
Assessment of Bi-Ventricular and Bi-Atrial Areas Using Four-Chamber Cine Cardiovascular Magnetic Resonance Imaging: Fully Automated Segmentation with a U-Net Convolutional Neural Network

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cine CMR Datasets
2.2. CMR Parameters
2.3. Image Pre-Processing
2.4. Image Segmentation Using Manual Delineation
2.5. Image Segmentation Using Deep Learning
2.6. Image Post-Processing
2.7. Evaluation Criteria
2.8. Image Categorization
2.9. Statistical Analyses
3. Results
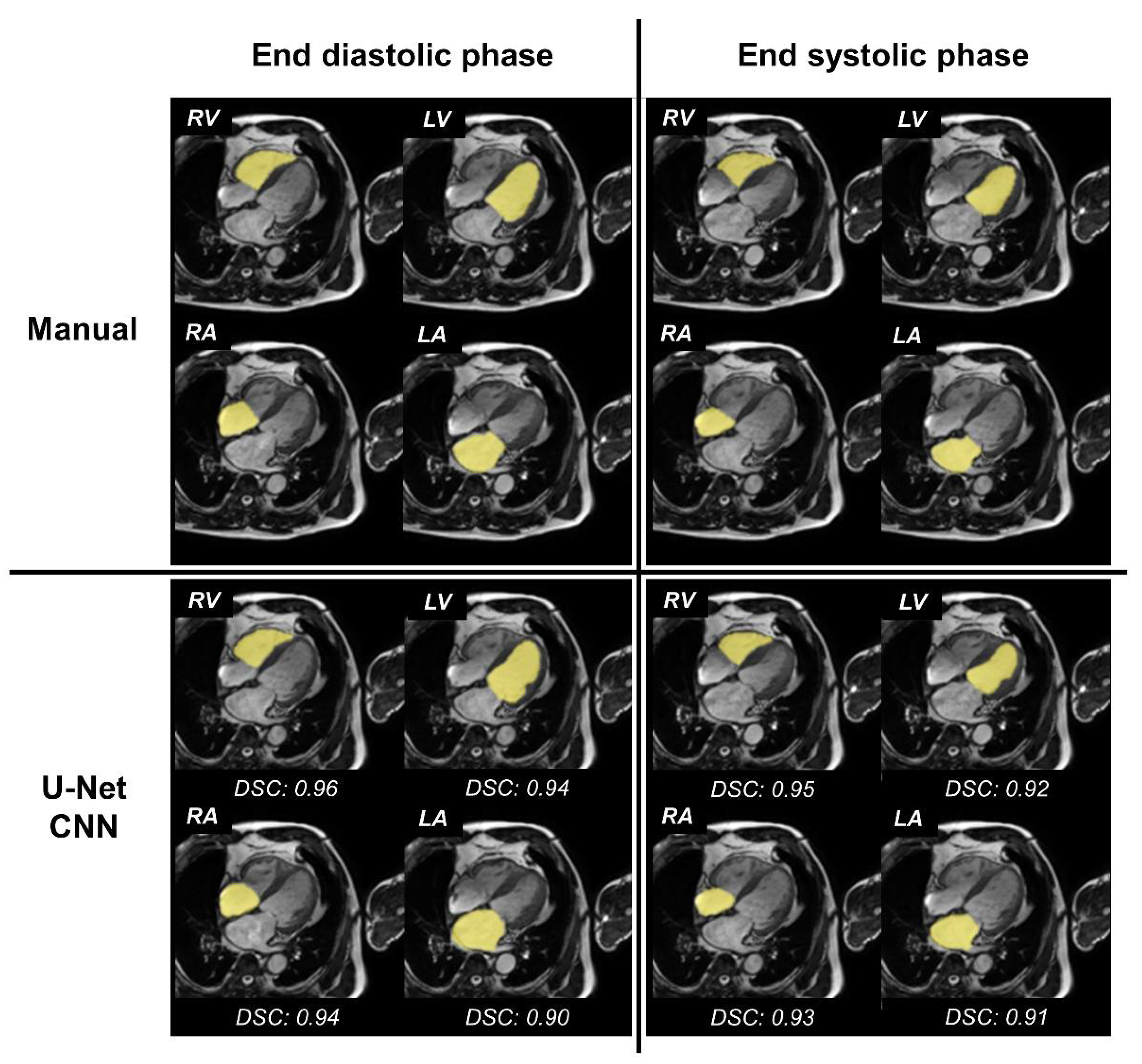
3.1. Accuracy of Segmentation of the Four Cardiac Chambers
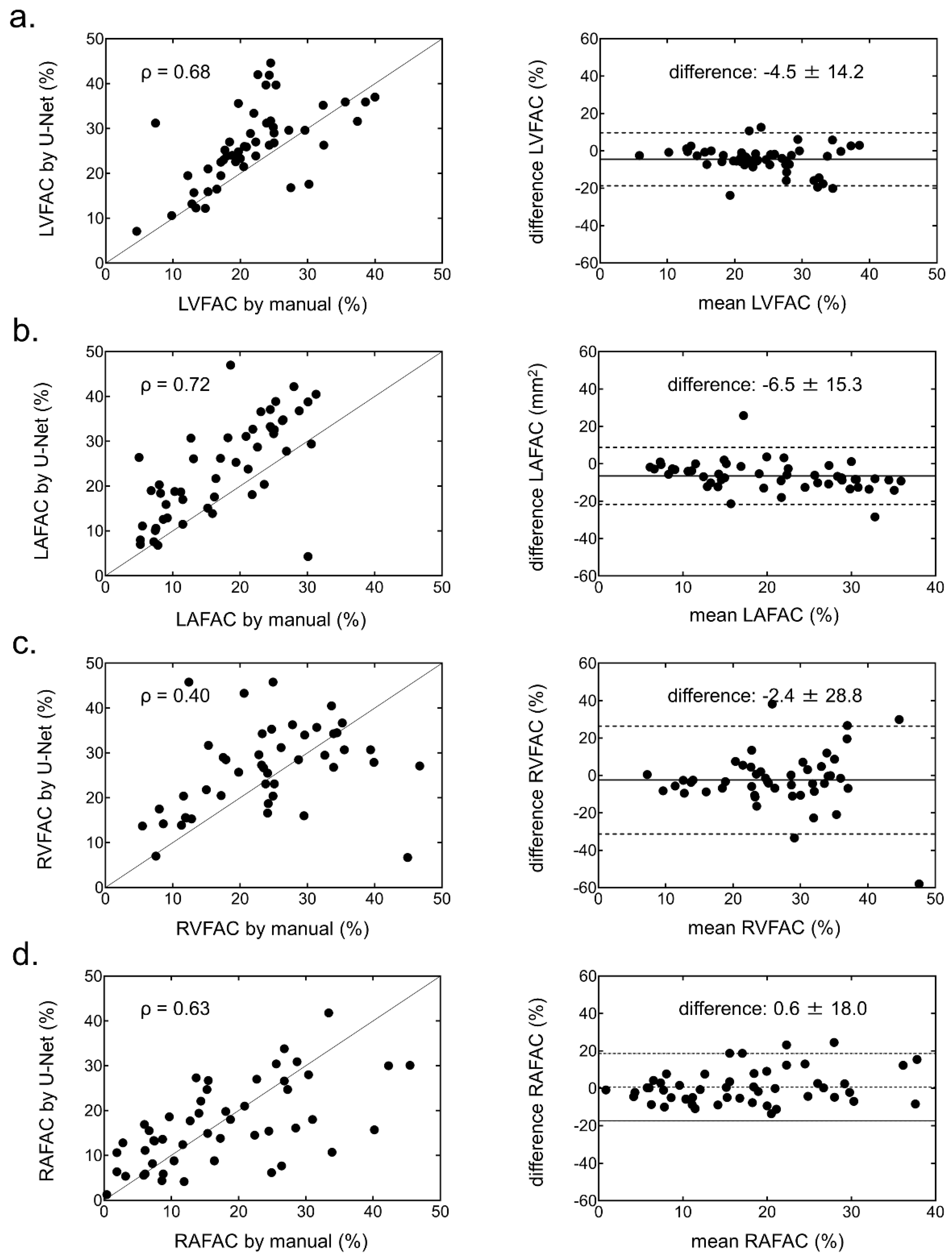
3.2. Functional Parameters of the Four Cardiac Chambers
3.3. Computation Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- White, H.D.; Norris, R.M.; Brown, M.A.; Brandt, P.W.; Whitlock, R.M.; Wild, C.J. Left Ventricular End-Systolic Volume as the Major Determinant of Survival after Recovery from Myocardial Infarction. Circulation 1987, 76, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Lopatin, M.; Stevenson, L.W.; De Marco, T.; Fonarow, G.C.; ADHERE Scientific Advisory Committee and Investigators. Clinical Presentation, Management, and In-Hospital Outcomes of Patients Admitted with Acute Decompensated Heart Failure with Preserved Systolic Function: A Report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database [Database]. J. Am. Coll. Cardiol. 2006, 47, 76–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsang, T.S.M.; Barnes, M.E.; Gersh, B.J.; Bailey, K.R.; Seward, J.B. Left Atrial Volume as a Morphophysiologic Expression of Left Ventricular Diastolic Dysfunction and Relation to Cardiovascular Risk Burden. Am. J. Cardiol. 2002, 90, 1284–1289. [Google Scholar] [CrossRef]
- Cronin, B.; O’Brien, E.O.; Gu, W.; Banks, D.; Maus, T. Intraoperative 3-Dimensional Echocardiography–Derived Right Ventricular Volumetric Analysis in Chronic Thromboembolic Pulmonary Hypertension Patients Before and After Pulmonary Thromboendarterectomy. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1498–1503. [Google Scholar] [CrossRef]
- Kido, T.; Ueno, T.; Taira, M.; Kanaya, T.; Okuda, N.; Toda, K.; Kuratani, T.; Sawa, Y. Clinical Significance of Right Atrial Volume in Patients with Repaired Tetralogy of Fallot. Interact. Cardiovasc. Thorac. Surg. 2020, 30, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Victor, M.A.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 233–271. [Google Scholar] [CrossRef] [Green Version]
- Andersson, B.; Caidahl, K.; Waagstein, F. An Echocardiographic Evaluation of Patients with Idiopathic Heart Failure. Chest 1995, 107, 680–689. [Google Scholar] [CrossRef] [Green Version]
- Lo, L.W.; Lin, Y.J.; Tsao, H.M.; Chang, S.L.; Udyavar, A.R.; Hu, Y.F.; Ueng, K.C.; Tsai, W.C.; Tuan, T.C.; Chang, C.J.; et al. The Impact of Left Atrial Size on Long-Term Outcome of Catheter Ablation of Chronic Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2009, 20, 1211–1216. [Google Scholar] [CrossRef]
- Spruijt, O.A.; Di Pasqua, M.C.; Bogaard, H.J.; van der Bruggen, C.E.; Oosterveer, F.; Marcus, J.T.; Vonk-Noordegraaf, A.; Handoko, M.L. Serial Assessment of Right Ventricular Systolic Function in Patients with Precapillary Pulmonary Hypertension using Simple Echocardiographic Parameters: A Comparison with Cardiac Magnetic Resonance Imaging. J. Cardiol. 2017, 69, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Luong, C.L.; Thompson, D.J.; Gin, K.G.; Jue, J.; Nair, P.; Lee, P.K.; Tsang, M.Y.; Barnes, M.E.; Colley, P.; Tsang, T.S. Usefulness of the Atrial Emptying Fraction to Predict Maintenance of Sinus Rhythm after Direct Current Cardioversion for Atrial Fibrillation. Am. J. Cardiol. 2016, 118, 1345–1349. [Google Scholar] [CrossRef]
- Sun, J.P.; James, K.B.; Yang, X.S.; Solankhi, N.; Shah, M.S.; Arheart, K.L.; Thomas, J.D.; Stewart, W.J. Comparison of Mortality Rates and Progression of Left Ventricular Dysfunction in Patients with Idiopathic Dilated Cardiomyopathy and Dilated versus Nondilated Right Ventricular Cavities. Am. J. Cardiol. 1997, 80, 1583–1587. [Google Scholar] [CrossRef]
- Almodares, Q.; Guron, C.W.; Thurin, A.; Fu, M.; Kontogeorgos, S.; Thunstrom, E.; Johansson, M.C. Larger Right Atrium than Left Atrium is Associated with All-Cause Mortality in Elderly Patients with Heart Failure. Echocardiography 2017, 34, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Guron, C.W.; Hartford, M.; Rosengren, A.; Thelle, D.; Wallentin, I.; Caidahl, K. Usefulness of Atrial Size Inequality as an Indicator of Abnormal Left Ventricular Filling. Am. J. Cardiol. 2005, 95, 1448–1452. [Google Scholar] [CrossRef] [PubMed]
- Kawakubo, M.; Nagao, M.; Kumazawa, S.; Yamasaki, Y.; Chishaki, A.S.; Nakamura, Y.; Honda, H.; Morishita, J. Evaluation of Ventricular Dysfunction using Semi-Automatic Longitudinal Strain Analysis of Four-Chamber Cine MR Imaging. Int. J. Cardiovasc. Imaging 2016, 32, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, Y.; Abe, K.; Kamitani, T.; Hosokawa, K.; Kawakubo, M.; Sagiyama, K.; Hida, T.; Matsuura, Y.; Murayama, Y.; Funatsu, R.; et al. Balloon Pulmonary Angioplasty Improves Right Atrial Reservoir and Conduit Functions in Chronic Thromboembolic Pulmonary Hypertension. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Tao, Q.; Yan, W.; Wang, Y.; Shamonin, D.P.; Garg, P.; Plein, S.; Huang, L.; Xia, L.; Sramko, M.; Tintera, J.; et al. Deep Learning-Based Method for Fully Automatic Quantification of Left Ventricle Function from Cine MR Images: A Multivendor, Multicenter Study. Radiology 2019, 290, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Tran, C.T.; Halicek, M.; Dormer, J.D.; Tandon, A.; Hussain, T.; Fei, B. Fully Automated Segmentation of the Right Ventricle in Patients with Repaired Tetralogy of Fallot using U-Net. Proc. SPIE Int. Soc. Opt. Eng. 2020, 11317, 113171M. [Google Scholar]
- Lucas, B.D.; Kanade, T. Iterative Image Registration Technique with an Application to Stereo Vision. IJCAI 1981, 2, 674–679. [Google Scholar]
- Sony Neural Network Console. Available online: https://dl.sony.com/ (accessed on 4 December 2020).
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5 October 2015; pp. 234–241. [Google Scholar]
- Bradley, D.; Roth, G. Adaptive thresholding using the integral image. J. Graph. Tool 2007, 12, 13–21. [Google Scholar] [CrossRef]
- Dice, L.R. Measures of the Amount of Ecologic Association between Species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Mahalanobis, P.C. On the Generalized Distance in Statistics. Proc. Indian Natl. Sci. Acad. 1936, 2, 49–55. [Google Scholar]
- Kou, S.; Caballero, L.; Dulgheru, R.; De Sousa, C.; Kacharava, G.; Athanassopoulos, G.D.; Barone, D.; Baroni, M.; Cardim, N.; Gomez De Diego, J.J.; et al. Echocardiographic Reference Ranges for Normal Cardiac Chamber Size: Results from the NORRE Study. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 680–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawel-Boehm, N.; Hetzel, S.J.; Ambale-Venkatesh, B.; Captur, G.; Francois, C.J.; Jerosch-Herold, M.; Salerno, M.; Teague, S.D.; Valsangiacomo-Buechel, E.; van der Geest, R.J.; et al. Reference ranges (‘normal values’) for Cardiovascular Magnetic Resonance (CMR) in Adults and Children: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 22, 87. [Google Scholar] [CrossRef] [PubMed]
- Ruijsink, B.; Puyol-Antón, E.; Oksuz, I.; Sinclair, M.; Bai, W.; Schnabel, J.A.; Razavi, R.; King, A.P. Fully Automated, Quality-Controlled Cardiac Analysis from CMR: Validation and Large-Scale Application to Characterize Cardiac Function. JACC Cardiovasc. Imaging 2020, 13, 684–695. [Google Scholar] [CrossRef] [PubMed]
- Avendi, M.R.; Kheradvar, A.; Jafarkhani, H. Automatic Segmentation of the Right Ventricle from Cardiac MRI using a Learning-Based Approach. Magn. Reson. Med. 2017, 78, 2439–2448. [Google Scholar] [CrossRef] [Green Version]
- Bai, W.; Sinclair, M.; Tarroni, G.; Oktay, O.; Rajchl, M.; Vaillant, G.; Lee, A.M.; Aung, N.; Lukaschuk, E.; Sanghvi, M.M.; et al. Automated Cardiovascular Magnetic Resonance Image Analysis with Fully Convolutional Networks. J. Cardiovasc. Magn. Reson. 2018, 20, 65. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training (n = 70) | Validation (n = 30) | Test (n = 50) | p Value | |
|---|---|---|---|---|
| Clinical characteristics | ||||
| Age, years | 66 ± 13 | 71 ± 10 | 68 ± 12 | 0.20 |
| Male | 48 (69) | 19 (63) | 29 (58) | 0.49 |
| Heart rate, beats/min | 65 ± 13 | 65 ± 13 | 70 ± 16 | 0.27 |
| Weight, kg | 64 ± 13 | 60 ± 13 | 60 ± 14 | 0.16 |
| Height, cm | 163 ± 9 | 162 ± 9 | 161 ± 10 | 0.48 |
| Body surface area, m2 | 1.7 ± 0.2 | 1.6 ± 0.2 | 1.6 ± 0.3 | 0.16 |
| Body mass index, kg | 24 ± 4 | 23 ± 3 | 23 ± 4 | 0.42 |
| Cardiovascular disease | ||||
| ICM | 10 (14) | 12 (40) | 10 (20) | |
| HHD | 6 (9) | 1 (3) | 3 (6) | |
| Arrhythmia | 18 (26) | 9 (30) | 14 (28) | |
| HCM | 9 (13) | 3 (10) | 9 (18) | |
| DCM | 8 (11) | 1 (3) | 3 (6) | |
| Sarcoidosis | 3 (4) | 1 (3) | 2 (4) | |
| Amyloidosis | 7 (10) | 2 (7) | 2 (4) | |
| Others | 9 (13) | 1 (3) | 7 (14) | |
| CMR measurements | ||||
| LV function | ||||
| EDV, mL | 169 ± 86 | 137 ± 40 | 143 ± 51 | 0.25 |
| ESV, mL | 110 ± 116 | 70 ± 41 | 77 ± 48 | 0.25 |
| EF, % | 46 ± 17 | 52 ± 16 | 49 ± 14 | 0.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arai, H.; Kawakubo, M.; Sanui, K.; Iwamoto, R.; Nishimura, H.; Kadokami, T. Assessment of Bi-Ventricular and Bi-Atrial Areas Using Four-Chamber Cine Cardiovascular Magnetic Resonance Imaging: Fully Automated Segmentation with a U-Net Convolutional Neural Network. Int. J. Environ. Res. Public Health 2022, 19, 1401. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031401
Arai H, Kawakubo M, Sanui K, Iwamoto R, Nishimura H, Kadokami T. Assessment of Bi-Ventricular and Bi-Atrial Areas Using Four-Chamber Cine Cardiovascular Magnetic Resonance Imaging: Fully Automated Segmentation with a U-Net Convolutional Neural Network. International Journal of Environmental Research and Public Health. 2022; 19(3):1401. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031401
Chicago/Turabian StyleArai, Hideo, Masateru Kawakubo, Kenichi Sanui, Ryoji Iwamoto, Hiroshi Nishimura, and Toshiaki Kadokami. 2022. "Assessment of Bi-Ventricular and Bi-Atrial Areas Using Four-Chamber Cine Cardiovascular Magnetic Resonance Imaging: Fully Automated Segmentation with a U-Net Convolutional Neural Network" International Journal of Environmental Research and Public Health 19, no. 3: 1401. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031401