
Long-Term Risk of Breast Cancer after Diagnosis of Benign Breast Disease by Screening Mammography

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Study Population
2.2. Analyses
3. Results
3.1. Study Population Characteristics
3.2. Rates of Breast Cancer among Women with and witthout a Benign Breast Disease
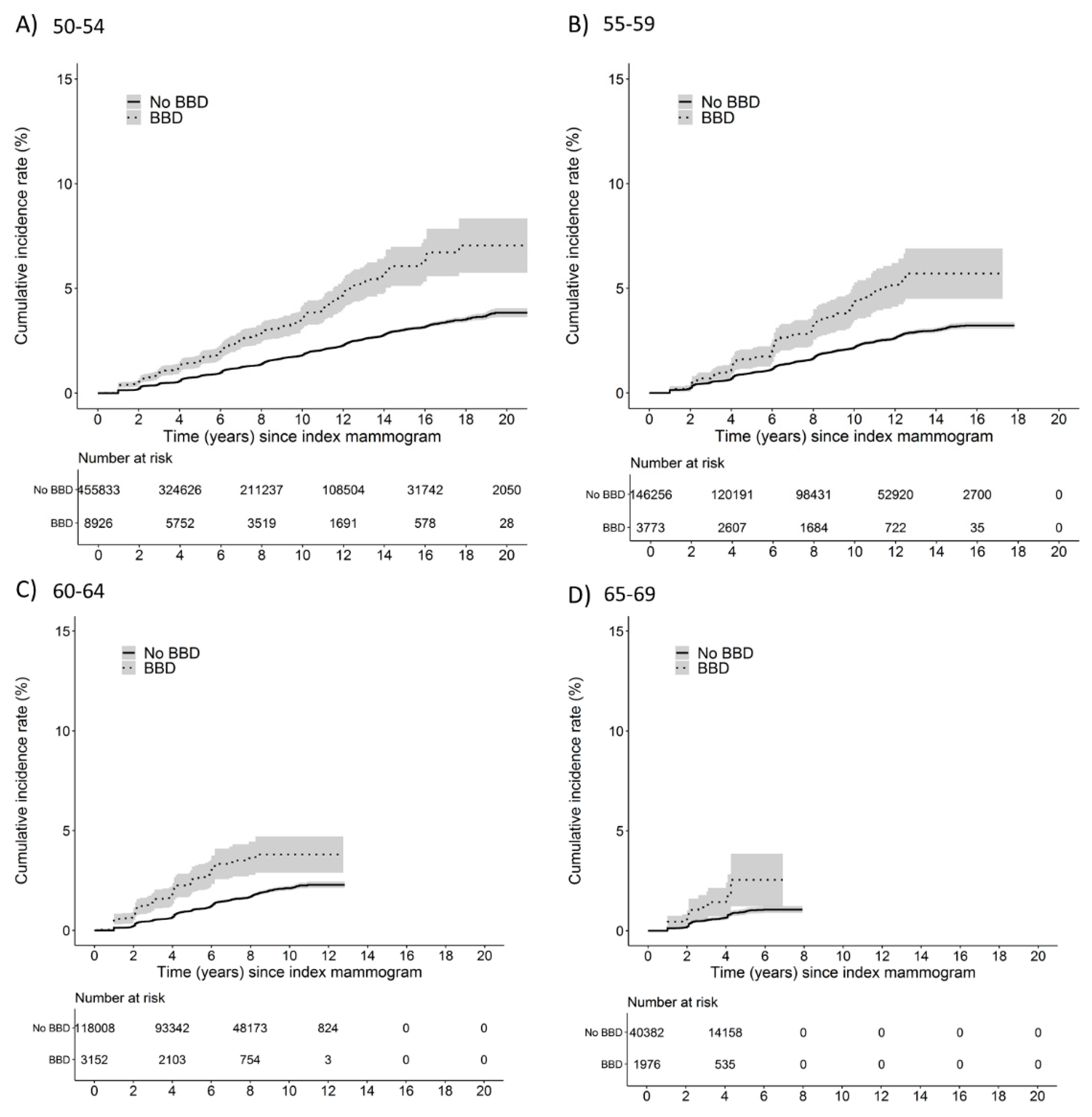
3.3. Cumulative Incidence of Breast Cancer by Year and Age at Index Mammogram
3.4. Risk of Breast Cancer among Women with and without a Benign Breast Disease
3.5. Supplementary Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hartmann, L.C.; Sellers, T.A.; Frost, M.H.; Lingle, W.L.; Degnim, A.C.; Ghosh, K.; Vierkant, R.; Maloney, S.D.; Pankratz, V.S.; Hillman, D.W.; et al. Benign Breast Disease and the Risk of Breast Cancer. N. Engl. J. Med. 2005, 353, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Castells, X.; Domingo, L.; Corominas, J.M.; Torá-Rocamora, I.; Quintana, M.J.; Baré, M.; Vidal, C.; Natal, C.; Sánchez, M.; Saladié, F.; et al. Breast cancer risk after diagnosis by screening mammography of nonproliferative or proliferative benign breast disease: A study from a population-based screening program. Breast Cancer Res. Treat. 2015, 149, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Buch, K.A.; Qureshi, M.M.; Carpentier, B.; Cunningham, D.A.; Stone, M.; Jaffe, C.; Quinn, M.; Gonzalez, C.; LaVoye, J.; Hines, N.; et al. Surveillance of Probably Benign (BI-RADS 3) Lesions in Mammography: What Is the Right Follow-Up Protocol? Breast J. 2015, 21, 168–174. [Google Scholar] [CrossRef]
- Lavoué, V.; Fritel, X.; Antoine, M.; Beltjens, F.; Bendifallah, S.; Boisserie-Lacroix, M.; Boulanger, L.; Canlorbe, G.; Catteau-Jonard, S.; Chabbert-Buffet, N.; et al. Clinical practice guidelines from the French College of Gynecologists and Obstetricians (CNGOF): Benign breast tumors—Short text. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 200, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Rao, R.; Ludwig, K.; Bailey, L.; Berry, T.S.; Buras, R.; Degnim, A.; Fayanju, O.M.; Froman, J.; Golesorkhi, N.; Greenburg, C.; et al. Select Choices in Benign Breast Disease: An Initiative of the American Society of Breast Surgeons for the American Board of Internal Medicine Choosing Wisely® Campaign. Ann. Surg. Oncol. 2018, 25, 2795–2800. [Google Scholar] [CrossRef]
- Tyrer, J.; Duffy, S.W.; Cuzick, J. A breast cancer prediction model incorporating familial and personal risk factors. Stat. Med. 2004, 23, 1111–1130. [Google Scholar] [CrossRef] [Green Version]
- Tice, J.A.; Miglioretti, D.L.; Li, C.-S.; Vachon, C.M.; Gard, C.C.; Kerlikowske, K. Breast Density and Benign Breast Disease: Risk Assessment to Identify Women at High Risk of Breast Cancer. J. Clin. Oncol. 2015, 33, 3137–3143. [Google Scholar] [CrossRef] [Green Version]
- Schousboe, J.T.; Kerlikowske, K.; Loh, A.; Cummings, S.R. Personalizing Mammography by Breast Density and Other Risk Factors for Breast Cancer: Analysis of Health Benefits and Cost-Effectiveness. Ann. Intern. Med. 2011, 155, 10–20. [Google Scholar] [CrossRef] [Green Version]
- Vilaprinyo, E.; Forne, C.; Carles, M.; Sala, M.; Pla, R.; Castells, X.; Domingo, L.; Rue, M. the Interval Cancer (INCA) Study Group Cost-Effectiveness and Harm-Benefit Analyses of Risk-Based Screening Strategies for Breast Cancer. PLoS ONE 2014, 9, e86858. [Google Scholar] [CrossRef] [Green Version]
- Tice, J.A.; O’Meara, E.S.; Weaver, D.L.; Vachon, C.; Ballard-Barbash, R.; Kerlikowske, K. Benign Breast Disease, Mammographic Breast Density, and the Risk of Breast Cancer. J. Natl. Cancer Inst. 2013, 105, 1043–1049. [Google Scholar] [CrossRef]
- Dyrstad, S.W.; Yan, Y.; Fowler, A.M.; Colditz, G.A. Breast cancer risk associated with benign breast disease: Systematic review and meta-analysis. Breast Cancer Res. Treat. 2015, 149, 569–575. [Google Scholar] [CrossRef]
- Perry, N.; Broeders, M.; de Wolf, C.; Törnberg, S.; Holland, R.; von Karsa, L. European guidelines for quality assurance in breast cancer screening and diagnosis. Fourth edition—Summary document. Ann. Oncol. 2008, 19, 614–622. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Lerda, D.; Quinn, C.; Follmann, M.; Alonso-Coello, P.; Rossi, P.G.; Lebeau, A.; Nyström, L.; Broeders, M.; Ioannidou-Mouzaka, L.; et al. Breast Cancer Screening and Diagnosis: A Synopsis of the European Breast Guidelines. Ann. Intern. Med. 2020, 172, 46–56. [Google Scholar] [CrossRef] [Green Version]
- European Commission Initiative on Breast Cancer Contributor Group. European Guidelines on Breast Cancer Screening and Diagnosis. Available online: https://healthcare-quality.jrc.ec.europa.eu/european-breast-cancer-guidelines (accessed on 11 February 2022).
- Castells, X.; Sala, M.; Ascunce, N.; Salas, D.; Zubizarreta, R.; Casamitjana, M. Descripción del Cribado del Cáncer en España. Proyecto DESCRIC. Madrid: Plan de Calidad para el Sistema Nacional de Salud. Ministerio de Sanidad y Consumo. Agència d’Avaluació de Tecnologia i Recerca Mèiques de Cataluña. Available online: https://www.sergas.es/Docs/Avalia-t/AATRM200601.pdf (accessed on 11 February 2022).
- Ascunce, N.; Salas, D.; Zubizarreta, R.; Almazán, R.; Ibáñez, J.; Ederra, M.; Fernández, R.; Moreo, P.; Natal, C.; Sánchez-Contador, C.; et al. Cancer screening in Spain. Ann. Oncol. 2010, 21, iii43–iii51. [Google Scholar] [CrossRef]
- Sickles, E.A.; D’Orsi, C.J.; Bassett, L.W. ACR BI-RADS® Mammography. In ACR BI-RADS® Atlas; Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Dupont, W.D.; Page, D.L. Risk Factors for Breast Cancer in Women with Proliferative Breast Disease. N. Engl. J. Med. 1985, 312, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Putter, H.; Fiocco, M.; Geskus, R.B. Tutorial in biostatistics: Competing risks and multi-state models. Stat. Med. 2006, 26, 2389–2430. [Google Scholar] [CrossRef]
- Román, M.; Louro, J.; Posso, M.; Alcántara, R.; Peñalva, L.; Sala, M.; del Riego, J.; Prieto, M.; Vidal, C.; Sánchez, M.; et al. Breast density, benign breast disease, and risk of breast cancer over time. Eur. Radiol. 2021, 31, 4839–4847. [Google Scholar] [CrossRef]
- Kabat, G.C.; Jones, J.G.; Olson, N.; Negassa, A.; Duggan, C.; Ginsberg, M.; Kandel, R.A.; Glass, A.G.; Rohan, T.E. A multi-center prospective cohort study of benign breast disease and risk of subsequent breast cancer. Cancer Causes Control 2010, 21, 821–828. [Google Scholar] [CrossRef] [Green Version]
- Dupont, W.D.; Page, D.L.; Parl, F.F.; Vnencak-Jones, C.L.; Plummer, W.D.; Rados, M.S.; Schuyler, P.A. Long-Term Risk of Breast Cancer in Women with Fibroadenoma. N. Engl. J. Med. 1994, 331, 10–15. [Google Scholar] [CrossRef]
- Hofvind, S.; Geller, B.; Vacek, P.M.; Thoresen, S.; Skaane, P. Using the European guidelines to evaluate the Norwegian Breast Cancer Screening Program. Eur. J. Epidemiol. 2007, 22, 447–455. [Google Scholar] [CrossRef]
- Wang, J.; Costantino, J.P.; Tan-Chiu, E.; Wickerham, D.L.; Paik, S.; Wolmark, N. Lower-Category Benign Breast Disease and the Risk of Invasive Breast Cancer. J. Natl. Cancer Inst. 2004, 96, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Louro, J.; Román, M.; Posso, M.; Vázquez, I.; Saladié, F.; Rodriguez-Arana, A.; Quintana, M.J.; Domingo, L.; Baré, M.; Marcos-Gragera, R.; et al. Developing and validating an individualized breast cancer risk prediction model for women attending breast cancer screening. PLoS ONE 2021, 16, e0248930. [Google Scholar] [CrossRef] [PubMed]
- Brentnall, A.R.; Harkness, E.F.; Astley, S.M.; Donnelly, L.S.; Stavrinos, P.; Sampson, S.; Fox, L.; Sergeant, J.C.; Harvie, M.N.; Wilson, M.; et al. Mammographic density adds accuracy to both the Tyrer-Cuzick and Gail breast cancer risk models in a prospective UK screening cohort. Breast Cancer Res. 2015, 17, 147. [Google Scholar] [CrossRef] [Green Version]
- Louro, J.; Posso, M.; Boon, M.H.; Román, M.; Domingo, L.; Castells, X.; Sala, M. A systematic review and quality assessment of individualised breast cancer risk prediction models. Br. J. Cancer 2019, 121, 76–85. [Google Scholar] [CrossRef] [Green Version]
- Sala, M.; Salas, D.; Belvis, F.; Sánchez, M.; Ferrer, J.; Ibáñez, J.; Román, R.; Ferrer, F.; Vega, A.; Laso, M.S.; et al. Reduction in False-Positive Results after Introduction of Digital Mammography: Analysis from Four Population-based Breast Cancer Screening Programs in Spain. Radiology 2011, 258, 388–395. [Google Scholar] [CrossRef] [Green Version]
- Harvey, J.A.; Gard, C.C.; Miglioretti, D.L.; Yankaskas, B.C.; Kerlikowske, K.; Buist, D.S.M.; Geller, B.A.; Onega, T.L. For the Breast Cancer Surveillance Consortium Reported Mammographic Density: Film-Screen versus Digital Acquisition. Radiology 2013, 266, 752–758. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| No BBD (n = 760,479) | BBD (n = 17,827) | Total (n = 778,306) | ||
|---|---|---|---|---|
| Year at index mammogram | ||||
| 1996–2000 | 117,837 (15.5%) | 2287 (12.8%) | 120,124 (15.4%) | |
| 2001–2005 | 237,613 (31.2%) | 3985 (22.4%) | 241,598 (31.0%) | |
| 2006–2010 | 210,947 (27.7%) | 5156 (28.9%) | 216,103 (27.8%) | |
| 2011–2015 | 194,082 (25.5%) | 6399 (35.9%) | 200,481 (25.8%) | |
| Age at index mammogram | ||||
| 50–54 | 455,833 (59.9%) | 8926 (50.1%) | 464,759 (59.7%) | |
| 55–59 | 146,256 (19.2%) | 3773 (21.2%) | 150,029 (19.3%) | |
| 60–64 | 118,008 (15.5%) | 3152 (17.7%) | 121,160 (15.6%) | |
| 65–69 | 40,382 (5.3%) | 1976 (11.1%) | 42,358 (5.4%) | |
| Time since index mammogram | ||||
| ≤4 years | 242,557 (31.9%) | 7582 (42.5%) | 250,139 (32.1%) | |
| >4 and ≤8 years | 179,167 (23.6%) | 4662 (26.2%) | 183,829 (23.6%) | |
| >8 and ≤12 years | 188,399 (24.8%) | 3361 (18.9%) | 191,760 (24.6%) | |
| >12 years | 150,356 (19.8%) | 2222 (12.5%) | 152,578 (19.6%) | |
| Breast Cancer | ||||
| No | 749,213 (98.5%) | 17,385 (97.5%) | 766,598 (98.5%) | |
| Yes | 11,266 (1.5%) | 442 (2.5%) | 11,708 (1.5%) | |
| No Benign Breast Disease | Benign Breast Disease | |||||
|---|---|---|---|---|---|---|
| Women | Number of Breast Cancer cases | Rate per 1000 Women | Women | Number of Breast Cancer Cases | Rate per 1000 Women | |
| Year at index mammogram | ||||||
| 1996–2000 | 117,837 | 2776 | 23.6 (22.7–24.5) | 2287 | 95 | 41.5 (34.0–50.8) |
| 2001–2005 | 237,613 | 5042 | 21.2 (20.6–21.8) | 3985 | 156 | 39.1 (33.5–45.8) |
| 2006–2010 | 210,947 | 2715 | 12.9 (12.4–13.4) | 5156 | 128 | 24.8 (20.9–29.5) |
| 2011–2015 | 194,082 | 733 | 3.8 (3.5–4.1) | 6399 | 63 | 9.8 (7.7–12.6) |
| Age at index mammogram | ||||||
| 50–54 | 455,833 | 6477 | 14.2 (13.9–14.6) | 8926 | 233 | 26.1 (23.0–29.7) |
| 55–59 | 146,256 | 2938 | 20.1 (19.4–20.8) | 3773 | 107 | 28.4 (23.5–34.3) |
| 60–64 | 118,008 | 1645 | 13.9 (13.3–14.6) | 3152 | 79 | 25.1 (20.1–31.2) |
| 65–69 | 40,382 | 206 | 5.1 (4.5–5.8) | 1976 | 23 | 11.6 (7.7–17.5) |
| Time since index mammogram | ||||||
| ≤4 years | 242,557 | 4096 | 16.9 (16.4–17.4) | 7582 | 201 | 26.5 (23.1–30.4) |
| >4 and ≤8 years | 179,167 | 3990 | 22.3 (21.6–23.0) | 4662 | 147 | 31.5 (26.8–37.1) |
| >8 and ≤12 years | 188,399 | 2337 | 12.4 (11.9–12.9) | 3361 | 69 | 20.5 (16.2–26.0) |
| >12 years | 150,356 | 843 | 5.6 (5.2–6.0) | 2222 | 25 | 11.3 (7.6–16.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Román, M.; Louro, J.; Posso, M.; Vidal, C.; Bargalló, X.; Vázquez, I.; Quintana, M.J.; Alcántara, R.; Saladié, F.; del Riego, J.; et al. Long-Term Risk of Breast Cancer after Diagnosis of Benign Breast Disease by Screening Mammography. Int. J. Environ. Res. Public Health 2022, 19, 2625. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052625
Román M, Louro J, Posso M, Vidal C, Bargalló X, Vázquez I, Quintana MJ, Alcántara R, Saladié F, del Riego J, et al. Long-Term Risk of Breast Cancer after Diagnosis of Benign Breast Disease by Screening Mammography. International Journal of Environmental Research and Public Health. 2022; 19(5):2625. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052625
Chicago/Turabian StyleRomán, Marta, Javier Louro, Margarita Posso, Carmen Vidal, Xavier Bargalló, Ivonne Vázquez, María Jesús Quintana, Rodrigo Alcántara, Francina Saladié, Javier del Riego, and et al. 2022. "Long-Term Risk of Breast Cancer after Diagnosis of Benign Breast Disease by Screening Mammography" International Journal of Environmental Research and Public Health 19, no. 5: 2625. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052625