - | - | - |
| University | 7676 | 14,779 | 1974 | 1518 | 4178 | 3440 | 10,197 | 2490 | 92,853 | - | 8874 | 225 | 1871 | - | 250 | 2269 | 771 | |
| Hospital | - | 498 | 167 | - | 807 | - | - | - | 18,566 | - | - | 289 | 214 | - | - | - | - | |
| Institute | - | 37,323 | - | - | - | 2758 | 23,879 | - | 22,943 | - | - | - | - | - | - | - | 15,655 | |
| Agency | - | 393 | - | - | - | - | - | - | 144 | - | - | - | - | - | - | - | 29,990 | |
| Smart-health (CLS 4) | Industry | 6047 | 30,032 | 1131 | 2915 | 825 | 5475 | 4125 | 3262 | 37,877 | - | 1164 | 1301 | - | 836 | - | 442 | 283 |
| University | 1900 | 12,835 | - | 2292 | 613 | 6961 | 6360 | 1475 | 40,137 | - | 11,965 | 308 | 42 | 3799 | - | 1191 | 25 | |
| Hospital | - | 3859 | 1181 | - | - | - | 21 | - | 9467 | - | - | 5499 | - | 58 | - | 83 | - | |
| Institute | - | 5654 | - | 7148 | 765 | 58 | 26,598 | - | 29,638 | - | - | 83 | - | - | - | 656 | - | |
| Agency | - | 54 | - | 231 | - | 404 | - | 2863 | 5244 | - | - | - | - | - | - | - | 559 | |
| Cohort (CLS 7) | Industry | 108 | 2146 | 1000 | 148 | - | - | 3201 | 1083 | 28,390 | - | - | - | - | 4 | - | - | 1717 |
| University | 747 | 12,578 | 242 | 65 | 6723 | 3555 | 2052 | 920 | 55,083 | 250 | 20,186 | 1660 | - | 7588 | - | 723 | 1792 | |
| Hospital | - | 4994 | 1136 | - | 941 | 1422 | 67 | 334 | 16,301 | 42 | - | 2332 | 27 | 1386 | - | - | 417 | |
| Institute | - | 7012 | - | - | - | 1203 | 20,417 | - | 2833 | - | - | - | - | - | - | - | - | |
| Agency | - | 929 | - | - | - | 1271 | - | - | 1686 | - | - | - | - | - | - | - | 34,318 | |
| Clinical Information (CLS 2) | Industry | 375 | 2563 | - | 148 | - | - | 1104 | 7275 | 12,925 | - | - | - | - | 141 | - | - | - |
| University | 1439 | 4861 | 1435 | 2105 | 1535 | 8724 | 12,762 | 124 | 43,613 | - | 15,632 | 1554 | - | - | 245 | 1431 | 192 | |
| Hospital | 376 | 1388 | 252 | - | 388 | 696 | - | - | 10,117 | - | - | 343 | - | - | - | - | - | |
| Institute | - | 5908 | - | - | - | 11,485 | 18,473 | - | 5022 | - | - | - | - | - | - | - | - | |
| Agency | - | - | - | - | - | 1567 | 13,447 | - | 777 | - | - | - | - | - | - | - | 1770 | |
| Drug (CLS 5) | Industry | 1499 | 6599 | - | 650 | - | 417 | - | 100 | 2767 | 417 | - | 73 | - | - | 704 | - | 125 |
| University | - | 2785 | - | - | 613 | 2300 | 297 | 360 | 17,710 | - | 5233 | 592 | - | 2014 | - | 292 | - | |
| Hospital | - | 167 | - | - | 1619 | - | 1200 | - | 12,538 | - | - | - | - | - | - | - | - | |
| Institute | - | 4704 | - | - | - | - | 6276 | - | 6532 | - | - | - | - | - | - | - | - | |
| Agency | - | 6685 | 1568 | - | - | - | - | - | 10,859 | - | - | - | - | - | - | - | 662 | |
| Prediction (CLS 8) | Industry | 2408 | 10,452 | - | 441 | 446 | - | 1904 | 228 | 14,521 | 417 | - | 292 | - | - | - | 117 | - |
| University | 667 | 4287 | 2190 | 33 | 2071 | 217 | 4002 | 273 | 15,361 | 83 | 1310 | - | - | - | - | - | 3600 | |
| Hospital | - | - | 104 | - | 578 | - | 21 | - | 10,129 | - | - | - | - | - | - | - | - | |
| Institute | - | 358 | - | - | - | 417 | 4763 | - | 4300 | - | - | - | - | - | - | - | - | |
| Agency | - | - | 167 | 21 | 42 | - | - | - | - | - | - | - | - | - | - | - | 783 | |
| Therapies (CLS 6) | Industry | - | 96 | - | - | - | 167 | 1000 | - | 14,622 | - | - | - | - | - | - | 56 | 54 |
| University | 1367 | 1189 | 3167 | 1931 | 284 | 12,848 | 483 | 167 | 23,437 | - | 12 | - | - | - | - | 675 | - | |
| Hospital | - | 204 | - | - | 353 | - | - | - | 1642 | - | - | 1614 | 103 | - | - | - | 117 | |
| Institute | - | 248 | - | - | - | - | - | - | 11,617 | - | - | - | - | - | - | 533 | - | |
| Agency | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | |
| (Service (CLS 3) | Industry | 7360 | 9054 | - | - | - | - | 390 | - | 6851 | - | - | - | - | - | - | 392 | 1906 |
| University | 160 | 1257 | 1573 | 75 | - | 1025 | 104 | 558 | 10,634 | - | 1762 | 117 | - | 270 | - | 3049 | 433 | |
| Hospital | - | 206 | - | - | - | - | - | - | 933 | - | - | 17 | - | - | - | - | 81 | |
| Institute | - | 5365 | - | - | - | - | 3115 | - | 7523 | - | - | - | - | - | - | - | - | |
| Agency | 17 | 1379 | - | - | - | 555 | - | - | 4958 | - | - | - | - | - | - | - | 2437 | |
| TOTAL | Industry | 17,797 | 68,242 | 2131 | 4302 | 1271 | 6183 | 14,158 | 13,322 | 141,547 | 833 | 1414 | 2193 | - | 1037 | 704 | 1006 | 4085 |
| University | 13,955 | 54,571 | 10,579 | 8020 | 16,017 | 39,069 | 36,257 | 6368 | 298,828 | 333 | 64,974 | 4455 | 1913 | 13,671 | 495 | 9629 | 6813 | |
| Hospital | 376 | 11,315 | 2840 | - | 4685 | 2117 | 1308 | 334 | 79,691 | 42 | - | 10,093 | 344 | 1445 | - | 83 | 615 | |
| Institute | - | 66,571 | - | 7148 | 765 | 15,921 | 103,521 | - | 90,408 | - | - | 83 | - | - | - | 1190 | 15,655 | |
| Agency | 17 | 9440 | 1735 | 252 | 42 | 3797 | 13,447 | 2863 | 23,669 | - | - | - | - | - | - | - | 70,519 |
| Target Disease | Type of Organization | Organization | R&D Title | Project Manager | Region | Funding (USD Thousand) |
|---|---|---|---|---|---|---|
| Cancer | Institute | National Cancer Center | Prognostic impact of CT-determined sarcopenia and sarcopenic obesity in older patients with non-small cell lung cancer undergoing chemotherapy | Yoon-jung Jang | Gyeonggi-do | 596 |
| University | Yonsei University | Development of an app-based self-management program “HARU” for cancer patients and testing its effectiveness | Kyungmi Jung | Seoul | 11 | |
| University | Seoul National University | Evaluation of risk for oral diseases in cancer patients in Korea and the National Health Insurance coverage extension | Seo-kyung Han | Seoul | 75 | |
| University | Yonsei University | Development of prospective cohort and evidence-based management program for colorectal cancer survivors | Seon-ha Ji | Seoul | 55 | |
| Institute | Broad Institute Inc. | Making cancer precision medicine real bottlenecks and opportunities | Todd R. Golub | Cambridge, MA, USA | 1024 | |
| University | Royal College of Surgeons in Ireland | Advancing a precision medicine paradigm in metastatic colorectal cancer systems-based patient stratification solutions | Annette Byrne PhD | Dublin, Ireland | 6794 | |
| University | Queen Mary University of London | Optimal screening and surveillance regimes for early diagnosis of cancer and precision medicine using mathematical modelling | Kit Curtius | London, UK | 370 | |
| University | Keio University | Establishment of small cell lung cancer organoids for development of precision medicine | Mitsuishi Akifumi | Tokyo, Japan | 37 | |
| Brain disease | Hospital | Samsung Medical Center | Protocol development and validation of personalized CNS-PNS hybrid rehabilitation therapy for restoration of gait-related neural network in stroke Patients | Yeon-hee Kim | Seoul | 155 |
| Hospital | Seoul National University Hospital | Modeling of prognosis prediction for stroke using big data | Byung-Woo Yoon | Seoul | 108 | |
| Institute | Korea Institute of Science and Technology | Development of customized rehabilitation technology for stroke patients in neural plasticity evaluation and enhancement | In-chan Yoon | Seoul | 1083 | |
| University | Pusan National University | Effect of digital treatment system on upper limb functional recovery and brain plasticity in stroke patients | Yong-il Shin | Busan | 83 | |
| University | Gachon University | Development of biomarker monitoring system for verification of Korean medicine treatment towards stroke | Young-jun Kim | Gyeonggi | 183 | |
| University | Ohio State University | Laying the groundwork for personalized medicine in aphasia therapy genetic and cognitive predictors of restorative treatment response | Stacy M. Harnish | Columbus, Ohio, USA | 487 | |
| University | Charité-Universitätsmedizin Berlin | Personalised medicine by predictive modeling in stroke for better quality of life | Dietmar Frey | Berlin, Germany | 6773 | |
| University | King’s College London | Towards personalised medicine in psychiatric genetics the role of cardiometabolic traits in severe mental illness | Saskia Hagenaars | London, UK | 409 | |
| University | Hamamatsu University School of Medicine | Precision medicine in developmental psychiatry | Kenji J. Tsuchiya | Shizuoka, Japan | 159 | |
| Chronic disease | Industry | M2IT | Intelligent diagnosis prescription inquiry service using CDM-based chronic disease data | Wooseop Shin | Seoul | 417 |
| Agency | Korea Disease Control and Prevention Agency | Women’s health research for prevention and management of non-communicable diseases | Hyun-young Park | Chungcheongbuk-do | 278 | |
| Industry | Wisenut | Development of an interactive medical history taking software based on lifelog data for chronic disease patients | Wooyoung Kwon | Gyeonggi | 833 | |
| Industry | Medical Excellence | System advancement and development for chronic disease monitoring and education in primary clinics | Yoon-hee Choi | Seoul | 292 | |
| Hospital | Samsung Medical Center | Advancement and demonstration of a primary care-based chronic disease monitoring service model | Jaeheon Kang | Seoul | 208 | |
| University | Catholic University of Korea | Development of advanced system linkage service model for the optimal patient care of chronic diseases in primary clinics | Gun-ho Yoon | Seoul | 125 | |
| University | University of Washington | Central hub for kidney precision medicine | Jonathan Himmelfarb | Seattle, WA, USA | 4286 | |
| University | Academisch Ziekenhuis Groningen | Personalised medicine in diabetic chronic disease management | Hiddo J. L. Heerspink | Groningen, Netherlands | 3794 | |
| University | University College London | MICA: Medical Bioinformatics: Data-driven discovery for personalised medicine | Peter Coveney | London, UK | 11,685 | |
| University | The University of Tokyo | Development of a diagnostic algorithm through gene panel testing and genetic risk score analysis to facilitate precision medicine for diabetes | Hosoe Jun | Tokyo, Japan | 35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.; Kim, K. Public R&D Projects-Based Investment and Collaboration Framework for an Overarching South Korean National Strategy of Personalized Medicine. Int. J. Environ. Res. Public Health 2022, 19, 1291. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031291
Lee D, Kim K. Public R&D Projects-Based Investment and Collaboration Framework for an Overarching South Korean National Strategy of Personalized Medicine. International Journal of Environmental Research and Public Health. 2022; 19(3):1291. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031291
Chicago/Turabian StyleLee, Doyeon, and Keunhwan Kim. 2022. "Public R&D Projects-Based Investment and Collaboration Framework for an Overarching South Korean National Strategy of Personalized Medicine" International Journal of Environmental Research and Public Health 19, no. 3: 1291. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031291