
An Efficient Deep Learning Model to Detect COVID-19 Using Chest X-ray Images




Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition
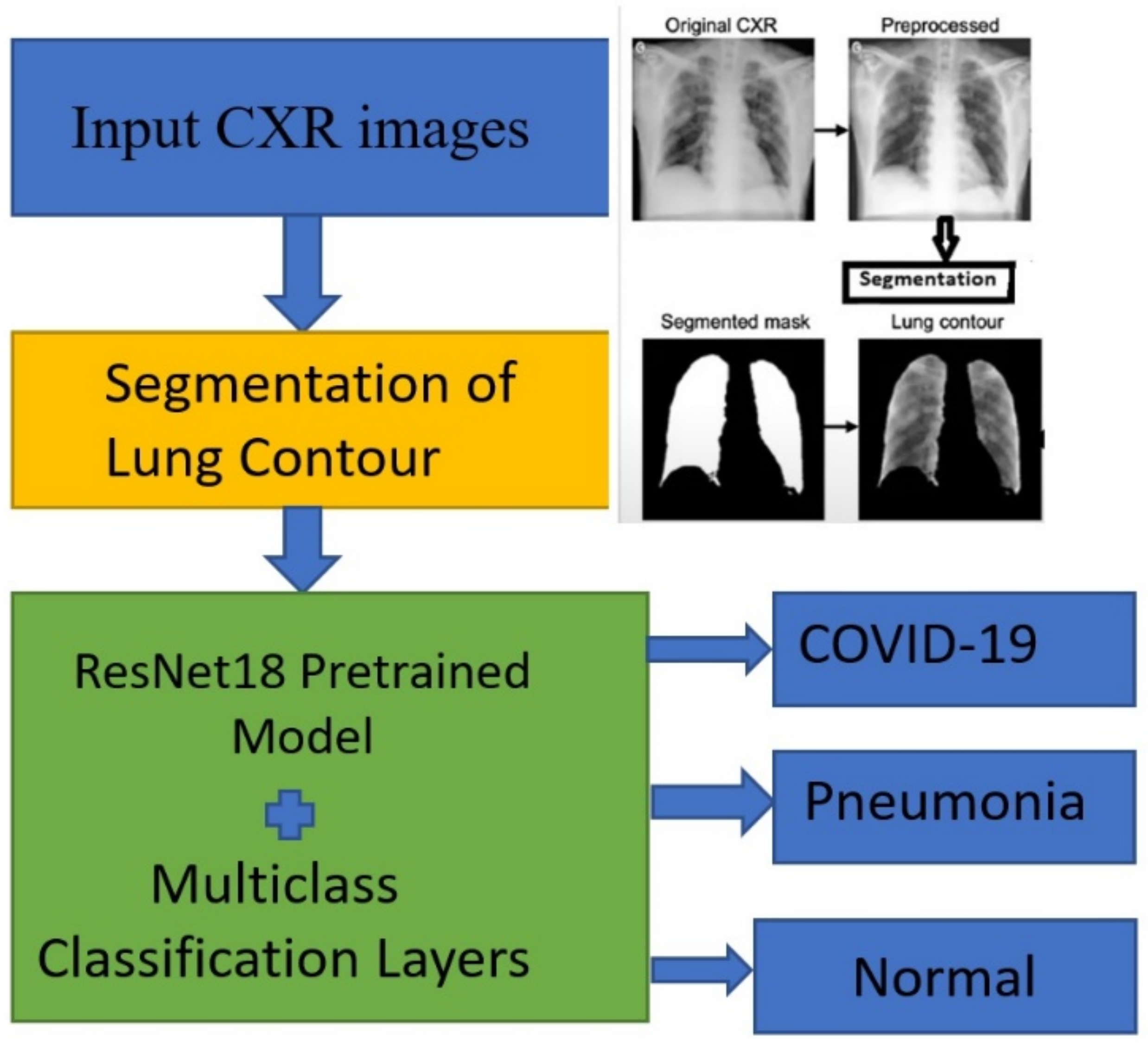
2.2. Preprocessing and Image Segmentation
2.3. Processes Used in the Deep Learning Model (DLM)
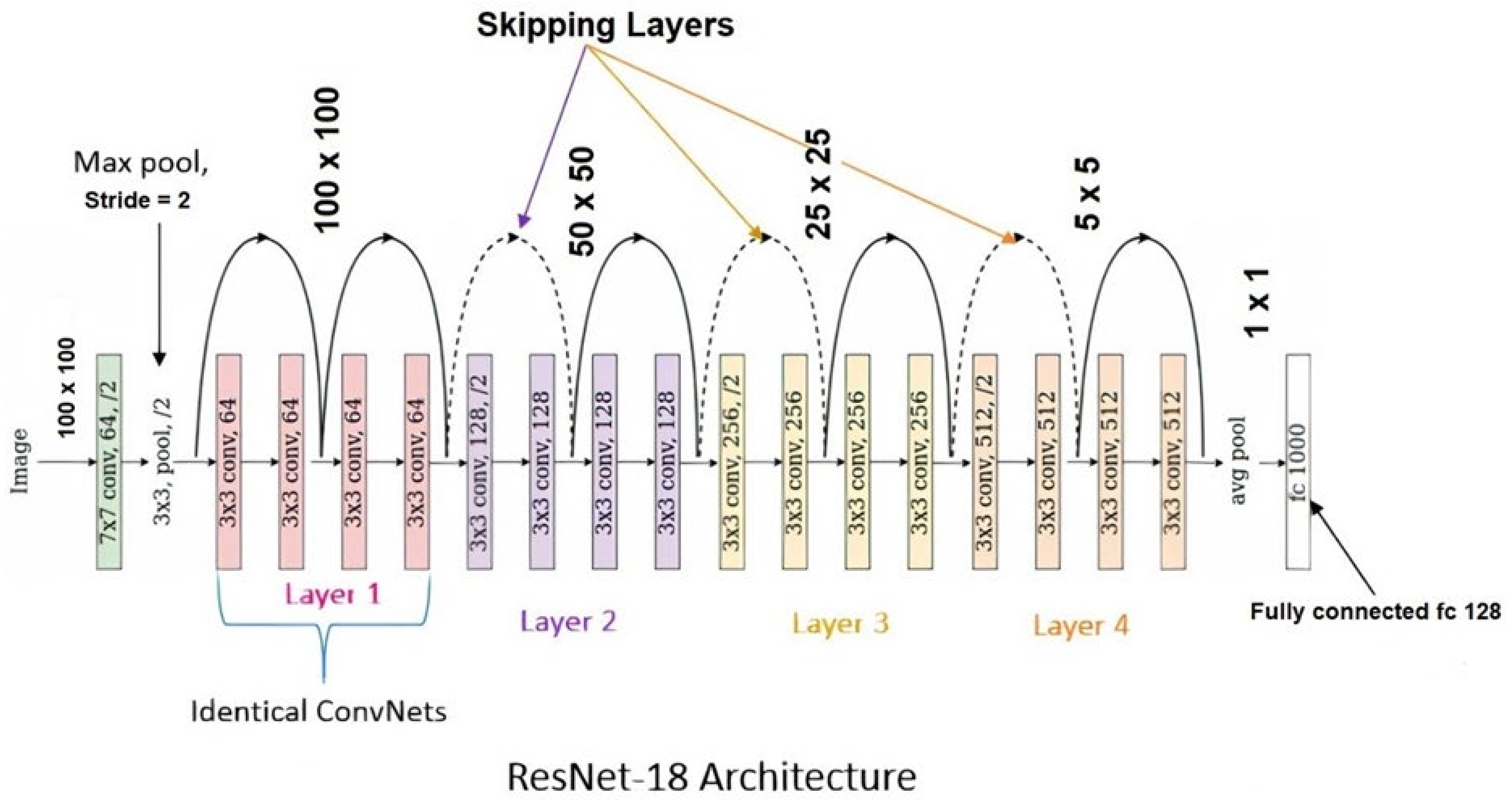
2.4. Description of Deep Learning Models
2.5. Training, Validation, Testing, and Augmentation of Images
2.6. Definitions and Statistical Formulae

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Based on the Gold Standard | |||
|---|---|---|---|
| Disease Present | Disease Absent | Total | |
| Predicted Model Positive | True positive (TP) | False positive (FP) | TP + FP |
| Predicted Model Negative | False negative (FN) | True negative (TN) | FN + TN |
| Total | TP + FN | FP + TN | TP + FP + FN + TN |
2.7. ROC Curve
2.8. Confusion Matrix
3. Results
3.1. Validity Data of the DLM Model
3.2. Comparison of Performance
4. Discussion
4.1. Limitations
4.2. Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Fauci, A.S.; Lane, H.C.; Redfield, R.R. COVID-19—Navigating the uncharted. N. Engl. J. Med. 2020, 382, 1268–1269. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WorldOMeter. Coronavirus. Available online: https://www.worldometers.info/coronavirus/ (accessed on 10 December 2021).
- Gavriatopoulou, M.; Korompoki, E.; Fotiou, D.; Ntanasis-Stathopoulos, I.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Organ-specific manifestations of COVID-19 infection. Clin. Exp. Med. 2020, 20, 493–506. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-Cov-2 in different types of clinical specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [Green Version]
- Brihn, A.; Chang, J.; OYong, K.; Balter, S.; Terashita, D.; Rubin, Z.; Yeganeh, N. Diagnostic performance of an antigen test with RT-PCR for the detection of SARS-CoV-2 in a hospital setting—Los Angeles County, California, June-August 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 702–706. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest CT and RT-PCR testing for coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Fan, L.; Li, D.; Xue, H.; Zhang, L.; Liu, Z.; Zhang, B.; Zhang, L.; Yang, W.; Xie, B.; Duan, X.; et al. Progress and prospect on imaging diagnosis of COVID-19. Chin. J. Acad. Radiol. 2020, 3, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Bai, H.X.; Hsieh, B.; Xiong, Z.; Halsey, K.; Choi, J.W.; Tran, T.M.L.; Pan, I.; Shi, L.-B.; Wang, D.-C.; Mei, J.; et al. Performance of radiologists in differentiating COVID-19 from viral pneumonia on chest CT. Radiology 2020, 296, 200823. [Google Scholar] [CrossRef]
- He, X.; Yang, X.; Zhang, S.; Zhao, J.; Zhang, Y.; Xing, E.; Xie, P. Sample-efficient deep learning for COVID-19 diagnosis based on CT scans. IEEE Trans. Med. Imaging. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.04.13.20063941v1.full.pdf (accessed on 10 December 2021).
- Gunraj, H.; Wang, L.; Wong, A. COVIDNet-CT: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest CT images. Front. Med. 2020. Available online: https://www.frontiersin.org/articles/10.3389/fmed.2020.608525/full (accessed on 10 December 2021).
- Harmon, S.A.; Sanford, T.H.; Xu, S.; Turkbey, E.B.; Roth, H.; Xu, Z.; Yang, D.; Myronenko, A.; Anderson, V.; Amalou, A.; et al. Artificial intelligence for the detection of COVID-19 pneumonia on chest CT using multinational datasets. Nat. Commun. 2020, 11, 4080. [Google Scholar] [CrossRef]
- Das, D.; Santosh, K.C.; Pal, U. Truncated inception net: COVID-19 outbreak screening using chest X-rays. Phys. Eng. Sci. Med. 2020, 43, 915–925. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, A.K.; Tiwari, P.; Kumar, S.; Gupta, D.; Khanna, A.; Rodrigues, J.P.C. Identifying pneumonia in chest X-rays: A deep learning approach. Measurement 2019, 145, 511–518. [Google Scholar] [CrossRef]
- Annarumma, M.; Withey, S.J.; Bakewell, R.J.; Pesce, E.; Goh, V. Automated triaging of adult chest radiographs with deep artificial neural networks. Radiology 2019, 291, 272. [Google Scholar] [CrossRef] [Green Version]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Delta Variant: What We Know about the Science. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/delta-variant.html?s_cid=11512:cdc%20delta%20variant:sem.ga:p:RG:GM:gen:PTN:FY21 (accessed on 9 December 2021).
- Centers for Disease Control and Prevention. Omicron Variant: What You Need to Know. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/omicron-variant.html (accessed on 9 December 2021).
- US Food & Drug Administration. Coronavirus Testing Basics. Available online: https://www.fda.gov/media/138094/download (accessed on 9 December 2021).
- Shiraishi, J.; Katsuragawa, S.; Ikezoe, J.; Matsumoto, T.; Kobayashi, T.; Komatsu, K.-I.; Matsui, M.; Fujita, H.; Kodera, Y.; Doi, K. Development of a digital image database for chest radiographs with and without a lung nodule. Am. J. Roentgenol. 2020, 174, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Praveen. Corona Hack-Chest X-ray-Dataset. Available online: https://www.kaggle.com/praveengovi/coronahack-chest-xraydataset (accessed on 8 December 2021).
- Cohen, J.P.; Morrison, P.; Dao, L. COVID-19 Image Data Collection. arXiv 2020, arXiv:2003.11597. Available online: https://arxiv.org/abs/2003.11597 (accessed on 8 December 2021).
- Paul, C.J. COVID-19 Image Data Collection. 2020. Available online: https://github.com/ieee8023/covid-chestxray-dataset (accessed on 7 December 2021).
- Paul, M. Kaggle Chest X-ray Images (Pneumonia) Dataset. 2020. Available online: https://www.kaggle.com/paultimothymooney/chest-xray-pneumonia (accessed on 8 December 2021).
- Mittal, A.; Kumar, D.; Mittal, M.; Saba, T.; Abunadi, I.; Rehman, A.; Roy, S. Detecting pneumonia using convolutions and dynamic capsule routing for chest X-ray images. Sensors 2020, 20, 1068. [Google Scholar] [CrossRef] [Green Version]
- Ginneken, B.V.; Stegmann, M.B.; Loog, M. Segmentation of anatomical structures in chest radiographs using supervised methods: A comparative study on a public database. Med. Image Anal. 2006, 10, 19–40. [Google Scholar] [CrossRef] [Green Version]
- Jaeger, S.; Candemir, S.; Antani, S.; Wang, Y.X.J.; Lu, P.X.; Thoma, G. Two public chest X-ray datasets for computer aided screening of pulmonary diseases. Quant. Imag. Med. Surg. 2014, 4, 475. [Google Scholar]
- Jegou, S.; Drozdzal, M.; Vazquez, D.; Romero, A.; Bengio, Y. The one hundred layers tiramisu: Fully convolutional DenseNets for semantic segmentation. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition Workshops, Honolulu, HI, USA, 21–26 July 2017; pp. 1175–1183. [Google Scholar] [CrossRef] [Green Version]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef] [Green Version]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet classification with deep convolutional neural networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Maaten, L.V.D.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zou, J.; He, K.; Sun, J. Accelerating very deep convolutional networks for classification and detection. IEEE Trans. Pattern Anal. Mach. Intell. 2016, 38, 1943–1955. [Google Scholar] [CrossRef] [Green Version]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. CheXNet: Radiologist-level pneumonia detection on chest X-rays with deep learning. arXiv 2017, arXiv:1711.05225. Available online: http://arxiv.org/abs/1711.05225 (accessed on 8 December 2021).
- Das, N.N.; Kumar, N.; Kaur, M.; Kumar, V.; Singh, D. Automated deep transfer learning-based approach for detection of COVID-19 infection in chest X-rays. Ing. Rech. Biomed. 2020; in press. [Google Scholar] [CrossRef]
- Wang, L.; Lin, Z.Q.; Wong, A. COVID-Net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci. Rep. 2020, 10, 19549. [Google Scholar] [CrossRef]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks. Pattern Anal. Appl. 2021, 24, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Altan, A.; Karasu, S.S. Recognition of COVID-19 disease from X-ray images by hybrid model consisting of 2D curvelet transform, chaotic salp swarm algorithm and deep learning technique. Chaos Solitons Fractals 2020, 140, 110071. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, T.; Talo, M.; Yildirim, E.A.; Baloglu, U.B.; Yildirim, O.; Acharya, U.R. Automated detection of COVID-19 cases using deep neural networks with X-ray images. Comput. Biol. Med. 2020, 121, 103792. [Google Scholar] [CrossRef]
- Minaee, S.; Kafish, R.; Sonka, M.; Yazdani, S.; Soufi, G.J. Deep-COVID: Predicting COVID-19 from chest X-ray images using deep transfer learning. Med. Image Anal. 2020, 65, 101794. [Google Scholar] [CrossRef]
- Khan, A.I.; Shah, J.L.; Bhat, M.M. CoroNet: A deep neural network for detection and diagnosis of COVID-19 from chest X-ray images. Comput. Meth. Prog. Biomed. 2020, 196, 105581. [Google Scholar] [CrossRef]
- Civit-Masot, J.; Luna-Perejón, F.; Morales, M.D.; Civit, A. Deep learning system for COVID-19 diagnosis aid using X-ray pulmonary images. Appl. Sci. 2020, 10, 4640. [Google Scholar] [CrossRef]
- Yang, D.; Martinez, C.; Visuña, L.; Khandhar, H.; Bhatt, C.; Carretero, J. Detection and analysis of COVID-19 in medical images using deep learning techniques. Sci. Rep. 2021, 11, 19638. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.Z.; Islam, M.M.; Asraf, A. A combined deep CNN-LSTM network for the detection of novel coronavirus (COVID-19) using X-ray images. Informat. Med. Unlocked. 2020, 20, 100412. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.M.; Bertolini, D.; Teixeira, L.O.; Silla, C.N.; Costa, Y.M.G. COVID-19 identification in chest X-ray images on at and hierarchical classification scenarios. Comput. Meth. Prog. Bio. 2020, 194, 105532. [Google Scholar] [CrossRef] [PubMed]
- Hemdan, E.E.D.; Shouman, M.A.; Karar, M.E. COVIDXNet: A framework of deep learning classifiers to diagnose COVID-19 in X-ray images. arXiv 2020, arXiv:2003.11055. Available online: http://arxiv.org/abs/2003.11055 (accessed on 8 December 2021).
- Panwar, H.; Gupta, P.K.; Siddiqui, M.K.; Morales-Menendez, R.; Bhardwaj, P.; Singh, V. A deep learning and grad-CAM based color visualization approach for fast detection of COVID-19 cases using chest X-ray and CT-Scan images. Chaos Solitons Fractals 2020, 140, 110190. [Google Scholar] [CrossRef]
- LeCun, Y.; Kavukcuoglu, K.; Farabet, C. Convolutional networks and applications in vision. In Proceedings of the ISCAS 2010—2010 IEEE International Symposium on Circuits and Systems: Nano-Bio Circuit Fabrics and Systems, Paris, France, 30 May–2 June 2010; IEEE: Piscataway, NY, USA, 2010; pp. 253–256. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, S. Category identification technique by a semantic feature generation algorithm. In Deep Learning for Internet of Things Infrastructure; CRC Press: Boca Raton, FL, USA, 2021; pp. 129–144. [Google Scholar]
- Zhang, K.; Liu, X.; Shen, J.; Li, Z.; Sang, Y.; Wu, X.; Zha, Y.; Liang, W.; Wang, C.; Wang, K.; et al. Clinically applicable AI system for accurate diagnosis, quantitative measurements, and prognosis of COVID-19 pneumonia using computed tomography. Cell 2020, 181, 1423–1433. [Google Scholar] [CrossRef]
- Rahaman, M.M.; Li, C.; Yao, Y.; Kulwa, F.; Rahman, M.A.; Wang, Q.; Qi, S.; Kong, F.; Zhu, X.; Zhao, X. Identification of COVID-19 samples from chest X-ray images using deep learning: A comparison of transfer learning approaches. J. X-ray Sci. Technol. 2020, 28, 821–839. [Google Scholar] [CrossRef]
- Manokaran, J.; Zabihollahy, F.; Hamilton-Wright, A.; Ukwatta, E. Detection of COVID-19 from chest X-ray images using transfer learning. J. Med. Imaging 2021, 8, 017503. [Google Scholar] [CrossRef]
- Arias-Garzón, D.; Alzate-Grisales, J.A.; Orozco-Arias, S.; Arteaga-Arteaga, H.B.; Bravo-Ortiz, M.A.; Mora-Rubio, A.; Saborit-Torres, J.M.; Serrano, J.M.; Tabares-Soto, R.; Vayá, M.D.L.I. COVID-19 detection in X-ray images using convolutional neural networks. Mach. Learn. Appl. 2021, 6, 100138. [Google Scholar] [CrossRef]
- Ebenuwa, S.H.; Sharif, M.S.; Alazab, M.; Nemrat, A.A. Variance ranking attributes selection techniques for binary classification problem in imbalance data. IEEE Access 2019, 7, 24649–24666. [Google Scholar] [CrossRef]
- Khushi, M.; Shaukat, K.; Alam, T.A.; Hameed, I.A.; Uddin, S.; Luo, S.; Yang, X.; Reyes, M.C. A comparative performance analysis of data resampling methods on imbalance medical data. IEEE Access 2021, 9, 109960–109975. [Google Scholar] [CrossRef]
- Jegierski, H.; Saganowski, S. An “Outside the Box” solution for imbalanced data classification. IEEE Access 2020, 8, 125191–125209. [Google Scholar] [CrossRef]
- Alam, T.; Ahmed, C.F.; Zahin, S.A.; Khan, M.A.H.; Islam, M.T. An effective recursive technique for multi-class classification and regression for imbalanced data. IEEE Access 2019, 7, 127615–127630. [Google Scholar] [CrossRef]
- Maillo, J.; Triguero, I.; Herrera, F. Redundancy and complexity metrics for big data classification: Towards smart data. IEEE Access 2020, 8, 87918–87928. [Google Scholar] [CrossRef]





| Stage of Data | COVID-19 | Pneumonia | Normal | Total |
|---|---|---|---|---|
| Before augmentation | 2143 | 3674 | 4223 | 10,040 |
| After augmentation | 3535 | 6072 | 6967 | 16,574 |
| Study [Ref] | No. Images Used | AI Method Used | Accuracy | Sensitivity | Specificity | F1-Score |
|---|---|---|---|---|---|---|
| Proposed Model | 10,040 | Deep Learning Model | 96.43 | 93.68 | 99.0 | 93.0 |
| Das et al. [35] | Unknown | Deep transfer learning | 92.41 | 91.29 | 92.0 | 89.0 |
| Wang et al. [36] | 13,975 | Deep convolutional neural network | 92.04 | 90.41 | 94.0 | 87.0 |
| Narin et al. [37] | 7486 | Deep convolutional neural network | 91.26 | 89.24 | 93.0 | 86.0 |
| Altan et al. [38] | 2905 | A hybrid model, having 2D Curvelet transformation, a Salp swarm algorithm (SSA) and deep learning | 91.85 | 92.42 | 91.0 | 90.0 |
| Ozturk et al. [39] | 1000 | Deep neural network | 93.40 | 92.12 | 89.0 | 90.0 |
| Minaee et al. [40] | 5,000 | Deep transfer learning | 90.49 | 92.08 | 91.0 | 88.0 |
| Khan et al. [41] | 1300 | Deep neural network | 89.60 | 84.98 | 87.0 | 86.0 |
| Civit-Masot et al. [42] | 396 | VGG16-based (convolutional) Deep Learning Model | 94.52 | 92.11 | 96.0 | 92.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chakraborty, S.; Murali, B.; Mitra, A.K. An Efficient Deep Learning Model to Detect COVID-19 Using Chest X-ray Images. Int. J. Environ. Res. Public Health 2022, 19, 2013. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042013
Chakraborty S, Murali B, Mitra AK. An Efficient Deep Learning Model to Detect COVID-19 Using Chest X-ray Images. International Journal of Environmental Research and Public Health. 2022; 19(4):2013. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042013
Chicago/Turabian StyleChakraborty, Somenath, Beddhu Murali, and Amal K. Mitra. 2022. "An Efficient Deep Learning Model to Detect COVID-19 Using Chest X-ray Images" International Journal of Environmental Research and Public Health 19, no. 4: 2013. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042013