
Interventions to Improve Physical Capability of Older Adults with Mild Disabilities: A Case Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Physical Activity Rehabilitation Program
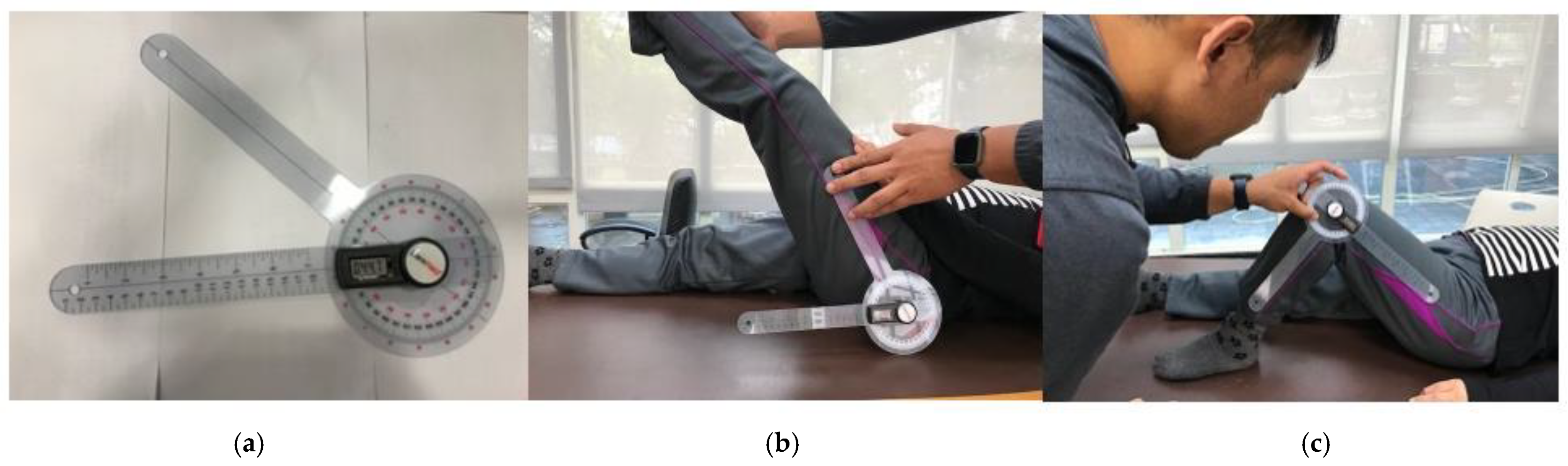
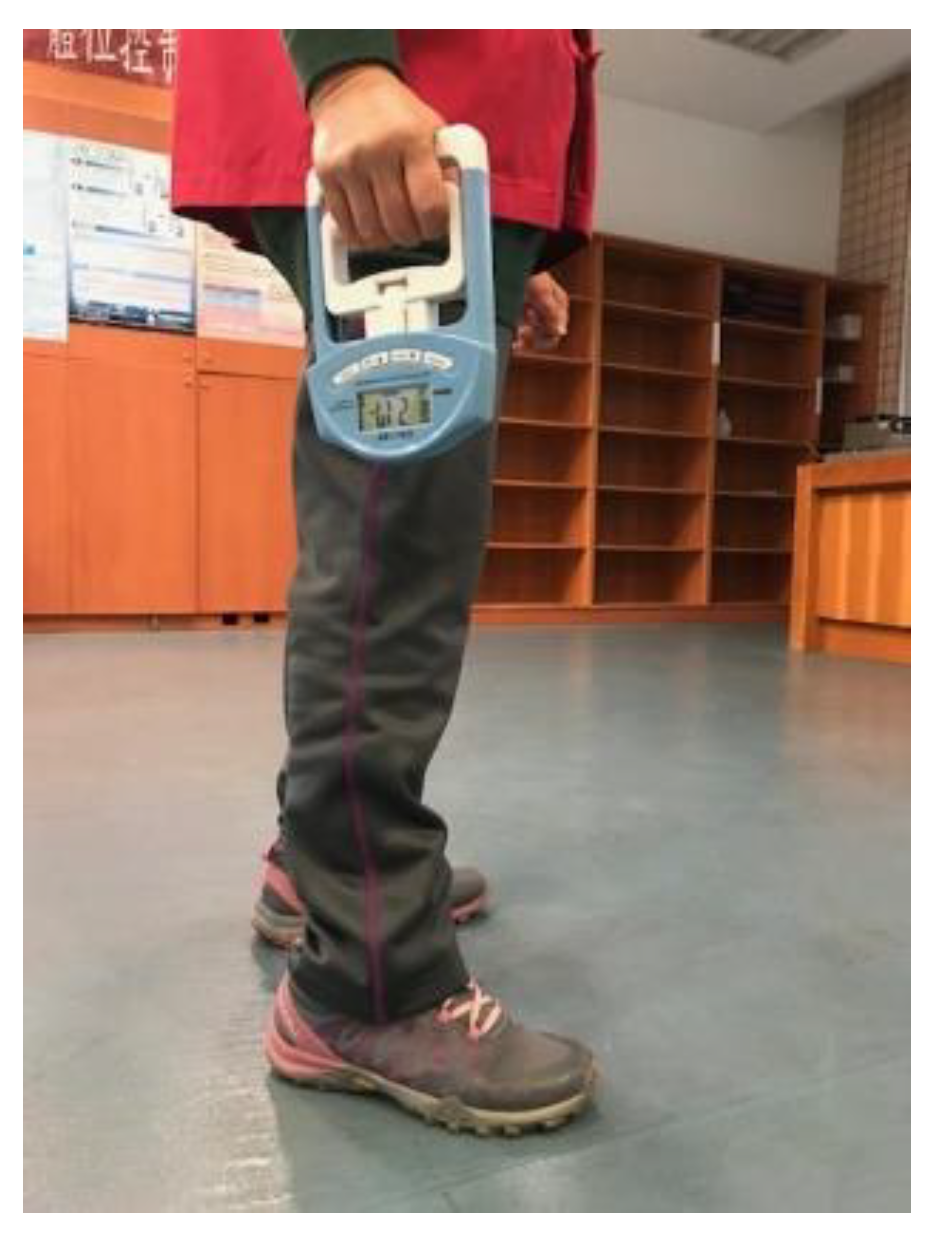
2.3. Apparatus and Measurements
2.4. Statistical Analysis
3. Results
3.1. Range of Joint Motion
3.2. Grip Strength and Gait Speed
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- OECD/WHO. Ratio of people aged 15-64 to people aged over 65 years, 2020 and 2050. In Health at a Glance: Asia/Pacific 2020: Measuring Progress towards Universal Health Coverage; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Ćwirlej-Sozańska, A.; Wiśniowska-Szurlej, A.; Wilmowska-Pietruszyńska, A.; Sozański, B. Determinants of ADL and IADL disability in older adults in southeastern Poland. BMC Geriatr. 2019, 19, 297. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Feldman, M.W. Disability trajectories in activities of daily living of elderly Chinese before death. China Popul. Dev. Stud. 2020, 4, 127–151. [Google Scholar] [CrossRef]
- Filippi, M.; Bar-Or, A.; Piehl, F.; Preziosa, P.; Solari, A.; Vukusic, S.; Rocca, M.A. Multiple sclerosis. Nat. Rev. Dis. Primers 2018, 4, 43. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.F.; Hu, J.L.; Chiou, H. Degrees of shortage and uncovered ratios for long-term care in Taiwan’s regions: Evidence from dynamic DEA. Int. J. Environ. Res. Public Health 2021, 18, 605. [Google Scholar] [CrossRef]
- Hsu, E.; Cohen, S.P. Postamputation pain: Epidemiology, mechanisms, and treatment. J. Pain Res. 2013, 6, 121–136. [Google Scholar] [CrossRef] [Green Version]
- Hirani, V.; Blyth, F.; Naganathan, V.; Le Couteur, D.G.; Seibel, M.J.; Waite, L.M.; Handelsman, D.J.; Cumming, R.G. Sarcopenia is associated with incident disability, institutionalization, and mortality in community-dwelling older men: The concord health and ageing in men project. J. Am. Med. Dir. Assoc. 2015, 16, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Adekoya, A.A.; Guse, L. Wandering behavior from the perspectives of older adults with mild to moderate dementia in long-term care. Res. Gerontol. Nurs. 2019, 12, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Tabira, T.; Hotta, M.; Murata, M.; Yoshiura, K.; Han, G.; Ishikawa, T.; Koyama, A.; Ogawa, N.; Maruta, M.; Ikeda, Y.; et al. Age-related changes in instrumental and basic activities of daily living impairment in older adults with very mild Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. Extra 2020, 10, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Phelan, E.A.; Williams, B.; Penninx, B.W.; LoGerfo, J.P.; Leveille, S.G. Activities of daily living function and disability in older adults in a randomized trial of the health enhancement program. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 838–843. [Google Scholar] [CrossRef] [Green Version]
- He, S.; Craig, B.A.; Xu, H.; Covinsky, K.E.; Stallard, E.; Thomas, J., 3rd; Hass, Z.; Sands, L.P. Unmet need for ADL assistance is associated with mortality among older adults with mild disability. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1128–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwaya, T.; Doi, T.; Seichi, A.; Hoshino, Y.; Ogata, T.; Akai, M. Characteristics of disability in activity of daily living in elderly people associated with locomotive disorders. BMC Geriatr. 2017, 17, 165. [Google Scholar] [CrossRef] [Green Version]
- Liao, W.L.; Chang, Y.H. Age trajectories of disability in instrumental activities of daily living and disability-free life expectancy among middle-aged and older adults in Taiwan: An 11-year longitudinal study. BMC Geriatr. 2020, 20, 530. [Google Scholar] [CrossRef]
- Kim, M.; Won, C.W. Sarcopenia is associated with cognitive impairment mainly due to slow gait speed: Results from the Korean frailty and aging cohort study (KFACS). Int. J. Environ. Res. Public Health 2019, 16, 1491. [Google Scholar] [CrossRef] [Green Version]
- Mile, M.; Balogh, L.; Papp, G.; Pucsok, J.M.; Szabó, K.; Barna, L.; Csiki, Z.; Lekli, I. Effects of functional training on sarcopenia in elderly women in the presence or absence of ACE inhibitors. Int. J. Environ. Res. Public Health 2021, 18, 6594. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Rizzoli, R.; Bruyère, O.; Reginster, J.Y.; Biver, E. Sarcopenia: Burden and challenges for public health. Arch. Public Health 2014, 72, 45. [Google Scholar] [CrossRef] [Green Version]
- Bravo-José, P.; Moreno, E.; Espert, M.; Romeu, M.; Martínez, P.; Navarro, C. Prevalence of sarcopenia and associated factors in institutionalised older adult patients. Clin. Nutr. ESPEN 2018, 27, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef]
- Welch, C.; Hassan-Smith, Z.K.; Greig, C.A.; Lord, J.M.; Jackson, T.A. Acute sarcopenia secondary to hospitalization—An emerging condition affecting older adults. Aging Dis. 2018, 9, 151–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, J.E.; von Haehling, S.; Anker, S.D.; Vellas, B. From sarcopenia to frailty: A road less traveled. J. Cachexia Sarcopenia Muscle 2014, 5, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Rejon, A.I.; Artacho, R.; Puerta, A.; Zuñiga, A.; Ruiz-Lopez, M.D. Diagnosis of sarcopenia in long-term care homes for the elderly: The sensitivity and specificity of two simplified algorithms with respect to the EWGSOP consensus. J. Nutr. Health Aging 2018, 22, 796–801. [Google Scholar] [CrossRef]
- Roquebert, Q.; Sicsic, J.; Santos-Eggimann, B.; Sirven, N.; Rapp, T. Frailty, sarcopenia and long term care utilization in older populations: A systematic review. J. Frailty Aging 2021, 10, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Peel, N.M.; Kuys, S.S.; Klein, K. Gait speed as a measure in geriatric assessment in clinical settings: A systematic review. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 39–46. [Google Scholar] [CrossRef]
- Cadore, E.L.; Casas-Herrero, A.; Zambom-Ferraresi, F.; Idoate, F.; Millor, N.; Gómez, M.; Rodríguez-Mañas, L.; Izquierdo, M. Multicomponent exercises including muscle power training enhance muscle mass, power output, and functional outcomes in institutionalized frail nonagenarians. Age 2014, 36, 773–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooney, J.K.; Law, R.J.; Matschke, V.; Lemmey, A.B.; Moore, J.P.; Ahmad, Y.; Jones, J.G.; Maddison, P.; Thom, J.M. Benefits of exercise in rheumatoid arthritis. J. Aging Res. 2011, 2011, 681640. [Google Scholar] [CrossRef] [Green Version]
- de Souto Barreto, P.; Morley, J.E.; Chodzko-Zajko, W.H.; Pitkala, K.; Weening-Djiksterhuis, E.; Rodriguez-Mañas, L.; Barbagallo, M.; Rosendahl, E.; Sinclair, A.; Landi, F.; et al. Recommendations on physical activity and exercise for older adults living in long-term care facilities: A taskforce report. J. Am. Med. Dir. Assoc. 2016, 17, 381–392. [Google Scholar] [CrossRef]
- Svensson, M.; Lind, V.; Löfgren Harringe, M. Measurement of knee joint range of motion with a digital goniometer: A reliability study. Physiother. Res. Int. 2019, 24, e1765. [Google Scholar] [CrossRef]
- Buchman, A.S.; Leurgans, S.E.; Wang, T.; Schnaider-Beeri, M.; Agarwal, P.; Dawe, R.J.; Delbono, O.; Bennett, D.A. Motor function is the primary driver of the associations of sarcopenia and physical frailty with adverse health outcomes in community-dwelling older adults. PLoS ONE 2021, 16, e0245680. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.G.; Juvanhol, L.L.; Silva-Costa, A.; Longo, G.Z. The mediating role of visceral adiposity in the relationship among schooling, physical inactivity, and unhealthy metabolic phenotype. Am. J. Hum. Biol. 2020, 32, e23425. [Google Scholar] [CrossRef] [PubMed]
- Valamatos, M.J.; Tavares, F.; Santos, R.M.; Veloso, A.P.; Mil-Homens, P. Influence of full range of motion vs. equalized partial range of motion training on muscle architecture and mechanical properties. Eur. J. Appl. Physiol. 2018, 118, 1969–1983. [Google Scholar] [CrossRef] [PubMed]
- Valderrabano, V.; Steiger, C. Treatment and prevention of osteoarthritis through exercise and sports. J. Aging Res. 2011, 2011, 374653. [Google Scholar] [CrossRef] [Green Version]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical activity and exercise: Strategies to manage frailty. Redox. Biol. 2020, 35, 101513. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I. Influence of sarcopenia on the development of physical disability: The cardiovascular health study. J. Am. Geriatr. Soc. 2006, 54, 56–62. [Google Scholar] [CrossRef]
- Valenzuela, T. Efficacy of progressive resistance training interventions in older adults in nursing homes: A systematic review. J. Am. Med. Dir. Assoc. 2012, 13, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Venturelli, M.; Lanza, M. Positive effects of physical training in activity of daily living-dependent older adults. Exp. Aging Res. 2010, 36, 190–205. [Google Scholar] [CrossRef]
- Krist, L.; Dimeo, F.; Keil, T. Can progressive resistance training twice a week improve mobility, muscle strength, and quality of life in very elderly nursing-home residents with impaired mobility? A pilot study. Clin. Interv. Aging 2013, 8, 443. [Google Scholar] [CrossRef] [Green Version]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-related loss of muscle mass and function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, USA, Target Heart Rate and Estimated Maximum Heart Rate. Available online: https://www.cdc.gov/physicalactivity/basics/measuring/heartrate.htm (accessed on 18 January 2022).
- Li, K.W.; Yu, R.-f. Assessment of grip force and subjective hand force exertion under handedness and postural conditions. Appl. Ergon. 2011, 42, 929–933. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Hillside: New York, NY, USA, 1988; pp. 20–26. [Google Scholar]
- Soucie, J.M.; Wang, C.; Forsyth, A.; Funk, S.; Denny, M.; Roach, K.E.; Boone, D.; Hemophilia Treatment Center Network. Range of motion measurements: Reference values and a database for comparison studies. Haemophilia 2011, 17, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Dodge, H.H.; Kadowaki, T.; Hayakawa, T.; Yamakawa, M.; Sekikawa, A.; Ueshima, H. Cognitive impairment as a strong predictor of incident disability in specific ADL-IADL tasks among community-dwelling elders: The Azuchi study. Gerontologist 2005, 45, 222–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medeiros, H.B.; de Araújo, D.S.; de Araújo, C.G. Age-related mobility loss is joint-specific: An analysis from 6000 Flexitest results. Age 2013, 35, 2399–2407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, K.; Doblhammer, G.; Rau, R.; Vaupel, J.W. Ageing populations: The challenges ahead. Lancet 2009, 74, 1196–1208. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.; Yamasaki, M. Association of lower extremity range of motion and muscle strength with physical performance of community-dwelling older women. J. Physiol. Anthropol. 2016, 35, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steultjens, M.P.; Dekker, J.; van Baar, M.E.; Oostendorp, R.A.; Bijlsma, J.W. Range of joint motion and disability in patients with osteoarthritis of the knee or hip. Rheumatology 2000, 39, 955–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beissner, K.L.; Collins, J.E.; Holmes, H. Muscle force and range of motion as predictors of function in older adults. Phys. Ther. 2000, 80, 556–563. [Google Scholar] [CrossRef] [Green Version]
- Bello, A.I.; Ababio, E.; Antwi-Baffoe, S.; Seidu, M.A.; Adjei, D.N. Pain, range of motion and activity level as correlates of dynamic balance among elderly people with musculoskeletal disorder. Ghana Med. J. 2014, 48, 214–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menz, H.B. Biomechanics of the ageing foot and ankle: A mini-review. Gerontology 2015, 61, 381–388. [Google Scholar] [CrossRef]
- Roaas, A.; Andersson, G.B. Normal range of motion of the hip, knee and ankle joints in male subjects, 30-40 years of age. Acta Orthop. Scand. 1982, 53, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Hai, S.; Wang, H.; Cao, L.; Liu, P.; Zhou, J.; Yang, Y.; Dong, B. Association between sarcopenia with lifestyle and family function among community-dwelling Chinese aged 60 years and older. BMC Geriatr. 2017, 17, 187. [Google Scholar] [CrossRef] [PubMed]
- Meuleman, J.R.; Brechue, W.F.; Kubilis, P.S.; Lowenthal, D.T. Exercise Training in the debilitated aged: Strength and functional outcomes. Arch. Phys. Med. Rehabil. 2000, 81, 312–318. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Course | Posture and Motions | Operation Method |
|---|---|---|
| Lower body strength training | Seated (single) knee lift 12 (reps) × 5 (5 sets) | Sit with the body on two-thirds of the chair and lift one foot to the abdomen |
| Upper body strength training | Seated arm curl 12 (reps) × 5 (sets) | Stretch both arms forward and hold a water bottle (0.6 kg) to curl the biceps |
| Aerobic endurance training | 3 min seated marching in place 3 min × 5 (sets) | Sit with two-thirds of the body on the chair, swing hands up and down on both sides of the chair, and step with the feet in place. |
| Stretching of lower limb | Seated with the back of the chair to extend the leg and ankle Left foot, right foot in turn 10 s × 12 (sets) | Raise one leg parallel to the ground, knee straight, tip the ankle up as far as possible, hold for 10 s |
| Stretching of upper limb | Seated shoulder and arm extensions for 10 s × 12 (sets) Seated back and pectoralis major extensions for 10 s × 12 (sets) | 1. Cross both arms up and extend the shoulder joint to the highest point. 2. Extend both arms forward and outward on both sides of the body. |
| Assessment | Content |
|---|---|
| Range of Joint motion | 1. Shoulder ROM: Flexion (0–180°), Extension (0–50°), Abduction (0–180°), Horizontal adduction (0–135°). 2. Elbow ROM: Flexion (0–150°). 3. Wrist ROM: Flexion (0–80°), Extension (0–80°). 4. Hip ROM: Flexion (0–100°), Extension (0–30°), Abduction/Protraction (0–40°), Abduction/Retraction (0–20°). 5. Knee ROM: Flexion (0–150°). 6. Ankle ROM: Plantarflexion (0–50°), Dorsiflexion (0–20°). |
| Sarcopenia | 1. Measure the maximum grip strengths. 2. Measure the gait speed of a 12 m walk test on a flat walkway. |
| Body Part and Movement | Control Group (n = 10) | Experimental Group (n = 10) | Improvement (%) | ||||
|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | p-Value | Pre-Test | Post-Test | p-Value | ||
| Shoulder flexion | 145.1 ± 12.6 | 145.2 ± 12.3 | 0.612 | 140.0 ± 12.5 | 157.0 ± 6.2 | 0.001 | 12.1 |
| Shoulder extension | 36.9 ± 4.9 | 37.0 ± 5.2 | 0.556 | 37.8 ± 3.9 | 42.8 ± 2.8 | 0.003 | 13.2 |
| Shoulder abduction | 136.4 ± 7.7 | 136.7 ± 7.4 | 0.134 | 140.8 ± 6.8 | 146.4 ± 6.2 | 0.002 | 3.8 |
| Shoulder horizontal flexion/ extension | 113.2 ± 5.3 | 113.8 ± 5.4 | 0.068 | 115.4 ± 9.1 | 124.9 ± 7.2 | 0.001 | 8.7 |
| Elbow flexion | 122.4 ± 11.8 | 122.0 ± 11.6 | 0.093 | 122.4 ± 11.7 | 1439.7 ± 9.1 | 0.001 | 14.8 |
| Wrist flexion | 66.4 ± 3.8 | 66.2 ± 3.7 | 0.083 | 64.0 ± 4.3 | 70.2 ± 4.9 | 0.003 | 9.4 |
| Wrist extension | 60.3 ± 3.1 | 60.9 ± 2.7 | 0.058 | 60.2 ± 2.6 | 67.1 ± 2.3 | 0.002 | 11.7 |
| Hip flexion | 67.6 ± 9.7 | 67.2 ± 9.9 | 0.112 | 67.6 ± 9.8 | 75.6 ± 10.6 | 0.004 | 11.8 |
| Hip extension | 18.2 ± 3.2 | 18.1 ± 3.2 | 0.574 | 18.3 ± 3.1 | 26.1 ± 3.0 | 0.001 | 52.9 |
| Hip abduction/protraction | 31.1 ± 2.4 | 31.2 ± 2.6 | 0.327 | 33.5 ± 3.2 | 42.1 ± 1.5 | 0.003 | 27.3 |
| Hip adduction/retraction | 10.2 ± 1.5 | 10.3 ± 1.6 | 0.276 | 10.1 ± 2.1 | 17.1 ± 2.3 | 0.001 | 71 |
| Knee flexion | 93.2 ± 8.4 | 94.6 ± 8.2 | 0.557 | 97.1 ± 8.4 | 114.9 ± 8.2 | 0.001 | 23.5 |
| Ankle plantarflexion | 35.7 ± 3.5 | 36.4 ± 3.4 | 0.077 | 35.9 ± 3.7 | 42.6 ± 2.1 | 0.003 | 19.4 |
| Ankle dorsiflexion | 8.5 ± 1.8 | 8.4 ± 1.5 | 0.486 | 9.1 ± 1.9 | 12.6 ± 1.9 | 0.001 | 44.4 |
| Body Part and Movement | Control Group (n = 10) | Experimental Group (n = 10) | Improvement (%) | ||||
|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | p-Value | Pre-Test | Post-Test | p-Value | ||
| Shoulder flexion | 139.1 ± 11.4 | 139.0 ± 11.5 | 0.449 | 139.4 ± 9.8 | 158.8 ± 7.5 | 0.001 | 13.6 |
| Shoulder extension | 36.6 ± 5.2 | 36.3 ± 5.5 | 0.437 | 37.2 ± 6.2 | 42.7 ± 4.1 | 0.007 | 16.2 |
| Shoulder abduction | 137.7 ± 7.4 | 138.5 ± 7.7 | 0.086 | 137.9 ± 8.4 | 152.3 ± 3.4 | 0.004 | 10.4 |
| Shoulder horizontal flexion/ extension | 118.6 ± 9.3 | 118.8 ± 9.2 | 0.257 | 115.8 ± 6.6 | 125.0 ± 5.0 | 0.008 | 7.8 |
| Elbow flexion | 108.9 ± 10.4 | 108.7 ± 10.0 | 0.362 | 110.2 ± 10.4 | 141.9 ± 5.0 | 0.003 | 29.1 |
| Wrist flexion | 58.8 ± 3.0 | 58.7 ± 3.1 | 0.163 | 57.8 ± 4.2 | 67.4 ± 4.0 | 0.004 | 15.5 |
| Wrist extension | 60.1 ± 2.6 | 60.4 ± 2.8 | 0.059 | 60.2 ± 2.4 | 67.9 ± 1.8 | 0.001 | 13.3 |
| Hip flexion | 60.8 ± 11.7 | 60.5 ± 11.6 | 0.485 | 60.4 ± 11.6 | 72.4 ± 8.1 | 0.002 | 20.0 |
| Hip extension | 18.9 ± 2.8 | 19.1 ± 2.47 | 0.313 | 18.4 ± 2.9 | 25.9 ± 2.1 | 0.001 | 44.4 |
| Hip abduction/protraction | 33.8 ± 3.7 | 33.9 ± 3.8 | 0.868 | 32.5 ± 2.6 | 40.5 ± 3.3 | 0.004 | 24.2 |
| Hip adduction/retraction | 10.3 ± 1.6 | 10.2 ± 1.6 | 0.513 | 10.2 ± 1.5 | 17.5 ± 2.1 | 0.001 | 75.0 |
| Knee flexion | 105.3 ± 4.1 | 105.7 ± 3.9 | 0.121 | 105.1 ± 3.3 | 120.8 ± 2.6 | 0.001 | 15.0 |
| Ankle plantarflexion | 36.1 ± 4.7 | 36.2 ± 4.7 | 0.717 | 35.6 ± 4.4 | 42.9 ± 2.5 | 0.001 | 22.9 |
| Ankle dorsiflexion | 9.2 ± 1.5 | 9.1 ± 1.2 | 0.375 | 8.9 ± 1.2 | 13.6 ± 1.8 | 0.003 | 75.0 |
| Variables | Control Group (n = 10) | Experimental Group (n = 10) | Improvement (%) | ||||
|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | p-Value | Pre-Test | Post-Test | p-Value | ||
| Males HS (kgf) | 6.2 ± 0.9 | 6.3 ± 0.9 | 0.085 | 7.1 ± 0.5 | 8.6 ± 0.6 | 0.001 | 20.3 |
| Females HS (kgf) | 6.0 ± 0.6 | 6.0 ± 0.7 | 0.432 | 6.0 ± 0.8 | 7.6 ± 1.1 | 0.003 | 25.4 |
| Males GS (m/s) | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.057 | 0.4 ± 0.1 | 0.6 ± 0.1 | 0.004 | 50.0 |
| Females GS (m/s) | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.109 | 0.5 ± 0.1 | 0.6 ± 0.1 | 0.004 | 22.9 |
| Improvement (%) | SF | EF | WF | WE | HF | HE | KF | AP | AD |
|---|---|---|---|---|---|---|---|---|---|
| Males HS | 0.77 * | 0.87 * | 0.72 * | 0.65 * | - | - | - | - | - |
| Females HS | 0.73 * | 0.75 * | 0.83 * | 0.77 * | - | - | - | - | - |
| Males GS | - | - | - | - | 0.62 * | 0.69 * | 0.81 * | 0.66 * | 0.69 * |
| Females GS | - | - | - | - | 0.67 * | 0.65 * | 0.82 * | 0.62 * | 0.74 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-E.; Li, K.W.; Chia, F.; Huang, W.-Y. Interventions to Improve Physical Capability of Older Adults with Mild Disabilities: A Case Study. Int. J. Environ. Res. Public Health 2022, 19, 2651. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052651
Wu C-E, Li KW, Chia F, Huang W-Y. Interventions to Improve Physical Capability of Older Adults with Mild Disabilities: A Case Study. International Journal of Environmental Research and Public Health. 2022; 19(5):2651. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052651
Chicago/Turabian StyleWu, Cheng-En, Kai Way Li, Fan Chia, and Wei-Yang Huang. 2022. "Interventions to Improve Physical Capability of Older Adults with Mild Disabilities: A Case Study" International Journal of Environmental Research and Public Health 19, no. 5: 2651. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052651