
Intimate Relationships and Stroke: Piloting a Dyadic Intervention to Improve Depression

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
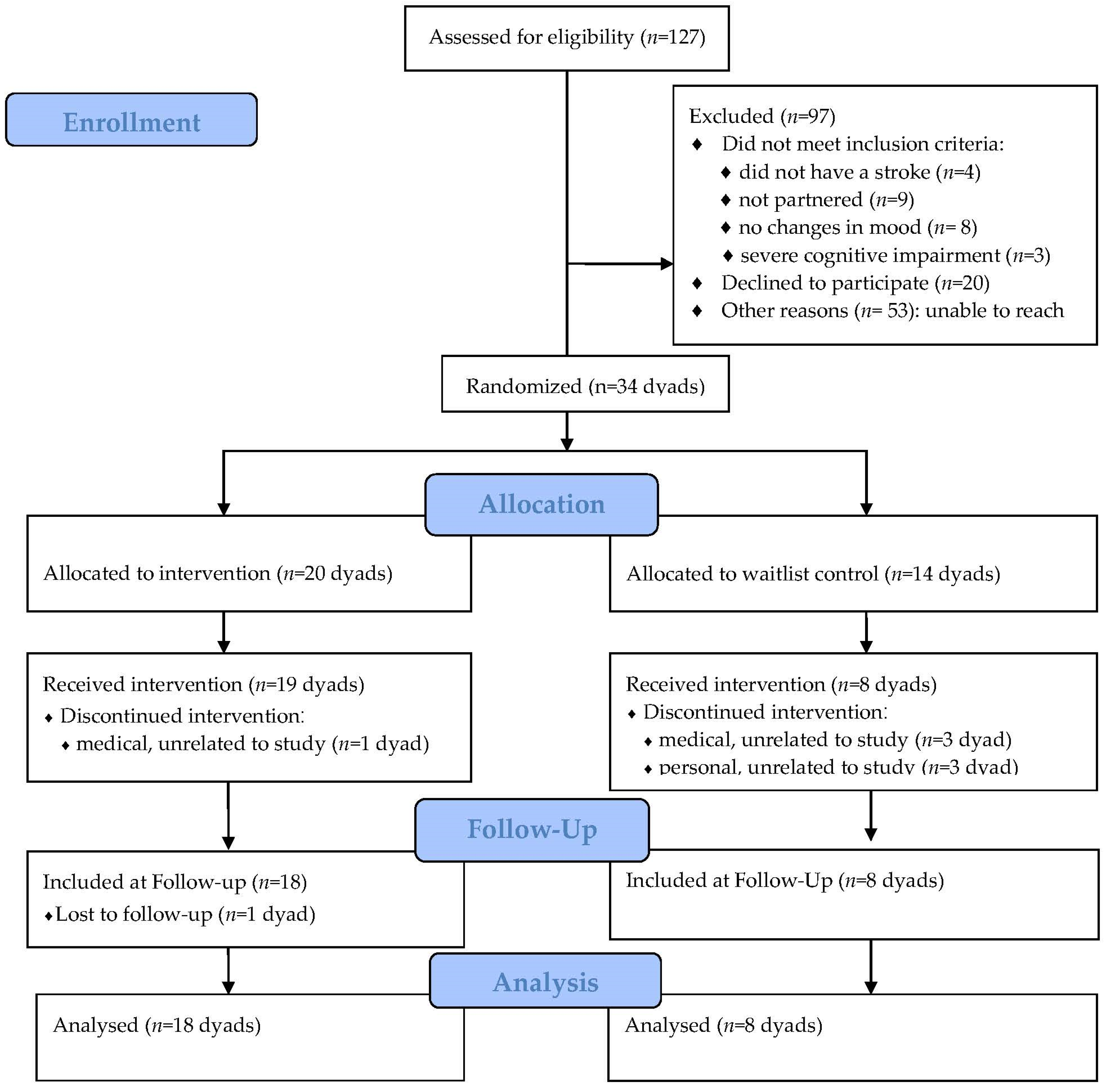
2.1. Design
2.2. Participants
2.3. Procedures
Intervention
2.4. Measures
2.5. Statistical Analysis
3. Results
3.1. Participant Descriptive Data
3.2. Intervention Effects
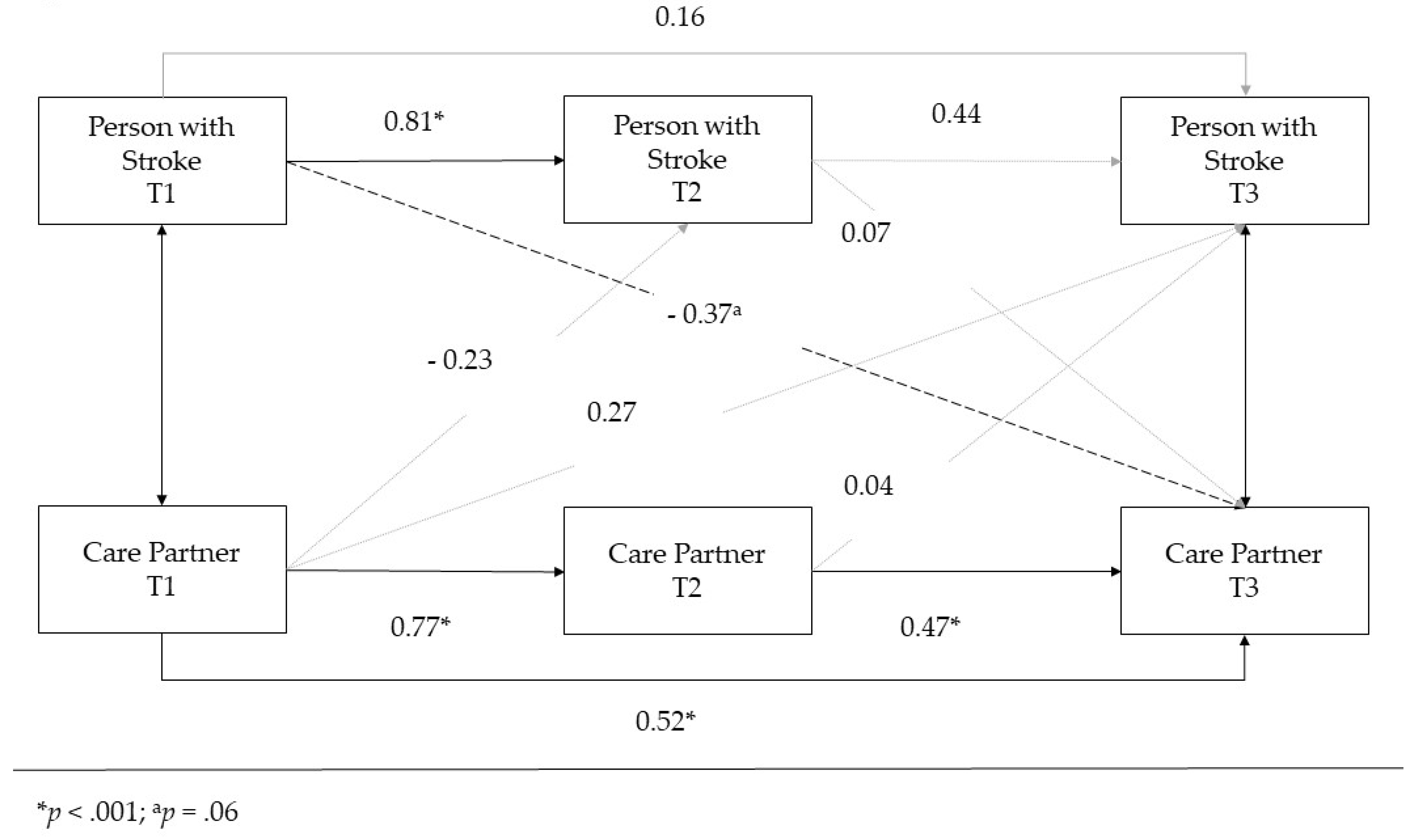
3.3. APIM Analysis
4. Discussion
Study Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Towfighi, A.; Ovbiagele, B.; El Husseini, N.; Hackett, M.L.; Jorge, R.E.; Kissela, B.M.; Mitchell, P.H.; Skolarus, L.E.; Whooley, M.A.; Williams, L.S. Poststroke Depression: A Scientific Statement for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2017, 48, e30–e43. [Google Scholar] [CrossRef] [PubMed]
- Villa, R.F.; Ferrari, F.; Moretti, A. Post-stroke depression: Mechanisms and pharmacological treatment. Pharmacol. Ther. 2018, 184, 131–144. [Google Scholar] [CrossRef]
- Owolabi, M.O. What Are the Consistent Predictors of Generic and Specific Post-Stroke Health-Related Quality of Life? Cerebrovasc. Dis. 2010, 29, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Kutlubaev, M.A.; Hackett, M.L. Part II: Predictors of Depression after Stroke and Impact of Depression on Stroke Outcome: An Updated Systematic Review of Observational Studies. Int. J. Stroke 2014, 9, 1026–1036. [Google Scholar] [CrossRef]
- Hadidi, N.; Treat-Jacobson, D.J.; Lindquist, R. Poststroke depression and functional outcome: A critical review of literature. Heart Lung 2009, 38, 151–162. [Google Scholar] [CrossRef]
- Ayerbe, L.; Ayis, S.; Crichton, S.; Wolfe, C.D.A.; Rudd, A.G. The long-term outcomes of depression up to 10 years after stroke; the South London Stroke Register. J. Neurol. Neurosurg. Psychiatry 2014, 85, 514–521. [Google Scholar] [CrossRef]
- Loh, A.Z.; Tan, J.S.; Zhang, M.W.; Ho, R.C. The Global Prevalence of Anxiety and Depressive Symptoms Among Caregivers of Stroke Survivors. J. Am. Med Dir. Assoc. 2017, 18, 111–116. [Google Scholar] [CrossRef]
- McCarthy, M.J.; Bauer, E. In Sickness and in Health: Couples Coping with Stroke across the Life Span. Health Soc. Work 2015, 40, e92–e100. [Google Scholar] [CrossRef]
- van Heugten, C.; Visser-Meily, A.; Post, M.; Lindeman, E. Care for carers of stroke patients: Evidence-based clinical practice guidelines. J. Rehabil. Med. 2006, 38, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Perrin, P.B.; Heesacker, M.; Hinojosa, M.S.; Uthe, C.E.; Rittman, M.R. Identifying at-risk, ethnically diverse stroke caregivers for counseling: A longitudinal study of mental health. Rehabil. Psychol. 2009, 54, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Perrin, P.B.; Heesacker, M.; Stidham, B.S.; Rittman, M.R.; Gonzalez-Rothi, L.J. Structural equation modeling of the relationship between caregiver psychosocial variables and functioning of individuals with stroke. Rehabil. Psychol. 2008, 53, 54–62. [Google Scholar] [CrossRef]
- McCarthy, M.J.; Lyons, K.S.; Powers, L.E. Expanding Poststroke Depression Research: Movement Toward a Dyadic Perspective. Top. Stroke Rehabil. 2011, 18, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Bakas, T.; Clark, P.C.; Kelly-Hayes, M.; King, R.B.; Lutz, B.J.; Miller, E.L. Evidence for Stroke Family Caregiver and Dyad Interventions: A statement for healthcare professionals from the American Heart Association and American Stroke Association. Stroke 2014, 45, 2836–2852. [Google Scholar] [CrossRef] [Green Version]
- Bakas, T.; McCarthy, M.; Miller, E.T. State-of-the-Science Nursing Review: Update on the State of the Evidence for Stroke Family Caregiver and Dyad Interventions. Stroke 2017, 48, e122–e125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrill, A.L.; Reblin, M.; MacKenzie, J.J.; Cardell, B.; Einerson, J.; Berg, C.A.; Majersik, J.J.; Richards, L. Development of a novel positive psychology-based intervention for couples post-stroke. Rehabil. Psychol. 2018, 63, 43–54. [Google Scholar] [CrossRef]
- Seligman, M.E.P.; Steen, T.A.; Park, N.; Peterson, C. Positive Psychology Progress: Empirical Validation of Interventions. Am. Psychol. 2005, 60, 410–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, D.S.; Dougherty, S.B. Prospects for a Positive Psychology of Rehabilitation. Rehabil. Psychol. 2005, 50, 305–311. [Google Scholar] [CrossRef]
- Alschuler, K.N.; Arewasikporn, A.; Nelson, I.K.; Molton, I.R.; Ehde, D.M. Promoting resilience in individuals aging with multiple sclerosis: Results from a pilot randomized controlled trial. Rehabil. Psychol. 2018, 63, 338–348. [Google Scholar] [CrossRef]
- Cohn, M.A.; Pietrucha, M.E.; Saslow, L.R.; Hult, J.R.; Moskowitz, J.T. An online positive affect skills intervention reduces depression in adults with type 2 diabetes. J. Posit. Psychol. 2014, 9, 523–534. [Google Scholar] [CrossRef]
- Müller, R.; Gertz, K.J.; Molton, I.R.; Terrill, A.; Bombardier, C.H.; Ehde, D.; Jensen, M.P. Effects of a Tailored Positive Psychology Intervention on Well-Being and Pain in Individuals with Chronic Pain and a Physical Disability: A feasibility trial. Clin. J. Pain 2016, 32, 32–44. [Google Scholar] [CrossRef]
- Bolier, L.; Haverman, M.; Westerhof, G.J.; Riper, H.; Smit, F.; Bohlmeijer, E. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public Health 2013, 13, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sin, N.L.; Lyubomirsky, S. Enhancing well-being and alleviating depressive symptoms with positive psychology interventions: A practice-friendly meta-analysis. J. Clin. Psychol. 2009, 65, 467–487. [Google Scholar] [CrossRef] [Green Version]
- Cohn, M.A.; Fredrickson, B.L. In search of durable positive psychology interventions: Predictors and consequences of long-term positive behavior change. J. Posit. Psychol. 2010, 5, 355–366. [Google Scholar] [CrossRef] [Green Version]
- Cook, W.L.; Kenny, D.A. The Actor–Partner Interdependence Model: A model of bidirectional effects in developmental studies. Int. J. Behav. Dev. 2005, 29, 101–109. [Google Scholar] [CrossRef]
- van Belle, G. Statistical Rules of Thumb; Wiley & Sons: New York, NY, USA, 2002. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Patient Health Questionnaire-2: Validity of a two-item depression screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699, Corrigendum in J. Am. Geriatr. Soc. 2019, 67, 1991. [Google Scholar] [CrossRef]
- Barnay, J.-L.; Wauquiez, G.; Bonnin-Koang, H.; Anquetil, C.; Pérennou, D.; Piscicelli, C.; Lucas-Pineau, B.; Muja, L.; le Stunff, E.; de Boissezon, X.; et al. Feasibility of the Cognitive Assessment scale for Stroke Patients (CASP) vs. MMSE and MoCA in aphasic left hemispheric stroke patients. Ann. Phys. Rehabil. Med. 2014, 57, 422–435. [Google Scholar] [CrossRef] [PubMed]
- Flowers, H.L.; Skoretz, S.A.; Silver, F.L.; Rochon, E.; Fang, J.; Flamand-Roze, C.; Martino, R. Poststroke Aphasia Frequency, Recovery, and Outcomes: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2016, 97, 2188–2201.e8. [Google Scholar] [CrossRef]
- Sexton, E.; McLoughlin, A.; Williams, D.J.; Merriman, N.A.; Donnelly, N.; Rohde, D.; Hickey, A.; Wren, M.-A.; Bennett, K. Systematic review and meta-analysis of the prevalence of cognitive impairment no dementia in the first year post-stroke. Eur. Stroke J. 2019, 4, 160–171. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Pilkonis, P.A.; Yu, L.; Dodds, N.E.; Johnston, K.L.; Maihoefer, C.C.; Lawrence, S.M. Validation of the depression item bank from the Patient-Reported Outcomes Measurement Information System (PROMIS®) in a three-month observational study. J. Psychiatr. Res. 2014, 56, 112–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schalet, B.D.; Pilkonis, P.A.; Yu, L.; Dodds, N.; Johnston, K.L.; Yount, S.; Riley, W.; Cella, D. Clinical validity of PROMIS Depression, Anxiety, and Anger across diverse clinical samples. J. Clin. Epidemiol. 2016, 73, 119–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Horton, N.; Carpenter, J.; Pocock, S.J. Strategy for intention to treat analysis in randomised trials with missing outcome data. BMJ 2011, 342, d40. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-Y.; Song, X.-Y. Evaluation of the Bayesian and Maximum Likelihood Approaches in Analyzing Structural Equation Models with Small Sample Sizes. Multivar. Behav. Res. 2004, 39, 653–686. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Pucciarelli, G.; Vellone, E.; Savini, S.; Simeone, S.; Ausili, D.; Alvaro, R.; Lee, C.S.; Lyons, K.S. Roles of Changing Physical Function and Caregiver Burden on Quality of Life in Stroke. Stroke 2017, 48, 733–739. [Google Scholar] [CrossRef]
- Tseung, V.; Jaglal, S.B.; Salbach, N.M.; Cameron, J.I. Implementing Caregiver Support Programs in a Regional Stroke System. Stroke 2019, 50, 3585–3591. [Google Scholar] [CrossRef]
- Creasy, K.R.; Lutz, B.J.; Young, M.E.; Ford, A.; Martz, C. The Impact of Interactions with Providers on Stroke Caregivers’ Needs. Rehabil. Nurs. 2013, 38, 88–98. [Google Scholar] [CrossRef] [Green Version]
- Jia, Y.; Shi, J.; Sznajder, K.K.; Yang, F.; Cui, C.; Zhang, W.; Yang, X. Positive effects of resilience and self-efficacy on World Health Organization Quality of Life Instrument score among caregivers of stroke inpatients in China. Psychogeriatrics 2021, 21, 89–99. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Activities | Descriptions | Examples * |
|---|---|---|
| Gratitude | Be grateful for life circumstances and persons. | Write a thank you note to the therapist. |
| Acts of kindness | Perform good deeds for others. | Drop off a meal for a neighbor who recently had a baby. |
| Relationships | Strengthen relationships, make time for people and be supportive | Have a family game night without electronic “gadgets”. |
| Positive focus | Replay positive experiences | Tell the partner about progress made during therapy. |
| Savoring | Replay life’s momentary pleasures, relish ordinary experiences | Watch the sunset together. |
| Goals | Identify a meaningful goal and devote time to pursuing it | Cook more often/eat out less. |
| Finding meaning | Seek meaning and purpose, find the sacred in ordinary life | Sharing life goals with the partner. |
| Individual Characteristics | Partners with Stroke (n = 34) | Care Partners (n = 34) |
|---|---|---|
| Female, n (%) | 14 (41.17) | 20 (58.82) |
| Age, mean years (SD) | 53.37 (16.14) | 52.97 (14.38) |
| Married, n (%) | 62 (91.2) | |
| Length of relationship, mean years (SD) | 24.89 (17.79) | |
| Education/Employment | ||
| >12 years of education, n (%) | 26 (76.47) | 27 (79.41) |
| Full- or part-time work, n (%) | 3 (8.82) | 19 (55.88) |
| Non-paid work (e.g., homemaker), n (%) | 6 (17.65) | 2 (5.88) |
| Retired, n (%) | 16 (47.06) | 11 (32.35) |
| Unemployed, n (%) | 8 (23.53) | 1 (2.94) |
| Race/Ethnicity | ||
| White, n (%) | 31 (91.18) | 31 (91.18) |
| Asian, n (%) | 1 (2.94) | -- |
| Native Hawaiian or Pacific Islander, n (%) | -- | 1 (2.94) |
| Preferred not to answer/missing, n (%) | 2 (5.88) | 2 (5.88) |
| Depressive Symptoms | ||
| PROMIS-D-SF, mean raw score (SD) | 17.09 (6.93) a | 14.12 (5.53) a |
| Female: PROMIS-D-SF, mean raw score (SD) | 16.92 (6.65) b | 15.65 (6.25) * |
| Male: PROMIS-D-SF, mean raw score (SD) | 17.20 (7.27) b | 11.77 (3.14) * |
| Taking antidepressants, n (%) | 14 (43.8) | 7 (21.9) |
| Stroke Characteristics | ||
| Time since stroke, mean years (SD) | 3.45 (4.72) | |
| Stroke type: ischemic, n (%) | 24 (70.59) | |
| Stroke location: | ||
| Left hemisphere, n (%) | 17 (50.00) | |
| Right hemisphere, n (%) | 11 (32.35) | |
| Other (e.g., brainstem, bilateral), n (%) | 6 (17.65) | |
| Cognitive Screening Score c | ||
| MoCA, mean score (SD) | 16.90 (2.40) | |
| CASP (n = 3), mean score (SD) | 32.00 (1.32) | |
| Physical Function d | ||
| Lawton (IADL) Scale, mean score (SD) | 18.83 (4.44) |
| Dyad Member | Pre-Intervention (T1) M (SD) | Post-Intervention (T2) M (SD) | Mean Difference (T1–T2) | 3-Month Follow-Up (T3) M (SD) | Mean Difference (T2–T3) |
|---|---|---|---|---|---|
| Person with stroke | |||||
| All | 16.68 (6.91) | 14.72 (6.40) | 1.96; p < 0.05 | 15.40 (6.78) | −0.68, p = n/s |
| Score >50th %ile | 22.00 (5.40) | 18.31 (7.03) | 3.69, p < 0.05 | 19.38 (6.71) | −1.08, p = n/s |
| Care partner | |||||
| All | 14.50 (5.78) | 14.54 (6.65) | −0.04, p = n/s | 14.41 (6.23) | 0.13, p = n/s |
| Score >50th %ile | 18.54 (4.93) | 17.23 (7.21) | 1.31, p = n/s | 17.08 (6.90) | 0.15, p = n/s |
| Path | B (SD) | [95% CI] |
|---|---|---|
| T1 Stroke → T2 Stroke | 0.81 (0.15) * | [0.51–1.10] |
| T1 Partner → T2 Stroke | −0.23 (0.16) | [−0.55–0.16] |
| T1 Partner → T2 Partner | 0.77 (0.22) * | [0.23–1.17] |
| T1 Stroke → T2 Partner | −0.06 (0.17) | [−0.47–0.23] |
| T2 Partner → T3 Stroke | 0.04 (0.24) | [−0.54–0.47] |
| T2 Stroke → T3 Stroke | 0.44 (0.35) | [−0.37–1.08] |
| T2 Partner → T3 Partner | 0.47 (0.15) * | [0.19–0.75] |
| T2 Stroke → T3 Partner | 0.07 (0.22) | [−0.34–0.49] |
| Total Actor Effects: T1 Stroke → T3 Stroke | 0.54 (0.23) *** | [0.04–0.95] |
| Direct Effect: T1 Stroke → T3 Stroke | 0.16 (0.34) | [−0.50–0.84] |
| Indirect Effects Total | 0.36 (0.28) | [−0.23–0.93] |
| T1 Stroke → T2 Partner → T3 Stroke | 0.01 (0.04) | [−0.10–0.10] |
| T1 Stroke → T2 Stroke → T3 Stroke | 0.37 (0.29) | [−0.25–0.94] |
| Total Actor Effects: T1 Partner → T3 Partner | 0.85 (0.18) * | [0.48–1.17] |
| Direct Effect: T1 Partner → T3 Partner | 0.52 (0.18) ** | [0.15–0.83] |
| Indirect Effects Total | 0.32 (0.17) *** | [0.04–0.67] |
| T1 Partner → T2 Partner → T3 Partner | 0.33 (0.15) | [0.09–0.65] |
| T1 Partner → T2 Stroke → T3 Partner | −0.01 (0.06) | [−0.17–0.10] |
| Total Partner Effects: T1 Stroke → T3 Partner | −0.33 (0.13) ** | [−0.63–−0.13] |
| Direct Effect: T1 Stroke → T3 Partner | −0.37 (0.21) a | [−0.81–0.01] |
| Indirect Effects Total | 0.03 (0.19) | [−0.37–0.44] |
| T1 Stroke → T2 Partner → T3 Partner | −0.3 (0.08) | [−0.24–0.10] |
| T1 Stroke → T2 Stroke → T3 Partner | 0.06 (0.18) | [−0.29–0.39] |
| Total Partner Effects: T1 Partner → T3 Stroke | 0.18 (0.28) | [−0.40–0.72] |
| Direct Effect: T1 Partner → T3 Stroke | 0.27 (0.34) | [−0.47–0.98] |
| Indirect Effects Total | −0.07 (0.23) | [−0.66–0.31] |
| T1 Partner → T2 Partner → T3 Stroke | 0.03 (0.19) | [−0.41–0.36] |
| T1 Partner → T2 Stroke → T3 Stroke | −0.08 (0.13) | [−0.44–0.11] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terrill, A.L.; Reblin, M.; MacKenzie, J.J.; Baucom, B.R.W.; Einerson, J.; Cardell, B.; Richards, L.G.; Majersik, J.J. Intimate Relationships and Stroke: Piloting a Dyadic Intervention to Improve Depression. Int. J. Environ. Res. Public Health 2022, 19, 1804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031804
Terrill AL, Reblin M, MacKenzie JJ, Baucom BRW, Einerson J, Cardell B, Richards LG, Majersik JJ. Intimate Relationships and Stroke: Piloting a Dyadic Intervention to Improve Depression. International Journal of Environmental Research and Public Health. 2022; 19(3):1804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031804
Chicago/Turabian StyleTerrill, Alexandra L., Maija Reblin, Justin J. MacKenzie, Brian R. W. Baucom, Jackie Einerson, Beth Cardell, Lorie G. Richards, and Jennifer J. Majersik. 2022. "Intimate Relationships and Stroke: Piloting a Dyadic Intervention to Improve Depression" International Journal of Environmental Research and Public Health 19, no. 3: 1804. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031804