
Posture Correction Therapy and Pelvic Floor Muscle Function Assessed by sEMG with Intravaginal Electrode and Manometry in Female with Urinary Incontinence

Abstract
:1. Introduction
2. Material and Method
- (1)
- A personal questionnaire with subjects’ demographics and with questions related to the type of work, physical activity, childbirths, and any issues related to the pelvic floor (pre-test).
- (2)
- Pelvic floor muscle assessment with the use of the PERFECT Scheme and the Oxford scale palpation examination, sEMG with an intravaginal electrode (MyoPlus Pro electromyograph produced by Neurotrack, Verity, Ireland) and manometry with intravaginal probe (Myo200 manometer produced by Gymna, Bilzen, Belgium)—pre-test and post-test. For the EMG test of each of the subjects, a separate intravaginal probe Periform Plus was used (produced by Neen Performance Health, Nottinghamshire, UK).
- (3)
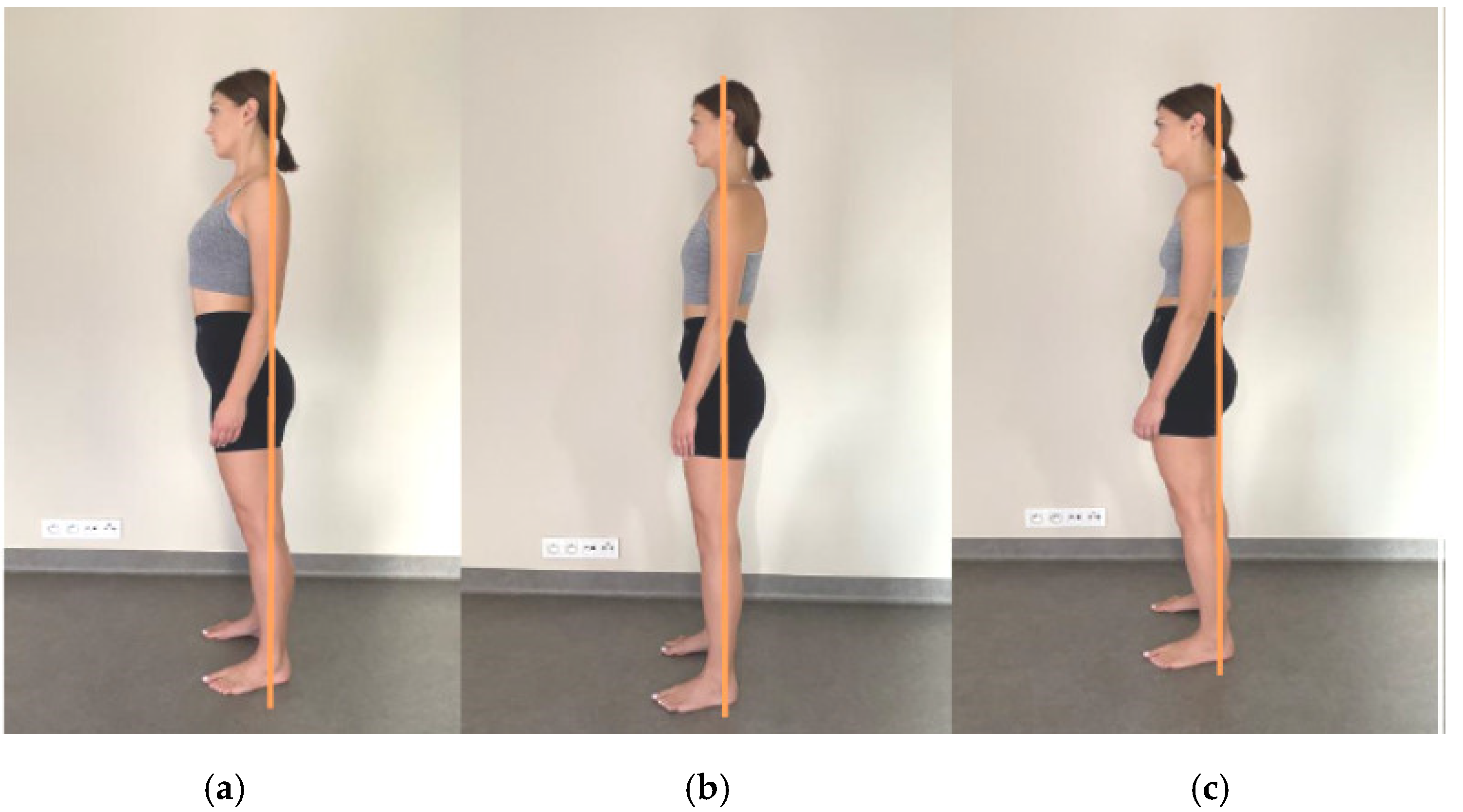
- Subjective assessment of body posture in the sagittal plane according to the McKenzie methodology—mechanical diagnosis and therapy (ear lobe projection)—used in the therapeutic part (information for the person performing the therapy as well as education for the subject on how to assume the correct body posture).
2.1. Education
- (1)
- Information on the anatomy and function of pelvic floor muscles. Anatomy chart presentation.
- (2)
- Perception exercises: self-palpation of bony anatomical landmarks (anterior superior iliac spines, the ilium, the sacrum, the coccyx, the ischial tuberosities, the pubic symphysis) when seated in a chair, with or without a tennis ball.
- (3)
- The activity of pelvic floor muscles during activities of daily life: sitting and standing positions and their corrections, positions to take when sneezing/coughing, in the toilet, and during physical activity.
- (4)
- Learning the correct activation of pelvic floor muscles in lower positions and without load (depending on the needs of the assessed subject); instructions “exhale and then tighten the anus and the urethra, then pull your perineum up, as if you wanted to pull in a tampon into your vagina”.
- (5)
- Learning how to correct one’s posture during activities of daily living.
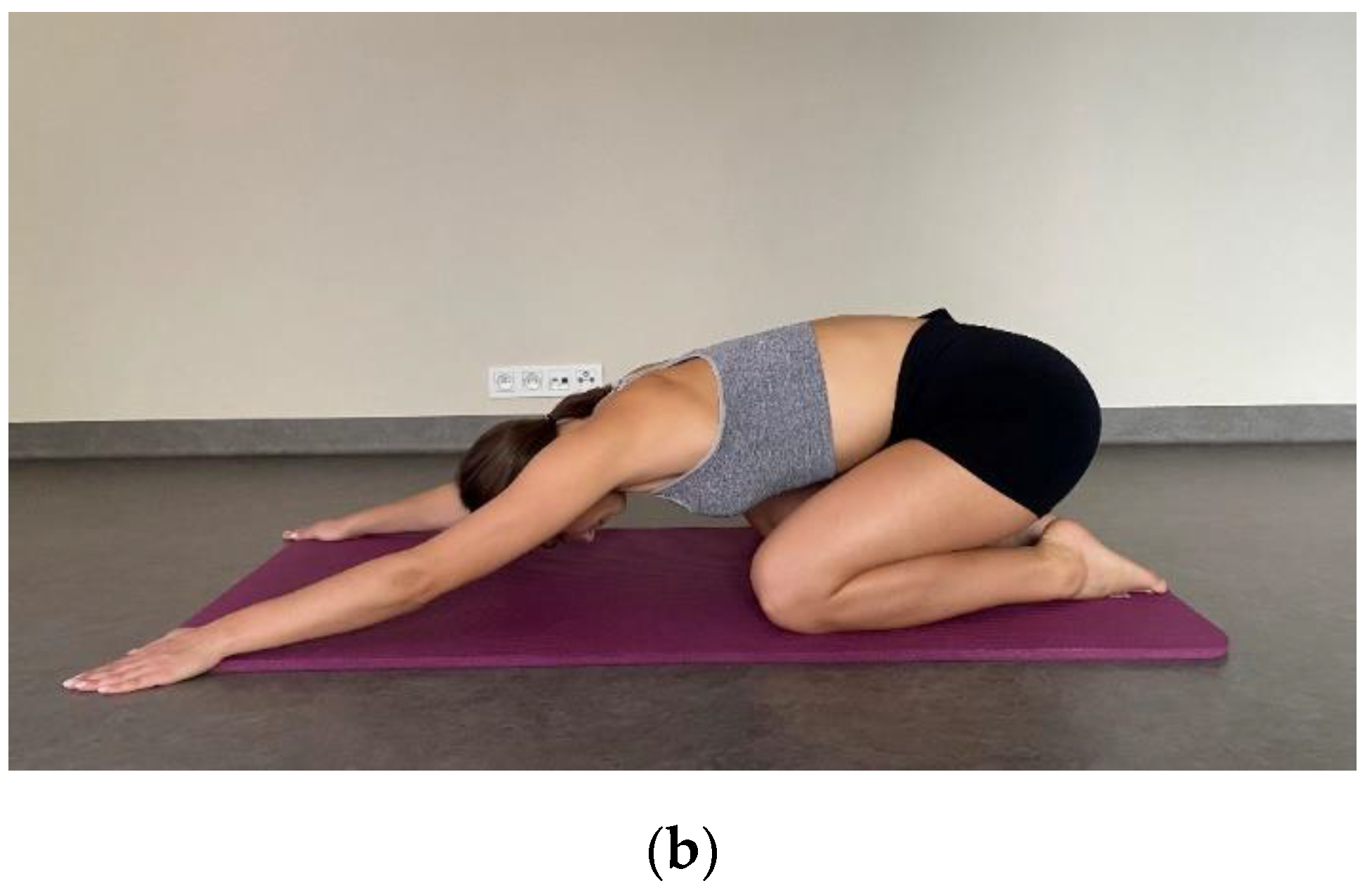
2.2. Posture Correction Therapy
2.3. Statistical Analysis
3. Results
3.1. The Implemented Therapeutic Programme and Pelvic Floor Muscles at Rest
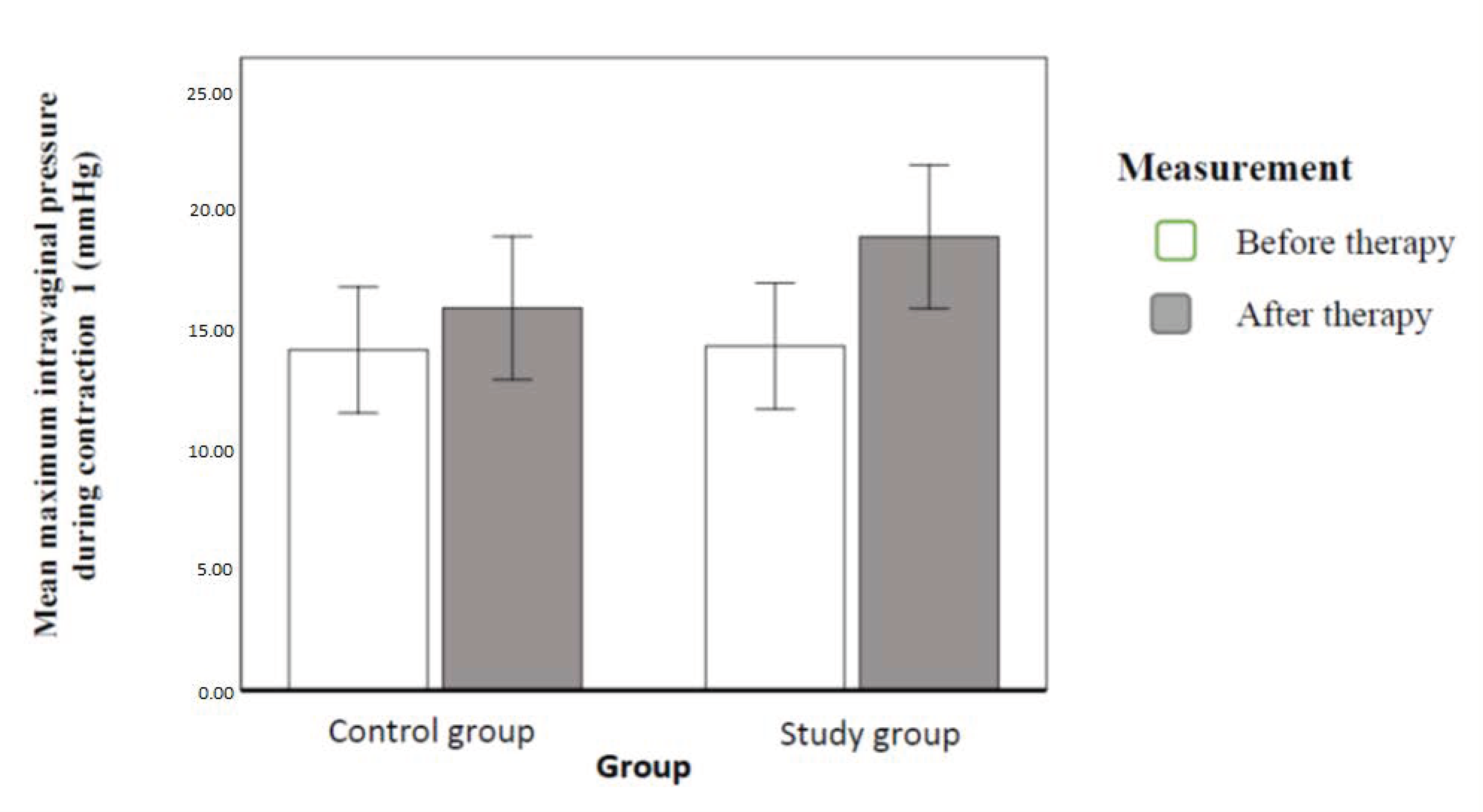
3.2. The Implemented Therapeutic Programme and Pelvic Floor Muscle Tension Parameters
4. Discussion
4.1. Electromyography
4.2. Palpation Examination
4.3. Manometry
5. Conclusions
- (1)
- Education of the pelvic floor and change of habits statistically significantly affect the activity of PFM. It decreases PFM tension at rest and increases PFM power and endurance during MVC.
- (2)
- Posture correction therapy in the sagittal plane (manual therapy and stretching exercise) did not have a significant impact on PFM in comparison to education in the study population. We recommend in the therapy of patients with stress urinary incontinence of the I and II degree to start physiotherapy with education and training in autotherapy.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Comerford, M.; Mottram, S. Kinetic Control–Ocena i Reedukacja Nieskoordynowanego Ruchu; Edra Urban & Partner: Wrocław, Poland, 2012. [Google Scholar]
- Gruszczyńska, D.; Dąbek, A.; Rekowski, W. Diastasis recti abdominis–what may cause it in postpartum women? Adv. Rehabil. 2021, 35, 24–31. [Google Scholar] [CrossRef]
- Hodges, P.W.; Sapsford, R.; Pangel, H.M. Feedforward Activity of the Pelvic Floor Muscles Precedes Rapid Upper Limb Movements; Australian Physiotherapy Association: Melbourne, VIC, Australia, 2002. [Google Scholar]
- Cordo, P.J.; Nashner, L.M. Properties of postural adjustments associated with rapid arm movements. J. Neurophysiol. 1982, 47, 287–302. [Google Scholar] [CrossRef] [PubMed]
- Lee, K. Investigation of Electromyographic Activity of Pelvic Floor Muscles in Different Body Positions to Prevent Urinary Incontinence. Med. Sci. Monit. 2019, 25, 9357–9363. [Google Scholar] [CrossRef] [PubMed]
- Ansarian, M.; Gharamaleki, M.E.; Ghaderi, F. The relationship between stress urinary incontinence in women and flat foot by using two methods. Adv. Environ. Biol. 2014, 8, 377–386. [Google Scholar]
- Cerruto, M.; Vedovi, E.; Mantovani, W.; D’Elia, C.; Artibani, W. Effects of ankle position on pelvic floor muscle electromyographic activity in female stress urinary incontinence: Preliminary reduta from a pilot study. Arch. Ital. Urol. Androl. 2012, 84, 184–188. [Google Scholar] [PubMed]
- Haugstad, G.K.; Haugstad, T.S.; Kirste, U.M.; Leganger, S.; Wojniusz, S.; Klemmetsen, I.; Malt, U.F. Posture, movement patterns, and body awareness in women with chronic pelvic pain. J. Psychosom. Res. 2006, 61, 637–644. [Google Scholar] [CrossRef]
- Meyer, I.; McArthur, T.A.; Tang, Y.; McKinney, J.L.; Morgan, S.L.; Richter, H.E. Pelvic floor symptoms and spinal curvatue in women. Female Pelvic Med. Reconstr. Surg. 2016, 22, 219–223. [Google Scholar] [CrossRef] [Green Version]
- Miranda, R.; Schor, E.; Girã, M.J. Postural evaluation in women with chronic pelvic pain. Rev. Bras. Ginecol. Obstet. 2009, 31, 353–560. [Google Scholar]
- Montenegro, M.L.; Mateus-Vasconcelos, E.C.; E Silva, J.C.R.; Dos Reis, F.J.C.; A Nogueira, A.; Poli-Neto, O.B. Postural changes in women with chronic pelvic pain: A case control study. BMC Musculoskelet. Disord. 2009, 10, 82. [Google Scholar] [CrossRef]
- Nguyen, J.K.; Lind, L.R.; Choe, J.Y. Lumbosacral spine and pelvic inlet changes associated with pelvic organ prolapse. Obstet Gynecol. 2000, 95, 332–336. [Google Scholar]
- Nygaard, I.E.; Wacki, C.G.; Saltzman, C.L. Relationship between foot flexibility and urinary incontinence in nulliparous varsity athletes. Obstet Gynecol. 1996, 87, 1049–1051. [Google Scholar] [CrossRef] [PubMed]
- Zhoolideh, P.; Ghaderi, F.; Salahzadeh, Z. Are There any Relations Between Posture and Pelvic Floor Disorders? A Literature Review. Crescent J. Med. Biol. Sci. 2017, 4, 153–159. [Google Scholar]
- Myers, T.M. Taśmy Anatomiczne. Meridiany Mięśniowo-Powięziowe dla Terapeutów Manualnych i Specjalistów Leczenia Ruchem; DB Publishing: Warszawa, Poland, 2015. [Google Scholar]
- George, D.; Mallery, P. IBM SPSS Statistics 23 Step by Step: A Simple Guide and Reference, 14th ed.; Routledge: New York, NY, USA, 2016. [Google Scholar]
- Kędziorek, J.; Błażkiewicz, M. Effect of voluntary muscle contraction on postural stability in healthy adults. Adv. Rehabil. 2021, 35, 33–37. [Google Scholar] [CrossRef]
- Feldman, A.G. The Relationship Between Postural and Movement Stability. Adv. Exp. Med. Biol. 2016, 957, 105–120. [Google Scholar]
- Kendall, F.P.; McCreary, E.K.; Provance, P.G. Muscles: Testing and Function, 4th ed.; Williams and Wilkins: Baltimore, MD, USA, 1993. [Google Scholar]
- McKenzie, R.; May, S. The Lumbar Spine Mechanical Diagnosis & Therapy Vol I; Spinal Publications: Raumati Beach, New Zealand, 2003. [Google Scholar]
- Kasper-Jędrzejewska, M.; Jędrzejewski, G.; Ptaszkowska, L.; Ptaszkowski, K.; Schleip, R.; Halski, T. The Rolf Method of Structural Integration and Pelvic Floor Muscle Facilitation: Preliminary Results of a Randomized, Interventional Study. J. Clin. Med. 2020, 9, 3981. [Google Scholar] [CrossRef]
- Sheikhhoseini, R.; Arab, A.M. Dry Needling in myofascial tracks in Non-Relaxing Pelvic Floor Dysfunction: A case study. J. Bodyw. Mov. Ther. 2018, 22, 337–340. [Google Scholar] [CrossRef]
- Martins Reis, A.; Oliveira Brito, L.G.; Pignatti Frederice Teixeira, C.; de Araújo, C.C.; Facio, F.A.; Herrmann, V.; Juliato, C.R.T. Is there a Difference in Whole Body Standing Posture in Women with Urinary Incontinence Based on the Presence of Myofascial Dysfunction in the Pelvic Floor Muscles? Phys. Ther. 2021, 101, 171. [Google Scholar] [CrossRef]
- Chmielewska, D.; Stania, M.; Sobota, G.; Kwaśna, K.; Błaszczak, E.; Taradaj, J.; Juras, G. Impact of Different Body Positions on Bioelectrical Activity of the Pelvic Floor Muscles in Nulliparous Continent Women. BioMed Res. Int. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Albaladejo-Belmonte, M.; Tarazona-Motes, M.; Nohales-Alfonso, F.; De-Arriba, M.; Alberola-Rubio, J.; Garcia-Casado, J. Characterization of Pelvic Floor Activity in Healthy Subjects and with Chronic Pelvic Pain: Diagnostic Potential of Surface Electromyography. Sensors 2021, 21, 2225. [Google Scholar] [CrossRef]
- Zawadzka, I.; Truszczyńska-Baszak, A.; Jórasz, K. Urinary incontinence due to chronic disc disease and sciatica. Adv. Rehabilitation 2020, 34, 10–15. [Google Scholar] [CrossRef]
- Laycock, J.; Jerwood, D. Pelvic Floor Muscle Assessment: The PERFECT Scheme. Physiother. 2001, 87, 631–642. [Google Scholar] [CrossRef]
- Antônio, F.I.; Herbert, R.D.; Bø, K.; Rosa-E-Silva, A.C.J.S.; Lara, L.A.S.; Franco, M.D.M.; Ferreira, C.H.J. Pelvic floor muscle training increases pelvic floor muscle strength more in post-menopausal women who are not using hormone therapy than in women who are using hormone therapy: A randomised trial. J. Physiother. 2018, 64, 166–171. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Age (Years) | Body Height (m) | Body Mass (kg) | BMI [kg/m2] |
|---|---|---|---|---|
| Study group | 38.3 ± 5.54 | 1.7 ± 0.05 | 63.4 ± 7.3 | 22.8 ± 2.6 |
| Control Group | 35.5 ± 4.7 | 1.7 ± 0.04 | 63.9 ± 0.04 | 23.2 ± 1.7 |
| Parameter | Description |
|---|---|
| P (power) | PFM (pelvic floor muscles) power during MVC (maximum voluntary contraction) (the Oxford scale 0–5) |
| E (endurance) | Time (in seconds) of maintaining MVC (0–10) |
| R (repetition) | Number of contractions with power P maintaining E for certain amount of time (0–10) |
| F (fast contractions) | Number of fast contractions, lasting for 1 s, with 1 s long relax between contractions (0–10) |
| E (elevation) | Elevation of the perineum (yes/no) |
| C (co-contraction) | Other muscle groups contract during PFM contraction (yet/no) |
| T (timing) | There is involuntary PFM contraction in the coughing test (yes/no) |
| M | Me | SD | Sk. | Kurt. | Min. | Maks. | W | p | |
|---|---|---|---|---|---|---|---|---|---|
| Clinical control group | |||||||||
| Power (PERFECT) 1 | 2.5 | 2 | 1.14 | 0.68 | −0.17 | 1 | 5 | 0.87 | 0.002 |
| Power (PERFECT) 2 | 3.47 | 3 | 0.94 | 0.24 | −0.73 | 2 | 5 | 0.88 | 0.004 |
| Endurance (PERFECT) 1 | 5.03 | 5 | 3.22 | 0.39 | −1.13 | 1 | 10 | 0.89 | 0.005 |
| Endurance (PERFECT) 2 | 9.03 | 10 | 1.67 | −1.33 | 4.73 | 3 | 10 | 0.67 | <0.001 |
| Intravaginal pressure at rest 1 (mmHg) | 1.32 | 1.2 | 1.13 | 1.3 | 2.23 | 0 | 4.9 | 0.87 | 0.002 |
| Intravaginal pressure at rest | 0.45 | 0.5 | 0.46 | 1.69 | 4.81 | 0 | 2.1 | 0.81 | <0.001 |
| 2 (mmHg) | |||||||||
| Mean tension at rest 1 (µV) | 7.52 | 7.45 | 3.09 | 0.2 | 0.05 | 1.4 | 14 | 0.97 | 0.456 |
| Mean tension at rest 2 (µV) | 6.44 | 5.6 | 3.21 | 1.45 | 2.85 | 2 | 16.7 | 0.86 | 0.001 |
| Mean maximum intravaginal pressure during contraction 1 (mmHg) | 14.16 | 14.1 | 5.87 | 0.9 | 0.15 | 7 | 27 | 0.9 | 0.013 |
| Mean maximum intravaginal pressure during contraction 2 (mmHg) | 15.9 | 15.43 | 6.2 | 0.73 | −0.1 | 7.6 | 29.4 | 0.94 | 0.09 |
| Mean tension during contraction 1 (µV) | 27.2 | 24.1 | 9.66 | 0.94 | 0.23 | 16.1 | 50.5 | 0.91 | 0.022 |
| Mean tension during contraction 2 (µV) | 27.99 | 27.25 | 8.78 | 0.71 | 0.09 | 17 | 51 | 0.95 | 0.189 |
| M | Me | SD | Sk. | Kurt. | Min. | Maks. | W | p | |
|---|---|---|---|---|---|---|---|---|---|
| Study population | |||||||||
| Power (PERFECT) 1 | 2.57 | 2 | 1.19 | 0.68 | −0.22 | 1 | 5 | 0.81 | 0.07 |
| Power (PERFECT) 2 | 3.47 | 3 | 1.07 | 0.18 | −1.19 | 2 | 5 | 0.81 | 0.077 |
| Endurance (PERFECT) 1 | 4.57 | 5 | 2.82 | 0.44 | −0.62 | 1 | 10 | 0.81 | 0.069 |
| Endurance (PERFECT) 2 | 6.97 | 7.5 | 3.21 | −0.36 | −1.62 | 2 | 10 | 0.81 | 0.072 |
| Intravaginal pressure at rest 1 (mmHg) | 1.47 | 1.45 | 0.96 | 0.5 | 0.32 | 0 | 3.9 | 0.92 | 0.49 |
| Intravaginal pressure at rest 2 (mmHg) | 0.48 | 0.25 | 0.54 | 1.35 | 1.33 | 0 | 2 | 0.89 | 0.297 |
| Mean tension at rest 1 (µV) | 7.39 | 7.7 | 3.78 | 1.4 | 4.82 | 1.2 | 21.1 | 0.91 | 0.418 |
| Mean tension at rest 2 (µV) | 5.96 | 5.25 | 3.47 | 1.44 | 3.07 | 1.1 | 17.4 | 0.97 | 0.889 |
| Mean maximum intravaginal pressure during contraction 1 (mmHg) | 14.32 | 11.65 | 8.29 | 1.67 | 3.58 | 4.1 | 42.6 | 0.81 | 0.066 |
| Mean maximum intravaginal pressure during contraction 2 (mmHg) | 18.87 | 16.9 | 9.74 | 1.29 | 1.46 | 5.4 | 46.6 | 0.88 | 0.247 |
| Mean tension during contraction 1 (µV) | 24.36 | 20.15 | 14.71 | 0.94 | 0.11 | 8.6 | 61.6 | 0.96 | 0.782 |
| Mean tension during contraction 2 (µV) | 26.71 | 21.85 | 14.78 | 0.95 | −0.03 | 9.8 | 60.5 | 0.91 | 0.47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jórasz, K.; Truszczyńska-Baszak, A.; Dąbek, A. Posture Correction Therapy and Pelvic Floor Muscle Function Assessed by sEMG with Intravaginal Electrode and Manometry in Female with Urinary Incontinence. Int. J. Environ. Res. Public Health 2023, 20, 369. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010369
Jórasz K, Truszczyńska-Baszak A, Dąbek A. Posture Correction Therapy and Pelvic Floor Muscle Function Assessed by sEMG with Intravaginal Electrode and Manometry in Female with Urinary Incontinence. International Journal of Environmental Research and Public Health. 2023; 20(1):369. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010369
Chicago/Turabian StyleJórasz, Katarzyna, Aleksandra Truszczyńska-Baszak, and Aneta Dąbek. 2023. "Posture Correction Therapy and Pelvic Floor Muscle Function Assessed by sEMG with Intravaginal Electrode and Manometry in Female with Urinary Incontinence" International Journal of Environmental Research and Public Health 20, no. 1: 369. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010369