
Between and Within-Country Variations in Infant and Young Child Feeding Practices in South Asia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Population
2.3. Measurement of IYCF Indicators
2.4. Exposure Variables
2.5. Statistical Analyses
3. Results
3.1. Sociodemographic Characteristics of the Participants in SACs
3.2. Pooled Prevalence of IYCF Practices in SACs
3.3. Between-Country Variations of IYCF Practices in SACs
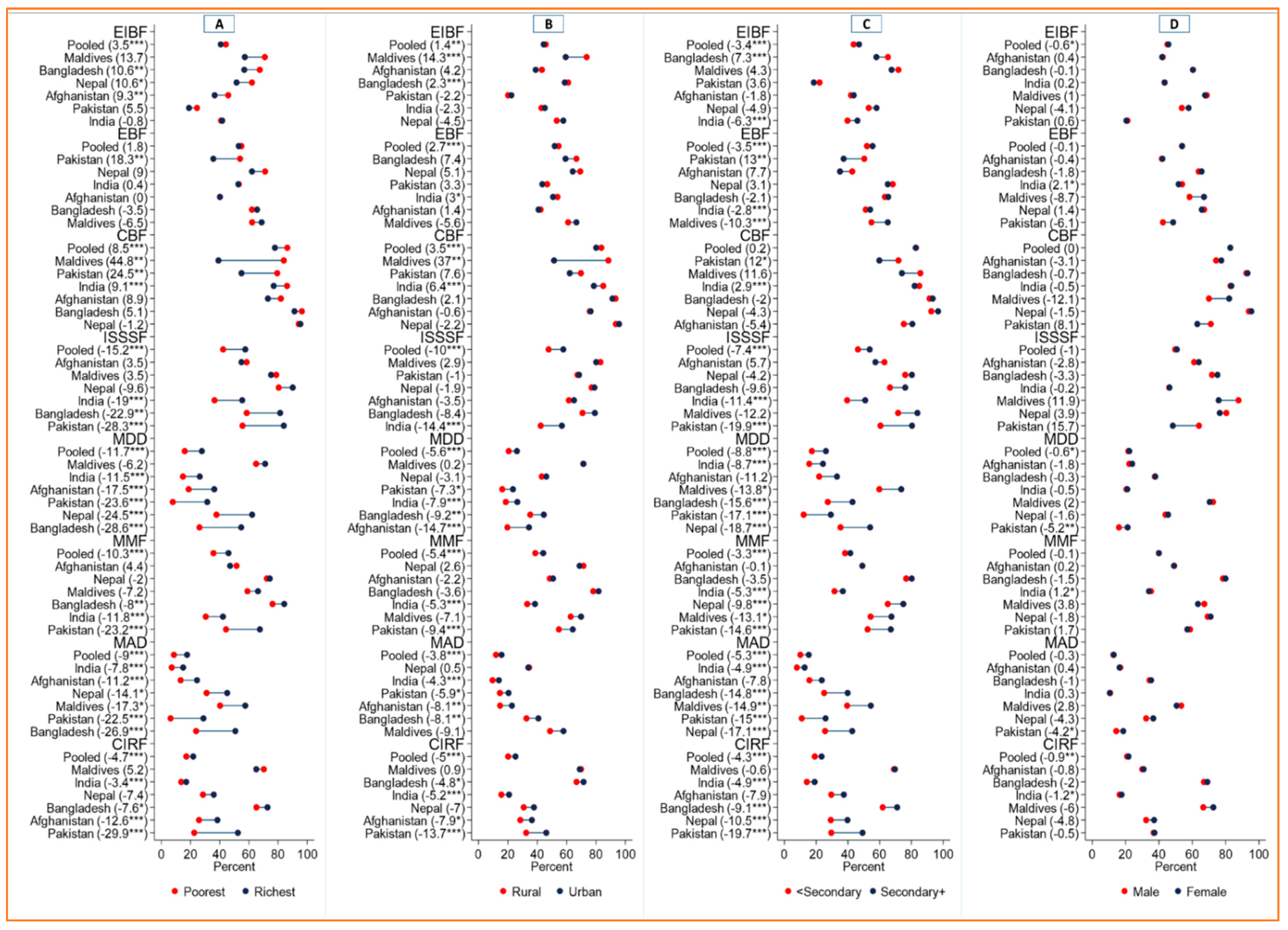
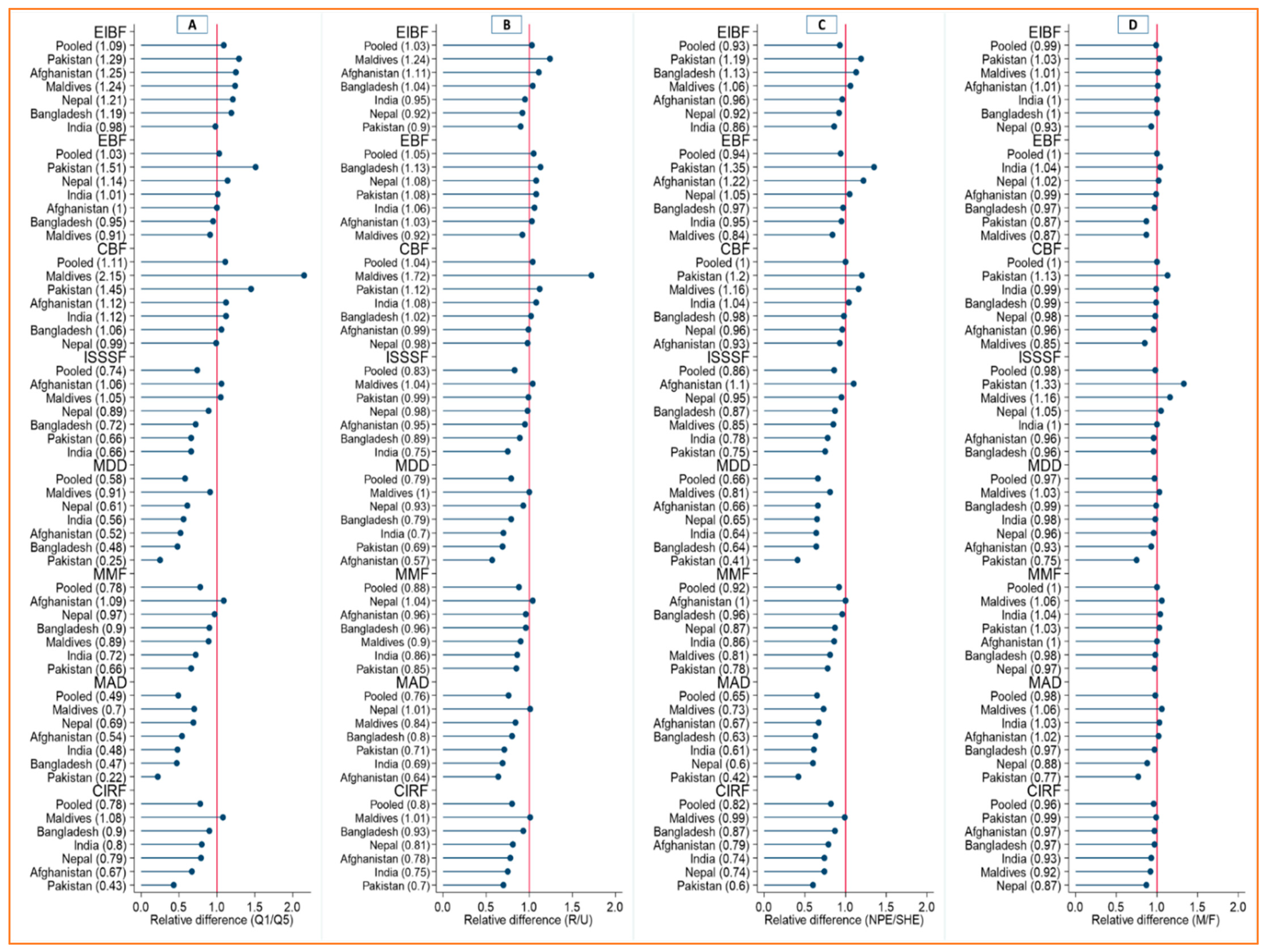
3.4. Within-Country Variations in IYCF Practices in Individual SACs across Subgroups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deki, P. Factors Affecting Early Childhood Growth and Development: Golden 1000 Days. Adv. Pract. Nurs. 2016, 1, 1–4. [Google Scholar] [CrossRef]
- Ayana, D.; Tariku, A.; Feleke, A.; Woldie, H. Complementary feeding practices among children in Benishangul Gumuz Region, Ethiopia. BMC Res. Notes 2017, 10, 335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations Children’s Fund (UNICEF); World Health Organization (WHO). WHO: Indicators for Assessing Infant and Young Child Feeding Practices; WHO and UNICEF: Geneva, Switzerland, 2007; Volume 2007, pp. 1–19. ISBN 978-92-4-159975-7. [Google Scholar]
- Aguayo, V.M.; Menon, P. Stop stunting: Improving child feeding, women’s nutrition and household sanitation in South Asia. Matern. Child Nutr. 2016, 12, 3–11. [Google Scholar] [CrossRef] [Green Version]
- United Nations Children’s Fund (UNICEF). Children in South Asia; UNICEF: New York, NY, USA, 2021. [Google Scholar]
- United Nations Children’s Fund (UNICEF). The State of the World’s Children 2016—A Fair Chance For Every Child; UNICEF: New York, NY, USA, 2016. [Google Scholar]
- Liu, X.; Liao, X.; Ren, Q.; Luo, M.; Yang, L.; Lin, J.; Chang, J. Concerns regarding complementary feeding practices among urban Chinese mothers: A focus group study in Xi’an. J. Health Popul. Nutr. 2018, 37, 20. [Google Scholar] [CrossRef] [PubMed]
- Aguayo, V.M. Complementary feeding practices for infants and young children in South Asia. A review of evidence for action post-2015. Matern. Child Nutr. 2017, 13, e12439. [Google Scholar] [CrossRef] [Green Version]
- Kabir, I.; Khanam, M.; Agho, K.E.; Mihrshahi, S.; Dibley, M.J.; Roy, S.K. Determinants of inappropriate complementary feeding practices in infant and young children in Bangladesh: Secondary data analysis of Demographic Health Survey 2007. Matern. Child Nutr. 2012, 8, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Saleem, A.F.; Mahmud, S.; Baig-Ansari, N.; Zaidi, A.K.M. Impact of Maternal Education about Complementary Feeding on Their Infants’ Nutritional Outcomes in Low- and Middle-income Households: A Community-based Randomized Interventional Study in Karachi, Pakistan. J. Health Popul. Nutr. 2014, 32, 623–633. [Google Scholar] [CrossRef]
- Senarath, U.; Agho, K.E.; Akram, D.E.S.; Godakandage, S.S.P.; Hazir, T.; Jayawickrama, H.; Joshi, N.; Kabir, I.; Khanam, M.; Patel, A.; et al. Comparisons of complementary feeding indicators and associated factors in children aged 6–23 months across five South Asian countries. Matern. Child Nutr. 2012, 8, 89–106. [Google Scholar] [CrossRef]
- United States Agency for International Development (USAID); International Coaching Federation (ICF). DHS Program; USAID: Rockville, MD, USA, 2021. [Google Scholar]
- National Institute of Population Research and Training (NIPORT); Mitra and Associates; International Coaching Federation (ICF). Bangladesh Demographic and Health Survey 2014; NIPORT: Dhaka, Bangladesh; Mitra and Associates: Dhaka, Bangladesh; ICF: Rockville, MD, USA, 2016. [Google Scholar]
- International Institute for Population Sciences (IIPS); International Coaching Federation (ICF). National Family Health Survey (NFHS-4), 2015–2016; IIPS: Mumbai, India, 2017. [Google Scholar]
- Ministry of Health, Nepal; New ERA; International Coaching Federation (ICF). Nepal Demographic and Health Survey 2016; Ministry of Health, Nepal: Kathmandu, Nepal, 2017. [Google Scholar]
- National Institute of Population Studies (NIPS) [Pakistan]; International Coaching Federation (ICF). Pakistan Demographic and Health Survey 2017–2018; NIPS: Islamabad, Pakistan; ICF: Rockville, MD, USA, 2019. [Google Scholar]
- Ministry of Health (MOH) [Maldives]; International Coaching Federation (ICF). Maldives Demographic and Health Survey 2016–2017; MOH: Malé, Maldives; ICF: Rockville, MD, USA, 2018. [Google Scholar]
- Central Statistics Organization (CSO); Ministry of Public Health (MoPH); International Coaching Federation (ICF). Afghanistan Demographic and Health Survey 2015; Central Statistics Organization: Kabul, Afghanistan, 2017. [Google Scholar]
- Rutstein, O.S.; Johnson, K. DHS Comaparative Reports, The DHS Wealth Index; USAID: Rockville, MD, USA, 2004. [Google Scholar]
- Elkasabi, M.; Ren, R.; Pullum, T.W. Multilevel Modeling Using DHS Surveys: A Framework to Approximate Level-Weights; USAID: Rockville, MD, USA, 2020. [Google Scholar]
- Publication, A.S.P. Stata Survey Data Reference Manual; Stata Press: College Station, TX, USA, 2021; ISBN 9781597180931. [Google Scholar]
- Ezeh, O.K.; Ogbo, F.A.; Stevens, G.J.; Tannous, W.K.; Uchechukwu, O.L.; Ghimire, P.R.; Agho, K.E. Factors associated with the early initiation of breastfeeding in economic community of West African States (ECOWAS). Nutrients 2019, 11, 2765. [Google Scholar] [CrossRef] [Green Version]
- Agho, K.E.; Ezeh, O.K.; Ghimire, P.R.; Uchechukwu, O.L.; Stevens, G.J.; Tannous, W.K.; Fleming, C.; Ogbo, F.A. Exclusive breastfeeding rates and associated factors in 13 “economic community of West African states” (ECOWAS) countries. Nutrients 2019, 11, 3007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zong, X.; Wu, H.; Zhao, M.; Magnussen, C.G.; Xi, B. Global prevalence of WHO infant feeding practices in 57 LMICs in 2010–2018 and time trends since 2000 for 44 LMICs. EClinicalMedicine 2021, 37, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Analysis, C.A.T.; Mallick, L.; Wang, W.; Farid, S. Initiation of Breastfeeding in Low- and Middle-Income. Glob. Health Sci. Pract. 2020, 9, 308–317. [Google Scholar]
- Nguyen, P.H.; Avula, R.; Headey, D.; Tran, L.M.; Ruel, M.T.; Menon, P. Progress and inequalities in infant and young child feeding practices in India between 2006 and 2016. Matern. Child Nutr. 2018, 14, e12663. [Google Scholar] [CrossRef] [PubMed]
- Sharma, I.K.; Byrne, A. Early initiation of breastfeeding: A systematic literature review of factors and barriers in South Asia. Int. Breastfeed. J. 2016, 11, 17. [Google Scholar] [CrossRef] [Green Version]
- Asim, M.; Asim, M.; Asim, M.; Ahmed, Z.H.; Hayward, M.D.; Widen, E.M. Prelacteal feeding practices in Pakistan: A mixed-methods study. Int. Breastfeed. J. 2020, 15, 53. [Google Scholar] [CrossRef]
- Benedict, R.K.; Craig, H.C.; Torlesse, H.; Stoltzfus, R.J. Trends and predictors of optimal breastfeeding among children 0–23 months, South Asia: Analysis of national survey data. Matern. Child Nutr. 2018, 14, e12698. [Google Scholar] [CrossRef]
- Rahimi, B.A.; Mohamadi, E.; Stanikzai, M.H.H.; Wasiq, A.W. Determinants of Exclusive Breastfeeding Practices in Kandahar, Afghanistan: A Cross-Sectional Analytical Study. Int. J. Pediatr. 2020, 8, 11125–11140. [Google Scholar] [CrossRef]
- Torlesse, H.; Raju, D. Feeding of Infants and Young Children in South Asia; UNICEF: New York, NY, USA; World Bank Group: Washington, DC, USA, 2018. [Google Scholar]
- International Baby Foods Action Network (IBFAN); World Health Organization (WHO); United Nations Children’s Fund (UNICEF). Marketing of Breast-Milk Substitutes: National Implementation of the International Code; UNICEF: New York, NY, USA, 2020; ISBN 978-92-4-156532-5. [Google Scholar]
- Barenners, H.; Guenther, S.; Sophie, G. Enforcing the International Code of Marketing of Breast-milk Substitutes for Better Promotion of Exclusive Breastfeeding: Can Lessons Be Learned? J. Hum. Lact. 2015, 32, 20–27. [Google Scholar] [CrossRef]
- Dhami, M.V.; Ogbo, F.A.; Diallo, T.M.O.; Olusanya, B.O.; Goson, P.C.; Agho, K.E. Infant and young child feeding practices among adolescent mothers and associated factors in India. Nutrients 2021, 13, 2376. [Google Scholar] [CrossRef]
- Neogi, D. A wider regional disparities in terms of Human Development Index and Human Poverty Index have been reported in the Human Development Report of the I. Int. J. Humanit. Technol. 2010, 4, 259–266. [Google Scholar]
- Malhotra, C.; Do, Y.K. Socio-economic disparities in health system responsiveness in India. Health Policy Plan. 2013, 28, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jejeebhoy, S.J.; Sathar, Z.A. Women’s autonomy in India and Pakistan: The influence of religion and region. Popul. Dev. Rev. 2001, 27, 687–712. [Google Scholar] [CrossRef]
- Manikam, L.; Prasad, A.; Dharmaratnam, A.; Moen, C.; Robinson, A.; Light, A.; Ahmed, S.; Lingam, R.; Lakhanpaul, M. Systematic review of infant and young child complementary feeding practices in South Asian families: The India perspective. Public Health Nutr. 2018, 21, 637–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manikam, L.; Sharmila, A.; Dharmaratnam, A.; Alexander, E.C.; Kuah, J.Y.; Prasad, A.; Ahmed, S.; Lingam, R.; Lakhanpaul, M. Systematic review of infant and young child complementary feeding practices in South Asian families: The Pakistan perspective. Public Health Nutr. 2018, 21, 655–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhami, M.V.; Ogbo, F.A.; Osuagwu, U.L.; Agho, K.E. Prevalence and factors associated with complementary feeding practices among children aged 6–23 months in India: A regional analysis. BMC Public Health 2019, 19, 1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadesse, F.; Alemayehu, Y.; Shine, S.; Asresahegn, H.; Tadesse, T. Exclusive breastfeeding and maternal employment among mothers of infants from three to five months old in the Fafan zone, Somali regional state of Ethiopia: A comparative cross-sectional study. BMC Public Health 2019, 19, 1015. [Google Scholar] [CrossRef]
- Gebrekidan, K.; Hall, H.; Plummer, V.; Fooladi, E. Exclusive breastfeeding continuation and associated factors among employed women in North Ethiopia: A cross-sectional study. PLoS ONE 2021, 16, 1–16. [Google Scholar] [CrossRef]
- Gebrekidan, K.; Fooladi, E.; Plummer, V.; Hall, H. Enablers and barriers of exclusive breastfeeding among employed women in low and lower middle-income countries. Sex. Reprod. Healthc. 2020, 25, 100514. [Google Scholar] [CrossRef]
- Hasan, A.M.R.; Smith, G.; Selim, M.A.; Akter, S.; Uz, N.; Khan, Z.; Sharmin, T.; Rasheed, S. Work and breast milk feeding: A qualitative exploration of the experience of lactating mothers working in ready made garments factories in urban Bangladesh. Int. Breastfeed. J. 2020, 15, 93. [Google Scholar] [CrossRef]
- Kimani-Murage, E.W.; Wilunda, C.; Macharia, T.N.; Kamande, E.W.; Gatheru, P.M.; Zerfu, T.; Donfouet, H.P.P.; Kiige, L.; Jabando, S.; Dinga, L.A.; et al. Effect of a baby-friendly workplace support intervention on exclusive breastfeeding in Kenya. Matern. Child Nutr. 2021, 17, e13191. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Compte, M.; Hernández-Cordero, S.; Ancira-Moreno, M.; Burrola-Méndez, S.; Ferre-Eguiluz, I.; Omaña, I.; Pérez Navarro, C. Breastfeeding at the workplace: A systematic review of interventions to improve workplace environments to facilitate breastfeeding among working women. Int. J. Equity Health 2021, 20, 110. [Google Scholar] [CrossRef] [PubMed]
- Benedict, R.K.; Craig, H.C.; Torlesse, H.; Stoltzfus, R.J. Effectiveness of programmes and interventions to support optimal breastfeeding among children 0–23 months, South Asia: A scoping review. Matern. Child Nutr. 2018, 14, e12697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatica-Domínguez, G.; Neves, P.A.R.; Barros, A.J.D.; Victora, C.G. Complementary Feeding Practices in 80 Low-and Middle-Income Countries: Prevalence of and Socioeconomic Inequalities in Dietary Diversity, Meal Frequency, and Dietary Adequacy. J. Nutr. 2021, 151, 1956–1964. [Google Scholar] [CrossRef]
- Ryckman, T.; Beal, T.; Nordhagen, S.; Murira, Z.; Torlesse, H. Affordability of nutritious foods for complementary feeding in South Asia. Nutr. Rev. 2021, 79, 52–68. [Google Scholar] [CrossRef]
- Ali, M.; Arif, M.; Shah, A.A. Complementary feeding practices and associated factors among children aged 6–23 months in Pakistan. PLoS ONE 2021, 16, 1–21. [Google Scholar] [CrossRef]
- Rao, S.; Swathi, P.M.; Unnikrishnan, B.; Hegde, A. Study of complementary feeding practices among mothers of children aged six months to two years—A study from coastal south India. Australas. Med. J. 2011, 4, 252–257. [Google Scholar] [CrossRef]
- Nguyen, P.H.; Avula, R.; Ruel, M.T.; Saha, K.K.; Ali, D.; Tran, L.M.; Frongillo, E.A.; Menon, P.; Rawat, R. Maternal and child dietary diversity are associated in bangladesh, vietnam, and ethiopia. J. Nutr. 2013, 143, 1176–1183. [Google Scholar] [CrossRef]
- World Breastfeeding Trends Initiative. Assessment Report, Maldives; International Baby Food Action Network (IBFAN) Asia: Delhi, India, 2015; Available online: https://www.worldbreastfeedingtrends.org/uploads/country-data/country-report/WBTi-Maldives-2015.pdf (accessed on 10 February 2022).
- Integrated National Nutrition Strategic Plan 2013–2017. Maldives. 2017. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/MDV%202016%20Integrated%20National%20Nutrition%20Strategic%20Plan.pdf (accessed on 10 February 2022).
- Jangid, M.; Neupane, S.; Scott, S.; Nguyen, P.H.; Kim, S.S.; Murira, Z.; Torlesse, H.; Menon, P. Are Data Available for Tracking Progress on Nutrition Policies, Programs, and Outcomes in Bangladesh? International Food Policy Research Institute: Washington, DC, USA, 2021. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Pooled Data (2015–2018) | Afghanistan (2015 ¥) | Bangladesh (2017–2018 ¥) | India (2015–2016 ¥) | Maldives (2016–2017 ¥) | Nepal (2016 ¥) | Pakistan (2017–2018 ¥) | p-Value |
|---|---|---|---|---|---|---|---|---|
| n (%) n = 120,830 | n (%) n = 11,762 | n (%) n = 3411 | n (%) n = 97,935 | n (%) n = 1147 | n (%) n = 1919 | n (%) n = 4656 | ||
| Mother’s Age | ||||||||
| 15–24 years | 52,217 (43.2) | 4293 (37.6) | 1883 (55.1) | 43,310 (47.0) | 258 (20.1) | 1034 (52.6) | 1439 (31.6) | <0.001 |
| 25–34 years | 58,794 (48.7) | 5454 (44.8) | 1328 (39.3) | 48,028 (47.5) | 704 (61.9) | 786 (42.2) | 2494 (54.5) | |
| ≥35 years | 9819 (8.1) | 2015 (17.7) | 200 (5.6) | 6597 (6.7) | 185 (18.1) | 99 (5.2) | 723 (13.9) | |
| Mother’s Education | ||||||||
| <Secondary | 57,216 (47.4) | 10,751 (89.3) | 1174 (34.0) | 41,308 (40.8) | 190 (16.4) | 900 (48.7) | 2893 (63.1) | <0.001 |
| ≥Secondary | 63,614 (52.6) | 1011 (10.7) | 2237 (66.0) | 56,627 (59.2) | 957 (83.6) | 1019 (51.3) | 1763 (36.9) | |
| Child Sex | ||||||||
| Male | 63,146 (52.3) | 6111 (52.0) | 1769 (52.0) | 51,299 (52.5) | 574 (59.6) | 1038 (53.8) | 2355 (50.3) | 0.280 |
| Female | 57,684 (47.7) | 5651 (48.0) | 1642 (48.0) | 46,636 (47.5) | 573 (50.4) | 881 (46.2) | 2301 (49.7) | |
| Child age, mean (sd) | 11.3 (6.6) | 10.6 (6.6) | 11.2 (6.9) | 11.4 (6.6) | 11.7 (6.8) | 11.8 (6.8) | 10.8 (6.6) | <0.001 * |
| Place of Residence | ||||||||
| Urban | 30,159 (25.0) | 2920 (24.2) | 1167 (26.7) | 22,790 (27.5) | 114 (9.9) | 1089 (53.6) | 2079 (33.1) | <0.001 |
| Rural | 90,671 (75.0) | 8842 (75.8) | 2244 (73.3) | 75,145 (72.6) | 1033 (90.1) | 830 (46.5) | 2577 (67.0) | |
| Wealth Quantile | ||||||||
| Poorest | 29,792 (24.7) | 2019 (17.8) | 724 (20.5) | 25,225 (24.8) | 311 (27.1) | 486 (21.0) | 1027 (21.5) | <0.001 |
| Poorer | 28,187 (23.3) | 2667 (20.0) | 712 (21) | 23,044 (22.0) | 327 (28.5) | 407 (21.2) | 1030 (19.1) | |
| Middle | 24,750 (20.5) | 2676 (21.5) | 627 (19.2) | 19,765 (20.2) | 328 (28.6) | 413 (23.0) | 941 (21.5) | |
| Richer | 20,959 (17.3) | 2654 (21.5) | 684 (20.5) | 16,336 (18.1) | 120 (10.5) | 371 (20.5) | 794 (18.6) | |
| Richest | 17,142 (14.2) | 1746 (19.3) | 664 (18.8) | 13,565 (14.8) | 61 (5.3) | 242 (14.4) | 864 (19.3) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tariqujjaman, M.; Hasan, M.M.; Mahfuz, M.; Ahmed, T.; Hossain, M. Between and Within-Country Variations in Infant and Young Child Feeding Practices in South Asia. Int. J. Environ. Res. Public Health 2022, 19, 4350. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19074350
Tariqujjaman M, Hasan MM, Mahfuz M, Ahmed T, Hossain M. Between and Within-Country Variations in Infant and Young Child Feeding Practices in South Asia. International Journal of Environmental Research and Public Health. 2022; 19(7):4350. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19074350
Chicago/Turabian StyleTariqujjaman, Md., Md. Mehedi Hasan, Mustafa Mahfuz, Tahmeed Ahmed, and Muttaquina Hossain. 2022. "Between and Within-Country Variations in Infant and Young Child Feeding Practices in South Asia" International Journal of Environmental Research and Public Health 19, no. 7: 4350. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19074350