
Telerehabilitation in the Finnish Outpatient Rehabilitation Setting from the Perspective of the Socio-Technical Systems Theory

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Approach
2.2. Study Setting and Participants
2.3. Data Collection
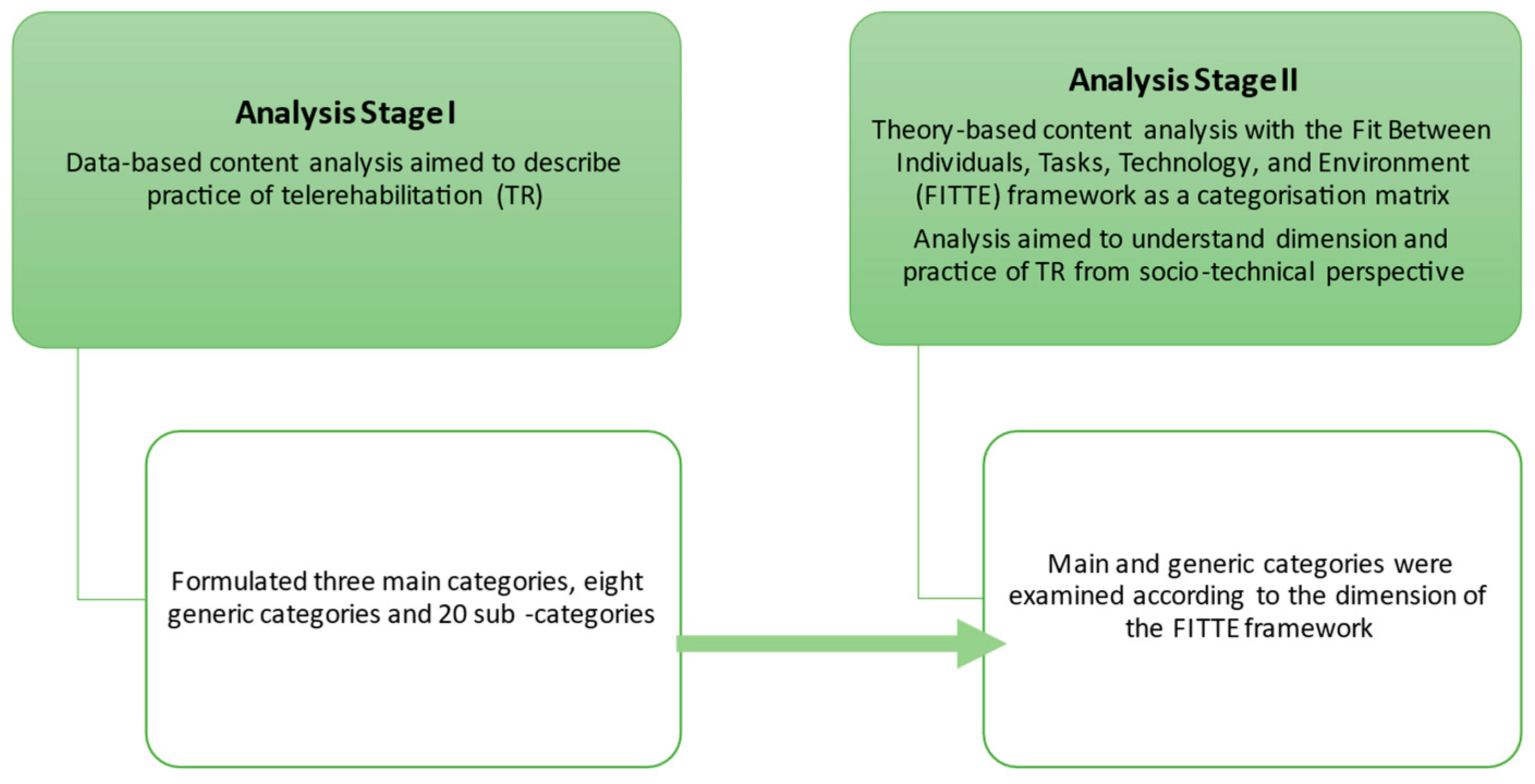
2.4. Data Analysis
3. Results
3.1. Data-Based Content Analysis
Moving to telerehabilitation may have brought some new dimensions and aspects of everyday life to rehabilitation, which we were able to advance through the already developed process.(Music therapist)
With some, our work approach included more guiding of everyday life. A lot of knowledge and information and tips were forwarded to everyday life.(Music therapist)
For the most part, the goals are everyday-life-oriented, which makes it possible to apply the methods in telerehabilitation too.(Occupational therapist)
The more challenging exercises are not safe to perform remotely, and the equipment available at home is not versatile enough.(Physiotherapist)
With young rehabilitees, the supportive person and the parent play a big role in guiding the rehabilitee. If a supportive person could not be found in the rehabilitee’s everyday life for the duration of therapy, telerehabilitation could not be started.(Music therapist)
With telerehabilitation, I’ve started to pay more attention to the parent as an active participant in therapy. Since I tend to engage the parent in teletherapy even without noticing, it is easier for them to take responsibility for the weekly exercises outside the sessions as well.(Speech and language therapist)
In day care centres, therapy can be implemented by personal assistants guiding the exercises. Works well with guided therapy, the child’s close associate can instruct.(Occupational therapist)
Other methods (e.g., homework) have been considered in the rehabilitation of visual-perceptual difficulties as demonstrating the exercise in practice during rehabilitation sessions is not possible in the same way during remote sessions.(Neuropsychologist)
Body language does not come to its own in remote contact, and clients whose expression or speech comprehension needs to be interpreted and supported in many ways are not, in my opinion, suitable for telerehabilitation.(Speech and language therapist)
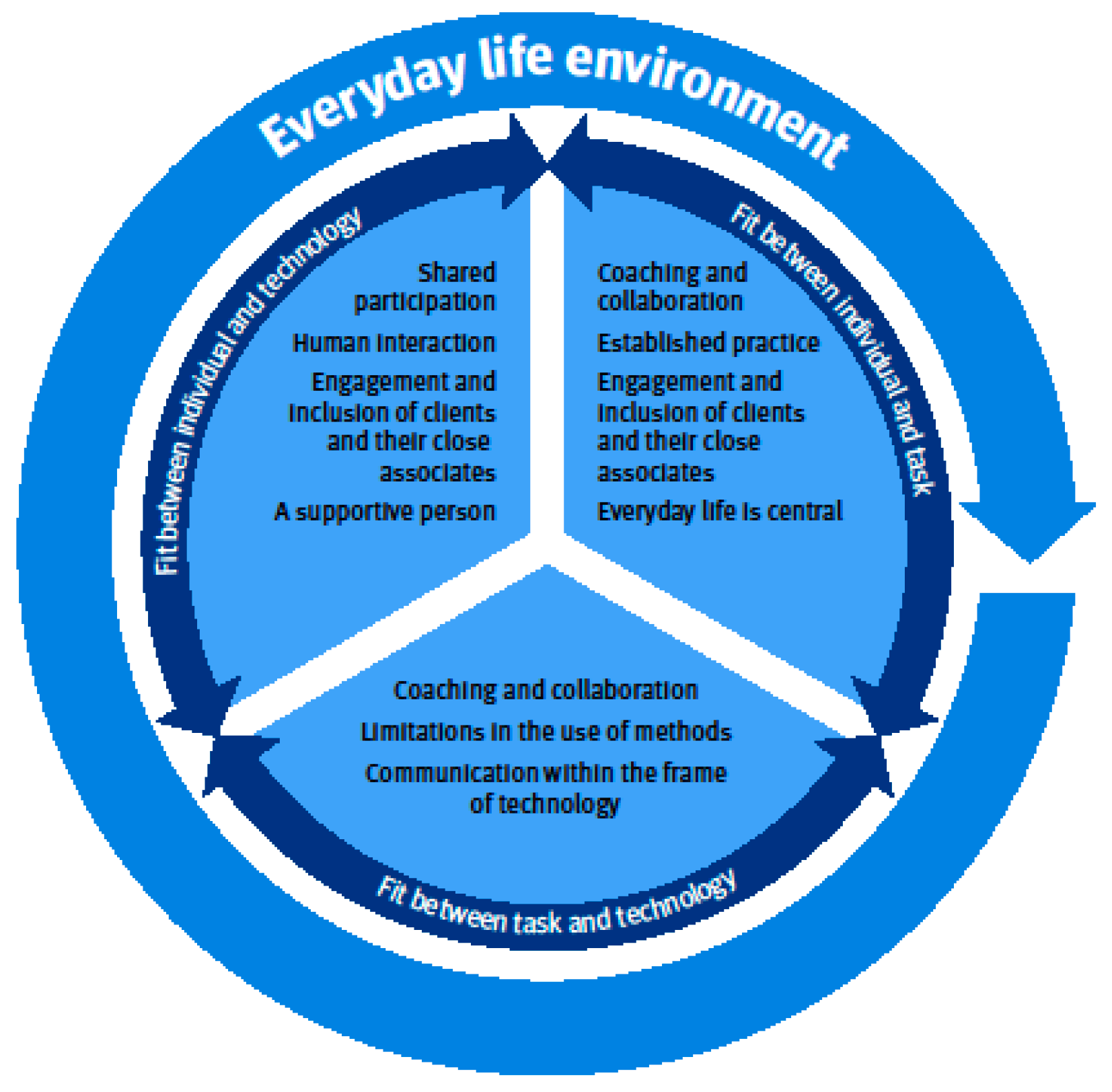
3.2. Theory-Based Analysis with the FITTE Framework
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nanda, M.; Sharma, R. A Review of Patient Satisfaction and Experience with Telemedicine: A Virtual Solution During and Beyond COVID-19 Pandemic. Telemed. E-Health 2021, 27, 1325–1331. [Google Scholar] [CrossRef]
- American Occupational Therapy Association. Telehealth in Occupational Therapy. AOTA Position Paper. Am. J. Occup. Ther. 2018, 72, 1–18. [Google Scholar]
- Heiskanen, T.; Rinne, H.; Miettinen, S.; Salminen, A.-L. Uptake of Tele-Rehabilitation in Finland amongst Rehabilitation Professionals during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18 (Suppl. S2), 4383. [Google Scholar] [CrossRef]
- Nikolaev, V.A.; Nikolaev, A.A. Recent Trends in Telerehabilitation of Stroke Patients: A Narrative Review. NeuroRehabilitation 2022, 51, 1–22. [Google Scholar]
- American Physical Therapy Association. Impact of COVID-19 on the Physical Therapy Profession over One Year; The American Physical Therapy Association: Alexandria, VA, USA, 2021; pp. 10–11. Available online: https://www.apta.org/apta-and-you/news-publications/2021/impact-of-covid-19-on-the-physical-therapy-profession (accessed on 25 May 2023).
- Kreider, C.M.; Hale-Gallardo, J.; Kramer, J.C.; Mburu, S.; Slamka, M.R.; Findley, K.E.; Myers, K.J.; Romero, S. Providers’ Shift to Telerehabilitation at the U.S. Veterans Health Administration during COVID-19: Practical Applications. Front. Public Health 2022, 10, 831762. [Google Scholar] [CrossRef]
- Szekeres, M.; Valdes, K. Virtual Health Care & Telehealth: Current Therapy Practice Patterns. J. Hand Ther. 2022, 35, 124–130. [Google Scholar]
- Scott Kruse, C.; Karem, P.; Shifflett, K.; Vegi, L.; Ravi, K.; Brooks, M. Evaluating Barriers to Adopting Telemedicine Worldwide: A Systematic Review. J. Telemed. Telecare 2018, 24, 4–12. [Google Scholar] [CrossRef] [Green Version]
- Buckingham, S.A.; Anil, K.; Demain, S.; Gunn, H.; Jones, R.B.; Kent, B.; Logan, A.; Marsden, J.; Playford, E.D.; Freeman, J. Telerehabilitation for People with Physical Disabilities and Movement Impairment: A Survey of United Kingdom Practitioners. JMIRx Med. 2022, 3, e30516. [Google Scholar] [CrossRef]
- Cramer, S.C.; Dodakian, L.; Le, V.; McKenzie, A.; See, J.; Augsburger, R.; Zhou, R.J.; Raefsky, S.M.; Nguyen, T.; Vanderschelden, B.; et al. A Feasibility Study of Expanded Home-Based Telerehabilitation After Stroke. Front. Neurol. 2021, 11, 611453. [Google Scholar] [CrossRef]
- Beit Yosef, A.; Maeir, T.; Khalailh, F.; Gilboa, Y. Perceived Feasibility of an Occupation-Based Telerehabilitation Intervention for Older Adults with Chronic Health Conditions in Israel. Hong Kong J. Occup. Ther. 2022, 35, 62–70. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, Y.-N.; Sun, Z.-X.; Yan, D.-R.; Chen, Y.-W.; Lin, K.-C.; Ge, X.-J.; Qin, X.-L. Effects of Coaching-Based Teleoccupational Guidance for Home-Based Stroke Survivors and Their Family Caregivers: A Pilot Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 16355. [Google Scholar] [CrossRef]
- Kettlewell, J.; Lindley, R.; Radford, K.; Patel, P.; Bridger, K.; Kellezi, B.; Timmons, S.; Andrews, I.; Fallon, S.; Lannin, N.; et al. Factors Affecting the Delivery and Acceptability of the ROWTATE Telehealth Vocational Rehabilitation Intervention for Traumatic Injury Survivors: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 9744. [Google Scholar] [CrossRef]
- Krasovsky, T.; Silberg, T.; Barak, S.; Eisenstein, E.; Erez, N.; Feldman, I.; Guttman, D.; Liber, P.; Patael, S.Z.; Sarna, H.; et al. Transition to Multidisciplinary Pediatric Telerehabilitation during the COVID-19 Pandemic: Strategy Development and Implementation. Int. J. Environ. Res. Public Health 2021, 18, 1484. [Google Scholar] [CrossRef]
- Bødker, M.; Juul Nielsen, A. Providing Rehabilitation Online—Invisible Work and Diagnostic Agents. J. Health Organ. Manag. 2015, 29, 948–964. [Google Scholar] [CrossRef] [PubMed]
- Pekkarinen, S.; Melkas, H.; Hyypiä, M. Elderly Care and Digital Services: Toward a Sustainable Sociotechnical Transition. In Human-Centered Digitalization and Services; Toivonen, M., Saari, E., Eds.; Translational Systems Sciences; Springer: Singapore, 2019; Volume 19, pp. 259–284. [Google Scholar]
- Alsobayel, H.; Alodaibi, F.; Albarrati, A.; Alsalamah, N.; Alhawas, F.; Alhowimel, A. Does Telerehabilitation Help in Reducing Disability among People with Musculoskeletal Conditions? A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 19, 72. [Google Scholar] [CrossRef]
- Hawley-Hague, H.; Lasrado, R.; Martinez, E.; Stanmore, E.; Tyson, S. A Scoping Review of the Feasibility, Acceptability, and Effects of Physiotherapy Delivered Remotely. Disabil. Rehabil. 2022, 2, 1–17. [Google Scholar] [CrossRef]
- Ammenwerth, E.; Iller, C.; Mahler, C. IT-Adoption and the Interaction of Task, Technology and Individuals: A Fit Framework and a Case Study. BMC Med. Inform. Decis. Mak. 2006, 6, 3. [Google Scholar] [CrossRef] [Green Version]
- Prgomet, M.; Georgiou, A.; Callen, J.; Westbrook, J. Fit Between Individuals, Tasks, Technology, and Environment (FITTE) Framework: A Proposed Extension of FITT to Evaluate and Optimise Health Information Technology Use. Stud. Health Technol. Inform 2019, 21, 744–748. [Google Scholar]
- Kujala, S.; Ammenwerth, E.; Kolanen, H.; Ervast, M. Applying and Extending the FITT Framework to Identify the Challenges and Opportunities of Successful EHealth Services for Patient Self-Management: Qualitative Interview Study. J. Med. Internet Res. 2020, 22, e17696. [Google Scholar] [CrossRef] [PubMed]
- Turpin, M.; Iwama, M.K. Person-Environment-Occupation Models. In Using Occupational Therapy Models in Practice, 1st ed.; Churchill Livingstone Elsevier: Edinburg, UK, 2011; pp. 89–115. [Google Scholar]
- Polatajko, H.J.; Backman, C.; Baptiste, S.; Davis, J.; Eftekhar, P.; Harvey, A.; Jarman, J.; Krupa, T.; Lin, N.; Pentland, W.; et al. Human Occupation in Context. In Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-Being, & Justice through Occupation, 1st ed.; Townsend, E.A., Polatjko, H.J., Eds.; CAOT Publications ACE: Ottawa, ON, Canada, 2007; pp. 37–62. [Google Scholar]
- Christiansen, C.H.; Townsend, E.A. An Introduction to Occupation. In Introduction to Occupation. The Art and Science of Living; Prentice Hall: Upper Saddle River, NJ, USA, 2004; pp. 1–28. [Google Scholar]
- O’Keeffe, M.; Cullinane, P.; Hurley, J.; Leahy, I.; Bunzli, S.; O’Sullivan, P.B.; O’Sullivan, K. What Influences Patient-Therapist Interactions in Musculoskeletal Physical Therapy? Qualitative Systematic Review and Meta-Synthesis. Phys. Ther. 2016, 96, 609–622. [Google Scholar]
- Babatunde, F.; MacDermid, J.; MacIntyre, N. Characteristics of Therapeutic Alliance in Musculoskeletal Physiotherapy and Occupational Therapy Practice: A Scoping Review of the Literature. BMC Health Serv. Res. 2017, 17, 375. [Google Scholar]
- Intensive Medical Rehabilitation. Available online: https://www.kela.fi/intensive-medical-rehabilitation (accessed on 25 May 2023).
- Rouder, J.; Saucier, O.; Kinder, R.; Jans, M. What to Do with All Those Open-Ended Responses? Data Visualization Techniques for Survey Researchers. Surv. Pract. 2021, 14, 1–9. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lindgren, B.-M.; Lundman, B. Methodological Challenges in Qualitative Content Analysis: A Discussion Paper. Nurse Educ. Today 2017, 56, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngäs, H. The Qualitative Content Analysis Process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Vears, D.F.; Gillam, L. Inductive Content Analysis: A Guide for Beginning Qualitative Researchers. Focus Health Prof. Educ. 2022, 23, 111–127. [Google Scholar] [CrossRef]
- Atlas.ti. Available online: https://atlasti.com/ (accessed on 25 May 2023).
- Oswald, A.G. Improving Outcomes with Qualitative Data Analysis Software: A Reflective Journey. Qual. Soc. Work. 2019, 18, 436–442. [Google Scholar] [CrossRef]
- The Application of ATLAS.Ti in Different Qualitative Data Analysis Strategies. BEST PRACTICE 2023. Available online: https://atlasti.com/research-hub/the-application-of-atlas-ti-in-different-qualitative-data-analysis-strategies (accessed on 25 May 2023).
- Dinesen, B.; Nielsen, G.; Andreasen, J.J.; Spindler, H. Integration of Rehabilitation Activities into Everyday Life through Telerehabilitation: Qualitative Study of Cardiac Patients and Their Partners. J. Med. Internet Res. 2019, 21, e13281. [Google Scholar] [CrossRef]
- Lawford, B.J.; Delany, C.; Bennell, K.L.; Hinman, R.S. “I Was Really Pleasantly Surprised”: Firsthand Experience and Shifts in Physical Therapist Perceptions of Telephone-Delivered Exercise Therapy for Knee Osteoarthritis–A Qualitative Study. Arthritis Care Res. 2019, 71, 545–557. [Google Scholar] [CrossRef]
- Kessler, D.; Anderson, N.D.; Dawson, D.R. Occupational Performance Coaching for Stroke Survivors Delivered via Telerehabilitation Using a Single-Case Experimental Design. Br. J. Occup. Ther. 2021, 84, 488–496. [Google Scholar] [CrossRef]
- Macdonald, G.; Townsend, A.; Adam, P.; Li, L.; Kerr, S.; McDonald, M.; Backman, C. eHealth Technologies, Multimorbidity, and the Office Visit: Qualitative Interview Study on the Perspectives of Physicians and Nurses. J. Med. Internet Res. 2018, 20, e31. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Profession | N | % |
|---|---|---|
| Physiotherapist | 249 | 40 |
| Speech and language therapist | 195 | 31 |
| Occupational therapist | 140 | 22 |
| Music therapist | 27 | 4 |
| Neuropsychologist | 18 | 3 |
| Total | 629 | 100.00 |
| Open-Ended Question | Responses (n) | Pages | Words |
|---|---|---|---|
| You can share your thoughts on the impact of the COVID-19 pandemic on your work and telerehabilitation | 356 | 47 | 19,959 |
| Have there been changes in the duration and frequency of therapy visits due to telerehabilitation? | 197 | 9 | 1801 |
| Have there been changes in the goals of the therapy due to telerehabilitation? | 184 | 9 | 1933 |
| With what kind of clients has tele-rehabilitation not been a possible method of rehabilitation? | 176 | 13 | 4044 |
| With what kind of clients have you started implementing telerehabilitation? | 185 | 14 | 4064 |
| Total | 92 | 31,801 |
| Main Category | Generic Category | Subcategory |
|---|---|---|
| Everyday-life centred | Everyday life is central | Part of everyday life and everyday events |
| Goals based on everyday life | ||
| Everyday life environment | Safe training in everyday environments | |
| Use of places, therapeutic equipment, and materials | ||
| Shared participation | A supportive person | Need for a supportive person/an assistant |
| Assistant’s/supportive person’s competence | ||
| Human interaction | Third party interaction | |
| Maintaining interaction | ||
| Engagement and inclusion of clients and their close associates | Inclusion of the client’s close associates | |
| Commitment and responsibility | ||
| Coaching and collaboration | Established practice | Guidance and coaching methods |
| Self-directed training/exercise | ||
| Contents of therapy and the choice of methods | ||
| Therapy practice in a technological frame | ||
| Limitations in the use of methods | Observation, assessments, and evaluation | |
| Manual guidance and tactile methods | ||
| Physical presence and shared activity | ||
| Communication within the frame of technology | Contact is limited by technology | |
| The importance of speech and language skills | ||
| Shared language |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Partanen, T.; Seppänen-Järvelä, R.; Hiekkala, S.; Lindh, J. Telerehabilitation in the Finnish Outpatient Rehabilitation Setting from the Perspective of the Socio-Technical Systems Theory. Int. J. Environ. Res. Public Health 2023, 20, 6519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20156519
Partanen T, Seppänen-Järvelä R, Hiekkala S, Lindh J. Telerehabilitation in the Finnish Outpatient Rehabilitation Setting from the Perspective of the Socio-Technical Systems Theory. International Journal of Environmental Research and Public Health. 2023; 20(15):6519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20156519
Chicago/Turabian StylePartanen, Tuija, Riitta Seppänen-Järvelä, Sinikka Hiekkala, and Jari Lindh. 2023. "Telerehabilitation in the Finnish Outpatient Rehabilitation Setting from the Perspective of the Socio-Technical Systems Theory" International Journal of Environmental Research and Public Health 20, no. 15: 6519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20156519