
Clinical Manifestations, Diagnosis and Management of Synovial Fistula Associated Lateral Ankle Sprain or Instability: A Retrospective Study of 19 Surgically Confirmed Patients


Abstract
:1. Introduction
2. Materials and Methods
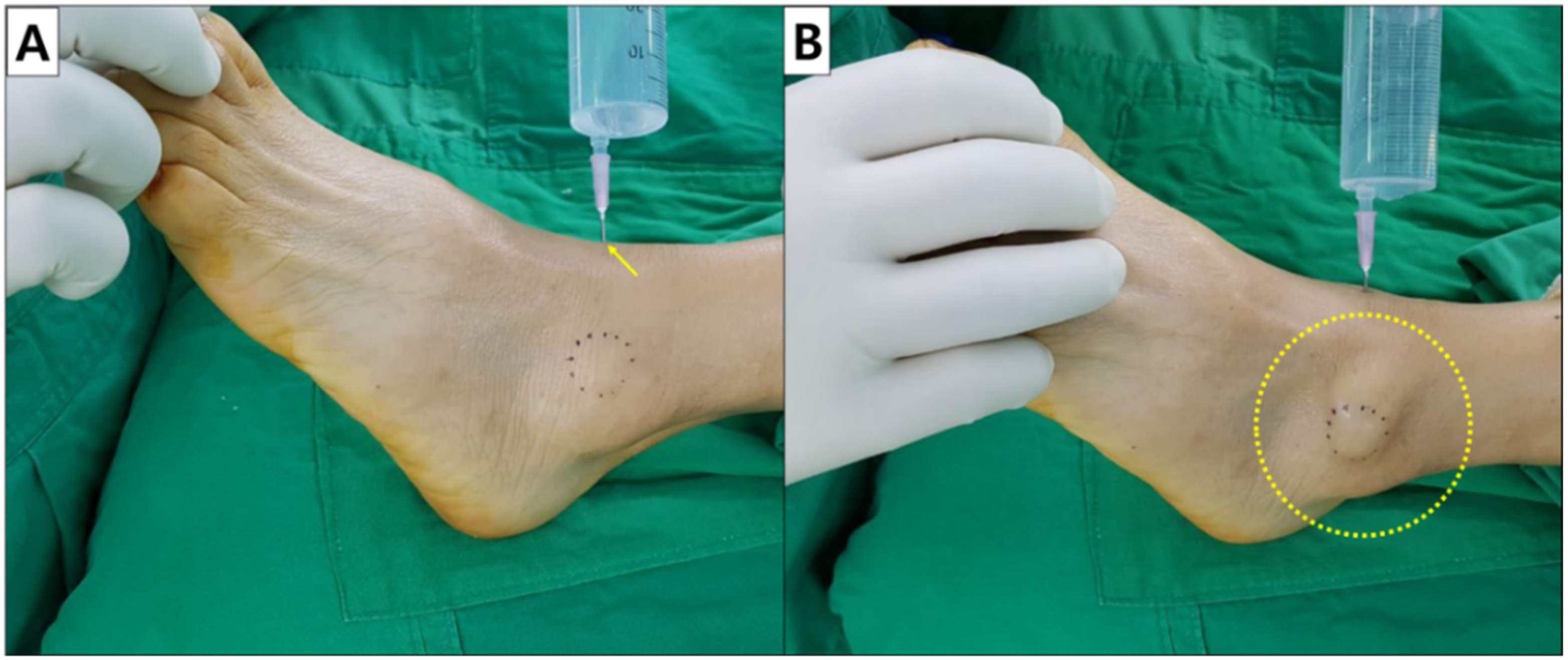
2.1. Surgical Technique
2.2. Postoperative Protocol
3. Results
Illustrative Case
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heredia, J.D.; Iban, M.A.R.; Gutiérrez, R.C.; Diaz, R.R.; del Val, I.C.M.; Merino, L.T. Early Postoperative Transtibial Articular Fistula Formation after Anterior Cruciate Ligament Reconstruction: A Review of Three Cases. Arch. Orthop. Trauma Surg. 2014, 134, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Proffer, D.S.; Drez, D.; Daus, G.P. Synovial Fistula of the Knee: A Complication of Arthroscopy. Arthrosc. J. Arthrosc. Relat. Surg. 1991, 7, 98–100. [Google Scholar] [CrossRef]
- Richards, R.S.; Curl, L.A.; Moorman, C.T.; Mallon, W.J. Sterile Synovio-Cutaneous Fistula: A Potential Complication of Repair of Large and Massive Rotator Cuff Tears. J. Shoulder Elb. Surg. 2006, 15, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Shirley, D.S.; Mullet, H.; Stanley, J.K. Extensor Tendon Sheath Fistula Formation as a Complication of Wrist Arthroscopy. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 1311–1312. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.A.; Wright, T.W. Synovial Cutaneous Fistula of the Shoulder after Failed Rotator Cuff Repair. Orthopedics 1999, 22, 1095–1097. [Google Scholar] [CrossRef]
- Van Kampen, A.; Hinton, F. Diagnosis and Treatment of Postsurgical Synovial Fistula of the Knee. J. Knee Surg. 2011, 24, 295–298. [Google Scholar] [CrossRef]
- Yiannakopoulos, C.K. Diagnosis and Treatment of Postarthroscopic Synovial Knee Fistulae–a Report of Four Cases and Review of the Literature. J. Knee Surg. 2007, 20, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Grainger, A.; Tirman, P.F.J.; Elliott, J.M.; Kingzett-Taylor, A.; Steinbach, L.S.; Genant, H.K. Mr Anatomy of the Subcoracoid Bursa and the Association of Subcoracoid Effusion with Tears of the Anterior Rotator Cuff and the Rotator Interval. Am. J. Roentgenol. 2000, 174, 1377–1380. [Google Scholar] [CrossRef]
- Rauschning, W. Anatomy and Function of the Communication between Knee Joint and Popliteal Bursae. Ann. Rheum. Dis. 1980, 39, 354–358. [Google Scholar] [CrossRef] [Green Version]
- Steinbach, L.S.; Schneider, R.; Goldman, A.B.; Kazam, E.; Ranawat, C.S.; Ghelman, B. Bursae and Abscess Cavities Communicating with the Hip. Diagnosis Using Arthrography and Ct. Radiology 1985, 156, 303–307. [Google Scholar] [CrossRef]
- Jang, H.-S.; Choi, H.-J. Surgery for Synovial Fistula after Excision of the Lateral Malleolar Bursitis of the Ankle: A Case Report. J. Korean Foot Ankle Soc. 2015, 19, 118–121. [Google Scholar] [CrossRef] [Green Version]
- Ji, J.H.; Kim, W.Y.; Lee, Y.S.; Park, S.-E.; Ra, K.-H.; Kwon, O.-H. Secondary Septic Arthritis Due to Lateral Malleolar Bursitis—A Case Report. J. Korean Foot Ankle Soc. 2006, 10, 274–278. [Google Scholar]
- Lee, H.W.; Yang, I.; Liu, Y.; Lee, J.-H.; Kim, H.N. Saline Load Test and Quilting Sutures to Treat Intractable Lateral Malleolar Bursitis. J. Foot Ankle Surg. 2021, 60, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Kannus, P.; Renström, P. Treatment for Acute Tears of the Lateral Ligaments of the Ankle. Operation, Cast, or Early Controlled Mobilization. J. Bone Jt. Surg. 1991, 73, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Franson, J.; Baravarian, B. Lateral Ankle Triad: The Triple Injury of Ankle Synovitis, Lateral Ankle Instability, and Peroneal Tendon Tear. Clin. Podiatr. Med. Surg. 2011, 28, 105–115. [Google Scholar] [CrossRef]
- Navarro-Flores, E.; Losa-Iglesias, M.E.; Becerro-De-Bengoa-Vallejo, R.; Lopez-Lopez, D.; Vilar-Fernandez, J.M.; Palomo-Lopez, P.; Calvo-Lobo, C. Transcultural Adaptation and Validation of the Spanish Bristol Foot Score (Bfs-S). Aging Dis. 2018, 9, 861–868. [Google Scholar] [CrossRef] [Green Version]
- Hertel, J. Functional Anatomy, Pathomechanics, and Pathophysiology of Lateral Ankle Instability. J. Athl. Train. 2002, 37, 364. [Google Scholar]
- Me, M.A. Treatment of Chronic Recurrent Synovial Fistulae with Myofascial Flaps. Br. J. Plast. Surg. 1993, 46, 303–306. [Google Scholar]
- Bariteau, J.T.; Blankenhorn, B.D.; DiGiovanni, C.W. Evaluation of Saline Load Test for Simulated Traumatic Arthrotomies of the Ankle. Injury 2013, 44, 1498–1501. [Google Scholar] [CrossRef]
- Lee, K.M.; Chung, C.Y.; Kwon, S.S.; Sung, K.H.; Lee, S.Y.; Won, S.H.; Lee, D.J.; Lee, S.C.; Park, M.S. Transcultural Adaptation and Testing Psychometric Properties of the Korean Version of the Foot and Ankle Outcome Score (Faos). Clin. Rheumatol. 2013, 32, 1443–1450. [Google Scholar] [CrossRef]
- Avci, S.; Şayli, U. Lateral Premalleolar Bursitis as a Result of Sitting on the Foot. Foot Ankle Int. 2001, 22, 64–66. [Google Scholar] [CrossRef] [PubMed]
- Robertson, B.; Haywood, I.R. “Floor Layers Foot”—An Occupational Bursa. J. R. Army Med. Corps. 1983, 129, 48–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, M.; Amado, P.; Babulal, J. Ankle Instability—Review and New Trends. J. Orthop. Trauma Rehabil. 2021, 28, 22104917211035552. [Google Scholar] [CrossRef]
- Lee, W.-C.; Kim, J.-H.; Song, J.-K.; Moon, J.-S. Fistula of the Ankle: A Complication of Ankle Sprain. J. Korean Foot Ankle Soc. 2002, 6, 261–264. [Google Scholar]
- Naito, M.; Matsumoto, T.; Chang, S.H.; Ikegami, M.; Hirose, J.; Tanaka, S. Recalcitrant Lateral Premalleolar Bursitis of the Ankle Associated with Lateral Ankle Instability. Case Rep. Orthop. 2017, 2017, 4854812. [Google Scholar] [CrossRef] [Green Version]
- Tonogai, I.; Sairyo, K. A Case of Ankle Osteoarthritis Associated with Lateral Premalleolar Bursitis Caused by Chronic Ankle Instability. Int. J. Surg. Case Rep. 2021, 80, 105671. [Google Scholar] [CrossRef]
- Bohl, D.D.; Frank, R.M.; Hamid, K.S.; Holmes, G.B., Jr.; Lin, J.; Lee, S. Sensitivity of the Saline Load Test for Traumatic Arthrotomy of the Ankle with Ankle Arthroscopy Simulation. Foot Ankle Int. 2018, 39, 736–740. [Google Scholar] [CrossRef]
- Park, C.H.; Ryu, S.M.; Park, J.W. Unhealed Wound of the Lower Leg Due to Synovial Fistula of the Ankle Joint. J. Korean Foot Ankle Soc. 2017, 21, 113–116. [Google Scholar] [CrossRef] [Green Version]
- Okazaki, K.; Miyagi, S.; Tokunaga, J. Anatomic Reconstruction of the Lateral Ligament of the Ankle Using a Periosteal Flap from the Fibula. Tech. Foot Ankle Surg. 2005, 4, 98–103. [Google Scholar] [CrossRef]
- Navarro-Flores, E.; Losa-Iglesias, M.E.; Becerro-De-Bengoa-Vallejo, R.; Reina-Bueno, M.; López-López, D.; Romero-Morales, C.; Palomo-López, P.; Calvo-Lobo, C. Cross-Cultural Adaptation, Translation, and Validation of the Spanish Foot and Ankle Outcome Score Questionnaire. Int. Wound J. 2020, 17, 1384–1390. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age, yr | Sex | Time to Visitafter Trauma, mo | Saline Load Test | MRI | Bursitis (Location/SF Communication) | Surgical Procedure | FAOS | Recurrence | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| +/− | ATFL | CFL | |||||||||
| 1 | 59 | F | 3 | Positive | + | Complete tear | Intact | + (LM/−) | P | 80.13 | − |
| 2 | 42 | F | 24 | Positive | + | Partial tear | Partial tear | − (−/−) | C | 86.75 | − |
| 3 | 70 | M | 3 | Positive | − | + (LM/−) | P | 78.53 | − | ||
| 4 | 77 | M | 3 | Positive | − | + (PM/+) | C | 77.40 | − | ||
| 5 | 75 | M | 3 | Positive | + | Complete tear | Partial tear | + (LM/+) | C | 83.47 | − |
| 6 | 39 | F | 3 | Positive | + | Partial tear | Intact | + (PM/+) | C | 92.30 | − |
| 7 | 62 | F | 4 | Positive | + | Partial tear | Intact | + (PM/+) | P | 90.65 | − |
| 8 | 59 | M | 8 | Positive | − | − (−/−) | C | 96.74 | − | ||
| 9 | 60 | F | 12 | Positive | + | Partial tear | Partial tear | − (−/−) | C | 94.88 | − |
| 10 | 82 | F | 3 | Positive | − | − (−/−) | P | 98.15 | − | ||
| 11 | 74 | M | 6 | Positive | − | + (PM/+) | C | 80.80 | − | ||
| 12 | 78 | F | 24 | Positive | + | Complete tear | Intact | + (PM/+) | P | 77.40 | − |
| 13 | 52 | F | 3 | Positive | + | Complete tear | Partial tear | − (−/−) | P | 94.88 | − |
| 14 | 42 | M | 24 | Positive | + | Partial tear | Intact | + (PM/+) | Initial: C Revision: P | 93.36 | + |
| 15 | 67 | F | 24 | Positive | + | Partial tear | Intact | + (PM/+) | C | 92.37 | − |
| 16 | 40 | F | 84 | Positive | + | Complete tear | Partial tear | − (−/−) | P | 86.77 | − |
| 17 | 55 | F | 6 | Positive | + | Partial tear | Partial tear | − (−/−) | C | 82.47 | − |
| 18 | 34 | M | 6 | Positive | - | + (PM/-) | C | 90.07 | − | ||
| 19 | 32 | M | 3 | Positive | + | Complete tear | Partial tear | − (−/−) | C | 88.38 | − |
| Mean | 57.8 | 12.9 | 87.65 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Shim, B.-J.; Yang, J.-S.; Bat-Ulzii, A.; Cho, J. Clinical Manifestations, Diagnosis and Management of Synovial Fistula Associated Lateral Ankle Sprain or Instability: A Retrospective Study of 19 Surgically Confirmed Patients. Int. J. Environ. Res. Public Health 2022, 19, 2428. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042428
Kim J, Shim B-J, Yang J-S, Bat-Ulzii A, Cho J. Clinical Manifestations, Diagnosis and Management of Synovial Fistula Associated Lateral Ankle Sprain or Instability: A Retrospective Study of 19 Surgically Confirmed Patients. International Journal of Environmental Research and Public Health. 2022; 19(4):2428. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042428
Chicago/Turabian StyleKim, Jahyung, Bum-Jin Shim, Jae-Shin Yang, Altanzul Bat-Ulzii, and Jaeho Cho. 2022. "Clinical Manifestations, Diagnosis and Management of Synovial Fistula Associated Lateral Ankle Sprain or Instability: A Retrospective Study of 19 Surgically Confirmed Patients" International Journal of Environmental Research and Public Health 19, no. 4: 2428. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042428