
The Robust Italian Validation of the Coping Humor Scale (RI-CHS) for Adult Health Care Workers

 ,
,  ,
,  ,
,  ,
, 

Abstract
:1. Introduction
1.1. Measurement of Coping Humor Strategy
2. Materials and Methods
2.1. Participants/Data Collection
2.2. Sample Characteristics
3. Results
3.1. Data Analysis
3.1.1. Confirmatory Factor Analysis
3.1.2. Measurement Invariance Analysis
3.1.3. Internal Consistency Reliability
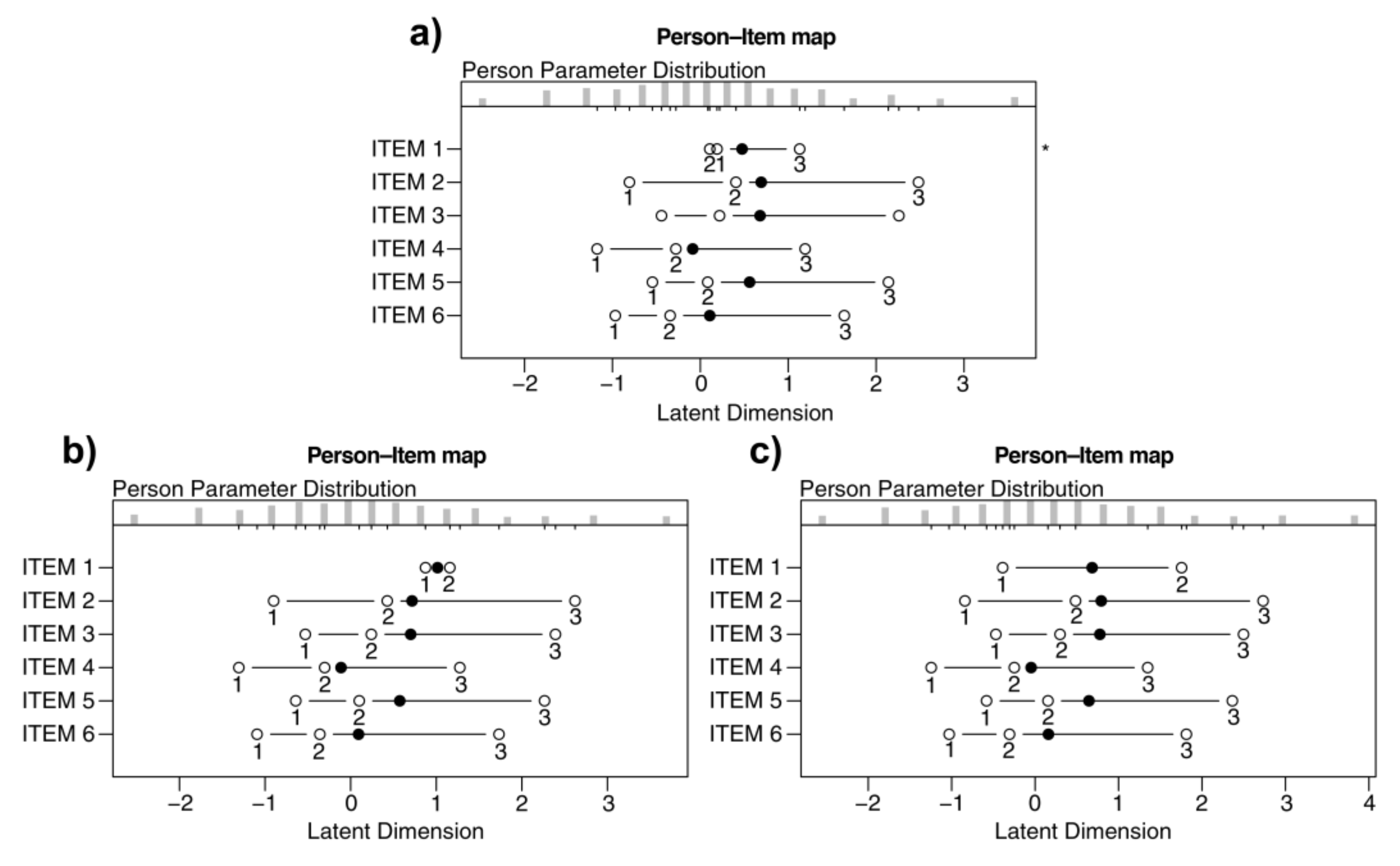
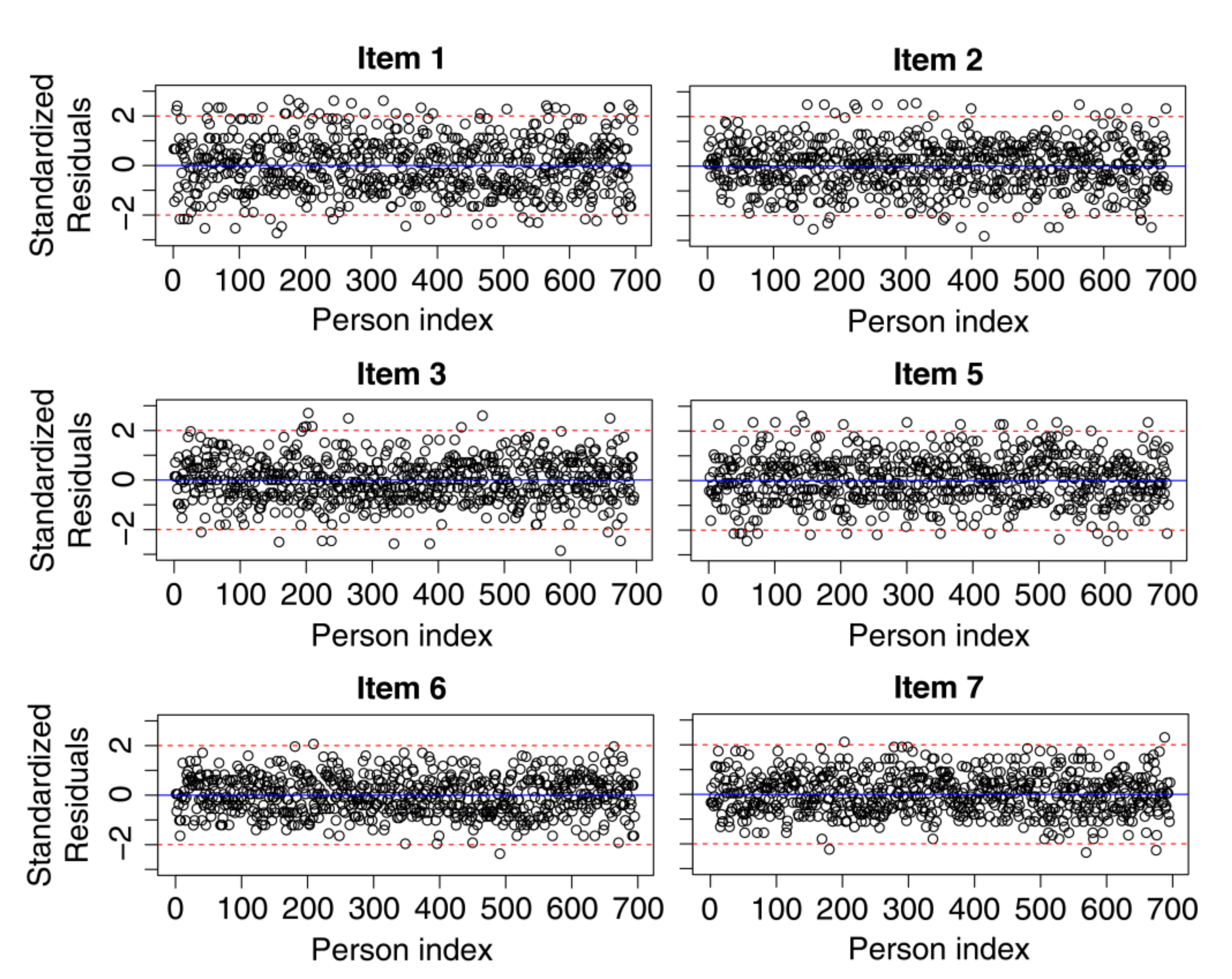
3.1.4. Rasch Analysis
Checking Requirements of the 6-Items Solution
3.1.5. Criterion Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lefcourt, H.M. Humor. In Handbook of Positive Psychology; Snyder, C.R., Lopez, S.J., Eds.; Oxford University Press: New York, NY, USA, 2002; pp. 619–631. [Google Scholar]
- Vaillant, G.E. Adaptive mental mechanisms: Their role in a positive psychology. Am. Psychol. 2000, 55, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.; Seligman, M.E.P. Character Strengths and Virtues: A Handbook and Classification; Oxford University Press: New York, NY, USA, 2004. [Google Scholar]
- Müller, L.; Ruch, W. Humor and strengths of character. J. Posit. Psychol. 2011, 6, 368–376. [Google Scholar] [CrossRef]
- Abel, M.H. Humor, stress, and coping strategies. HUMOR 2002, 15, 365–381. [Google Scholar] [CrossRef]
- Henman, L.D. Humor as a coping mechanism: Lessons from POWs. HUMOR 2001, 14, 83–94. [Google Scholar] [CrossRef]
- Kuiper, N.A. Humor and Resiliency: Towards a Process Model of Coping and Growth. Eur. J. Psychol. 2012, 8, 475–491. [Google Scholar] [CrossRef]
- Geisler, F.C.M.; Weber, H. Harm that does not hurt: Humour in coping with self-threat. Motiv. Emot. 2010, 34, 446–456. [Google Scholar] [CrossRef]
- Kuiper, N.A.; Martin, R.A.; Olinger, L.J. Coping humour, stress, and cognitive appraisals. Can. J. Behav. Sci. Rev. Can. Des Sci. Du Comport. 1993, 25, 81–96. [Google Scholar] [CrossRef] [Green Version]
- Gerbino, M.; Milioni, M.; Alessandri, G.; Eisenberg, N.; Caprara, M.; Kupfer, A.; Pastorelli, C.; Caprara, G.V. Self-Efficacy in Retrieving Positive Emotional Experience and Using Humor. Eur. J. Psychol. Assess. 2018, 34, 409–420. [Google Scholar] [CrossRef]
- Crawford, S.A.; Caltabiano, N.J. Promoting emotional well-being through the use of humour. J. Posit. Psychol. 2011, 6, 237–252. [Google Scholar] [CrossRef]
- Doosje, S.; Landsheer, J.A.; de Goede, M.P.M.; van Doornen, L.J.P. Humorous coping scales and their fit to a stress and coping framework. Q. Quantity 2012, 46, 267–279. [Google Scholar] [CrossRef]
- Martin, R.A.; Lefcourt, H.M. Sense of humor as a moderator of the relation between stressors and moods. J. Pers. Soc. Psychol. 1983, 45, 1313–1324. [Google Scholar] [CrossRef]
- Martin, R.A.; Kuiper, N.A.; Olinger, L.J.; Dance, K.A. Humor, coping with stress, self-concept, and psychological well-being. HUMOR 1993, 6, 89–104. [Google Scholar] [CrossRef]
- Koestler, A. The Act of Creation; Hutchinson: London, UK, 1964. [Google Scholar]
- Wyer, R.S.; Collins, J.E. A theory of humor elicitation. Psychol. Rev. 1992, 99, 663–688. [Google Scholar] [CrossRef] [PubMed]
- Forabosco, G. Cognitive aspects of the humor process: The concept of incongruity. HUMOR 1992, 5, 45–68. [Google Scholar] [CrossRef]
- Dixon, N.F. Humor: A cognitive alternative to stress? In Stress and Anxiety; Sarason, I.G., Spielberger, C.D., Eds.; Hemi-sphere: Washington, DC, USA, 1980; Volume 7, pp. 281–289. [Google Scholar]
- Martin, R.A. Humour and the mastery of living: Using humour to cope with the daily stresses of growing up. In Humour and Children’s Development: A Guide to Practical Applications; McGhee, P.E., Ed.; Ha worth Press: New York, NY, USA, 1989; pp. 135–154. [Google Scholar] [CrossRef]
- Canestrari, C.; Branchini, E.; Bianchi, I.; Savardi, U.; Burro, R. Pleasures of the Mind: What Makes Jokes and Insight Problems Enjoyable. Front. Psychol. 2018, 8, 2297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gick, M.L.; Lockhart, R.S. Cognitive and affective components of insight. In The Nature of Insight; Sternberg, R.J., Davidson, J.E., Eds.; MIT Press: Cambridge, MA, USA, 1995; pp. 197–228. [Google Scholar]
- Kozbelt, A.; Nishioka, K. Humor comprehension, humor production, and insight: An exploratory study. HUMOR 2010, 23, 375–401. [Google Scholar] [CrossRef]
- Wanzer, M.; Booth-Butterfield, M.; Booth-Butterfield, S. “If We Didn’t Use Humor, We’d Cry”: Humorous Coping Communication in Health Care Settings. J. Health Commun. 2005, 10, 105–125. [Google Scholar] [CrossRef] [PubMed]
- Strick, M.; Holland, R.W.; van Baaren, R.B.; van Knippenberg, A. Finding comfort in a joke: Consolatory effects of humor through cognitive distraction. Emotion 2009, 9, 574–578. [Google Scholar] [CrossRef] [Green Version]
- Martin, R.A. Humor, laughter, and physical health: Methodological issues and research findings. Psychol. Bull. 2001, 127, 504–519. [Google Scholar] [CrossRef]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the Brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Thomas, S.E. An Investigation into the Use of Humor for Coping with Stress. Doctoral Dissertation, Waterloo University, Waterloo, ON, Canada, 2000. [Google Scholar]
- De Koning, E.; Weiss, R.L. The Relational Humor Inventory: Functions of Humor in Close Relationships. Am. J. Fam. Ther. 2002, 30, 1–18. [Google Scholar] [CrossRef]
- Doosje, S.; De Goede, M.; Van Doornen, L.; Goldstein, J. Measurement of occupational humorous coping. HUMOR 2010, 23, 275–306. [Google Scholar] [CrossRef]
- Martin, R.A. The Situational Humor Response Questionnaire (SHRQ) and Coping Humor Scale (CHS): A decade of research findings. HUMOR 1996, 9, 251–272. [Google Scholar] [CrossRef]
- Nezlek, J.B.; Derks, P.; Derks, J.B.N.P. Use of humor as a coping mechanism, psychological adjustment, and social interaction. HUMOR 2001, 14, 251–272. [Google Scholar] [CrossRef] [Green Version]
- Overholser, J.C. Sense of humor when coping with life stress. Pers. Individ. Differ. 1992, 13, 799–804. [Google Scholar] [CrossRef]
- Ruch, W. Psychology of humor. In The Primer of Humor Research; Raskin, V., Ed.; Mouton de Gruyter: Berlin, Germany, 2008; pp. 17–100. [Google Scholar] [CrossRef]
- Bischetti, L.; Canal, P.; Bambini, V. Funny but aversive: A large-scale survey of the emotional response to Covid-19 humor in the Italian population during the lockdown. Lingua 2020, 249, 102963. [Google Scholar] [CrossRef]
- Canestrari, C.; Bongelli, R.; Fermani, A.; Riccioni, I.; Bertolazzi, A.; Muzi, M.; Burro, R. Coronavirus Disease Stress Among Italian Healthcare Workers: The Role of Coping Humor. Front. Psychol. 2021, 11, 601574. [Google Scholar] [CrossRef]
- Molteni, M. Implicazioni psicosociali di un disastro naturale: Uno studio sul terremoto dell’Abruzzo. Riv. Di Psicol. Dell’emergenza E Dell’assistenza Um. 2011, 5, 51–75. [Google Scholar]
- Forabosco, G. Il settimo senso. In Psicologia Del Senso Dell’umorismo Con Istruzioni Per L’uso; Muzzio: Padova, Italy, 1994. [Google Scholar]
- Pietrantoni, L.; Dionigi, A. “Quando ridere fa male”: La relazione tra eventi di vita, stili umoristici e disagio psicologico. Psicoter. Cogn. E Comport. 2006, 3, 301–315. [Google Scholar]
- Vagnoli, L.; Stefanenko, E.; Graziani, D.; Duradoni, M.; Ivanova, A. Measuring the fear of being laughed at in Italian and Russian adolescents. Curr. Psychol. 2021, 1–17. [Google Scholar] [CrossRef]
- Navarro-Carrillo, G.; Torres-Marín, J.; Corbacho-Lobato, J.M.; Carretero-Dios, H. The effect of humour on nursing professionals’ psychological well-being goes beyond the influence of empathy: A cross-sectional study. Scand. J. Caring Sci. 2019, 34, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Proyer, R.T.; Rodden, F.A. Virtuous Humor in Health Care. AMA J. Ethic 2020, 22, E615–E618. [Google Scholar] [CrossRef]
- Sun, P.; Chen, J.J.; Jiang, H. Coping Humor as a Mediator Between Emotional Intelligence and Job Satisfaction. A study on Chinese primary school teachers. J. Pers. Psychol. 2017, 16, 155–159. [Google Scholar] [CrossRef]
- Plester, B. Healthy humour: Using humour to cope at work. Kōtuitui N. Z. J. Soc. Sci. Online 2009, 4, 89–102. [Google Scholar] [CrossRef] [Green Version]
- Beck, C.T. Humor in nursing practice: A phenomenological study. Int. J. Nurs. Stud. 1997, 34, 346–352. [Google Scholar] [CrossRef]
- Dionigi, A.; Canestrari, C. The role of laughter in cognitive-behavioral therapy: Case studies. Discourse Stud. 2018, 20, 323–339. [Google Scholar] [CrossRef] [Green Version]
- Dionigi, A.; Canestrari, C. The use of humor by therapists and clients in cognitive therapy. Eur. J. Humour Res. 2018, 6, 50–67. [Google Scholar] [CrossRef] [Green Version]
- Levinson, W. Physician-patient communication. The relationship with malpractice claims among primary care physicians and surgeons. JAMA 1997, 277, 553–559. [Google Scholar] [CrossRef]
- Rowe, A.; Regehr, C. Whatever Gets You Through Today: An Examination of Cynical Humor Among Emergency Service Professionals. J. Loss Trauma 2010, 15, 448–464. [Google Scholar] [CrossRef]
- Preti, E.; Di Mattei, V.; Perego, G.; Ferrari, F.; Mazzetti, M.; Taranto, P.; Di Pierro, R.; Madeddu, F.; Calati, R. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Curr. Psychiatry Rep. 2020, 22, 43. [Google Scholar] [CrossRef]
- Chong, M.-Y.; Wang, W.-C.; Hsieh, W.-C.; Lee, C.-Y.; Chiu, N.-M.; Yeh, W.-C.; Huang, O.-L.; Wen, J.-K.; Chen, C.-L. Psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital. Br. J. Psychiatry 2004, 185, 127–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The Psychological Impact of the SARS Epidemic on Hospital Employees in China: Exposure, Risk Perception, and Altruistic Acceptance of Risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Ripoll, M.J.; Meneses-Echavez, J.F.; Ricci-Cabello, I.; Fraile-Navarro, D.; Fiol-deRoque, M.A.; Pastor-Moreno, G.; Castro, A.; Ruiz-Pérez, I.; Zamanillo Campos, R.; Gonçalves-Bradley, D.C. Impact of viral epidemic outbreaks on mental health of healthcare workers: A rapid systematic review and meta-analysis. J. Affect Disord. 2020, 277, 347–357. Available online: https://ssrn.com/abstract=3569883 (accessed on 22 July 2021). [CrossRef] [PubMed]
- Du, J.; Dong, L.; Wang, T.; Yuan, C.; Fu, R.; Zhang, L.; Liu, B.; Zhang, M.; Yin, Y.; Qin, J.; et al. Psychological symptoms among frontline healthcare workers during COVID-19 outbreak in Wuhan. Gen. Hosp. Psychiatry 2020, 67, 144–145. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC7194721/ (accessed on 22 July 2021). [CrossRef]
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Badiale, C.S.; Pietrabissa, G.; Manna, C.; Badiale, M.S.; Riva, G.; Castelnuovo, G.; Molinari, E. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Magnavita, N.; Tripepi, G.; Di Prinzio, R.R. Symptoms in Health Care Workers during the COVID-19 Epidemic. A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 5218. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Hardiness, Stress and Secondary Trauma in Italian Healthcare and Emergency Workers during the COVID-19 Pandemic. Sustainability 2020, 12, 5592. [Google Scholar] [CrossRef]
- Yin, Q.; Sun, Z.; Liu, T.; Ni, X.; Deng, X.; Jia, Y.; Shang, Z.; Zhou, Y.; Liu, W. Posttraumatic stress symptoms of health care workers during the corona virus disease 2019. Clin. Psychol. Psychother. 2020, 27, 384–395. [Google Scholar] [CrossRef]
- Bongelli, R.; Canestrari, C.; Fermani, A.; Muzi, M.; Riccioni, I.; Bertolazzi, A.; Burro, R. Associations between Personality Traits, Intolerance of Uncertainty, Coping Strategies, and Stress in Italian Frontline and Non-Frontline HCWs during the COVID-19 Pandemic—A Multi-Group Path-Analysis. Healthcare 2021, 9, 1086. [Google Scholar] [CrossRef] [PubMed]
- Luce, R.; Tukey, J.W. Simultaneous conjoint measurement: A new type of fundamental measurement. J. Math. Psychol. 1964, 1, 1–27. [Google Scholar] [CrossRef]
- Bond, T.G.; Fox, C.M. Applying the Rasch Model: Fundamental Measurement in the Human Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2007. [Google Scholar]
- Andrich, D. Rasch Models for Measurement; Sage Publications: Beverly Hills, CA, USA, 1988. [Google Scholar]
- Rasch, G. Probabilistic Models for Some Intelligence and Attainment Tests; The University of Chicago Press: Chicago, IL, USA, 1960. [Google Scholar]
- Burro, R.; Vicentini, G.; Rocca, E.; Barnaba, V.; Hall, R.; Raccanello, D. Development and Validation of the Robust—Pandemic Coping Scale (R-PCS). Front. Psychol. 2021, 9, 725344. [Google Scholar] [CrossRef] [PubMed]
- Chiu, M.; Wong, H.; Ho, W. A comparative study of confirmatory factor analysis and Rasch Analysis as item reduction strategies for SAMHSA recovery inventory for Chinese (SAMHSA-RIC). Eur. J. Psychiatry 2020, 34, 74–81. [Google Scholar] [CrossRef]
- Panella, L.; La Porta, F.; Caselli, S.; Marchisio, S.; Tennant, A. Predicting the need for institutional care shortly after admis-sion to rehabilitation: Rasch analysis and predictive validity of the BRASS index. Eur. J. Phys. Rehabil. Med. 2012, 48, 443–454. [Google Scholar]
- Raccanello, D.; Vicentini, G.; Trifiletti, E.; Burro, R. A Rasch Analysis of the School-Related Well-Being (SRW) Scale: Measuring Well-Being in the Transition from Primary to Secondary School. Int. J. Environ. Res. Public Health 2020, 18, 23. [Google Scholar] [CrossRef]
- Vidotto, G.; Moroni, L.; Burro, R.; Filipponi, L.; Balestroni, G.; Bettinardi, O.; Bruletti, G.; Giorgi, I.; Naimo, M.; Bertolotti, G. A revised short version of the depression questionnaire. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 187–197. [Google Scholar] [CrossRef]
- Burro, R. To be objective in Experimental Phenomenology: A Psychophysics application. SpringerPlus 2016, 5, 1720. [Google Scholar] [CrossRef] [Green Version]
- Bretagnolle, J. Test of monotonicity for the Rasch model. In Goodnessof-Fit Tests and Model Validity; Huber-Carol, C., Balakrishnan, N., Nikulin, M.S., Mesbah, M., Eds.; Statistics for Industry and Technology: Boston, MA, USA, 2002; pp. 365–370. [Google Scholar] [CrossRef]
- Kang, H.-A.; Su, Y.-H.; Chang, H.-H. A note on monotonicity of item response functions for ordered polytomous item response theory models. Br. J. Math. Stat. Psychol. 2018, 71, 523–535. [Google Scholar] [CrossRef]
- Debelak, R.; Koller, I. Testing the Local Independence Assumption of the Rasch Model with Q3-Based Nonparametric Model Tests. Appl. Psychol. Meas. 2019, 44, 103–117. [Google Scholar] [CrossRef]
- Marais, I. Local dependence. In Rasch Models in Health; Christensen, K.B., Kreiner, S., Mesbah, M., Eds.; ISTE Ltd.: London, UK; Wiley & Sons: Hoboken, NJ, USA, 2013; pp. 111–130. [Google Scholar] [CrossRef]
- Pallant, J.F.; Tennant, A. An introduction to the Rasch measurement model: An example using the hospital anxiety and de-pression scale (HADS). Br. J. Clin. Psychol. 2007, 46 Pt 1, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, K.B.; Bjorner, J.B.; Kreiner, S.; Petersen, J.H. Testing unidimensionality in polytomous Rasch models. Psychometrika 2002, 67, 563–574. [Google Scholar] [CrossRef]
- Smith, E.V., Jr. Detecting and evaluating the impact of multidimensionality using item fit statistics and principal component analysis of residuals. J. Appl. Meas. 2002, 3, 205–231. [Google Scholar] [PubMed]
- Hagquist, C.; Andrich, D. Recent advances in analysis of differential item functioning in health research using the Rasch model. Health Qual. Life Outcomes 2017, 15, 181. [Google Scholar] [CrossRef] [Green Version]
- Tennant, A.; Penta, M.; Tesio, L.; Grimby, G.; Thonnard, J.-L.; Slade, A.; Lawton, G.; Simone, A.; Carter, J.; Lundgren-Nilsson, Å.; et al. Assessing and Adjusting for Cross-Cultural Validity of Impairment and Activity Limitation Scales Through Differential Item Functioning within the Framework of the Rasch Model: The PRO-ESOR project. Med. Care 2004, 42, 37–48. [Google Scholar] [CrossRef]
- Linacre, J.M. Optimizing rating scale category effectiveness. J. Appl. Meas. 2002, 3, 85–106. [Google Scholar]
- Tennant, A.; Conaghan, P.G. The Rasch measurement model in rheumatology: What is it and why use it? When should it be applied, and what should one look for in a Rasch paper? Arthritis Care Res. 2007, 57, 1358–1362. [Google Scholar] [CrossRef]
- Wolins, L.; Wright, B.D.; Masters, G.N. Rating Scale Analysis: Rasch Measurement. J. Am. Stat. Assoc. 1983, 78, 497. [Google Scholar] [CrossRef]
- Wright, B.D.; Linacre, J.M. Reasonable mean-square-fit values. Rasch Meas. Trans. 1994, 8, 370. [Google Scholar]
- Wright, B.D. Separation, reliability and skewed distributions: Statistically different levels of performance. Rasch Meas. Trans. 2001, 14, 786. [Google Scholar]
- Kreiner, S.; Christensen, K.B. Person parameter estimation and measurement in Rasch models. In Rasch Models in Health; Christensen, K.B., Kreiner, S., Mesbah, M., Eds.; ISTE Ltd.: London, UK; Wiley & Sons: Hoboken, NJ, USA, 2013; pp. 63–78. [Google Scholar] [CrossRef]
- Andersen, H. Abductive and Deductive Change. Language 1973, 49, 765. [Google Scholar] [CrossRef]
- Masters, G.N.; Wright, B.D. The partial credit model. In Handbook of Modern Item Response Theory; Van der Linden, W.J., Hambleton, R.K., Eds.; Springer: New York, NY, USA, 1997; pp. 101–121. [Google Scholar] [CrossRef]
- Limesurvey GmbH. LimeSurvey: An Open Source Survey Tool; LimeSurvey GmbH: Hamburg, Germany, 2012; Available online: http://www.limesurvey.org (accessed on 4 May 2020).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org (accessed on 3 November 2021).
- Hu, L.-T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Marsh, H.W.; Hau, K.T.; Grayson, D. Goodness of fit evaluation in structural equation modeling. In Contemporary Psychometrics; Maydeu-Olivares, A., McArdle, J., Eds.; Erlbaum: Mahwah, NJ, USA, 2005; pp. 275–340. [Google Scholar]
- Schumacker, R.E.; Lomax, R.G. A beginner’s Guide to Structural Equation Modeling, 2nd ed.; Erlbaum: Mahwah, NJ, USA, 2004. [Google Scholar] [CrossRef]
- Fan, X.; Thompson, B.; Wang, L. Effects of sample size, estimation methods, and model specification on structural equation modeling fit indexes. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 56–83. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; The Guilford Press: New York, NY, USA, 2018; ISBN 978-1-60623-877-6. [Google Scholar]
- Chen, G.-H.; Martin, R.A. A comparison of humor styles, coping humor, and mental health between Chinese and Canadian university students. HUMOR 2007, 20, 215–234. [Google Scholar] [CrossRef]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. A Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Chou, Y.-T.; Wang, W.-C. Checking Dimensionality in Item Response Models with Principal Component Analysis on Standardized Residuals. Educ. Psychol. Meas. 2010, 70, 717–731. [Google Scholar] [CrossRef]
- Raiche, G. Critical eigenvalue sizes in standardized residual principal components analysis. Rasch Meas. Trans. 2005, 19, 1012. [Google Scholar]
- Smith, R.M. A comparison of methods for determining dimensionality in Rasch measurement. Struct. Equ. Model. A Multidiscip. J. 1996, 3, 25–40. [Google Scholar] [CrossRef]
- Linacre, J.M. Winsteps Rasch Measurement (Version 3.92.1). 2016. Available online: Winsteps.com (accessed on 4 May 2020).
- Dorans, N.J.; Schmitt, A.P.; Bleistein, C.A. The standardization approach to assessing comprehensive differential item functioning. J. Educ. Meas. 1992, 29, 309–319. [Google Scholar] [CrossRef]
- Ruch, W.; McGhee, P.E. Humor intervention programs. In The Wiley Blackwell Handbook of Positive Psychological Interventions, 1st ed.; Parks, A.C., Schueller, S., Eds.; John Wiley & Sons: West Sussex, UK, 2014; pp. 179–193. [Google Scholar] [CrossRef]
- Osincup, P. How to Use Humor in Clinical Settings. AMA J. Ethic 2020, 22, E588–E595. [Google Scholar] [CrossRef]
- Tagalidou, N.; Baier, J.; Laireiter, A.-R. The effects of three positive psychology interventions using online diaries: A randomized-placebo controlled trial. Internet Interv. 2019, 17, 100242. [Google Scholar] [CrossRef] [PubMed]
- Wellenzohn, S.; Proyer, R.; Ruch, W. Who Benefits from Humor-Based Positive Psychology Interventions? The Moderating Effects of Personality Traits and Sense of Humor. Front. Psychol. 2018, 9, 821. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) |
|---|---|
| Total | 735 (100%) |
| Socio-demographic characteristics | |
| Gender | |
| Female | 516 (70.2%) |
| Male | 219 (29.8%) |
| Age | |
| 18–30 | 137 (18.6%) |
| 31–40 | 141 (19.2%) |
| 41–50 | 196 (26.7%) |
| 51–60 | 208 (28.3%) |
| >60 | 53 (7.2%) |
| Marital status | |
| Married | 332 (45.1%) |
| Unmarried | 202 (27.5%) |
| Domestic partner | 115 (15.7%) |
| Divorced/separated | 72 (9.8%) |
| Widower/widow | 14 (1.9%) |
| Children | |
| Yes | 426 (57.9%) |
| No | 309 (42.1%) |
| Religion | |
| Believer occasionally practitioner | 282 (38.4%) |
| Believer non-practitioner | 175 (23.8%) |
| Non-Believer | 122 (16.6%) |
| Believer practitioner | 116 (15.8%) |
| Prefer not to answer | 40 (5.4%) |
| Job characteristics | |
| Place of work | |
| North Italy | 516 (70.2%) |
| Centre Italy | 138 (18.8%) |
| South Italy | 81 (11.0%) |
| Job position | |
| Nurse | 558 (75.9%) |
| Physician | 177 (24.1%) |
| Job area | |
| Medical specialties | 381 (51.8%) |
| Diagnostic and therapeutic specialties | 155 (21.1%) |
| Surgical specialties | 114 (15.5%) |
| Primary care nurse serv. | 85 (11.6%) |
| Seniority | |
| More than 20 years | 350 (47.6%) |
| Less than 5 years | 162 (22.0%) |
| 10–20 years | 131 (17.8%) |
| 5–10 years | 92 (12.6%) |
| Job exposure to COVID-19 | |
| Wards | |
| Worked in COVID-19-dedicated wards | 302 (41.1%) |
| Worked in other wards | 433 (58.9%) |
| Models | ΔCFI | ΔRMSEA | ΔSRMR |
|---|---|---|---|
| Configural | −0.001 | 0.009 | 0.006 |
| Metric | −0.000 | −0.006 | 0.004 |
| Scalar | −0.002 | −0.005 | −0.003 |
| Original CHS Item Number | Infit-MSQ | Outfit-MSQ |
|---|---|---|
| 1 (reverse) | 1.356 | 1.399 |
| 2 | 0.949 | 0.959 |
| 3 | 0.798 | 0.788 |
| 5 | 0.946 | 0.941 |
| 6 | 0.608 | 0.605 |
| 7 | 0.650 | 0.642 |
| Total Raw Scores | Interval Logit Scores |
|---|---|
| 6 | 1 |
| 7 | 1.909 |
| 8 | 2.743 |
| 9 | 3.271 |
| 10 | 3.682 |
| 11 | 4.035 |
| 12 | 4.359 |
| 13 | 4.670 |
| 14 | 4.981 |
| 15 | 5.300 |
| 16 | 5.637 |
| 17 | 6.001 |
| 18 | 6.400 |
| 19 | 6.848 |
| 20 | 7.368 |
| 21 | 8.013 |
| 22 | 8.969 |
| 23 | 10 |
| Items Number | CHS Items (English) | CHS Response Scale | RI-CHS Items (Italian) | RI-CHS Response Scale |
|---|---|---|---|---|
| 1 (reverse item) | I often lose my sense of humor when I am having problems | 4–Strongly disagree 3–Mildly disagree 2–Mildly agree 1–Strongly agree | Perdo il senso dell’umorismo quando ho problemi | 3–Molto in disaccordo 2–Un poco in disaccordo 2–Un poco d’accordo 1–Molto d’accordo |
| 2 | I have often found that my problems have been greatly reduced when I try to find something funny in them | 1–Strongly disagree 2–Mildly disagree 3–Mildly agree 4–Strongly agree | Ho riscontrato che i miei problemi si sono fortemente ridotti quando ho provato a trovare in essi qualcosa di divertente | 1–Molto in disaccordo 2–Un poco in disaccordo 3–Un poco d’accordo 4–Molto d’accordo |
| 3 | I usually look for something comical to say when I am in tense situations | 1–Strongly disagree 2–Mildly disagree 3–Mildly agree 4–Strongly agree | Cerco qualcosa di comico da dire quando sono in situazioni tese | 1–Molto in disaccordo 2–Un poco in disaccordo 3–Un poco d’accordo 4–Molto d’accordo |
| 4 (reverse item) | I must admit my life would probably be a lot easier if I had more of a sense of humor | 4–Strongly disagree 3–Mildly disagree 2–Mildly agree 1–Strongly agree | Devo ammettere che la mia vita sarebbe più facile se avessi maggiore senso dell’umorismo | NO RESPONSE SCALE This item has been excluded from RI-CHS |
| 5 | I have often felt that if I am in a situation where I have to either cry of laugh, it’s better to laugh | 1–Strongly disagree 2–Mildly disagree 3–Mildly agree 4–Strongly agree | Mi è capitato di pensare che, se sono in una situazione dove si può piangere o ridere, è meglio ridere | 1–Molto in disaccordo 2–Un poco in disaccordo 3–Un poco d’accordo 4–Molto d’accordo |
| 6 | I can usually find something to laugh or joke about even in trying situations | 1–Strongly disagree 2–Mildly disagree 3–Mildly agree 4–Strongly agree | Riesco a trovare qualcosa su cui ridere o scherzare persino in situazioni difficili | 1–Molto in disaccordo 2–Un poco in disaccordo 3–Un poco d’accordo 4–Molto d’accordo |
| 7 | It has been my experience that humor is often a very effective way of coping with problems | 1–Strongly disagree 2–Mildly disagree 3–Mildly agree 4–Strongly agree | Fa parte della mia esperienza pensare che l’umorismo sia spesso una via efficace per fronteggiare i problemi | 1–Molto in disaccordo 2–Un poco in disaccordo 3–Un poco d’accordo 4–Molto d’accordo |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burro, R.; Fermani, A.; Bongelli, R.; Riccioni, I.; Muzi, M.; Bertolazzi, A.; Canestrari, C. The Robust Italian Validation of the Coping Humor Scale (RI-CHS) for Adult Health Care Workers. Int. J. Environ. Res. Public Health 2022, 19, 2522. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052522
Burro R, Fermani A, Bongelli R, Riccioni I, Muzi M, Bertolazzi A, Canestrari C. The Robust Italian Validation of the Coping Humor Scale (RI-CHS) for Adult Health Care Workers. International Journal of Environmental Research and Public Health. 2022; 19(5):2522. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052522
Chicago/Turabian StyleBurro, Roberto, Alessandra Fermani, Ramona Bongelli, Ilaria Riccioni, Morena Muzi, Alessia Bertolazzi, and Carla Canestrari. 2022. "The Robust Italian Validation of the Coping Humor Scale (RI-CHS) for Adult Health Care Workers" International Journal of Environmental Research and Public Health 19, no. 5: 2522. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052522