
Nasopharyngeal Carcinoma and Its Effect on Dry Eye Disease: A Nationwide Cohort Study


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
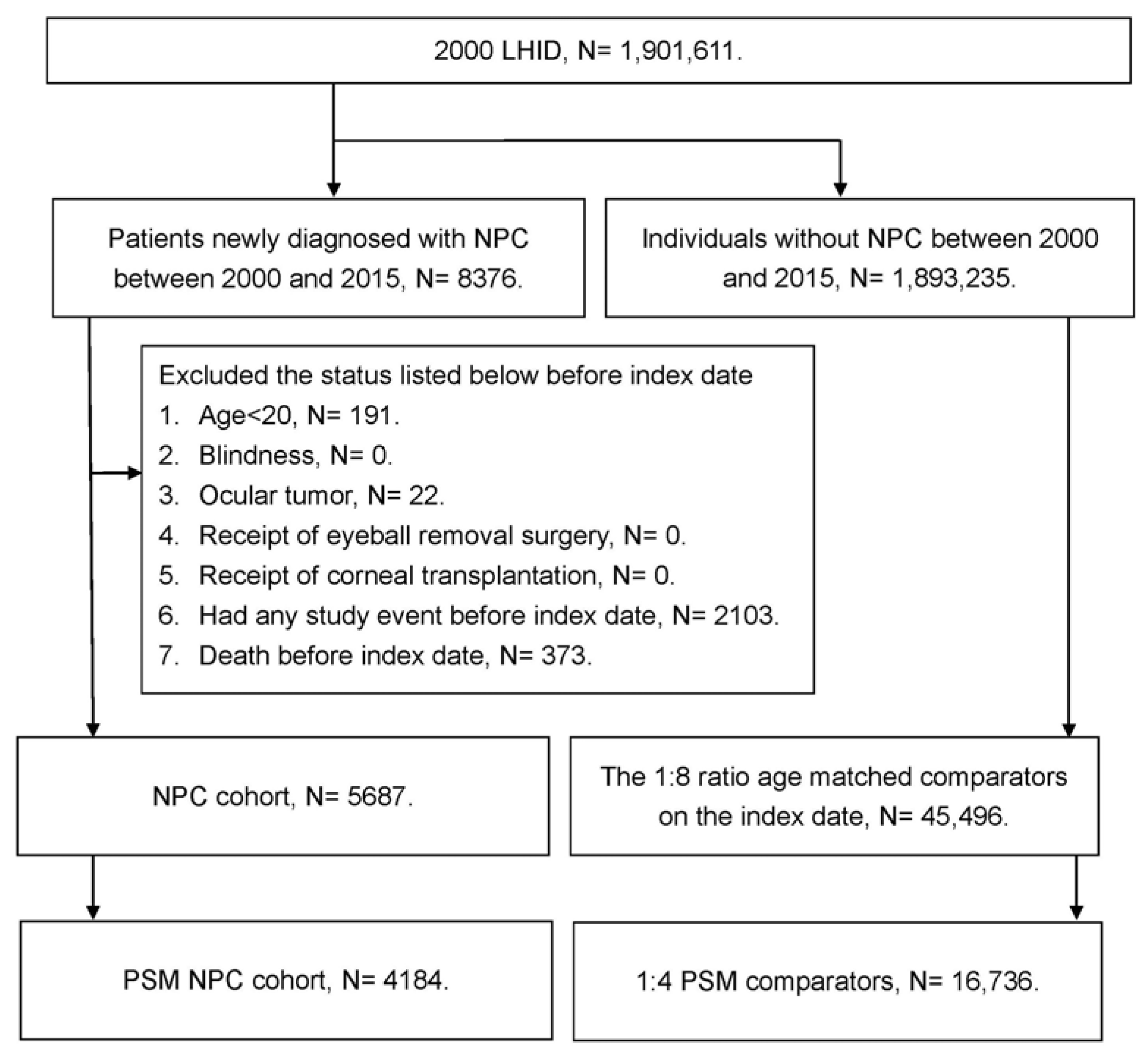
2.2. Patient Selection
2.3. Primary-Outcome Measurement
2.4. Demographic and Comorbidity Covariates
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics in the Non-NPC and NPC Groups
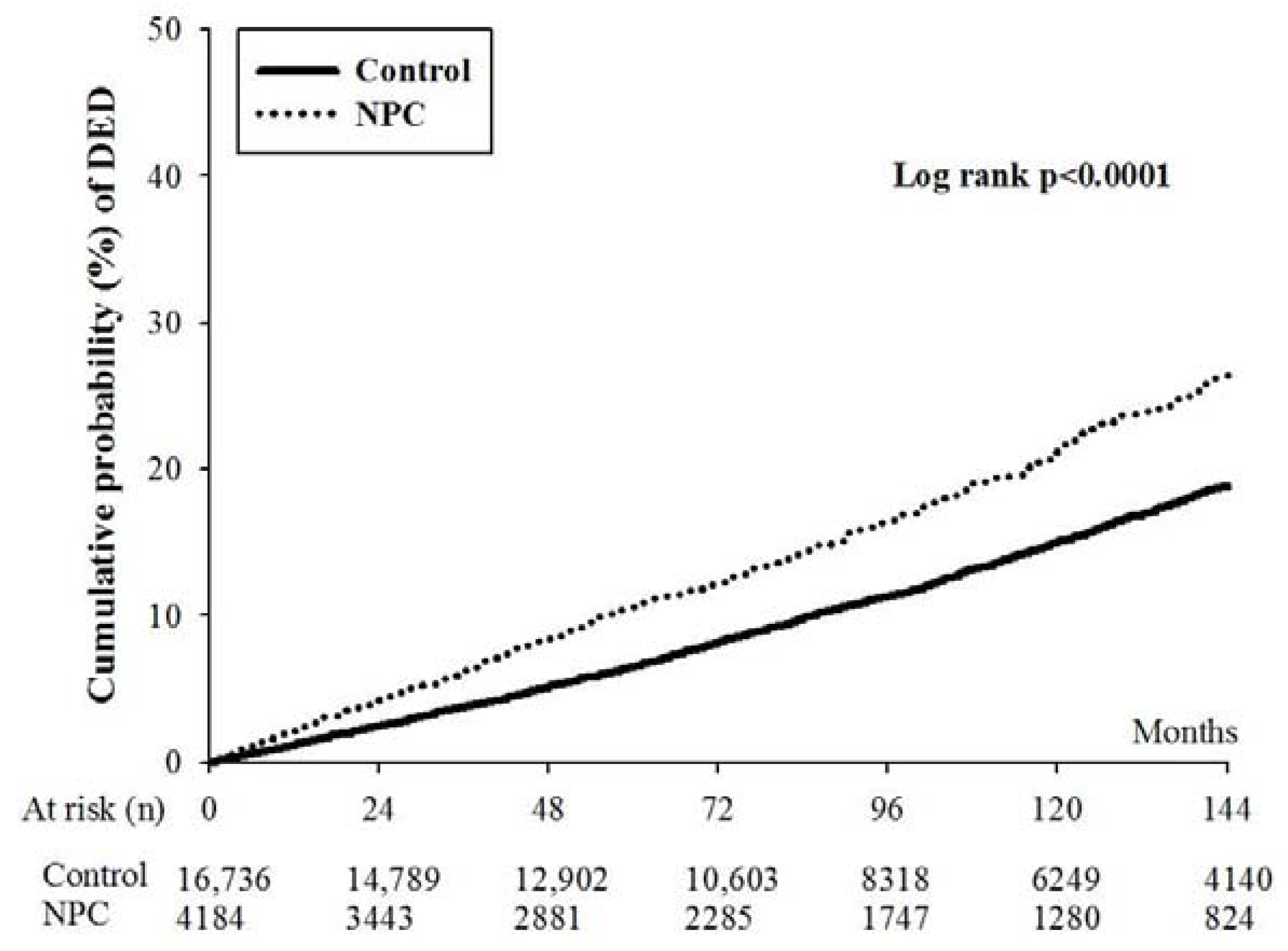
3.2. Risk of DED in NPC and Non-NPC Groups
3.3. The Effect of Radiotherapy and Chemotherapy on the Development of DED
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chua, M.L.K.; Wee, J.T.S.; Hui, E.P.; Chan, A.T.C. Nasopharyngeal carcinoma. Lancet 2016, 387, 1012–1024. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.T.; Ye, W.; Zeng, Y.X.; Adami, H.O. The evolving epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol. Biomarkers Prev. 2021, 30, 1035–1047. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.P.; Chan, A.T.C.; Le, Q.T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Jeyakumar, A.; Brickman, T.M.; Jeyakumar, A.; Doerr, T. Review of nasopharyngeal carcinoma. Ear Nose Throat J. 2006, 85, 168–170, 172–163, 184. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.W.M.; Ng, W.T.; Chan, J.Y.W.; Corry, J.; Mäkitie, A.; Mendenhall, W.M.; Rinaldo, A.; Rodrigo, J.P.; Saba, N.F.; Strojan, P.; et al. Management of locally recurrent nasopharyngeal carcinoma. Cancer Treat. Rev. 2019, 79, 101890. [Google Scholar] [CrossRef]
- Caponigro, F.; Longo, F.; Ionna, F.; Perri, F. Treatment approaches to nasopharyngeal carcinoma: A review. Anticancer Drugs 2010, 21, 471–477. [Google Scholar] [CrossRef]
- Yu, B.; Lin, F.; Duan, J.; Ning, H. The influence of marital status on survival in patients with nasopharyngeal carcinoma: A surveillance, epidemiology, and end results database analysis. Medicine 2022, 101, e30516. [Google Scholar] [CrossRef]
- Wu, L.; Li, C.; Pan, L. Nasopharyngeal carcinoma: A review of current updates. Exp. Ther. Med. 2018, 15, 3687–3692. [Google Scholar] [CrossRef] [Green Version]
- Reffai, A.; Mesmoudi, M.; Derkaoui, T.; Ghailani Nourouti, N.; Barakat, A.; Sellal, N.; Mallick, P.; Bennani Mechita, M. Epidemiological profile and clinicopathological, therapeutic, and prognostic characteristics of nasopharyngeal carcinoma in northern morocco. Cancer Control 2021, 28, 10732748211050587. [Google Scholar] [CrossRef]
- Hung, S.H.; Chen, P.Y.; Lin, H.C.; Ting, J.; Chung, S.D. Association of rhinosinusitis with nasopharyngeal carcinoma: A population-based study. Laryngoscope 2014, 124, 1515–1520. [Google Scholar] [CrossRef]
- Young, Y.H. Irradiated ears in nasopharyngeal carcinoma survivors: A review. Laryngoscope 2019, 129, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Ku, P.K.; Yuen, E.H.; Cheung, D.M.; Chan, B.Y.; Ahuja, A.; Leung, S.F.; Tong, M.C.; van Hasselt, A. Early swallowing problems in a cohort of patients with nasopharyngeal carcinoma: Symptomatology and videofluoroscopic findings. Laryngoscope 2007, 117, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Liang, K.L.; Jiang, R.S.; Lin, J.C.; Chiu, Y.J.; Shiao, J.Y.; Su, M.C.; Hsin, C.H. Central nervous system infection in patients with postirradiated nasopharyngeal carcinoma: A case-controlled study. Am. J. Rhinol. Allergy 2009, 23, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.M.; Wang, A.G. Nasopharyngeal carcinoma with orbital invasion. Eye 2004, 18, 833–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, W.M.; Young, S.M.; Amrith, S. Ophthalmic involvement in nasopharyngeal carcinoma. Orbit 2017, 36, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. Late side effects of radiation treatment for head and neck cancer. Radiat. Oncol. J. 2020, 38, 84–92. [Google Scholar] [CrossRef]
- Clayton, J.A. Dry eye. N. Engl. J. Med. 2018, 378, 2212–2223. [Google Scholar] [CrossRef]
- Tsubota, K.; Pflugfelder, S.C.; Liu, Z.; Baudouin, C.; Kim, H.M.; Messmer, E.M.; Kruse, F.; Liang, L.; Carreno-Galeano, J.T.; Rolando, M.; et al. Defining dry eye from a clinical perspective. Int. J. Mol. Sci. 2020, 21, 9271. [Google Scholar] [CrossRef]
- Lee, K.Y.; Seah, L.L.; Tow, S.; Cullen, J.F.; Fong, K.S. Nasopharyngeal carcinoma with orbital involvement. Ophthalmic Plast. Reconstr. Surg. 2008, 24, 185–189. [Google Scholar] [CrossRef]
- Ko, A.C.; Satterfield, K.R.; Lee, B.W.; Alameddine, R.M.; Korn, B.S.; Kikkawa, D.O. Unilateral alacrima as a presenting symptom of nasopharyngeal carcinoma. Ophthalmic Plast. Reconstr. Surg. 2017, 33, 185–189. [Google Scholar] [CrossRef]
- Wahab, Z.; Tai, E.; Wan Hitam, W.H.; Sonny Teo, K.S. Corticosteroid therapy in optic neuropathy secondary to nasopharyngeal carcinoma. Cureus 2021, 13, e13735. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Wu, Y.; Liao, D.; Zhang, H. Quantitative assessment of the association between interleukin-10 promoter gene polymorphisms and nasopharyngeal carcinoma susceptibility. Minerva Med. 2016, 107, 92–100. [Google Scholar] [PubMed]
- Riley, C.A.; Marino, M.J.; Hawkey, N.; Lawlor, C.M.; McCoul, E.D. Sinonasal tract inflammation as a precursor to nasopharyngeal carcinoma: A systematic review and meta-analysis. Otolaryngol. Head Neck Surg. 2016, 154, 810–816. [Google Scholar] [CrossRef]
- O’Neil, E.C.; Henderson, M.; Massaro-Giordano, M.; Bunya, V.Y. Advances in dry eye disease treatment. Curr. Opin. Ophthalmol. 2019, 30, 166–178. [Google Scholar] [CrossRef] [PubMed]
- De, A.F.G.B.; Santhiago, M.R.; de Azevedo, M.N.; Moraes, H.V., Jr. Evaluation of dry eye signs and symptoms in patients with systemic sclerosis. Graefes Arch. Clin. Exp. Ophthalmol. 2012, 250, 1051–1056. [Google Scholar]
- Bjordal, O.; Norheim, K.B.; Rødahl, E.; Jonsson, R.; Omdal, R. Primary sjögren’s syndrome and the eye. Surv. Ophthalmol. 2020, 65, 119–132. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.Y.; Chen, H.C.; Sun, C.C.; Lin, H.Y.; Lu, K.H.; Huang, J.Y.; Yeh, C.B.; Yang, S.F. Gout as a risk factor for dry eye disease: A population-based cohort study. J. Clin. Med. 2019, 8, 62. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.Y.; Yang, K.L.; Sun, C.C.; Huang, J.Y.; Chen, H.C.; Chen, H.C.; Yang, S.F. The development of dry eye disease after surgery-indicated chronic rhinosinusitis: A population-based cohort study. Int. J. Environ. Res. Public Health 2020, 17, 3829. [Google Scholar] [CrossRef]
- Lin, K.T.; Lee, S.Y.; Liu, S.C.; Tsao, C.C.; Hsu, S.D.; Chien, W.C.; Chung, C.H.; Chang, W.K.; Chen, Y.W.; Lin, C.S. Risk of ocular complications following radiation therapy in patients with nasopharyngeal carcinoma. Laryngoscope 2020, 130, 1270–1277. [Google Scholar] [CrossRef]
- Rouen, P.A.; White, M.L. Dry eye disease: Prevalence, assessment, and management. Home Healthc. Now 2018, 36, 74–83. [Google Scholar] [CrossRef]
- Tsao, S.W.; Yip, Y.L.; Tsang, C.M.; Pang, P.S.; Lau, V.M.; Zhang, G.; Lo, K.W. Etiological factors of nasopharyngeal carcinoma. Oral Oncol. 2014, 50, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Bikbov, M.M.; Kazakbaeva, G.M.; Rakhimova, E.M.; Rusakova, I.A.; Fakhretdinova, A.A.; Tuliakova, A.M.; Panda-Jonas, S.; Gilmanshin, T.R.; Zainullin, R.M.; Bolshakova, N.I.; et al. The prevalence of dry eye in a very old population. Acta Ophthalmol. 2022, 100, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Serefoglu Cabuk, K.; Cakir, İ.; Kirgiz, A.; Atalay, K.; Taskapili, M. Dry eye disease in patients with metabolic syndrome. Saudi Med. J. 2016, 37, 1334–1338. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, A.; Modugno, R.L.; Salami, E. Allergy and dry eye disease. Ocul. Immunol. Inflamm. 2021, 29, 1168–1176. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characters | Non-NPC Group | NPC Group | ASD |
|---|---|---|---|
| N | 16,736 | 4184 | |
| Sex | 0.0244 | ||
| Female | 5952 (35.56%) | 1537 (36.74%) | |
| Male | 10784 (64.44%) | 2647 (63.26%) | |
| Age (mean ± SD) | 49.0 ± 13.8 | 49.7 ± 14.1 | 0.0567 |
| 20–30 | 1349 (8.06%) | 326 (7.79%) | |
| 30–40 | 2914 (17.41%) | 687 (16.42%) | |
| 40–50 | 4485 (26.80%) | 1100 (26.29%) | |
| 50–60 | 4363 (26.07%) | 1078 (25.76%) | |
| 60–70 | 2285 (13.65%) | 607 (14.51%) | |
| 70–80 | 1032 (6.17%) | 300 (7.17%) | |
| 80–100 | 308 (1.84%) | 86 (2.06%) | |
| Marital status | 0.0532 | ||
| Unmarried | 2868 (17.14%) | 684 (16.35%) | |
| Married | 12,262 (73.27%) | 3063 (73.21%) | |
| Divorced | 995 (5.95%) | 262 (6.26%) | |
| Widowed | 611 (3.65%) | 175 (4.18%) | |
| Education level | 0.0447 | ||
| Elementary school or below | 4851 (28.99%) | 1264 (30.21%) | |
| Junior high school | 3023 (18.06%) | 775 (18.52%) | |
| Senior high school | 6916 (41.32%) | 1666 (39.82%) | |
| University or above | 1946 (11.63%) | 479 (11.45%) | |
| Comorbidities | |||
| Hypertension | 3148 (18.81%) | 851 (20.34%) | 0.0386 |
| Diabetes mellitus | 1567 (9.36%) | 407 (9.73%) | 0.0124 |
| Stable CAD | 683 (4.08%) | 210 (5.02%) | 0.0450 |
| Hyperlipidemia | 1529 (9.14%) | 424 (10.13%) | 0.0338 |
| Cerebrovascular disease | 752 (4.49%) | 201 (4.80%) | 0.0148 |
| Allergic pulmonary diseases | 1348 (8.05%) | 456 (10.90%) | 0.0972 |
| Rheumatic disease | 132 (0.79%) | 46 (1.10%) | 0.0321 |
| Allergic otolaryngologic diseases | 398 (2.38%) | 99 (2.37%) | 0.0008 |
| Allergic dermatological diseases | 3240 (19.36%) | 843 (20.15%) | 0.0198 |
| Chemotherapy | 1584 (37.9%) | ||
| Low dose radiotherapy | 922 (22.0%) | ||
| High dose radiotherapy | 934 (22.3%) |
| Outcome | Non-NPC Group | NPC Group |
|---|---|---|
| N | 16736 | 4184 |
| Person-months | 1603235 | 353946 |
| Event | 2225 | 717 |
| Crude HR (95% CI) * | Reference | 1.48 (1.36–1.61) |
| aHR (95% CI) | Reference | 1.45 (1.33–1.58) |
| Parameters | aHR (95% CI) | p Value |
|---|---|---|
| NPC | 1.45 (1.33–1.58) | <0.0001 * |
| Sex (ref = Female) | ||
| Male | 0.45 (0.42–0.49) | <0.0001 * |
| Age (ref = 30–40) | ||
| 20–30 | 0.88 (0.72–1.08) | 0.2175 |
| 40–50 | 1.32 (1.16–1.50) | <0.0001 * |
| 50–60 | 1.98 (1.74–2.26) | <0.0001 * |
| 60–70 | 2.31 (1.98–2.71) | <0.0001 * |
| 70–80 | 2.36 (1.94–2.88) | <0.0001 * |
| 80–100 | 1.73 (1.20–2.50) | 0.0034* |
| Marital status (ref = Married) | ||
| Unmarried | 0.92 (0.80–1.07) | 0.2730 |
| Divorced | 0.93 (0.79–1.10) | 0.4004 |
| Widowed | 0.83 (0.69–0.98) | 0.0295 * |
| Education (ref = Junior high school) | ||
| Elementary school or below | 1.02 (0.90–1.15) | 0.7483 |
| Senior high school | 1.18 (1.06–1.33) | 0.0040 * |
| University or above | 1.44 (1.24–1.67) | <0.0001 * |
| Comorbidities | ||
| Hypertension | 1.14 (1.03–1.26) | 0.0130 * |
| DM | 1.17 (1.03–1.32) | 0.0140 * |
| Stable CAD | 1.08 (0.92–1.28) | 0.3360 |
| Hyperlipidemia | 1.09 (0.96–1.24) | 0.1651 |
| Cerebrovascular disease | 1.02 (0.86–1.21) | 0.8558 |
| Allergic pulmonary diseases | 1.18 (1.05–1.32) | 0.0060 * |
| Rheumatic disease | 1.20 (0.88–1.63) | 0.2547 |
| Allergic otolaryngologic diseases | 1.28 (1.05–1.55) | 0.0136 * |
| Allergic dermatological diseases | 1.22 (1.12–1.33) | <0.0001 * |
| Outcome | Non-NPC Group (N = 16,736) | NPC Without Radiotherapy (N = 2328) | NPC With Low-Dose Radiotherapy (N = 922) | NPC With High-Dose Radiotherapy (N = 934) |
|---|---|---|---|---|
| Person-months # | 1,603,235 | 322,389 | 17,834 | 13,723 |
| DED event | 2225 | 635 | 52 | 30 |
| aHR (95% CI) | 0.705 (0.645–0.770) * | Reference | 1.528 (0.733–2.323) | 1.110 (0.770–1.601) |
| Outcome | Non-NPC Group (N = 16,736) | NPC Without Chemotherapy (N = 2600) | NPC With Chemotherapy (N = 1584) |
|---|---|---|---|
| Person-months # | 1,603,235 | 330,107 | 23,839 |
| Event of DED | 2225 | 661 | 56 |
| aHR (95% CI) | 0.693 (0.636–0.756) * | Reference | 1.456 (1.098–1.931) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-T.; Yang, S.-F.; Chao, S.-C.; Lee, C.-Y.; Huang, J.-Y.; Lin, H.-Y. Nasopharyngeal Carcinoma and Its Effect on Dry Eye Disease: A Nationwide Cohort Study. Int. J. Environ. Res. Public Health 2023, 20, 387. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010387
Chen C-T, Yang S-F, Chao S-C, Lee C-Y, Huang J-Y, Lin H-Y. Nasopharyngeal Carcinoma and Its Effect on Dry Eye Disease: A Nationwide Cohort Study. International Journal of Environmental Research and Public Health. 2023; 20(1):387. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010387
Chicago/Turabian StyleChen, Ching-Tai, Shun-Fa Yang, Shih-Chun Chao, Chia-Yi Lee, Jing-Yang Huang, and Hung-Yu Lin. 2023. "Nasopharyngeal Carcinoma and Its Effect on Dry Eye Disease: A Nationwide Cohort Study" International Journal of Environmental Research and Public Health 20, no. 1: 387. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010387