
Depression, Anxiety and Stress in Health Professionals in the COVID-19 Context

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Procedures and Data Collection
2.3. Instruments
2.4. Data Analysis
3. Results
3.1. Characteristics of Participants
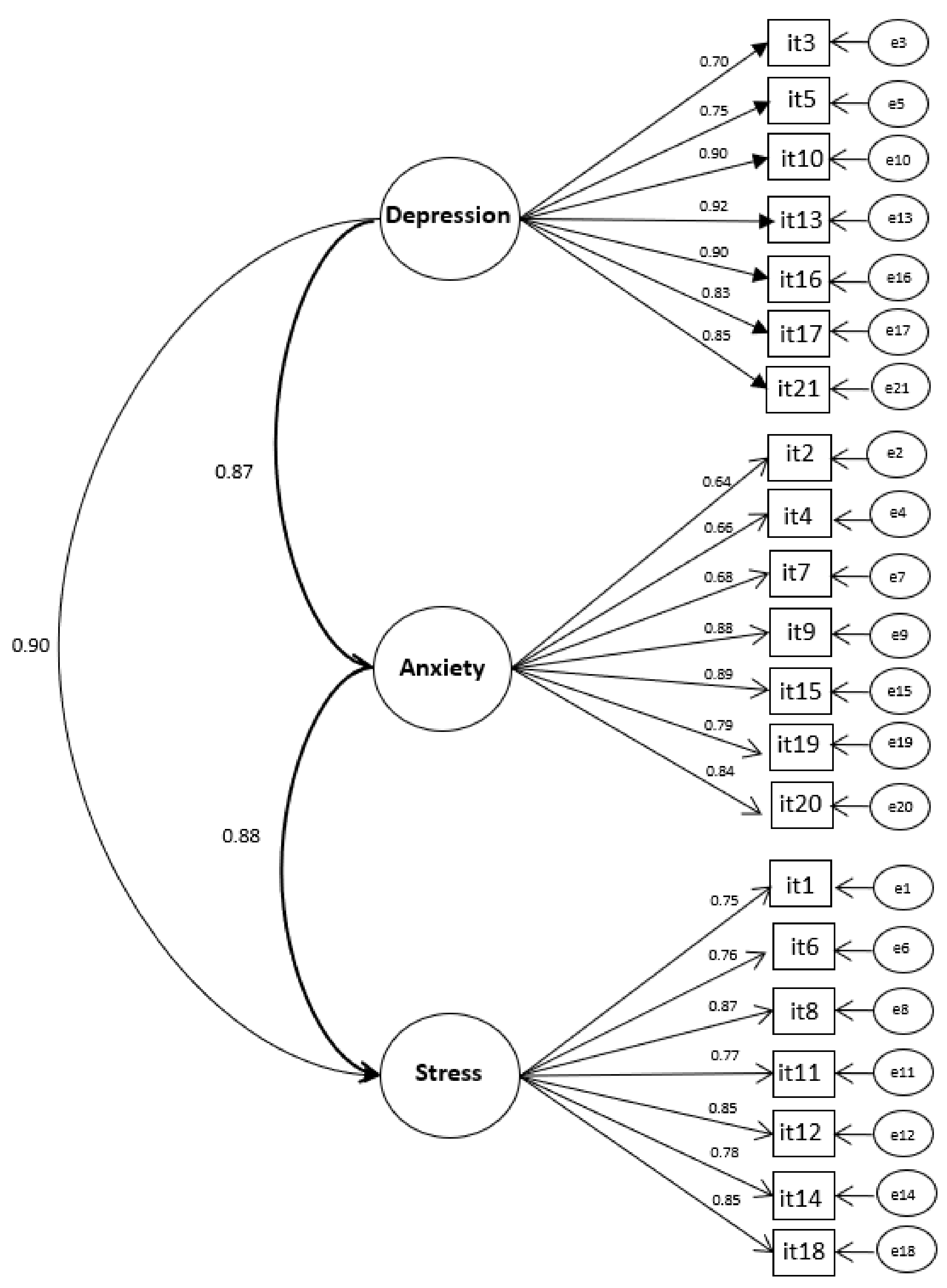
3.2. Psychometric Characteristics of the Measuring Instrument
3.3. Prevalence of Depression, Anxiety and Stress Symptoms in the Sample
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marziale, M.H.P.; Palha, P.F.; Dantas, R.A.S.; Dalri, M.C.B.; Reis, R.K.; Silveira, R.C.C.P.; Menegueti, M.G.; Braga, F.T.M.M.; Godoy, S.; Canini, S.R.M.S.; et al. Care in the Hospital Care Setting for Patients with Suspected or Diagnosed COVID-19; Ministry of Health: Brasília, Brazil, 2020; p. 62. Available online: https://www.gov.br/saude/pt-br/coronavirus/publicacoes-tecnicas/recomendacoes/cuidados-no-ambiente-de-assistencia-hospitalar (accessed on 26 January 2022).
- Barros-Delben, P.; Cruz, R.M.; Trevisan, K.R.R.; Gai, M.J.P.; Carvalho, R.V.C.; Carlotto, P.A.C.; Alves, R.B.; Silvestre, D.; Renner, C.O.; Silva, A.G.; et al. Mental health in emergency situation: COVID-19. Debates Psychiatry 2020, 2, 18–28. [Google Scholar] [CrossRef]
- Shen, X.; Zou, X.; Zhong, X.; Yan, J.; Li, L. Psychological stress of ICU nurses in the time of COVID-19. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, D.J.; Gomes, M.P.; Souza, F.B.A.; Gomes, A.M.T. Stress factors in nursing professionals in combating the COVID-19 pandemic: Synthesis of evidence. Commu. Ciênc. Saúde 2020, 31 (Suppl. 1), 31–47. Available online: http://www.escs.edu.br/revistaccs/index.php/comunicacaoemcienciasdasaude/article/view/651/291 (accessed on 26 January 2022).
- Walton, M.; Murray, E.; Christian, M.D. Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, M.V.L.O.; Silva, C.N.; Santana, V.V.F.; Cavalcante, R.S.; Carmo, M.G. Burnout Syndrome in healthcare professionals in the context of the COVID-19 pandemic: Integrative review. Braz. J. Dev. 2021, 7, 85508–85520. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef]
- Fernandez, R.; Sikhosana, N.; Green, H.; Halcomb, E.J.; Middleton, R.; Alananzek, I.; Trakis, S.; Moxham, L. Anxiety and depression among healthcare workers during the COVID-19 pandemic: A systematic umbrella review of the global evidence. BMJ Open 2021, 11, e054528. [Google Scholar] [CrossRef]
- Mahmud, S.; Hossain, S.; Muyeed, A.; Islam, M.M.; Mohsin, M. The global prevalence of depression, anxiety, stress, and, insomnia and its changes among health professionals during COVID-19 pandemic: A rapid systematic review and meta-analysis. Heliyon 2021, 7, e07393. [Google Scholar] [CrossRef]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and post-traumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar] [CrossRef]
- Silva Neto, R.M.; Benjamin, C.J.R.; Carvalho, P.M.M.; Rolim Neto, M.L. Psychological effects caused by the COVID-19 pandemic in health professionals: A systematic review with meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 104, 110062. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf?sfvrsn=6d3578af_10 (accessed on 21 January 2022).
- Sun, P.; Wang, M.; Song, T.; Wu, Y.; Luo, J.; Chen, L.; Yan, L. The Psychological Impact of COVID-19 Pandemic on Health Care Workers: A Systematic Review and Meta-Analysis. Front. Psychol. 2021, 12, 626547. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.A.; Watson, D. Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. J. Abnorm. Psychol. 1991, 100, 316–336. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the beck depression and anxiety inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- American Psychiatric Association. Manual Diagnóstico e Estatístico de Transtornos Mentais (DSM-5); Artmed: Porto Alegre, Brazil, 2014. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis; Prentice Hall: Hoboken, NJ, USA, 2010.
- National Health Council. Guidelines and Norms Regulating Research Involving Human Beings, Resolution n. 466. Brazil, 12 December 2012. Available online: https://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf (accessed on 26 January 2022).
- Vignola, R.C.B.; Tucci, A.M. Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. J. Affect Disord. 2014, 155, 104–109. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Marôco, J. Análise de Equações Estruturais: Fundamentos Teóricos, Software & Aplicações; Report Number: Pêro Pinheiro, Portugal, 2014. [Google Scholar]
- Arbuckle, J.L. AMOS 17.0 user’s guide. In Manual Software; Statistical Package for the Social Sciences: Chicago, IL, USA, 2008. [Google Scholar]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Kaplan, R.M.; Saccuzzo, D.P. Psychological Testing. Principles, Applications and Issues; Wadsworth Cengage Learning: Belmont, CA, USA, 2012. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating Structural Equation Models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Marôco, J.; Garcia-Marques, T. How Reliable is Cronbach’s Alpha? Old Questions and Modern Solutions? Lab. Psciol. 2006, 4, 65–90. [Google Scholar] [CrossRef] [Green Version]
- Pan American Health Organization. Nursing Photography in Brazil. Available online: https://apsredes.org/fotografia-da-enfermagem-no-brasil/ (accessed on 21 January 2022).
- Oliveira, A.P.C.; Ventura, C.A.A.; Silva, F.V.; Neto, H.A.; Mendes, I.A.; Souza, K.V.; Pinheiro, M.I.C.; Silva, M.C.N.; Padilla, M.; Ramalho, N.M.; et al. State of Nursing in Brazil. Rev. Latino-Am. Enferm. 2020, 28, e3404. [Google Scholar] [CrossRef]
- Chang, K.; Hau, W.; Pakpour, A.H.; Griffiths, M.D. Psychometric Testing of Three COVID-19-Related Scales Among People with Mental Illness. Int. J. Ment. Health Addict. 2020, 20, 324–336. [Google Scholar] [CrossRef]
- Marziale, M.H.P.; Rocha, F.L.R.; Cassenote, A.J.F.; Robazzi, M.L.C.C.; Palha, P.F.; Ballestero, J.G.A.; Terra, F.S.; Mininel, V.A.; Santos, H.E.C.; Fracarolli, I.F.L.; et al. Cultural adaptation and updating of the Risk assessment and management of exposure of health care workers in the context of COVID-19 questionnaire. Rev. Latino-Am. Enferm. 2021, 29, e3490. [Google Scholar] [CrossRef] [PubMed]
- Tareke, S.A.; Lelisho, M.E.; Hassen, S.S.; Seid, A.A.; Jemal, S.S.; Teshale, B.M.; Wotale, T.E.; Pandey, B.K. The Prevalence and Predictors of Depressive, Anxiety, and Stress Symptoms among Tepi Town Residents During the COVID-19 Pandemic Lockdown in Ethiopia. J. Racial Ethn. Health Disparities 2022, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Alshekaili, M.; Hassan, W.; Al Said, N.; Al Sulaimani, F.; Jayapal, S.K.; Al Mawali, A.; Chan, M.F.; Mahadvan, S.; Al Adawi, A. Factors associated with mental health outcomes across healthcare settings in Oman during COVID-19: Frontline versus non-frontline healthcare workers. BMJ Open 2020, 10, 042030. [Google Scholar] [CrossRef] [PubMed]
- Tiete, J.; Guatteri, M.; Lachaux, A.; Motossian, A.; Loas, G.; Rotsaert, M. Mental Health Outcomes in Healthcare Workers in COVID-19 and Non-COVID-19 Care Units: A Cross-Sectional Survey in Belgium. Front. Psychol. 2021, 20, 324–336. [Google Scholar] [CrossRef]
- Ali, S.; Maguire, S.; Marks, E.; Doyle, E.; Sheehy, C. Psychological impact of the COVID-19 pandemic on healthcare workers at acute hospital settings in the South-East of Ireland: An observational cohort multicentre study. BMJ Open 2020, 10, 042930. [Google Scholar] [CrossRef]
- Sharma, I.; Misra, A.; Kumar Shrestha, B.; Kumar Koirala, A.; Banjade, A.; Banjade, P. Depression, Anxiety and Stress among Nepali Health Care Workers during the Coronavirus Disease 2019 Pandemic: A Cross-sectional Survey. JNMA J. Nepal Med. Assoc. 2021, 59, 580–584. [Google Scholar] [CrossRef]
- Rosa, P.; Brown, R.; Pravecek, B.; Carotta, C.; Garcia, A.S.; Carson, P.; Callies, D.; Vukovich, M. Factors associated with nurses emotional distress during the COVID-19 pandemic. Appl. Nurs. Res. 2021, 62, 151502. [Google Scholar] [CrossRef]
- Silva, D.F.O.; Cabucci, R.N.; Rachetti, V.P.S.; Lima, S.C.V.C.; Andrade, F.B. Prevalence of anxiety among health professionals in times of COVID-19: A systematic review with meta-analysis. Ciência Saúde Coletiva 2021, 26, 693–710. [Google Scholar] [CrossRef]
- Sampaio, F.; Sequeira, C.; Teixeira, L. Impact of COVID-19 outbreak on nurses’ mental health: A prospective cohort study. Environ. Res. 2021, 194, 110620. [Google Scholar] [CrossRef]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, anxiety, stress levels of physicians and associated factors in COVID-19 pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef]
- Pereira, A.C.C.; Pereira, M.M.A.; Silva, B.L.L. O agravamento dos transtornos de ansiedade em profissionais de saúde no contexto da pandemia da COVID-19. Braz. J. Health Rev. 2021, 14, 4094–4110. [Google Scholar] [CrossRef]
- Campos, J.A.D.B.; Martins, B.G.; Campos, L.A.; Dias, F.F.V.; Maroco, J. Symptoms related to mental disorder in healthcare workers during the COVID-19 pandemic in Brazil. Int. Arch. Occup. Environ. Health 2021, 94, 1023–1032. [Google Scholar] [CrossRef]
- Dantas, E.S.O.; Filho, J.D.A.; Silva, G.W.S.; Silveira, M.Y.M.; Dantas, M.N.P.; Meira, K.C. Fatores associados à ansiedade em residentes multiprofissionais em saúde durante a pandemia por COVID-19. Rev. Bras. Enferm. 2021, 74, e20200961. [Google Scholar] [CrossRef]
- Ornell, F.; Halpern, S.C.; Kessler, F.H.P.; Narvaez, J.C.M. The impact of the COVID-19 pandemic on the mental health of healthcare professionals. Cad. De Saúde Pública 2020, 36, e00063520. [Google Scholar] [CrossRef]
- Eysenck, M.; Payne, S.; Santos, R. Anxiety and depression: Past, present, and future events. Cogn. Emot. 2006, 20, 274–294. [Google Scholar] [CrossRef]
- Rinaldi, L.; Locati, F.; Parolin, L.; Girelli, L. Distancing the present self from the past and the future: Psychological distance in anxiety and depression. Q. J. Exp. Psychol. (Hove) 2017, 70, 1106–1113. [Google Scholar] [CrossRef]
- Ayanian, J.Z. Mental Health Needs of Health Care Workers Providing Frontline COVID-19 Care. JAMA 2020, 1, e200397. [Google Scholar] [CrossRef]
- Kang, L.; Li, Y.; Hu, S.; Chen, M.; Yang, C.; Yang, B.X.; Wang, Y.; Hu, J.; Lai, J.; Ma, X.; et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavírus. Lancet Psychiatry 2020, 7, e14. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, C.F.S.; Soares, C.M.; Souza, E.A.; Lisboa, E.S.; Pinto, I.C.M.; Andrade, L.R.; Espiridião, M.A. The health of healthcare professionals coping with the COVID-19 pandemic. Ciência Saúde Coletiva 2020, 25, 3465–3474. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- De Sire, A.; Marotta, N.; Raimo, S.; Lippi, L.; Inzitari, M.T.; Tasselli, A.; Gimigliano, A.; Palermo, L.; Invernizzi, M.; Ammendolia, A. Psychological Distress and Work Environment Perception by Physical Therapists from Southern Italy during COVID-19 Pandemic: The C.A.L.A.B.R.I.A Study. Int. J. Environ. Res. Public Health 2021, 18, 9676. [Google Scholar] [CrossRef] [PubMed]
- Martins, B.G.; Silva, W.R.; Maroco, J.; Campos, J.A.B.D. Escala de Depressão, Ansiedade e Estresse: Propriedades psicométricas e prevalência das afetividades. J. Bras. Psiquiatr. 2019, 68, 32–41. [Google Scholar] [CrossRef] [Green Version]
- Bibi, A.; Lin, M.; Zhang, X.; Margraf, J. Psychometric properties and measurement invariance of Depression, Anxiety and Stress Scales (DASS-21) across cultures. Int. J. Psychol. 2020, 55, 916–925. [Google Scholar] [CrossRef] [PubMed]
- Talaee, N.; Varahram, M.; Jamaati, H.; Salimi, A.; Attarchi, M.; Dizaji, M.K.; Sadr, M.; Hassani, S.; Farzanegan, B.; Monjazebi, F.; et al. Stress and Burnout in health care workers during COVID-19 pandemic: Validation of a questionnaire. J. Public Health 2020, 30, 1–6. [Google Scholar] [CrossRef]
- Formiga, N.S.; Franco, J.B.M.; Oliveira, H.C.C.; Prochazka, G.L.; Beserra, T.K.P.; Valin, C.G.P.; Grangeiro, S.G.P.; Nascimento, R.L. Invariância fatorial, sensibilidade e diferenças da medida de ansiedade, estresse e depressão (DASS-21) em trabalhadores brasileiros. Res. Soc. Dev. 2021, 10, e26910715572. [Google Scholar] [CrossRef]
- Lee, J.; Lee, E.; Moon, S.H. Systematic review of the measurement properties of the Depression Anxiety Stress Scales-21 by applying updated COSMIN methodology. Qual. Life Res. 2019, 28, 2325–2339. [Google Scholar] [CrossRef]
- Jiang, L.; Yan, Y.; Jin, Z.S.; Hu, M.L.; Wang, L.; Song, Y.; Li, N.N.; Su, J.; Wu, D.X.; Xiao, T. The Depression Anxiety Stress Scale-21 in Chinese Hospital Workers: Reliability, Latent Structure, and Measurement Invariance across Genders. Front. Psychol. 2020, 11, 247. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | n (%) |
|---|---|
| Gender | |
| Female | 436 (82.5) |
| Male | 93 (17.5) |
| Professional Category | |
| Nurse | 353 (66.7) |
| Nurse technicians | 92 (17.3) |
| Nurse assistants | 02 (0.3) |
| Physician | 59 (11.1) |
| Physiotherapist | 23 (4.3) |
| Health care unit # | |
| First Aid/Emergency | 138 (26.0) |
| Adult or pediatric ward | 112 (21.1) |
| Adult, pediatric or neonatal Intensive Care Unit (ICU) | 98 (18.5) |
| Exclusive ICU for COVID-19 care | 58 (10.9) |
| Exclusive ward for COVID-19 care | 90 (17.0) |
| Surgical center and material and sterilization center | 54 (10.2) |
| Oncology units | 25 (4.7) |
| Administrative sectors | 47 (8.8) |
| Employment Contract(s) | |
| More than one job | 174 (32.9) |
| Only one job | 355 (67.1) |
| Work shift # | |
| Morning | 139 (26.2) |
| Afternoon | 107 (20.2) |
| Night | 140 (26.4) |
| Daytime (morning and afternoon) | 266 (50.2) |
| Evening | 85 (16.0) |
| Confirmatory Factor Analysis | Reliability | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample | n | λ | χ2 | df | χ2/df | RMSEA | 90% CI | CFI | TLI | AVE (D/A/S) | CR (D/A/S) | α# (D/A/S) |
| Total sample | 529 | 0.645–0.923 | 656.583 | 186 | 3.530 | 0.069 | 0.063–0.075 | 0.979 | 0.976 | 0.705/0.603/0.651 | 0.943/0.913/0.929 | 0.94/0.91/0.92 |
| DASS test | 271 | 0.588–0.915 | 427.824 | 186 | 2.300 | 0.069 | 0.061–0.078 | 0.976 | 0.973 | 0.706/0.566/0.636 | 0.944/0.900/0.924 | 0.94/0.90/0.92 |
| DASS validation | 258 | 0.626–0.941 | 363.971 | 186 | 1.957 | 0.061 | 0.052–0.070 | 0.986 | 0.984 | 0.710/0.644 0.669 | 0.944/0.926/0.934 | 0.94/0.92/0.93 |
| Severity | Depression | Anxiety | Stress | |||
|---|---|---|---|---|---|---|
| n | %[95% CI] | n | %[95% CI] | n | %[95% CI] | |
| Normal | 201 | 38.0 [33.9–42.1] | 196 | 37.0 [33.0–41.2] | 204 | 38.6 [34.4–42.8] |
| Mild | 71 | 13.4 [10.5–16.3] | 42 | 7.9 [5.6–10.2] | 72 | 13.6 [10.7–16.5] |
| Moderate | 100 | 18.9 [15.6–22.2] | 112 | 21.2 [17.7–24.7] | 92 | 17.4 [14.2–20.6] |
| Severe | 71 | 13.4 [10.5–16.3] | 43 | 8.1 [5.8–10.4] | 104 | 19.7 [16.3–23.1] |
| Extremely severe | 86 | 16.3 [13.1–19.5] | 136 | 25.7 [22.0–29.4] | 57 | 10.8 [8.2–13.4] |
| Total | 529 | 100 | 529 | 100 | 529 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, G.P.A.; Fracarolli, I.F.L.; dos Santos, H.E.C.; de Oliveira, S.A.; Martins, B.G.; Santin Junior, L.J.; Marziale, M.H.P.; Rocha, F.L.R. Depression, Anxiety and Stress in Health Professionals in the COVID-19 Context. Int. J. Environ. Res. Public Health 2022, 19, 4402. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19074402
Garcia GPA, Fracarolli IFL, dos Santos HEC, de Oliveira SA, Martins BG, Santin Junior LJ, Marziale MHP, Rocha FLR. Depression, Anxiety and Stress in Health Professionals in the COVID-19 Context. International Journal of Environmental Research and Public Health. 2022; 19(7):4402. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19074402
Chicago/Turabian StyleGarcia, Gracielle Pereira Aires, Isabela Fernanda Larios Fracarolli, Heloisa Ehmke Cardoso dos Santos, Samuel Andrade de Oliveira, Bianca Gonzalez Martins, Lacir José Santin Junior, Maria Helena Palucci Marziale, and Fernanda Ludmilla Rossi Rocha. 2022. "Depression, Anxiety and Stress in Health Professionals in the COVID-19 Context" International Journal of Environmental Research and Public Health 19, no. 7: 4402. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19074402