
Emergency Use and Efficacy of an Asynchronous Teledermatology System as a Novel Tool for Early Diagnosis of Skin Cancer during the First Wave of COVID-19 Pandemic

 , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Data
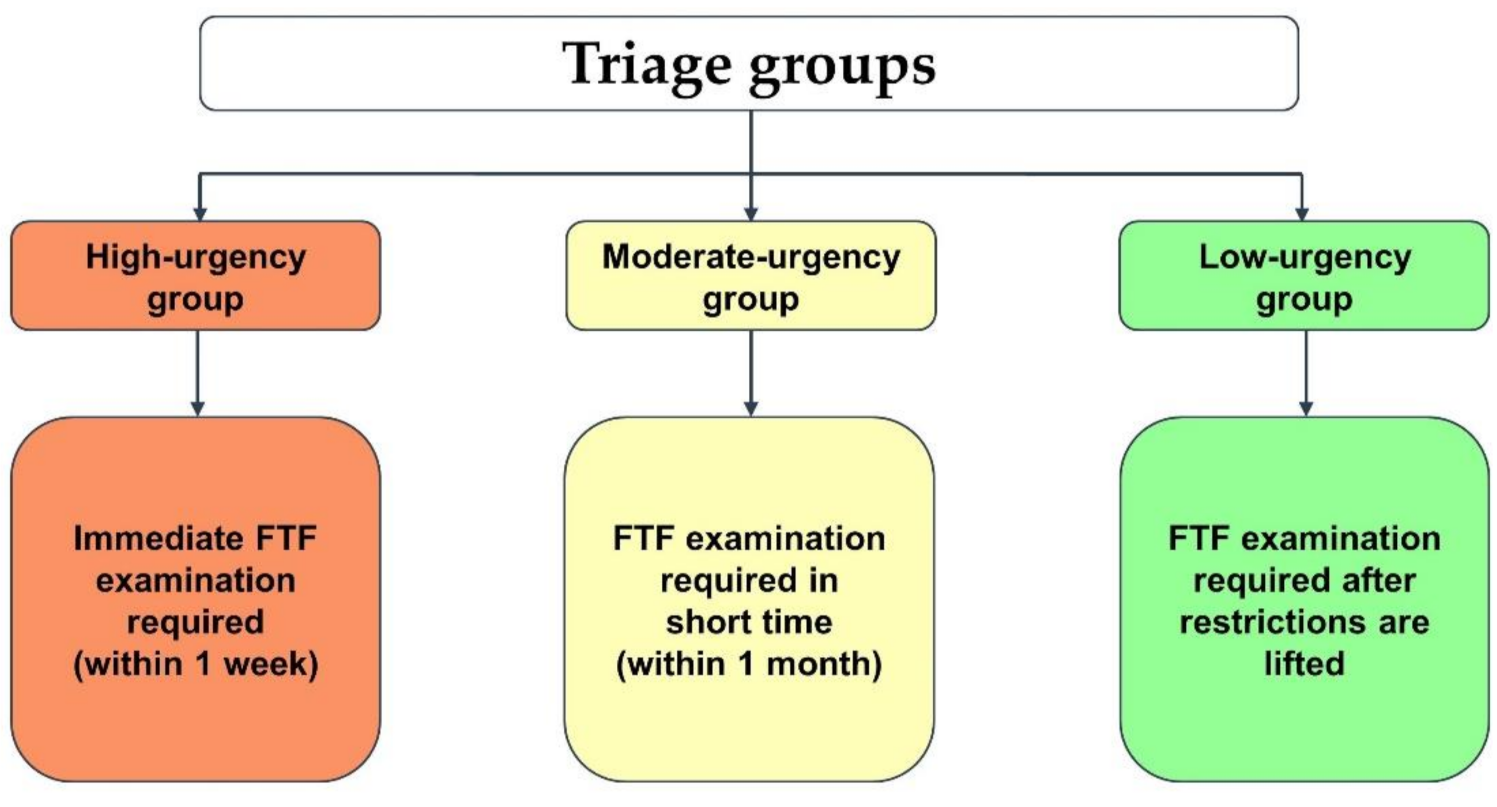
2.2. Diagnostic and Triage Groups
2.3. Outcome Measures
2.4. Statistical Analyses
2.5. Inclusion Criteria
2.6. Exclusion Criteria
3. Results
3.1. Patient Data
3.2. Triage Groups
3.3. Overall Primary and Aggregated Diagnostic Agreement
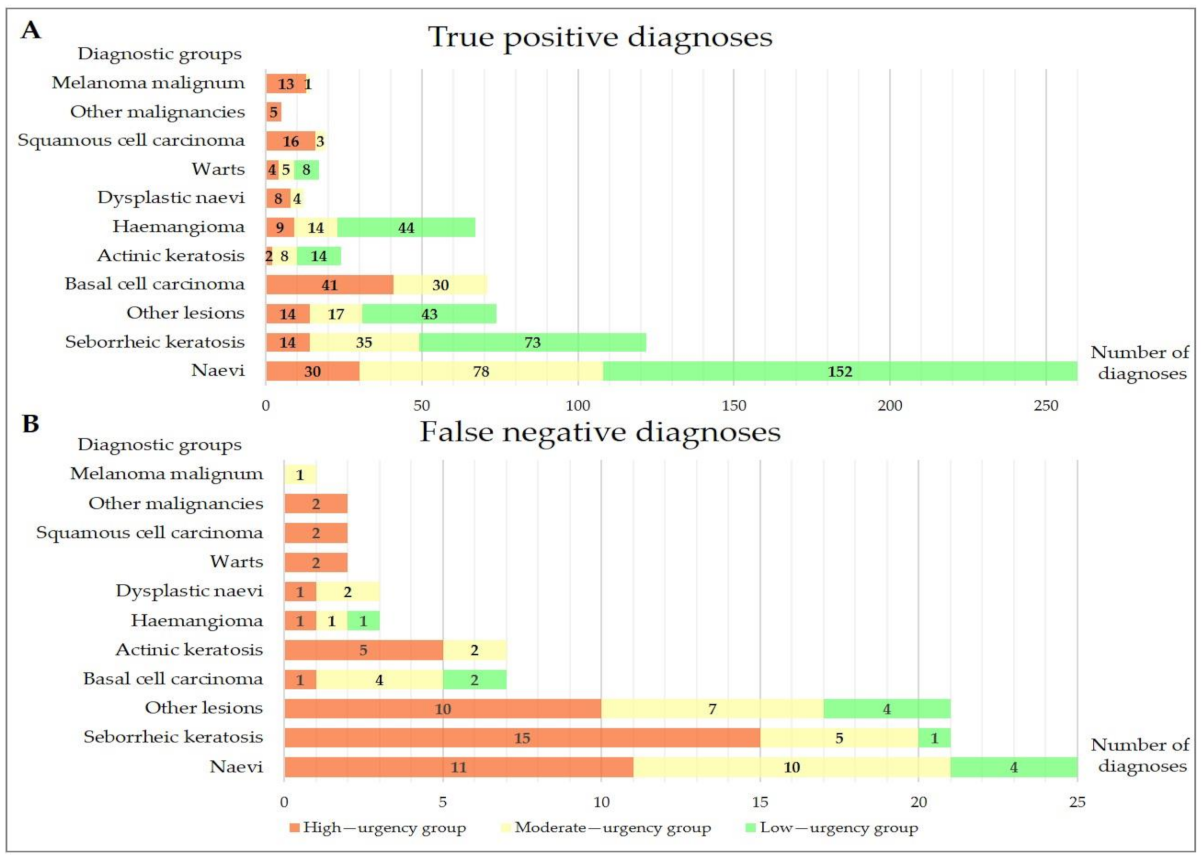
3.4. Diagnostic Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valentino, L.A.; Skinner, M.W.; Pipe, S.W. The role of telemedicine in the delivery of health care in the COVID-19 pandemic. Haemophilia 2020, 26, e230–e231. [Google Scholar] [CrossRef] [PubMed]
- Merkely, B.; Szabo, A.J.; Kosztin, A.; Berenyi, E.; Sebestyen, A.; Lengyel, C.; Merkely, G.; Karady, J.; Varkonyi, I.; Papp, C.; et al. Novel coronavirus epidemic in the Hungarian population, a cross-sectional nationwide survey to support the exit policy in Hungary. Geroscience 2020, 42, 1063–1074. [Google Scholar] [CrossRef] [PubMed]
- Bhaskar, S.; Nurtazina, A.; Mittoo, S.; Banach, M.; Weissert, R. Editorial: Telemedicine During and Beyond COVID-19. Front. Public Health 2021, 9, 662617. [Google Scholar] [CrossRef]
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef]
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med. Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, K.; Mabrouk, A.; Jain, V.K.; Venkatesan, A.; Vaishya, R. Learning opportunities from COVID-19 and future effects on health care system. Diabetes Metab. Syndr. 2020, 14, 943–946. [Google Scholar] [CrossRef] [PubMed]
- Hincapié, M.A.; Gallego, J.C.; Gempeler, A.; Piñeros, J.A.; Nasner, D.; Escobar, M.F. Implementation and Usefulness of Telemedicine During the COVID-19 Pandemic: A Scoping Review. J Prim. Care Community Health 2020, 11, 2150132720980612. [Google Scholar] [CrossRef]
- Patel, S.Y.; Mehrotra, A.; Huskamp, H.A.; Uscher-Pines, L.; Ganguli, I.; Barnett, M.L. Trends in Outpatient Care Delivery and Telemedicine During the COVID-19 Pandemic in the US. JAMA Intern. Med. 2021, 181, 388–391. [Google Scholar] [CrossRef]
- Tensen, E.; van der Heijden, J.P.; Jaspers, M.W.; Witkamp, L. Two Decades of Teledermatology: Current Status and Integration in National Healthcare Systems. Curr. Dermatol. Rep. 2016, 5, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, R.S.; Krupinski, E.A.; Doarn, C.R. Clinical Examination Component of Telemedicine, Telehealth, mHealth, and Connected Health Medical Practices. Med. Clin. North Am. 2018, 102, 533–544. [Google Scholar] [CrossRef]
- North, S. Telemedicine in the Time of COVID and Beyond. J. Adolesc. Health 2020, 67, 145–146. [Google Scholar] [CrossRef]
- Ramirez, A.V.; Ojeaga, M.; Espinoza, V.; Hensler, B.; Honrubia, V. Telemedicine in Minority and Socioeconomically Disadvantaged Communities Amidst COVID-19 Pandemic. Otolaryngol. Head Neck Surg. 2021, 164, 91–92. [Google Scholar] [CrossRef]
- Rodriguez Socarrás, M.; Loeb, S.; Teoh, J.Y.; Ribal, M.J.; Bloemberg, J.; Catto, J.; N’Dow, J.; Van Poppel, H.; Gómez Rivas, J. Telemedicine and Smart Working: Recommendations of the European Association of Urology. Eur. Urol. 2020, 78, 812–819. [Google Scholar] [CrossRef] [PubMed]
- Gillman-Wells, C.C.; Sankar, T.K.; Vadodaria, S. COVID-19 Reducing the Risks: Telemedicine is the New Norm for Surgical Consultations and Communications. Aesthetic Plast. Surg. 2021, 45, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Cantor, J.H.; McBain, R.K.; Pera, M.F.; Bravata, D.M.; Whaley, C.M. Who Is (and Is Not) Receiving Telemedicine Care During the COVID-19 Pandemic. Am. J. Prev. Med. 2021, 61, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Mehrtens, S.H.; Shall, L.; Halpern, S.M. A 14-year review of a UK teledermatology service: Experience of over 40,000 teleconsultations. Clin. Exp. Dermatol. 2019, 44, 874–881. [Google Scholar] [CrossRef]
- Barros-Tornay, R.; Ferrándiz, L.; Martín-Gutiérrez, F.J.; Fernández-Orland, A.; Serrano-Gotarredona, A.; de la Torre, J.M.; Conejo-Mir, M.D.; Ojeda-Vila, T.; Márquez-Enríquez, J.; Hernández, C.; et al. Feasibility and cost of a telemedicine-based short-term plan for initial access in general dermatology in Andalusia, Spain. JAAD Int. 2021, 4, 52–57. [Google Scholar] [CrossRef]
- Moscarella, E.; Pasquali, P.; Cinotti, E.; Tognetti, L.; Argenziano, G.; Rubegni, P. A survey on teledermatology use and doctors’ perception in times of COVID-19. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e772–e773. [Google Scholar] [CrossRef]
- Conforti, C.; Lallas, A.; Argenziano, G.; Dianzani, C.; Di Meo, N.; Giuffrida, R.; Kittler, H.; Malvehy, J.; Marghoob, A.A.; Soyer, H.P.; et al. Impact of the COVID-19 Pandemic on Dermatology Practice Worldwide: Results of a Survey Promoted by the International Dermoscopy Society (IDS). Dermatol. Pract. Concept. 2021, 11, e2021153. [Google Scholar] [CrossRef]
- Bhargava, S.; McKeever, C.; Kroumpouzos, G. Impact of COVID-19 pandemic on dermatology practices: Results of a web-based, global survey. Int. J. Womens Dermatol. 2021, 7, 217–223. [Google Scholar] [CrossRef]
- Giavina Bianchi, M.; Santos, A.; Cordioli, E. Dermatologists’ perceptions on the utility and limitations of teledermatology after examining 55,000 lesions. J. Telemed. Telecare 2021, 27, 166–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazi, R.; Evankovich, M.R.; Liu, R.; Liu, A.; Moorhead, A.; Ferris, L.K.; Falo, L.D., Jr.; English, J.C., 3rd. Utilization of Asynchronous and Synchronous Teledermatology in a Large Health Care System During the COVID-19 Pandemic. Telemed. J. eHealth 2021, 27, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Brinker, T.J.; Hekler, A.; von Kalle, C.; Schadendorf, D.; Esser, S.; Berking, C.; Zacher, M.T.; Sondermann, W.; Grabe, N.; Steeb, T.; et al. Teledermatology: Comparison of Store-and-Forward Versus Live Interactive Video Conferencing. J. Med. Internet Res. 2018, 20, e11871. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Wu, J.; Kovarik, C.L.; Goldyne, M.E.; Oh, D.H.; McKoy, K.C.; Shippy, A.M.; Pak, H.S. State of teledermatology programs in the United States. J. Am. Acad. Dermatol. 2012, 67, 939–944. [Google Scholar] [CrossRef]
- Lowe, A.; Atwan, A.; Mills, C. Teledermoscopy as a community based diagnostic test in the era of COVID-19? Clin. Exp. Dermatol. 2021, 46, 173–174. [Google Scholar] [CrossRef]
- Teuscher, M.; Diehl, K.; Schaarschmidt, M.L.; Weilandt, J.; Sasama, B.; Ohletz, J.; Könnecke, A.; Harth, W.; Hillen, U.; Peitsch, W.K. Effects of the COVID-19 pandemic on care of melanoma patients in Berlin, Germany: The Mela-COVID survey. Eur. J. Dermatol. 2021, 31, 521–529. [Google Scholar] [CrossRef]
- Gomolin, T.; Cline, A.; Handler, M.Z. The danger of neglecting melanoma during the COVID-19 pandemic. J. Dermatol. Treat. 2020, 31, 444–445. [Google Scholar] [CrossRef] [PubMed]
- Marson, J.W.; Maner, B.S.; Harding, T.P.; Meisenheimer, J.V.; Solomon, J.A.; Leavitt, M.; Levin, N.J.; Dellavalle, R.; Brooks, I.; Rigel, D.S. The magnitude of COVID-19’s effect on the timely management of melanoma and nonmelanoma skin cancers. J. Am. Acad. Dermatol. 2021, 84, 1100–1103. [Google Scholar] [CrossRef]
- Hoellwerth, M.; Kaiser, A.; Emberger, M.; Brandlmaier, M.; Laimer, M.; Egger, A.; Bauer, J.W.; Koelblinger, P. COVID-19-Induced Reduction in Primary Melanoma Diagnoses: Experience from a Dermatopathology Referral Center. J. Clin. Med. 2021, 10, 59. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Cazzaniga, S.; Di Leo, S.; Piaserico, S.; Bellinato, F.; Pizzolato, M.; Gatti, A.; Eccher, A.; Brunelli, M.; Saraggi, D.; et al. Impact of the COVID-19 pandemic on melanoma diagnosis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e714–e715. [Google Scholar] [CrossRef]
- Silveira, C.; Carcano, C.; Mauad, E.; Faleiros, H.; Filho, A. Cell phone usefulness to improve the skin cancer screening: Preliminary results and critical analysis of mobile app development. Rural Remote Health 2019, 19, 4895. [Google Scholar] [CrossRef] [PubMed]
- Chuchu, N.; Dinnes, J.; Takwoingi, Y.; Matin, R.N.; Bayliss, S.E.; Davenport, C.; Moreau, J.F.; Bassett, O.; Godfrey, K.; O’Sullivan, C.; et al. Teledermatology for diagnosing skin cancer in adults. Cochrane Database Syst. Rev. 2018, 12, CD013193. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, J.S.; Nelson, C.A.; James, W.D.; Margolis, D.J.; Littman-Quinn, R.; Kovarik, C.L.; Rosenbach, M. The reliability of teledermatology to triage inpatient dermatology consultations. JAMA Dermatol. 2014, 150, 419–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giavina-Bianchi, M.; Santos, A.P.; Cordioli, E. Teledermatology reduces dermatology referrals and improves access to specialists. EClinicalMedicine 2020, 29–30, 100641. [Google Scholar] [CrossRef] [PubMed]
- Warshaw, E.M.; Lederle, F.A.; Grill, J.P.; Gravely, A.A.; Bangerter, A.K.; Fortier, L.A.; Bohjanen, K.A.; Chen, K.; Lee, P.K.; Rabinovitz, H.S.; et al. Accuracy of teledermatology for pigmented neoplasms. J. Am. Acad. Dermatol. 2009, 61, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Ramirez, D.; Ferrandiz, L.; Nieto-Garcia, A.; Carrasco, R.; Moreno-Alvarez, P.; Galdeano, R.; Bidegain, E.; Rios-Martin, J.J.; Camacho, F.M. Store-and-forward teledermatology in skin cancer triage: Experience and evaluation of 2009 teleconsultations. Arch. Dermatol. 2007, 143, 479–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Yeboah, C.B.; Harvey, N.; Krishnan, R.; Lipoff, J.B. The Impact of COVID-19 on Teledermatology: A Review. Dermatol. Clin. 2021, 39, 599–608. [Google Scholar] [CrossRef]
- Temiz, S.A.; Dursun, R.; Daye, M.; Ataseven, A. Evaluation of dermatology consultations in the era of COVID-19. Dermatol. Ther. 2020, 33, e13642. [Google Scholar] [CrossRef] [PubMed]
- Kravets, K.; Vasylenko, O.; Dranyk, Z.; Bogomolets, O. Store-and-forward teledermatology for the most common skin neoplasms in Ukraine. Acta Derm. Alp. Pannonica Adriat. 2018, 27, 79–83. [Google Scholar] [CrossRef]
- Congalton, A.T.; Oakley, A.M.; Rademaker, M.; Bramley, D.; Martin, R.C. Successful melanoma triage by a virtual lesion clinic (teledermatoscopy). J. Eur. Acad. Dermatol. Venereol. 2015, 29, 2423–2428. [Google Scholar] [CrossRef] [PubMed]
- Massone, C.; Maak, D.; Hofmann-Wellenhof, R.; Soyer, H.P.; Frühauf, J. Teledermatology for skin cancer prevention: An experience on 690 Austrian patients. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Singhal, R.R.; Talati, K.N.; Gandhi, B.P.; Shinde, M.K.; Nair, P.A.; Phatak, A.G. Prevalence and Pattern of Skin Diseases in Tribal Villages of Gujarat: A Teledermatology Approach. Indian J. Community Med. 2020, 45, 199–203. [Google Scholar] [CrossRef]
- Gimeno-Vicente, M.; Alfaro-Rubio, A.; Gimeno-Carpio, E. Teledermatology by WhatsApp in Valencia: Characteristics of Remote Consultation and Its Emotional Impact on the Dermatologist. Actas Dermosifiliogr. 2020, 111, 364–380. [Google Scholar] [CrossRef]
- Ncube, B.; Mars, M.; Scott, R.E. The need for a telemedicine strategy for Botswana? A scoping review and situational assessment. BMC Health Serv. Res. 2020, 20, 794. [Google Scholar] [CrossRef] [PubMed]
- Jakhar, D.; Kaul, S.; Kaur, I. WhatsApp messenger as a teledermatology tool during coronavirus disease (COVID-19): From bedside to phone-side. Clin. Exp. Dermatol. 2020, 45, 739–740. [Google Scholar] [CrossRef] [Green Version]
- Kroemer, S.; Frühauf, J.; Campbell, T.M.; Massone, C.; Schwantzer, G.; Soyer, H.P.; Hofmann-Wellenhof, R. Mobile teledermatology for skin tumour screening: Diagnostic accuracy of clinical and dermoscopic image tele-evaluation using cellular phones. Br. J. Dermatol. 2011, 164, 973–979. [Google Scholar] [CrossRef]
- Lamel, S.A.; Haldeman, K.M.; Ely, H.; Kovarik, C.L.; Pak, H.; Armstrong, A.W. Application of mobile teledermatology for skin cancer screening. J. Am. Acad. Dermatol. 2012, 67, 576–581. [Google Scholar] [CrossRef]
- Giavina-Bianchi, M.; Azevedo, M.F.D.; Sousa, R.M.; Cordioli, E. Part II: Accuracy of Teledermatology in Skin Neoplasms. Front. Med. 2020, 7, 845. [Google Scholar] [CrossRef]
- Finnane, A.; Dallest, K.; Janda, M.; Soyer, H.P. Teledermatology for the Diagnosis and Management of Skin Cancer: A Systematic Review. JAMA Dermatol. 2017, 153, 319–327. [Google Scholar] [CrossRef] [Green Version]
- Silveira, C.E.; Silva, T.B.; Fregnani, J.H.; da Costa Vieira, R.A.; Haikel, R.L., Jr.; Syrjänen, K.; Carvalho, A.L.; Mauad, E.C. Digital photography in skin cancer screening by mobile units in remote areas of Brazil. BMC Dermatol. 2014, 14, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotes, M.E.; Daugherty, L.N.; Sargen, M.R.; Chen, S.C. Diagnostic accuracy of teledermatology for nonmelanoma skin cancer: Can patients be referred directly for surgical management? J. Am. Acad. Dermatol. 2021, 85, 464–466. [Google Scholar] [CrossRef] [PubMed]
- Şenel, E.; Baba, M.; Durdu, M. The contribution of teledermatoscopy to the diagnosis and management of non-melanocytic skin tumours. J. Telemed. Telecare 2013, 19, 60–63. [Google Scholar] [CrossRef]
- Manahan, M.N.; Soyer, H.P.; Loescher, L.J.; Horsham, C.; Vagenas, D.; Whiteman, D.C.; Olsen, C.M.; Janda, M. A pilot trial of mobile, patient-performed teledermoscopy. Br. J. Dermatol. 2015, 172, 1072–1080. [Google Scholar] [CrossRef] [Green Version]
- Arzberger, E.; Curiel-Lewandrowski, C.; Blum, A.; Chubisov, D.; Oakley, A.; Rademaker, M.; Soyer, H.; Hofmann-Wellenhof, R. Teledermoscopy in High-risk Melanoma Patients: A Comparative Study of Face-to-face and Teledermatology Visits. Acta Derm. Venereol. 2016, 96, 779–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knudsen, K.E.; Willman, C.; Winn, R. Optimizing the Use of Telemedicine in Oncology Care: Postpandemic Opportunities. Clin. Cancer Res. 2021, 27, 933–936. [Google Scholar] [CrossRef]
- Hsiao, J.L.; Oh, D.H. The impact of store-and-forward teledermatology on skin cancer diagnosis and treatment. J. Am. Acad. Dermatol. 2008, 59, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Ramírez, D.; Romero-Aguilera, G. Teledermatology: From the Tempest of Debate to Calmer Waters. Actas Dermosifiliogr. 2016, 107, 366–368. [Google Scholar] [CrossRef]
- Bozsányi, S.; Farkas, K.; Bánvölgyi, A.; Lőrincz, K.; Fésűs, L.; Anker, P.; Zakariás, S.; Jobbágy, A.; Lihacova, I.; Lihachev, A.; et al. Quantitative Multispectral Imaging Differentiates Melanoma from Seborrheic Keratosis. Diagnostics 2021, 11, 1315. [Google Scholar] [CrossRef]
- Carrera, C. The Many Faces of Seborrheic Keratosis. Actas Dermosifiliogr. 2019, 110, 338. [Google Scholar] [CrossRef]
- Moreno-Ramírez, D.; Raya-Maldonado, J.; Morales-Conde, M.; Ojeda-Vila, T.; Martín-Gutiérrez, F.J.; Ruíz-de-Casas, A.; Fernández-Orland, A.; Jm, H.E.; Ferrándiz, L. Increasing Frequency of Seborrheic Keratosis Diagnoses as a Favorable Consequence of Teledermatology-Based Skin Cancer Screening: A Cross-sectional Study of 34,553 Patients. Am. J. Clin. Dermatol. 2017, 18, 681–685. [Google Scholar] [CrossRef] [PubMed]
- Betlloch-Mas, I.; Martínez-Miravete, M.T.; Berbegal-DeGracia, L.; Sánchez-Vázquez, L.; Sánchez-Payá, J. Teledermatology in paediatrics: Health-care impact on the early treatment of infantile haemangiomas. J. Telemed. Telecare 2021, 27, 424–430. [Google Scholar] [CrossRef]
- Warshaw, E.M.; Gravely, A.A.; Nelson, D.B. Reliability of store and forward teledermatology for skin neoplasms. J. Am. Acad. Dermatol. 2015, 72, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Clarke, E.L.; Reichenberg, J.S.; Ahmed, A.M.; Keeling, B.; Custer, J.; Rathouz, P.J.; Jambusaria-Pahlajani, A. The utility of teledermatology in the evaluation of skin lesions. J. Telemed. Telecare 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Diagnostic Groups |
|---|
| Malignant melanoma |
| Squamous cell carcinoma |
| Basal cell carcinoma |
| Other malignancies |
| Actinic keratosis |
| Dysplastic naevi |
| Naevi |
| Seborrheic keratosis |
| Haemnagioma |
| Warts |
| Other lesions |
| Variables | No. |
|---|---|
| Age composition | |
| 0–19 | 87 (11.6%) |
| 20–39 | 225 (30.0%) |
| 40–59 | 245 (32.7%) |
| 60–79 | 164 (21.9%) |
| 80≤ | 28 (3.7%) |
| Sex | |
| Female | 474 (63.3%) |
| Male | 275 (36.7%) |
| Ethnicity | |
| Caucasian | 744 (99.3%) |
| Others | 5 (0.7%) |
| Lesion location | |
| Head/neck | 193 (24.8%) |
| Hand/arm | 117 (15.0%) |
| Trunk | 350 (44.9%) |
| Leg/foot | 103 (13.2%) |
| Buttock/groin | 16 (2.1%) |
| PD/AD | Accuracy (95% CI) | Cohen’s Kappa (95% CI) |
|---|---|---|
| Malignant lesions | ||
| PD | 86.3% (84.1–88.7%) | 0.647 (0.574–0.720) |
| AD | 85.3% (82.9–87.9%) | 0.644 (0.572–0.716) |
| Non-malignant lesions | ||
| PD | 81.3% (78.6–84.0%) | 0.811 (0.790–0.830) |
| AD | 86.5% (84.1–88.9%) | 0.790 (0.769–0.810) |
| Total lesions | ||
| PD | 81.2% (78.4–83.8%) | 0.769 (0.747–0.792) |
| AD | 87.9% (85.5–90.0%) | 0.754 (0.722–0.776) |
| PD/AD | No. of Diagnoses during TDC | TP | FN | Cohen’s Kappa (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Malignant melanoma | ||||||||
| PD | 32 | 10 | 5 | 0.410 (0.231–0.589) | 66.7% (41.7–84.8%) | 97.1% (95.7–98.1%) | 31.3% (18.0–48.6%) | 99.3% (98.44–99.7%) |
| AD | 42 | 14 | 1 | 0.476 (0.317–0.636) | 93.3% (70.2–99.7%) | 96.3% (94.8–97.5%) | 33.3% (21.0–48.5%) | 99.9% (99.2–100.0%) |
| Squamous cell carcinoma | ||||||||
| PD | 36 | 13 | 8 | 0.437 (0.273–0.600) | 61.9% (40.9–79.3%) | 97.0% (95.5–98.0%) | 36.1% (22.5–52.4%) | 98.9% (97.9–99.5%) |
| AD | 45 | 19 | 2 | 0.560 (0.415–0.704) | 90.5% (71.1–98.3%) | 96.6% (95.0–97.7%) | 42.2% (29.0–56.7%) | 99.7% (99.0–100.0%) |
| Basal cell carcinoma | ||||||||
| PD | 98 | 70 | 8 | 0.770 (0.698–0.842) | 89.7% (81.1–94.7%) | 96.0% (94.3–97.2%) | 71.4% (61.8–79.4%) | 98.8% (97.7–99.4%) |
| AD | 112 | 71 | 7 | 0.714 (0.638–0.789) | 91.00% (82.6–95.6%) | 94.2% (92.2–95.7%) | 63.4% (54.2–71.7%) | 99.00% (97.9–99.5%) |
| Other malignancies | ||||||||
| PD | 8 | 5 | 2 | 0.663 (0.386–0.941) | 71.4% (35.9–94.9%) | 99.6% (98.9–99.9%) | 62.5% (30.6–86.3%) | 99.7% (99.1–99.9%) |
| AD | 8 | 5 | 2 | 0.663 (0.386–0.941) | 71.4% (35.9–94.9%) | 99.6% (98.9–99.9%) | 62.5% (30.6–86.3%) | 99.7% (99.1–100.0%) |
| Actinic keratosis | ||||||||
| PD | 25 | 20 | 11 | 0.704 (0.566–0.842) | 64.5% (47.0–78.9%) | 99.3% (98.4–99.7%) | 80.0% (60.9–91.1%) | 98.5% (97.4–99.2%) |
| AD | 33 | 24 | 7 | 0.739 (0.617–0.862) | 77.4% (60.2–88.6%) | 98.8% (97.7–99.4%) | 72.7% (55.8–84.9%) | 99.1% (98.1–99.5%) |
| PD/AD | No. of Diagnoses during TDC | TP | FN | Cohen’s Kappa (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Dysplastic naevi | ||||||||
| PD | 38 | 12 | 3 | 0.437 (0.270–0.605) | 80.0% (54.8–93.0%) | 96.6% (95.1–97.7%) | 31.6% (19.1–47.5%) | 99.6% (98.8–99.9%) |
| AD | 46 | 12 | 3 | 0.375 (0.220–0.530) | 80.0% (54.8–93.0%) | 95.50% (93.9–96.8%) | 26.10% (15.6–40.3%) | 99.6% (98.8–99.9%) |
| Naevi | ||||||||
| PD | 265 | 248 | 37 | 0.848 (0.809–0.887) | 87.0% (82.6–90.4%) | 96.6% (94.6–97.8%) | 93.6% (90.0–96.0%) | 92.8% (90.2–94.7%) |
| AD | 290 | 260 | 25 | 0.848 (0.810–0.887) | 91.2% (87.4–94.0%) | 93.9% (91.5–95.7%) | 89.7% (85.6–92.7%) | 94.9% (92.6–96.5%) |
| PD/AD | No. of Diagnoses during TDC | TP | FN | Cohen’s Kappa (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Seborrheic keratosis | ||||||||
| PD | 123 | 112 | 31 | 0.810 (0.754–0.865) | 78.3% (70.9–84.3%) | 98.3% (96.9–99.0%) | 91.10% (84.7–94.9%) | 95.30% (93.4–96.7%) |
| AD | 154 | 122 | 21 | 0.780 (0.723–0.836) | 85.3% (78.6–90.2%) | 95.0% (93.0–96.4%) | 79.2% (72.1–84.9%) | 96.6% (94.9–97.8%) |
| Haemangiomas | ||||||||
| PD | 67 | 65 | 5 | 0.944 (0.903–0.985) | 92.9% (84.3–96.9%) | 99.7% (99.0–100.0%) | 97.0% (89.8–99.5%) | 99.3% (98.4–99.7%) |
| AD | 69 | 67 | 3 | 0.961 (0.926–0.995) | 95.7% (88.1–98.8%) | 99.7% (99.0–100.0%) | 97.1% (90.0–99.5%) | 99.6% (98.8–99.9%) |
| Warts | ||||||||
| PD | 15 | 15 | 4 | 0.880 (0.763–0.996) | 78.9% (56.7–91.5%) | 100% (99.5–100.0%) | 100% (79.6–100.0%) | 99.5% (98.7–99.8%) |
| AD | 17 | 17 | 2 | 0.943 (0.865–1.000) | 89.5% (68.6–98.1%) | 100% (99.5–100.0%) | 100% (81.6–100.0%) | 99.7% (99.1–100.0%) |
| Other lesions | ||||||||
| PD | 72 | 63 | 32 | 0.731 (0.652–0.810) | 66.3% (56.3–75.0%) | 98.7% (97.5–99.3%) | 87.5% (77.9–93.3%) | 95.5% (93.7–96.8%) |
| AD | 111 | 74 | 21 | 0.676 (0.598–0.753) | 77.9% (68.6–85.1%) | 94.6% (92.6–96.1%) | 66.7% (57.5–74.8%) | 96.9% (95.2–97.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jobbágy, A.; Kiss, N.; Meznerics, F.A.; Farkas, K.; Plázár, D.; Bozsányi, S.; Fésűs, L.; Bartha, Á.; Szabó, E.; Lőrincz, K.; et al. Emergency Use and Efficacy of an Asynchronous Teledermatology System as a Novel Tool for Early Diagnosis of Skin Cancer during the First Wave of COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 2699. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052699
Jobbágy A, Kiss N, Meznerics FA, Farkas K, Plázár D, Bozsányi S, Fésűs L, Bartha Á, Szabó E, Lőrincz K, et al. Emergency Use and Efficacy of an Asynchronous Teledermatology System as a Novel Tool for Early Diagnosis of Skin Cancer during the First Wave of COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(5):2699. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052699
Chicago/Turabian StyleJobbágy, Antal, Norbert Kiss, Fanni Adél Meznerics, Klára Farkas, Dóra Plázár, Szabolcs Bozsányi, Luca Fésűs, Áron Bartha, Endre Szabó, Kende Lőrincz, and et al. 2022. "Emergency Use and Efficacy of an Asynchronous Teledermatology System as a Novel Tool for Early Diagnosis of Skin Cancer during the First Wave of COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 5: 2699. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052699