
Study of a Quasi-Experimental Trial to Compare Two Models of Home Care for the Elderly in an Urban Primary Care Setting in Spain: Results of Intermediate Analysis


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Thical Aspects
2.2. Selection Criteria
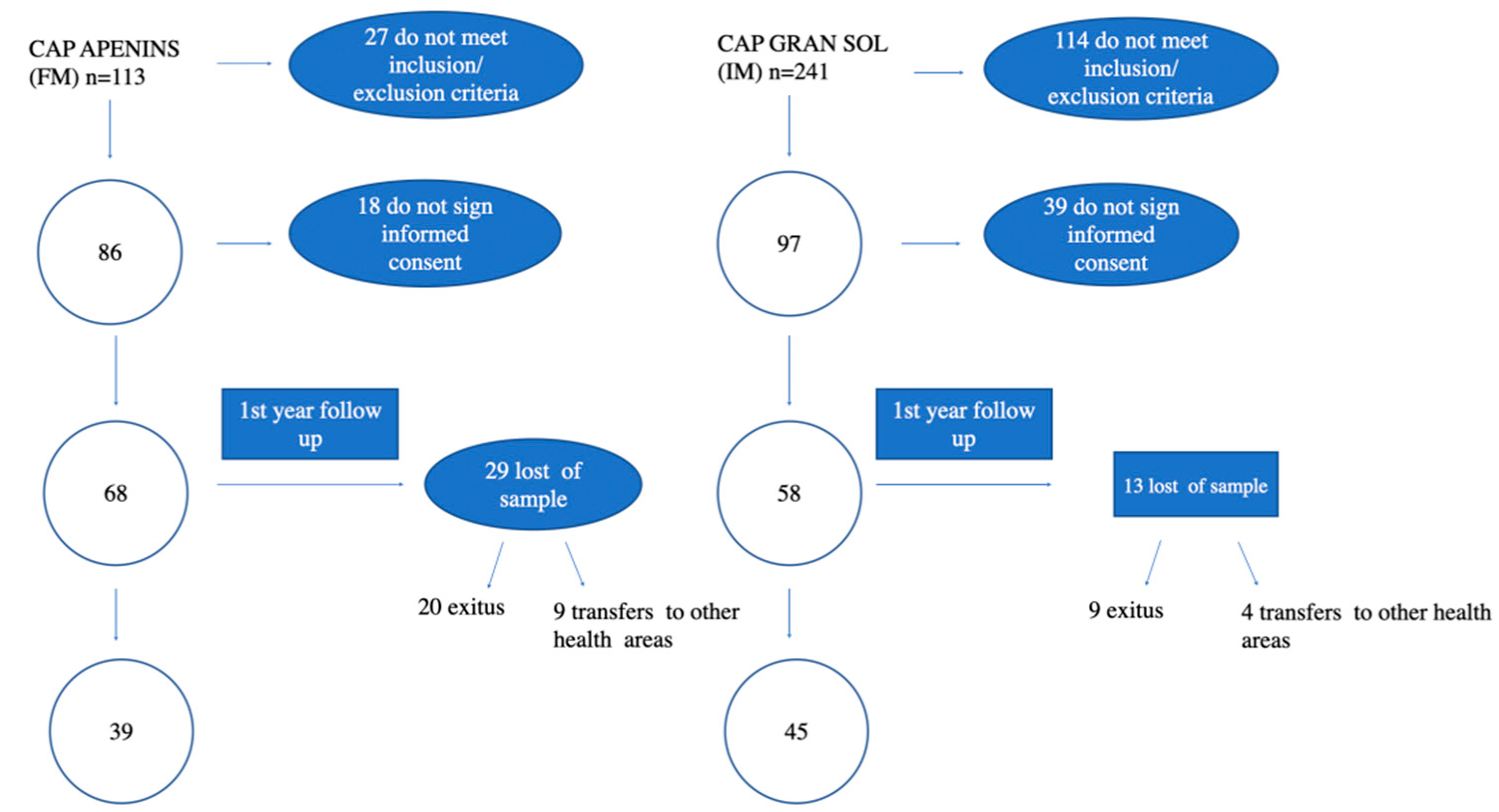
2.3. Patient Recruitment
2.4. Study Conduct
2.5. Endpoints and Variables
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Santaeugènia, S.J.; Contel, J.C.; Vela, E.; Cleries, M.; Amil, P.; Melendo-Azuela, E.M.; Gil-Sánchez, E.; Mir, V.; Amblàs-Novellas, J. Characteristics and Service Utilization by Complex Chronic and Advanced Chronic Patients in Catalonia: A Retrospective SevenYear Cohort-Based Study of an Implemented Chronic Care Program. Int. J. Environ. Res. Public Health 2021, 18, 9473. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.L.; Starfield, B.; Anderson, G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch. Intern. Med. 2002, 162, 2269–2276. [Google Scholar] [CrossRef] [PubMed]
- Mitnitski, A.B.; Rutenberg, A.D.; Farrell, S.; Rockwood, K. Aging, frailty, and complex networks. Biogerontology 2017, 18, 433–446. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística. Proyecciones de la Población de España a Largo Plazo (2020–2070); Ministerio de Asuntos Económicos y Transformación Digital: Madrid, Spain, 2019. [Google Scholar]
- Ministerio de Sanidad y Política Social. Unidad de Pacientes Pluripatológicos Estándares y Recomendaciones. Minist Sanid y Política Soc. 2009, 11–12. [Google Scholar]
- Gené Badia, J.; Borràs Santos, A.; Contel Segura, J.C.; Ascaso Terén, C.; González Ortega, M.; Gallo De Puelles, P. Factors associated with hospitalization in a cohort of elderly patients included in a home care program. Med. Clin. 2012, 139, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Contel, J.C. Impacto de la atención domiciliaria preventiva en el ingreso en centros sociosanitarios, estado funcional y mortalidad. FMC 2002, 9, 459. [Google Scholar]
- Counsell, S.R.; Callahan, C.M.; Clark, D.O.; Tu, W.; Buttar, A.B.; Stump, T.E.; Ricketts, G.D. Geriatric care management for low-income seniors: A randomized controlled trial. JAMA 2007, 298, 2623–2633. [Google Scholar] [CrossRef]
- Peterson, K.; Helfand, M.; Humphrey, L.; Christensen, V.; Carson, S. Evidence Brief: Effectiveness of Intensive Primary Care Programs; 2011-Created: February 2013; Department of Veterans Affairs (US): Washington, DC, USA, 2013.
- Vila, A.; Villegas, E.; Cruanyes, J.; Delgado, R.; Sabaté, R.A.; Ortega, J.; Araguás, C.; Humet, C. Cost-Effectiveness of a Barcelona Home Care Program for individuals with Multimorbility. J. Am. Geriatr. Soc. 2015, 63, 1017–1024. [Google Scholar] [CrossRef]
- Beswick, A.D.; Rees, K.; Dieppe, P.; Ayis, S.; Gooberman-Hill, R.; Horwood, J.; Ebrahim, S. Complex interventions to improve physical function and maintain independent living in elderly people: A systematic review and meta-analysis. Lancet 2008, 371, 725–735. [Google Scholar] [CrossRef] [Green Version]
- Mayo-Wilson, E.; Grant, S.; Burton, J.; Parsons, A.; Underhill, K.; Montgomery, P. Preventive home visits for mortality, morbidity and Institutionalitation in older Adults: A Systematic Rewiew and meta- Analysis. PLoS ONE 2014, 9, E89257. [Google Scholar] [CrossRef]
- Fusté, J.; Cànovas, J.; Oliete, C.; Fuertes, O. Análisis Comparado de los Modelos de Atención Domiciliaria Sanitarios y Sociales del Sistema Nacional de Salud y del Sistema de Atención a la Dependencia. 29 de Noviembre de 2019 Fundació Unió. Catalana d’hospitals. Available online: https://www.uch.cat/documents/anlisis-comparado-de-los-modelos-de-atencin-domiciliaria-fase-i-i-ii.pdf (accessed on 23 December 2021).
- Gorina, M.; Limonero, J.T.; Peñart, X.; Jiménez, J.; Gasso, J. Comparación de la satisfacción de los usuarios de atención domiciliaria: Modelo integrado vs. modelo dispensarizado. Aten. Primaria 2014, 46, 276–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yolanda, A.V.; Antonio, S.R.; Marta, P.A.; Julia, F. Relación de la Calidad de vida con Diferentes Modelos de Atención Domiciliaria en Enfermos Oncológicos Terminales de un Área Sanitaria de Madrid. Rev. Esp. Salud Publica 2003, 77, 567–579. [Google Scholar]
- Morales Asencio, J.M. Efectividad de un Nuevo Modelo de Atención Domiciliaria en Andalucía para Poblaciones Vulnerables en atención Primaria. Estudio Quasi-Experimental, Controlado, Multicéntrico. Doctoral Thesis, University of Malaga, Málaga, Spain, 9 June 2006. Available online: https://www.educacion.gob.es/teseo/mostrarRef.do?ref=39392 (accessed on 2 February 2022).
- Phyllis Pinnegar, H.; Paredes Millan, M.K.; Plaza Cerrato, L.; Palomino Español, E.; Baena Diez, J.M. Estudio comparativo de dos modelos de atención domiciliaria: Modelo integrado frente a modelo dispesarizado. Comunicaciones y ponencias semFYC: 2022; Comunicaciones: Resultados de investigación. In Proceedings of the XXXVIII Congreso de la semFYC, Barcelona, Spain, 10–12 May 2018. ISSN: 2339-9333. [Google Scholar]
- Programa de Millora de L’atenció al Domicili des de L’atenció Primària de Salut. Institut Català de la Salut. Generalitat de Catalunya Departament de Salut. April 2010. Available online: http://ics.gencat.cat/web/.content/documents/assistencia/protocols/atdom.pdf (accessed on 27 December 2021).
- Cegri Lombardo, F.; Aranzana Martínez, A. Atención domiciliaria: Caminando hacia la excelencia. Aten. Primaria 2007, 39, 34. [Google Scholar] [CrossRef] [Green Version]
- Burgos Diez, C.; Sequera Requero, R.; Tarazona-Santabalbina, F.J.; Contel-Segura, J.C.; Monzó Planella, M.; Santaeugènia-González, S.J. Study protocol of a quasi-experimental trial to compare two models of home care for older people in the primary setting. BMC Geriatr. 2020, 20, 101. [Google Scholar] [CrossRef] [PubMed]
- Monterde, D.; Vela, E.; Clèries, M. Grupo colaborativo GMA. Los grupos de morbilidad ajustados: Nuevo agrupador de morbilidad poblacional de utilidad en el ámbito de la atención primaria. Aten. Primaria 2016, 48, 674–682. [Google Scholar] [CrossRef] [Green Version]
- Spanish Society of Family and Community Medicine (SEMFYC). Program of preventive activities for Health promotion (PAPPS) Actualización 2020. Aten. Primaria 2020, 52, 1–172. [Google Scholar]
- Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- The EuroQol Group. EuroQol, a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Instrumento de Evaluación de la Experiencia del Paciente Crónico. Available online: www.iexpac.org.www.iemac.org/iexpac (accessed on 23 December 2021).
- Zarit, S.H.; Reever, K.E.; Bach-Peterson, J. Relatives of the impaired elderly: Correlates of feeling of burden. Gerontologist 1980, 20, 649–654. [Google Scholar] [CrossRef] [Green Version]
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The triple aim: Care, health, and cost. Health Aff. (Millwood) 2008, 27, 759–769. [Google Scholar] [CrossRef] [Green Version]
- Bases para un Modelo Catalán de Atención a las Personas con Necesidades Complejas. Conceptualización e Introducción a los Elementos Operativos. (Versión 6.0 del 27 de marzo de 2017). Programa de Prevenció i Atenció a la Cronicitat. Generalitat de Catalunya. 2017. Available online: https://scientiasalut.gencat.cat/bitstream/handle/11351/3305/bases_modelo_catalan_atencion_personas_necesidades_complejas_2017_cas.pdf?sequence=5&isAllowed=y. (accessed on 23 December 2021).
- Fi, M.; Dw, B. Functional evaluation: The barthel index. Md. State Med. J. 1965, 14, 56–61. [Google Scholar]
- Braden, B.; Bergstrom, N. A conceptual schema for the study of the etiology of pressure sores. Rehabil. Nurs. 1987, 12, 8–12. [Google Scholar] [CrossRef] [PubMed]
- González, D.C.; Caicoya, A.M.; Sánchez, A.F.; García, V.A.; González, J.G.; Palacios, E.D.; García, A.S. Evaluación de la fiabilidad y validez de una escala de valoración social en el anciano. Aten. Primaria 1999, 23, 434–440. [Google Scholar]
- Institut Català de la Salut. El Treball Social Sanitari en l’atenció al Pacient Crònic. [Internet]. 2013. Available online: https://treballsocialsanitariics.files.wordpress.com/2015/11/el-treball-social-sanitari-en-latencic3b3-al-pacientcrc3b2nic-document-de-metodologia-deprocc3a9s-2013-ics.pdf (accessed on 3 March 2020).
- Stuck, A.E.; Egger, M.; Hammer, A.; Minder, C.E.; Beck, J.C. Home Visits to Prevent Nursing Home Admission and Functional Decline in Elderly People: Systematic Review and Meta-regression Analysis. J. Am. Med. Assoc. 2002, 287, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.diba.cat/es/web/respir/respir-residencial-per-a-gent-gran (accessed on 23 December 2021).
- Vela, E.; Clèries, M.; Vella, V.A.; Adroher, C.; García-Altés, A. Análisis poblacional del gasto en servicios sanitarios en Cataluña (España): ¿qué y quién consume más recursos? [Population-based analysis of the Healthcare expenditure in Catalonia (Spain): What and who consumes more resources?]. Gac. Sanit. 2019, 33, 24–31. [Google Scholar] [CrossRef]
- Coderch, J.; Sánchez-Pérez, I.; Ibern, P.; Carreras, M.; Pérez-Berruezo, X.; Inoriza, J.M. Predicción del riesgo individual de alto coste sanitario para la identificación de pacientes crónicos complejos. Gac. Sanit. 2014, 28, 292–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochman, M.; Asch, S.M. Disruptive Models in Primary Care: Caring for High-Needs, High-Cost Populations. J. Gen. Intern. Med. 2017, 32, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Espaulella Panicot, J.; Molist Brunet, N.; Sevilla Sánchez, D.; González-Bueno, J.; Amblàs Novellas, J.; Sola Bonada, N.; Codina Jané, C. Modelo de prescripción centrado en la persona para mejorar la adecuación y adherencia terapéutica en los pacientes con multimorbilidad. Rev. Española Geriatría Gerontol. 2017, 52, 278–281. [Google Scholar] [CrossRef]
- Amblàs-Novellas, J.; Santaeugènia, S.J.; Vela, E.; Clèries, M.; Contel, J.C. What lies beneath: A retrospective, population-based cohort study investigating clinical and resource-use characteristics of institutionalized older people in Catalonia. BMC Geriatr. 2020, 20, 2–8. [Google Scholar] [CrossRef]
- Hogg, W.; Lemelin, J.; Dahrouge, S.; Liddy, C.; Armstrong, C.D.; Legault, F.; Dalziel, B.; Zhang, W. Randomized controlled trial of anticipatory and preventive multidisciplinary team care: For complex patients in a community-based primary care setting. Can. Fam. Physician 2009, 55, e76–e85. [Google Scholar]
- Manterola, C.; Otzen, T. Los Sesgos en Investigación Clínica. Int. J. Morphol. 2015, 201, 1156–1164. Available online: http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0717-95022015000300056&lng=es (accessed on 9 February 2022). [CrossRef] [Green Version]


{kind=link}
| Characteristics of the Healthcare Team | Integrated HC | Functional HC |
|---|---|---|
| Team composition | Nurse and family physician | Nurse and family physician. |
| Team function | The same healthcare team provides HC and manages patients in the primary health care centre independently of their care needs (prevention, health promotion, patients with complex needs, patients in HC program or patients at end of life). | The healthcare team is dedicated exclusively to HC. |
| Interprofessional communication | Healthcare professionals are part of the healthcare team regularly managing patients in the primary health care centre. | Although not managing patients in the primary health care centre, the HC team is part of the health care staff of the centre and their members participate in the centre meetings as specialists |
| Training | Regular training of family doctors, including regular stays at mental health and geriatric units. Regular training of nurses. | Regular training of family doctors, including regular stays at mental health and geriatric units. Nursing staff and doctor receives additional training regarding the management of chronic patients, fragility, and palliative care. Continuous updates. |
| Type of professional in each visit | Nurse, family doctor or both. | Nurse, family doctor or both. |
| Preventive visits | Visits of nursing staff scheduled based on the monitoring requirements of each disease as established by local guidelines. Visits of physician scheduled at physician’s discretion based on the disease progression and clinical status of patients. | Visits of nursing staff scheduled based on the monitoring requirements of each disease as established by local guidelines. Visits of physician scheduled at physician’s discretion based on the disease progression and clinical status of patients. |
| Dedication to the type of care activity | 90% Care at the health centre, 10% at home (depending on the organisation of the centres). | 100% Home care |
| Non-urgent acute visits | The patient calls the centre and the physician schedules the visits at home in a deferred way, according to agenda. | During working hours, the patient directly contacts the physician of the HC team. Outside working hours: the patient calls the centre and the physician available at that moment (not always the one regularly visiting the patient at the primary health care centre) visits the patient at home. |
| Urgent visits | The patient calls the PHCC and a doctor from the centre, who is on call, sees him/her (this may not be the patient’s usual doctor). | The patient calls the HC team until 15:00. From 15:00 to 20:00, the patient calls the PHCC and a doctor from the centre, who is on call, sees him/her (this may not be the patient’s usual doctor). |
| Financial approach | All visits are fully covered by the public health system. | All visits are fully covered by the public health system. |
| Integrated HC (PHCC Gran Sol) | Functional HC (PHCC Apenins) | p | |
|---|---|---|---|
| Location | Badalona, Catalonia, Spain | Badalona, Catalonia, Spain | |
| Professional profile | MDs and nurses specialized in family medicine | MDs and nurses specialized in family medicine | |
| Reference population b, No. | 19.442 | 19.043 | |
| Over-Aging index c,% | 11% | 9.2% | <0.001 |
| Foreign population d, n (%) | 3499 (17.9%) | 3046 (15.9%) | <0.001 |
| ≥65 years old, n (%) | 3480 (17.9%) | 2970 (15.6%) | <0.001 |
| AMG, adjusted indicator (IC 95%) | 1.189 (1.173–1.206) | 1.178 (1.161–1.195) | – |
| Mortality, annual (%) | 7 | 5.7 | 0.143 |
| IT application | eCAP | eCAP |
| Apenins | Gran Sol | p | |
|---|---|---|---|
| (Functional Model) | (Integrated Model) | ||
| n = 68 | n = 58 | ||
| Average age | 86.66 (7.6) | 87.2 (6.7) | 0.39 |
| Age %: | 0.457 | ||
| Group 1 (between 65 and 74) | 5.9 | 3.4 | |
| Group 2 (between 75 and 84) | 33.8 | 25.9 | |
| Group 3 (>=85 years) | 60.3 | 70.7 | |
| Sex: (%) | |||
| Male | 23.5 | 27.6 | 0.602 |
| Female | 76.5 | 72.4 | |
| Typologies of patients in the programme ATDOM 2 (%): | |||
| Patients with non-complex medical problems | 5.9 | 10.3 | 0.365 |
| Chronically complex patient (CCP 3) | 80.9 | 82.8 | |
| Chronically ill patients with advanced disease (MACA 4) | 13.2 | 6.9 | |
| ICIP 5 realizado n (%) | 45 (66.2) | 36 (62.1) | 0.632 |
| ICIP with PDA 6 n (%) | 39 (57.4) | 32 (55.2) | 0.806 |
| Adjusted Morbidity Groups (AMG 7) n (%) | 0.011 | ||
| Group 1 (1,2,3) | 6 (8.8) | 15 (25.9) | |
| Group 2 (4,5) | 62 (91.2) | 43 (74.1) | |
| Degree of dependency (average) | 0.011 | ||
| 0–1 | 41 (60.3) | 47 (81) | |
| 2–3 | 27 (39.7) | 11 (18.9) | |
| TIRS 8 n (%) | 6 (11.5) | 12 (26.6) | 0.056 |
| No falls n (%) | 63 (92.6) | 53 (91.3) | 0.957 |
| No presence of decubitus ulcers n (%) | 62 (91) | 52 (89) | 0.475 |
| Barthel | 55.15 (25,8) | 60.5 (21,4) | 0.262 |
| Pfeiffer | 3.94 (3.2) | 2.83 (3.0) | 0.078 |
| Braden | 17.75 (2.6) | 17.64 (2.4) | 0.824 |
| Private caregiver No. (%) | 22 (32.4) | 2 (3.4) | 0 |
| Euroqol (subjective assessment) | 4.75 (2.32) | 4.35 (1.87) | 0.291 |
| IEXPAC 9 | 5.85 (1.69) | 5.98 (1.17) | 0.004 |
| Caregiver overburden (Zarit) | 58.08 (17.1) | 29.27 (27.8) | 0.001 |
| Apenins (Functional Model) n = 68 | Gran Sol (Integrated Model) n = 58 | p | |
|---|---|---|---|
| Online consultations with a hospital specialist No. (%patients) | 13 (19.1) | 4 (6.9) | 0.045 |
| In-person referrals to hospital specialists No. (%patients) | 32 (47.1) | 25 (43.1) | 0.657 |
| ECG 1 (%patients) | 28 (41.2) | 0.00 (0.00) | 0.000 |
| Conventional XR 2 requested No. (%patients) | 44.2% | 13.7% | 0.053 |
| Ultrasound scans requested No. (%patients) | 16.1% | 8.6% | 0.445 |
| CAT 3 requested No.(%patients) | 22% | 3.4% | 0.021 |
| Blood and urine tests (mean + STD 4) | 2.9 (3.9) | 1.6 (1.5) | 0.020 |
| Prescribed drugs (mean + STD) | 10.05 (3.5) | 9.81 (5.13) | 0.757 |
| Online consultations +G.P. 5 BCU 6 (mean + STD) | 9.90 (6.27) | 9.07 (6.74) | 0.477 |
| In-person consultations G.P. BCU (mean + STD) | 6.25 (5.77) | 3.98 (3.41) | 0.008 |
| In-person consultations G.P. non- BCU (mean + STD) | 2.81 (2.55) | 0.57 (1.65) | 0.000 |
| Online consultations NUR 7 BCU (mean + STD) | 1.99 (3.23) | 4.90 (5.16) | 0.000 |
| In-person consultations NUR BCU (mean + STD) | 7.35 (9.50) | 4.33 (5.47) | 0.028 |
| In-person consultations NUR non- BCU (mean + STD) | 3.24 (9.35) | 5.33 (10.35) | 0.238 |
| MES 8 activation No. (%) | 34 (50) | 50 (86.2) | 0.055 |
| Admissions to private nursing homes No. (%) | 3 (4.4) | 15 (25.8) | 0.003 |
| Apenins (Functional Model) n = 68 | Gran Sol (Integrated Model) n = 58 | p | |
|---|---|---|---|
| Respite care (up to 30 days) (Respir 1) | 19 (27.9) | 7 (12.1) | 0.028 |
| Teleassistance | 60 (88.2) | 54 (93.1) | 0.353 |
| HHS 2 | 53 (77.9) | 50 (86.2) | 0.231 |
| Admissions to hospital ward (No.) | 0.71 (1.24) | 1.35 (1.90) | 0.031 |
| A&E 3 admissions (No.) | 2.01 (2.12) | 3.53 (3.59) | 0.006 |
| Admission in Intermediate Care Hospital. (No.) | 0.21 (0.47) | 0.12 (0.32) | 0.239 |
| No. of cumulative days of admission (on ward) per year. | 5.43 (10.92) | 14.69 (20.90) | 0.003 |
| No. Admission in Hospital at home | 0.01 (0.12) | 0.19 (0.68) | 0.060 |
| No. Admission in PADES 4 | 0.03 (0.17) | 0.14 (0.34) | 0.033 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burgos Díez, C.; Sequera Requero, R.M.; Ferrer Costa, J.; Tarazona-Santabalbina, F.J.; Monzó Planella, M.; Cunha-Pérez, C.; Santaeugènia González, S.J.; Grupo ATDOM. Study of a Quasi-Experimental Trial to Compare Two Models of Home Care for the Elderly in an Urban Primary Care Setting in Spain: Results of Intermediate Analysis. Int. J. Environ. Res. Public Health 2022, 19, 2329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042329
Burgos Díez C, Sequera Requero RM, Ferrer Costa J, Tarazona-Santabalbina FJ, Monzó Planella M, Cunha-Pérez C, Santaeugènia González SJ, Grupo ATDOM. Study of a Quasi-Experimental Trial to Compare Two Models of Home Care for the Elderly in an Urban Primary Care Setting in Spain: Results of Intermediate Analysis. International Journal of Environmental Research and Public Health. 2022; 19(4):2329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042329
Chicago/Turabian StyleBurgos Díez, Carolina, Rosa Maria Sequera Requero, Jose Ferrer Costa, Francisco José Tarazona-Santabalbina, Marià Monzó Planella, Cristina Cunha-Pérez, Sebastià Josep Santaeugènia González, and Grupo ATDOM. 2022. "Study of a Quasi-Experimental Trial to Compare Two Models of Home Care for the Elderly in an Urban Primary Care Setting in Spain: Results of Intermediate Analysis" International Journal of Environmental Research and Public Health 19, no. 4: 2329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042329