
Prevalence of Physical Activity and Sedentary Behaviors in the French Population: Results and Evolution between Two Cross-Sectional Population-Based Studies, 2006 and 2016

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
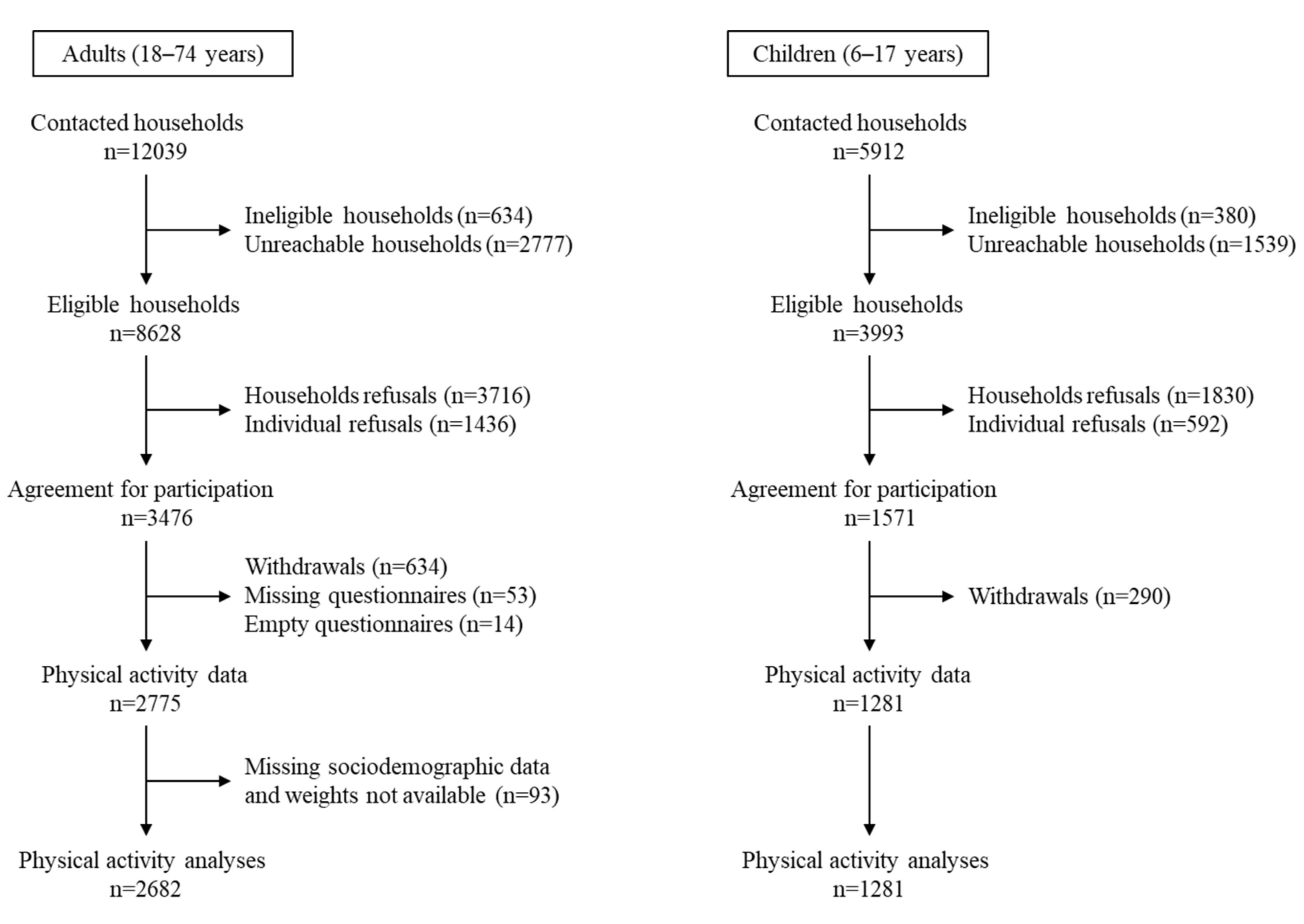
2.1. Study Design
2.2. Sociodemographic Data
2.3. Measures of Physical Activity and Sedentary Behaviors
2.4. Data Analysis
3. Results
3.1. Prevalence of Physical Activity and Sedentary Behaviors in Adults in the Esteban Study (2014–2016)
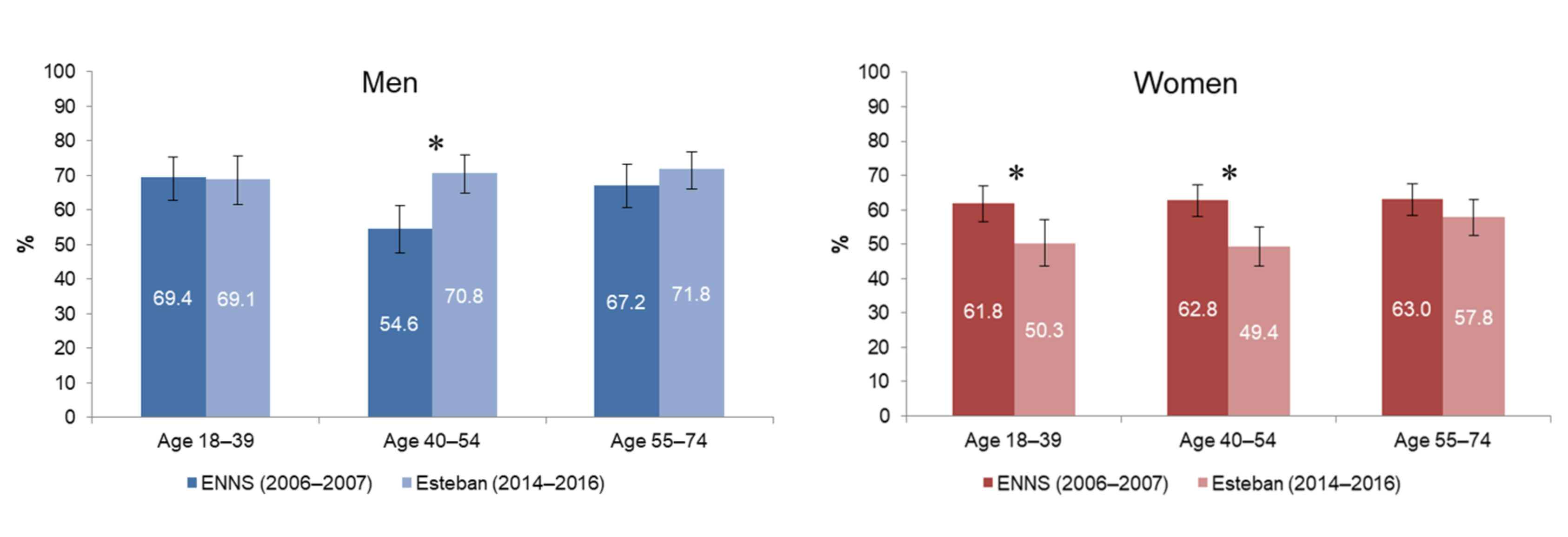
3.2. Physical Activity Prevalence of Adults since 2006
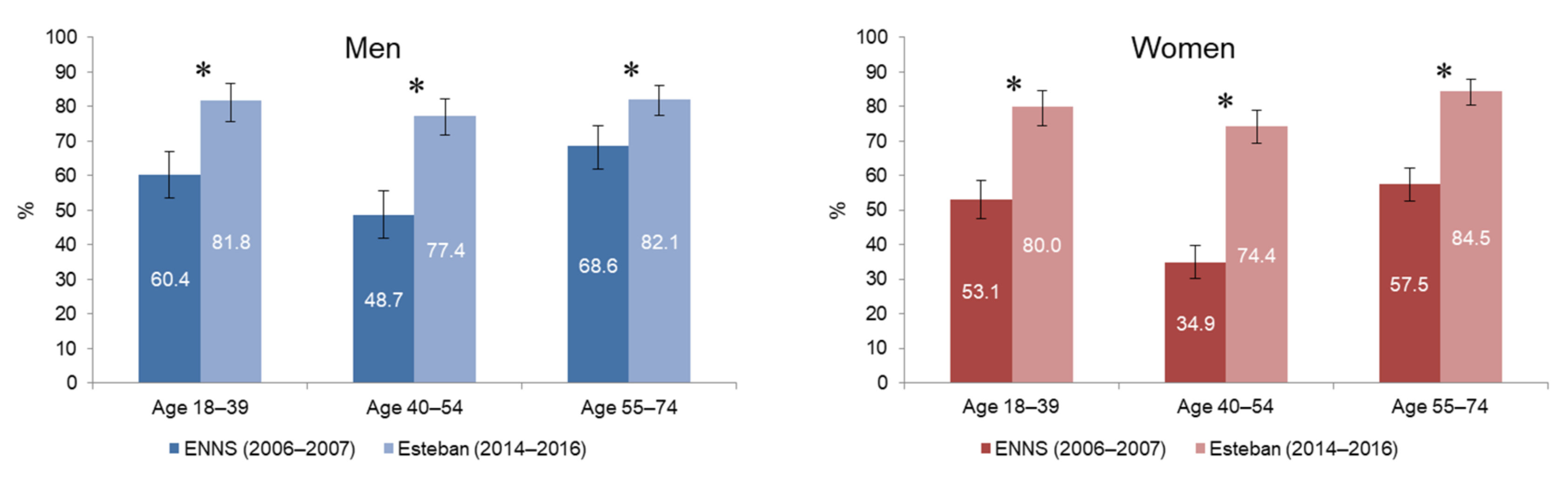
3.3. Daily Leisure Screen Time of Adults since 2006
3.4. Prevalence of Physical Activity and Sedentary Behaviors in Children in the Esteban Study (2014–2016)
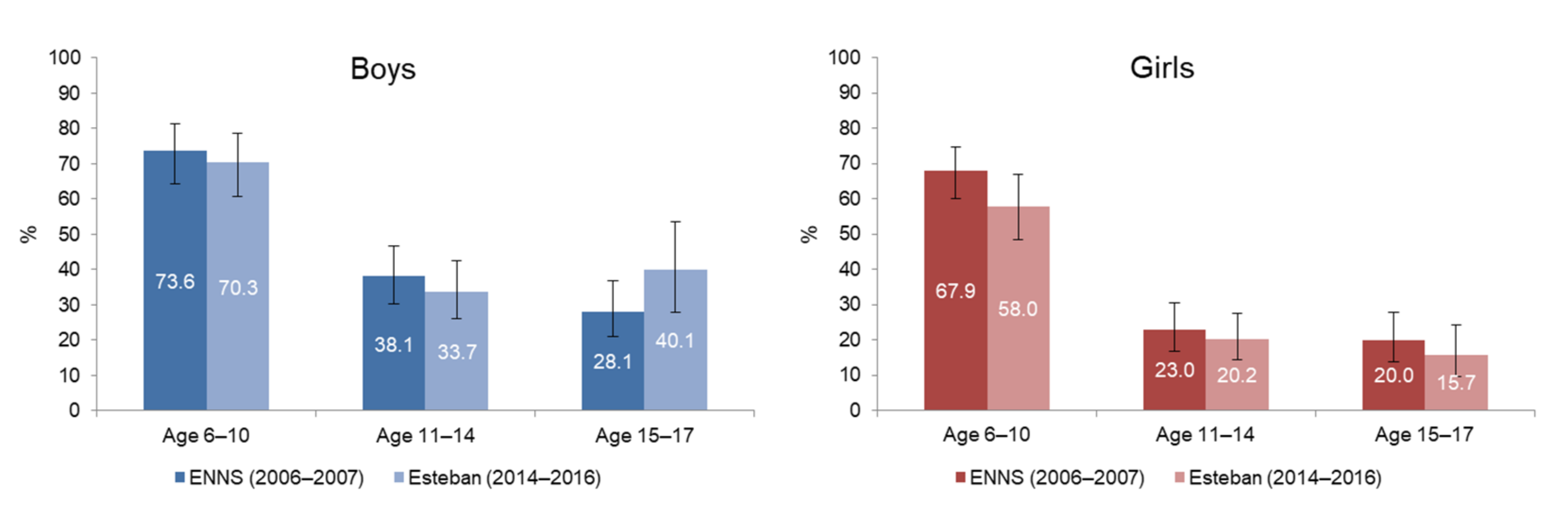
3.5. Physical Activity Prevalence of Children since 2006
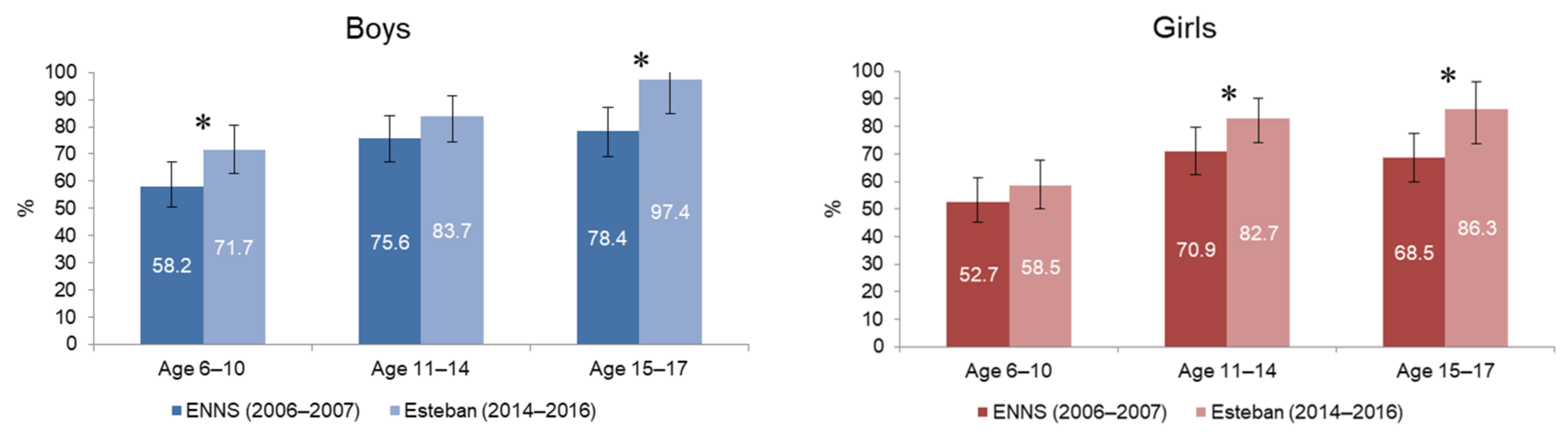
3.6. Daily Leisure Screen Time of Children since 2006
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Physical Activity; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Carson, V.; Lee, E.Y.; Hewitt, L.; Jennings, C.; Hunter, S.; Kuzik, N.; Stearns, J.A.; Unrau, S.P.; Poitras, V.J.; Gray, C.; et al. Systematic review of the relationships between physical activity and health indicators in the early years (0–4 years). BMC Public Health 2017, 17 (Suppl. 5), 854. [Google Scholar]
- Jakicic, J.M.; Kraus, W.E.; Powell, K.E.; Campbell, W.W.; Janz, K.F.; Troiano, R.; Sprow, K.; Torres, A.; Piercy, K.L. Association between Bout Duration of Physical Activity and Health: Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1213–1219. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Hillman, C.H.; Janz, K.F.; Katzmarzyk, P.T.; Powell, K.E.; Torres, A.; Whitt-Glover, M.C. Physical Activity and Health in Children Younger than 6 Years: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor Gorber, S.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Kahlmeier, S.; the Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Participants, S.T.C.P. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Mansoubi, M.; Pearson, N.; Biddle, S.J.; Clemes, S. The relationship between sedentary behaviour and physical activity in adults: A systematic review. Prev. Med. 2014, 69, 28–35. [Google Scholar] [CrossRef]
- Chau, J.Y.; Grunseit, A.; Chey, T.; Stamatakis, E.; Brown, W.J.; Matthews, C.; Bauman, A.E.; van der Ploeg, H. Daily Sitting Time and All-Cause Mortality: A Meta-Analysis. PLoS ONE 2013, 8, e80000. [Google Scholar] [CrossRef] [Green Version]
- Chau, J.Y.; Grunseit, A.; Midthjell, K.; Holmen, J.; Holmen, T.L.; Bauman, A.E.; van der Ploeg, H.P. Cross-sectional associations of total sitting and leisure screen time with cardiometabolic risk in adults. Results from the HUNT Study, Norway. J. Sci. Med. Sport 2014, 17, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezende, L.; Sa, T.; Mielke, G.; Viscondi, J.; Rey-Lopez, J.; Garcia, L. All-Cause Mortality Attributable to Sitting Time: Analysis of 54 Countries Worldwide. Am. J. Prev. Med. 2016, 51, 253–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Loyen, A.; van der Ploeg, H.; Bauman, A.; Brug, J.; Lakerveld, J. European Sitting Championship: Prevalence and Correlates of Self-Reported Sitting Time in the 28 European Union Member States. PLoS ONE 2016, 11, e0149320. [Google Scholar] [CrossRef] [Green Version]
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, D.; De Looze, M.; Roberts, C.; Samdal, O.; Smith, O.R.; Barnekow, V. Social determinants of health and well-being among young people. In Health Behaviour in School-aged Children (HBSC) Study: International Report from the 2009/2010 Survey; WHO Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Zhu, X.; Haegele, J.A.; Tang, Y.; Wu, X. Prevalence and Demographic Correlates of Overweight, Physical Activity, and Screen Time Among School-Aged Children in Urban China: The Shanghai Study. Asia Pac. J. Public Health 2018, 30, 118–127. [Google Scholar] [CrossRef]
- Biswas, A.; Oh, P.; Faulkner, G.; Bajaj, R.; Silver, M.; Mitchell, M.; Alter, D. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World: At-a-Glance; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Balicco, A.; Oleko, A.; Szego, E.; Boschat, L.; Deschamps, V.; Saoudi, A.; Zeghnoun, A.; Fillol, C. Protocole Esteban: Une Etude transversale de SanTé sur l’Environnement, la Biosurveillance, l’Activité physique et la Nutrition (2014–2016). Toxicol. Anal. Clin. 2017, 29, 517–537. [Google Scholar] [CrossRef]
- Castetbon, K.; Vernay, M.; Malon, A.; Salanave, B.; Deschamps, V.; Roudier, C.; Oleko, A.; Szego, E.; Hercberg, S. Dietary intake, physical activity and nutritional status in adults: The French nutrition and health survey (ENNS, 2006–2007). Br. J. Nutr. 2009, 102, 733–743. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Russell, S.J.; Cameron, C. Reliability and validity of Canada’s Physical Activity Monitor for assessing trends. Med. Sci. Sports Exerc. 2002, 34, 1462–1467. [Google Scholar] [CrossRef] [PubMed]
- Golubić, R.; May, A.M.; Borch, K.B.; Overvad, K.; Charles, M.-A.; Díaz, M.J.T.; Amiano, P.; Palli, M.; Valanou, E.; Vigl, M.; et al. Validity of Electronically Administered Recent Physical Activity Questionnaire (RPAQ) in Ten European Countries. PLoS ONE 2014, 9, e92829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fillon, A.; Genin, P.; Larras, B.; Vanhelst, J.; Luiggi, M.; Aubert, S.; Verdot, C.; Rey, O.; Lhuisset, L.; Bois, J.; et al. France’s 2020 Report Card on Physical Activity and Sedentary Behaviors in Children and Youth: Results and Progression. J. Phys. Act. Health 2021, 18, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Bennie, J.; Pedisic, Z.; van Uffelen, J.; Gale, J.; Banting, L.; Vergeer, I.; Stamatakis, E.; Bauman, A.; Biddle, S. The descriptive epidemiology of total physical activity, muscle-strengthening exercises and sedentary behaviour among Australian adults—Results from the National Nutrition and Physical Activity Survey. BMC Public Health 2016, 16, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention State Indicator. Report on Physical Activity, 2014; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2014.
- Kalman, M.; Inchley, J.; Sigmundová, D.; Iannotti, R.J.; Tynjälä, J.A.; Hamrik, Z.; Haug, E.; Bucksch, J. Secular trends in moderate-to-vigorous physical activity in 32 countries from 2002 to 2010: A cross-national perspective. Eur. J. Public Health 2015, 25, 37–40. [Google Scholar] [CrossRef] [Green Version]
- Gonzalo-Almorox, E.; Urbanos-Garrido, R.M. Decomposing socio-economic inequalities in leisure-time physical inactivity: The case of Spanish children. Int. J. Equity Health 2016, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Wijtzes, A.I.; Jansen, W.; Bouthoorn, S.H.; Pot, N.; Hofman, A.; Jaddoe, V.W.V.; Raat, H. Social inequalities in young children’s sports participation and outdoor play. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Wiltshire, G. Inequalities in young-people’s physical activity: How can school-based interventions make more of a difference? In Proceedings of the 7th International Society for Physical Activity and Health Congress, London, UK, 15–17 October 2018. [Google Scholar]
- Schaefer, L.; Plotnikoff, R.C.; Majumdar, S.R.; Mollard, R.; Woo, M.; Sadman, R.; Rinaldi, R.L.; Boulé, N.; Torrance, B.; Ball, G.D.; et al. Outdoor Time Is Associated with Physical Activity, Sedentary Time, and Cardiorespiratory Fitness in Youth. J. Pediatr. 2014, 165, 516–521. [Google Scholar] [CrossRef]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U.; Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Paduano, S.; Greco, A.; Borsari, L.; Salvia, C.; Tancredi, S.; Pinca, J.; Midili, S.; Tripodi, A.; Borella, P.; Marchesi, I. Physical and Sedentary Activities and Childhood Overweight/Obesity: A Cross-Sectional Study among First-Year Children of Primary Schools in Modena, Italy. Int. J. Environ. Res. Public Health 2021, 18, 3221. [Google Scholar] [CrossRef]
- Atkin, A.J.; Sharp, S.J.; Corder, K.; van Sluijs, E.M.; International Children’s Accelerometry Database, C. Prevalence and correlates of screen time in youth: An international perspective. Am. J. Prev. Med. 2014, 47, 803–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larouche, R.; Garriguet, D.; Gunnell, K.E.; Goldfield, G.S.; Tremblay, M.S. Outdoor time, physical activity, sedentary time, and health indicators at ages 7 to 14: 2012/2013 Canadian Health Measures Survey. Health Rep. 2016, 27, 3–13. [Google Scholar] [PubMed]
- Troiano, R.P.; Stamatakis, E.; Bull, F.C. How can global physical activity surveillance adapt to evolving physical activity guidelines? Needs, challenges and future directions. Br. J. Sports Med. 2020, 54, 1468–1473. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: At a Glance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Aubert, S.; Barnes, J.D.; Abdeta, C.; Nader, P.A.; Adeniyi, A.F.; Aguilar-Farias, N.; Tenesaca, D.S.A.; Bhawra, J.; Brazo-Sayavera, J.; Cardon, G.; et al. Global Matrix 3.0 Physical Activity Report Card Grades for Children and Youth: Results and Analysis from 49 Countries. J. Phys. Act. Health 2018, 15, S251–S273. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Level of Physical Activity Required |
|---|---|
| Adults 18 –74-year-olds | Accumulate 3 or more days per week with a vigorous-intensity physical activity of at least 25 min per day; Or accumulate 5 or more days per week with a moderate-intensity physical activity of at least 30 min per day; Or accumulate 5 or more days per week with a moderate- to vigorous-intensity physical activity to reach a minimum of 600 METs per week. |
| Adolescents 11–17-year-olds | Accumulate at least 60 min of moderate- to vigorous-intensity physical activity daily; Or accumulate 5 or more times per week with a vigorous-intensity physical activity of at least 40 consecutive minutes. |
| Children 6–10-year-olds | For children at school during the week surveyed: Accumulate 5 or more days per week with physical activity (including active play in outdoor, organized sports, physical education and active transportation to get to school). For children on holiday during the week surveyed: Child considered “physically active” by his parents and 3 or more days per week with organized sports; Or child considered “physically active” by his parents and average daily time spent outside ≥90 min 1. |
| Men (n = 1169) | Women (n = 1513) | p 1 | |||
|---|---|---|---|---|---|
| % | 95%CI | % | 95%CI | ||
| Prevalence of physical activity(achievement of recommendations) | 70.6 | [67.0–73.9] | 52.7 | [49.3–56.1] | <0.001 |
| Age groups | |||||
| 18–39 years old | 69.1 | [61.7–75.5] | 50.3 | [43.6–57.0] | <0.001 |
| 40–54 years old | 70.8 | [64.9–76.0] | 49.4 | [43.7–55.1] | <0.001 |
| 55–74 years old | 71.8 | [67.0–73.9] | 57.8 | [52.6–62.9] | <0.001 |
| Education level | |||||
| <High school degree | 70.9 | [65.0–76.1] | 51.6 | [45.9–57.2] | <0.001 |
| High school degree | 69.7 | [60.9–77.2] | 54 | [46.9–60.9] | 0.006 |
| Bachelor’s degree | 74.6 | [67.4–80.6] | 50.2 | [43.6–56.8] | <0.001 |
| Master’s degree | 68.5 | [61.9–74.3] | 57.3 | [50.8–63.5] | 0.02 |
| Daily leisure screen time | |||||
| <3 h/day | 80.1 | [73.5–85.4] | 58.3 | [51.3–65.0] | <0.001 |
| ≥3 h/day | 68.3 | [64.2–72.1] | 51.3 | [47.4–55.2] | <0.001 |
| Prevalence of sedentary behaviors (daily leisure screen time ≥3 h/day) | 80.5 | [77.4–83.2] | 79.8 | [77.1–82.2] | 0.7 |
| Age groups | |||||
| 18–39 years old | 81.8 | [75.6–86.7] | 80 | [74.6–84.5] | 0.6 |
| 40–54 years old | 77.4 | [71.9–82.1] | 74.4 | [69.5–78.9] | 0.4 |
| 55–74 years old | 82.1 | [77.3–86.0] | 84.5 | [80.5–87.8] | 0.4 |
| Education level | |||||
| <High school degree | 86.3 | [81.6–89.9] | 85.3 | [80.9–88.7] | 0.7 |
| High school degree | 77.1 | [68.5–83.9] | 81.2 | [75.1–86.1] | 0.4 |
| Bachelor’s degree | 80.9 | [74.1–86.2] | 78.6 | [73.2–83.2] | 0.6 |
| Master’s degree | 69 | [62.8–74.5] | 62.1 | [55.8–68.1] | 0.1 |
| Recommendations on physical activity | |||||
| achieved | 77.8 | [73.9–81.3] | 77.6 | [73.9–81.0] | 0.9 |
| non-achieved | 86.8 | [82.1–90.4] | 82.2 | [78.2–85.6] | 0.1 |
| Boys (n = 643) | Girls (n = 638) | p 1 | |||
|---|---|---|---|---|---|
| % | 95%CI | % | 95%CI | ||
| Prevalence of physical activity (achievement of recommendations) | 50.7 | [45.1–56.3] | 33.3 | [28.4–38.6] | <0.001 |
| Age groups | |||||
| 6–10 years old | 69.7 | [61.1–77.1] | 55.5 | [47.0–63.7] | 0.02 |
| 11–14 years old | 33.7 | [26.0–42.4] | 20.2 | [14.3–27.7] | 0.01 |
| 15–17 years old | 40.1 | [28.0–53.6] | 15.7 | [9.7–24.4] | <0.001 |
| Parent education level | |||||
| <High school degree | 48.8 | [39.7–57.9] | 27.7 | [20.3–36.5] | 0.001 |
| High school degree | 47.6 | [35.8–59.7] | 35.8 | [24.3–49.2] | 0.2 |
| Bachelor’s degree | 56.9 | [47.0–66.3] | 36 | [27.6–45.3] | 0.003 |
| Master’s degree | 55.2 | [45.5–64.6] | 42.5 | [32.7–53.0] | 0.08 |
| Daily screen time | |||||
| <2 h/day | 70.3 | [58.2–80.1] | 46.7 | [36.3–57.3] | 0.004 |
| ≥2 h/day | 47.6 | [41.0–54.4] | 30.1 | [24.5–36.5] | <0.001 |
| Prevalence of sedentary behaviors (daily screen time ≥2 h/day) | 80.7 | [75.8–84.8] | 73.4 | [68.2–78.0] | 0.03 |
| Age groups | |||||
| 6–10 years old | 71.7 | [63.4–78.7] | 58.5 | [49.8–66.8] | 0.03 |
| 11–14 years old | 83.7 | [75.6–89.5] | 82.7 | [75.6–88.0] | 0.83 |
| 15–17 years old | 97.4 | [92.7–99.1] | 86.3 | [75.6–92.7] | 0.003 |
| Parent education level | |||||
| <High school degree | 85.1 | [76.3–90.9] | 79.1 | [70.1–85.9] | 0.28 |
| High school degree | 84.6 | [73.8–91.5] | 70.5 | [57.2–81.0] | 0.06 |
| Bachelor’s degree | 75 | [65.5–82.6] | 73.2 | [63.1–81.4] | 0.78 |
| Master’s degree | 69.4 | [60.0–77.4] | 59.6 | [48.7–69.6] | 0.16 |
| Recommendations on physical activity | |||||
| achieved | 73.9 | [66.2–80.3] | 64 | [54.7–72.5] | 0.089 |
| non-achieved | 88 | [82.2–92.1] | 78.3 | [72.1–83.5] | <0.014 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verdot, C.; Salanave, B.; Aubert, S.; Ramirez Varela, A.; Deschamps, V. Prevalence of Physical Activity and Sedentary Behaviors in the French Population: Results and Evolution between Two Cross-Sectional Population-Based Studies, 2006 and 2016. Int. J. Environ. Res. Public Health 2022, 19, 2164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042164
Verdot C, Salanave B, Aubert S, Ramirez Varela A, Deschamps V. Prevalence of Physical Activity and Sedentary Behaviors in the French Population: Results and Evolution between Two Cross-Sectional Population-Based Studies, 2006 and 2016. International Journal of Environmental Research and Public Health. 2022; 19(4):2164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042164
Chicago/Turabian StyleVerdot, Charlotte, Benoît Salanave, Salomé Aubert, Andréa Ramirez Varela, and Valérie Deschamps. 2022. "Prevalence of Physical Activity and Sedentary Behaviors in the French Population: Results and Evolution between Two Cross-Sectional Population-Based Studies, 2006 and 2016" International Journal of Environmental Research and Public Health 19, no. 4: 2164. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042164