
The Evaluation of Physical Activity Habits in North Italian People before and during COVID-19 Quarantine: A Pilot Study

 ,
,  ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
- To investigate the physical activity habits of people who lived in two northern regions of Italy (Emilia-Romagna or Veneto) before the COVID-19 and during the first lockdown;
- To understand whether forced indoor PA, due to COVID-19 emergency restrictions, affected PA habits, and if PA acted in a health support role during quarantine. In addition, we wanted to evaluate whether PA mitigated psychological difficulties;
- To investigate peoples’ intentions and motivations to practice PA after lockdown.
2. Materials and Methods
2.1. Study Design
2.2. Questionnaire
2.3. Sample Inclusion Criteria
2.4. Statistical Analyses
3. Results
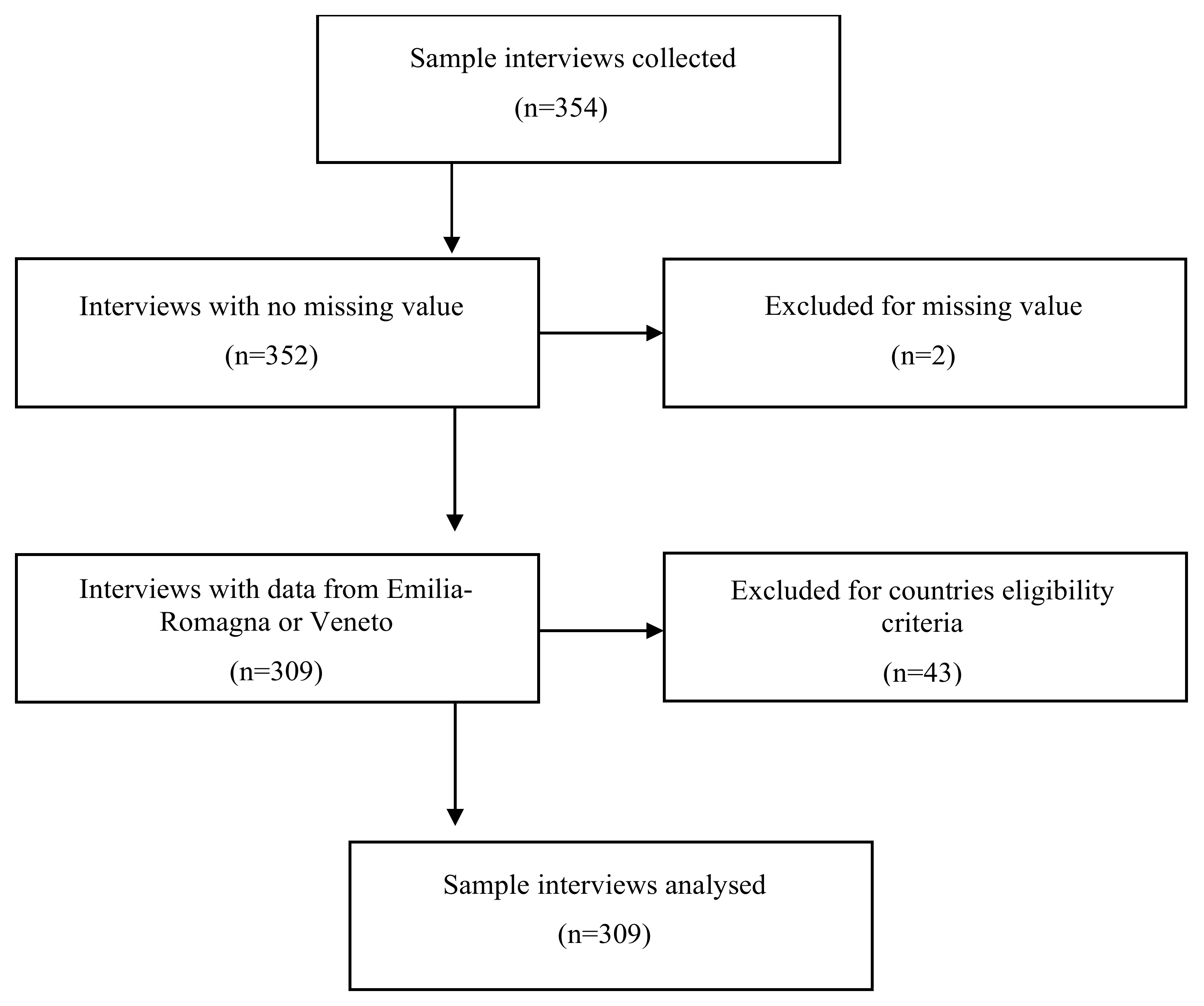
3.1. Sample
3.2. Participants’ Characteristics
3.3. Questionnaire Characteristics
3.4. Physical Activity Characteristics
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Did you practice outdoor physical activity?
- If no, why?
- How often?
- □
- Once per week
- □
- Two times per week
- □
- Three times per week
- □
- Four times per week
- □
- Five times per week
- □
- Everyday
- □
- Less than one time per week
- How many minutes?
- □
- 30
- □
- 60
- □
- 90
- □
- 120
- □
- 150
- □
- 180
- □
- More than 180
- You think your weekly physical activity is:
- □
- More than enough
- □
- Enough
- □
- Not enough
- □
- Poor
- □
- I do not know
- What kind of outdoor physical activity did you practice?
- □
- Walking
- □
- Running
- □
- Resistance training (bodyweight, free-weight, gym equipment)
- □
- Well-being (yoga, pilates, postural gymnastic)
- □
- Functional training
- □
- Other (please specify)
- How long have you practiced PA?
- What is the major problem in practicing outdoor physical activity? (Score 1 to 5, where 1 is absolutely disagree and 5 is absolutely agree)
- Transport
- Inconsistency
- No group coordination
- Conflicted group
- People with compromised autonomy in the group
- Inadequate space
- Did you practice PA alone?
- If not, how important is group activity for you? (Score 1 to 5)
- If you practiced outdoor PA, why did you prefer it to indoor PA?
- After you have practiced outdoor physical activity, what are your feelings? (Score 1 to 5)
- Physical well-being
- Psychological well-being
- Stress reduction
- Anxiety reduction
- Self-satisfaction
- Mood improvement
- Fatigue
- General well-being
- What did you think about your physical conditioning? (Score 1 to 5)
- What did you think about your psychological well-being? (Score 1 to 5)
- Do you think outdoor PA improves your health?
- Why?
- Does outdoor PA satisfy you?
- Did you perform OPA during winter?
- If yes, with the same activity and frequency?
- If no, did you perform indoor PA during winter?
- If yes, what kind of activity?
- Did you practice PA?
- What kind of PA did you practice?
- □
- Walking
- □
- Running
- □
- Resistance training (bodyweight, free-weight, gym equipment)
- □
- Well-being (yoga, pilates, postural gymnastic)
- □
- Functional training
- □
- Other (please specify)
- How often?
- □
- Once per week
- □
- Two times per week
- □
- Three times per week
- □
- Four times per week
- □
- Five times per week
- □
- Everyday
- □
- Less than one time per week
- How many minutes?
- □
- 30
- □
- 60
- □
- 90
- □
- 120
- □
- 150
- □
- 180
- □
- More than 180
- What about modality?
- □
- Autonomously
- □
- With a friend
- □
- With an online trainer
- □
- With a fitness app
- □
- With some social network
- If you practiced group activity, did activity by yourself impact your mood?
- □
- A lot
- □
- Quite
- □
- No
- □
- A little bit
- Was physical activity a support during this period? If yes, why?
- I missed contact with nature
- I missed group socialization
- I thought I would practice outdoor physical activity when lockdown ends
- Do you think you will practice outdoor PA again?
- How often?
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus-data (accessed on 5 December 2021).
- World Health Organization. Health Emergency Dashboard. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?gclid=Cj0KCQjwp86EBhD7ARIsAFkgakj6nMORwUklsOBN-ehjw-1Y0zCsUTTOaSN9oB3Pt9Dr2nQ3zCyJj9YaArKzEALw_wcB (accessed on 9 April 2021).
- Mattioli, A.V.; Puviani, M.B.; Nasi, M.; Farinetti, A. COVID-19 pandemic: The effects of quarantine on cardiovascular risk. Eur. J. Clin. Nutr. 2020, 74, 852–855. [Google Scholar] [CrossRef] [PubMed]
- Bentlage, E.; Ammar, A.; How, D.; Ahmed, M.; Trabelsi, K.; Chtourou, H.; Brach, M. Practical Recommendations for Maintaining Active Lifestyle during the COVID-19 Pandemic: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 6265. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef]
- Ammar, A.; Chtourou, H.; Boukhris, O.; Trabelsi, K.; Masmoudi, L.; Brach, M.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. COVID-19 Home Confinement Negatively Impacts Social Participation and Life Satisfaction: A Worldwide Multicenter Study. Int. J. Environ. Res. Public Health 2020, 17, 6237. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Da Molin, G.; De Giglio, O.; Caggiano, G.; Di Onofrio, V.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; Orsi, G.B.; et al. Understanding Knowledge and Behaviors Related to CoViD–19 Epidemic in Italian Undergraduate Students: The EPICO Study. Int. J. Environ. Res. Public Health 2020, 17, 3481. [Google Scholar] [CrossRef]
- Puccinelli, P.J.; da Costa, T.S.; Seffrin, A.; de Lira, C.; Vancini, R.L.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.; Hill, L.; Andrade, M.S. Correction to: Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: An internet-based survey. BMC Public Health 2021, 21, 693. [Google Scholar] [CrossRef]
- Bezerra, A.; Silva, C.; Soares, F.; Silva, J. Factors associated with people’s behavior in social isolation during the COVID-19 pandemic. Fatores associados ao comportamento da população durante o isolamento social na pandemia de COVID-19. Ciencia Saude Coletiva 2020, 25 (Suppl. S1), 2411–2421. [Google Scholar] [CrossRef]
- Huckins, J.F.; Dasilva, A.W.; Wang, W.; Hedlund, E.; Rogers, C.; Nepal, S.K.; Wu, J.; Obuchi, M.; Murphy, E.I.; Meyer, M.L.; et al. Mental Health and Behavior of College Students During the Early Phases of the COVID-19 Pandemic: Longitudinal Smartphone and Ecological Momentary Assessment Study. J. Med. Internet Res. 2020, 22, e20185. [Google Scholar] [CrossRef]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Prado-Laguna, M.; Hernández-Martínez, A. Physical Activity and Sedentary Lifestyle in University Students: Changes during Confinement Due to the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef]
- Violant-Holz, V.; Gallego-Jiménez, M.G.; González-González, C.S.; Muñoz-Violant, S.; Rodríguez, M.J.; Sansano-Nadal, O.; Guerra-Balic, M. Psychological Health and Physical Activity Levels during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9419. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Da Silveira, M.P.; da Silva Fagundes, K.K.; Bizuti, M.R.; Starck, É.; Rossi, R.C.; de Resende e Silva, D.T. Physical exercise as a tool to help the immune system against COVID-19: An integrative review of the current literature. Clin. Exp. Med. 2021, 21, 15–28. [Google Scholar] [CrossRef]
- Deslandes, A.; Moraes, H.; Ferreira, C.; Veiga, H.; Silveira, H.; Mouta, R.; Pompeu, F.A.; Coutinho, E.S.F.; Laks, J. Exercise and Mental Health: Many Reasons to Move. Neuropsychobiology 2009, 59, 191–198. [Google Scholar] [CrossRef]
- Schreiber, J.B. Issues and recommendations for exploratory factor analysis and principal component analysis. Res. Soc. Adm. Pharm. 2021, 17, 1004–1011. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2021, 2, 53–55. [Google Scholar] [CrossRef]
- Roschel, H.; Artioli, G.G.; Gualano, B. Risk of Increased Physical Inactivity During COVID-19 Outbreak in Older People: A Call for Actions. J. Am. Geriatr. Soc. 2020, 68, 1126–1128. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Ammar, A.; Trabelsi, K.; Brach, M.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: Insights from the ECLB-COVID19 multicentre study. Biol. Sport 2021, 38, 9–21. [Google Scholar] [CrossRef]
- Ansdell, P.; Thomas, K.; Hicks, K.M.; Hunter, S.K.; Howatson, G.; Goodall, S. Physiological sex differences affect the inte-grative response to exercise: Acute and chronic implications. Exp. Physiol. 2020, 105, 2007–2021. [Google Scholar] [CrossRef]
- Lustyk, M.K.; Widman, L.; Paschane, A.A.; Olson, K.C. Physical activity and quality of life: Assessing the influence of ac-tivity frequency, intensity, volume, and motives. Behav. Med. 2004, 30, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Markland, D.; Hardy, L. The exercise motivations inventory: Preliminary development and validity of a measure of indi-viduals’ reasons for participation in regular physical exercise. Pers. Indiv. Differ. 1993, 15, 289–296. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Physical Activity. 2018. Available online: http://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 6 December 2021).
- Grigoletto, A.; Mauro, M.; Latessa, P.M.; Iannuzzi, V.; Gori, D.; Campa, F.; Greco, G.; Toselli, S. Impact of Different Types of Physical Activity in Green Urban Space on Adult Health and Behaviors: A Systematic Review. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 20. [Google Scholar] [CrossRef]
- Nielsen, L.; Reiss, D. Motivation and aging: Toward the next generation of behavioral interventions. In Proceedings of the NIA-BBCSS Expert Meeting, Washington, DC, USA, 18–19 June 2012; National Research Council of the National Academies: Washington, DC, USA, 2012. [Google Scholar]
- Antunes, R.; Frontini, R.; Amaro, N.; Salvador, R.; Matos, R.; Morouço, P.; Rebelo-Gonçalves, R. Exploring Lifestyle Habits, Physical Activity, Anxiety and Basic Psychological Needs in a Sample of Portuguese Adults during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 4360. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Category | Frequency | Percent (%) | n | |
|---|---|---|---|---|
| Gender | Female | 193 | 62.46 | 309 |
| Male | 116 | 37.54 | ||
| Country | Emilia-Romagna | 166 | 53.72 | 309 |
| Veneto | 143 | 46.28 | ||
| Marital status | Married | 154 | 49.84 | 309 |
| Single | 86 | 37.83 | ||
| Engaged | 57 | 18.44 | ||
| Widow | 10 | 3.24 | ||
| Not declared | 2 | 0.65 | ||
| Education | Master’s degree | 108 | 34.95 | 309 |
| Diploma | 106 | 34.3 | ||
| Bachelor | 36 | 11.65 | ||
| Ph.D. | 27 | 8.74 | ||
| Primary or secondary school | 26 | 8.41 | ||
| Other | 6 | 1.94 | ||
| Mean (±std) | Min | Max | n | |
| Age (year) | 46.67 (±15.45) | 18 | 86 | 309 |
| Roommate number | 2.67 (±1.28) | 0 | 6 | 309 |
| Distance between house and park (metres) | 568.55 (±391.8) | 0 | 4000 | 248 |
| Factor 1 | Factor 2 | Factor 3 | |
|---|---|---|---|
| Items (22) | Health (11) | PA parameters (7) | PA problems (4) |
| Psychological well-being | 0.94 | −0.04 | 0.04 |
| Perceived mood | 0.93 | 0.03 | 0.02 |
| General well-being | 0.92 | 0.07 | −0.04 |
| Physical well-being | 0.91 | −0.01 | 0.02 |
| Stress reduction | 0.9 | −0.08 | 0.07 |
| Self-gratification | 0.88 | 0.01 | 0.05 |
| Anxiety reduction | 0.87 | −0.06 | 0.05 |
| Outdoor PA in future | 0.66 | 0.01 | 0.08 |
| Missing nature aspects | 0.54 | 0.05 | 0.2 |
| Perceived fatigue | 0.51 | −0.07 | 0.18 |
| Missing social aspects | 0.39 | −0.2 | 0.19 |
| PA day/week before COVID-19 | −0.12 | 0.78 | 0.13 |
| PA day/week lockdown | 0.03 | 0.75 | −0.01 |
| PA hour/week before COVID-19 | 0.04 | 0.74 | 0.14 |
| PA hour/week lockdown | 0.09 | 0.73 | −0.08 |
| PA day/week goal after lockdown | −0.16 | 0.56 | −0.06 |
| Importance of group for PA | 0.04 | −0.4 | 0.18 |
| Self-perceived PA condition | −0.17 | 0.38 | 0.18 |
| Group level | 0.07 | 0.12 | 0.78 |
| Group coordination | 0.12 | 0.05 | 0.72 |
| Group participant necessity | 0.03 | 0.03 | 0.6 |
| Transport to PA place | −0.02 | −0.15 | 0.48 |
| α = 0.816 | α = 926 | α = 0.78 | α = 0.69 |
| Characteristic | Pre | Lock | Between Groups | Within-Groups | n | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Lock | ∆ | ||||||||||
| χ2 | P | χ2 | P | Z | P | χ2 or Z | P | |||||
| General | 0.81 | 0.84 | 0.93 | 0.39 | 309 | |||||||
| Gender | M | 0.81 | 0.83 | 0.002 | 0.96 | 0.266 | 0.61 | 1.04 | 0.15 | 0.97 | 0.39 | 116 |
| F | 0.81 | 0.85 | 0.1 | 0.76 | 193 | |||||||
| Region | E | 0.84 | 0.85 | 2.73 | 0.1 | 0.17 | 0.68 | 2.35 | 0.01 * | 0.1 | 0.89 | 166 |
| V | 0.77 | 0.83 | 0.68 | 0.29 | 143 | |||||||
| Age | 18–25 | 0.77 | 0.94 | 20.33 | 0.001 * | 16.48 | <0.01 * | Z18–25 vs. 46–55 = 4 | <0.001 * | 2.73 | <0.01 * | 66 |
| 26–35 | 0.63 | 0.67 | Z26–35 vs. 46–55 = −3.47 | <0.001 * | Z18–25 vs. 26–35 = 4.06 | <0.001 * | Z18–25 vs. 56–65 = 10.7 | <0.001 * | 0.41 | 0.68 | 51 | |
| 36–45 | 0.78 | 0.84 | Z18–25 vs. >66 = 5.11 | <0.001 * | 0.77 | 0.443 | 49 | |||||
| 46–55 | 0.89 | 0.88 | Z26–35 vs. 56–65 = −3.9 | <0.001 * | Z26–35 vs. 46–55 = −2.8 | 0.002 * | Z26–35 vs. 56–65 = 4.12 | <0.001 * | 0.24 | 0.807 | 82 | |
| 56–65 | 0.93 | 0.85 | Z36–45 vs. 56–65 = 6.6 | <0.001 * | 1.34 | 0.18 | 46 | |||||
| > 66 | 0.87 | 0.8 | 0.49 | 0.624 | 15 | |||||||
| Pre COVID-19 | Lockdown | ∆ | t | p | ||||
|---|---|---|---|---|---|---|---|---|
| General | Hours/Week | 2.81 ± 1.79 (2.53; 3.1) | 2.63 ± 2.45 (2.25, 3.01) | (−0.12; 0.48) | 1.19 | 0.24 | ||
| Days/Week | 3.05 ± 1.85 (2.76; 3.3) | 3.32 ± 1.86 (3.05; 3.60) | (−0.56; 0.007) | 1.92 | 0.05 | |||
| F | p | F | p | |||||
| Region | Hours/week | 0.08 | 0.78 | 0.21 | 0.64 | |||
| Days/week | 1.73 | 0.19 | 0.12 | 0.73 | ||||
| Gender | Hours/week | 1.55 | 0.21 | 0.59 | 0.44 | |||
| Days/week | 0.02 | 0.88 | 6.26 | 0.01 * | ||||
| Age † | Hours/week | 0.62 | 0.69 | 1.25 | 0.29 | |||
| Days/week | 1.76 | 0.123 | 0.65 | 0.66 | ||||
| OPA | Nature | Group | Physical | Psychol | Anxiety | Stress | Gratific | Mood | Fatigue | General | Motivation | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OPA | 1 | |||||||||||
| Nature | 0.6571 | 1 | ||||||||||
| Group | 0.2499 | 0.247 | 1 | |||||||||
| Physical | 0.5567 | 0.4641 | 0.2233 | 1 | ||||||||
| Psychol | 0.5942 | 0.4889 | 0.2738 | 0.8827 | 1 | |||||||
| Anxiety | 0.5326 | 0.4761 | 0.2165 | 0.731 | 0.7608 | 1 | ||||||
| Stress | 0.5277 | 0.4723 | 0.2059 | 0.7678 | 0.8147 | 0.9102 | 1 | |||||
| Gratific | 0.5012 | 0.3968 | 0.2404 | 0.7663 | 0.7465 | 0.7009 | 0.7453 | 1 | ||||
| Mood | 0.5465 | 0.4335 | 0.2619 | 0.7896 | 0.8145 | 0.8197 | 0.8492 | 0.828 | 1 | |||
| Fatigue | 0.226 | 0.179 | 0.2131 | 0.3024 | 0.3295 | 0.3415 | 0.3241 | 0.3291 | 0.3673 | 1 | ||
| General | 0.5471 | 0.4625 | 0.2702 | 0.8148 | 0.7848 | 0.6976 | 0.7487 | 0.7812 | 0.8069 | 0.3039 | 1 | |
| Motivation | 0.0565 | 0.0894 | 0.2192 | 0.0843 | 0.0533 | 0.1178 | 0.1263 | 0.0694 | 0.1102 | 0.0679 | 0.0262 | 1 |
| Source | SS | df | MS | F | p | n |
|---|---|---|---|---|---|---|
| Model | 281.72 | 2 | 140.858 | 175.67 | <0.001 | 291 |
| Residual | 230.93 | 288 | 0.80184 | |||
| Total | 512.65 | 290 | 1.76774 | |||
| R2 = 0.549 | adjusted R2 = 0.546 | root MSE = 0.895 | ||||
| Coeff. | S.E. | t | p | 95% C.I. | ||
| Intercept | 0.195 | 0.224 | 0.87 | 0.385 | −0.246 | 0.64 |
| Pshychol | 0.453 | 0.06 | 7.62 | <0.001 | 0.336 | 0.57 |
| Nature | 0.494 | 0.044 | 11.21 | <0.001 | 0.41 | 0.58 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mauro, M.; Grigoletto, A.; Zambon, M.C.; Bettocchi, M.; Pegreffi, F.; Fimognari, C.; Bragonzoni, L.; Maietta Latessa, P.; Toselli, S. The Evaluation of Physical Activity Habits in North Italian People before and during COVID-19 Quarantine: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 1660. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031660
Mauro M, Grigoletto A, Zambon MC, Bettocchi M, Pegreffi F, Fimognari C, Bragonzoni L, Maietta Latessa P, Toselli S. The Evaluation of Physical Activity Habits in North Italian People before and during COVID-19 Quarantine: A Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1660. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031660
Chicago/Turabian StyleMauro, Mario, Alessia Grigoletto, Maria Cristina Zambon, Marzia Bettocchi, Francesco Pegreffi, Carmela Fimognari, Laura Bragonzoni, Pasqualino Maietta Latessa, and Stefania Toselli. 2022. "The Evaluation of Physical Activity Habits in North Italian People before and during COVID-19 Quarantine: A Pilot Study" International Journal of Environmental Research and Public Health 19, no. 3: 1660. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031660