
Research on the Application of Artificial Intelligence in Public Health Management: Leveraging Artificial Intelligence to Improve COVID-19 CT Image Diagnosis

(This article belongs to the Section Digital Health)
Abstract
:1. Introduction
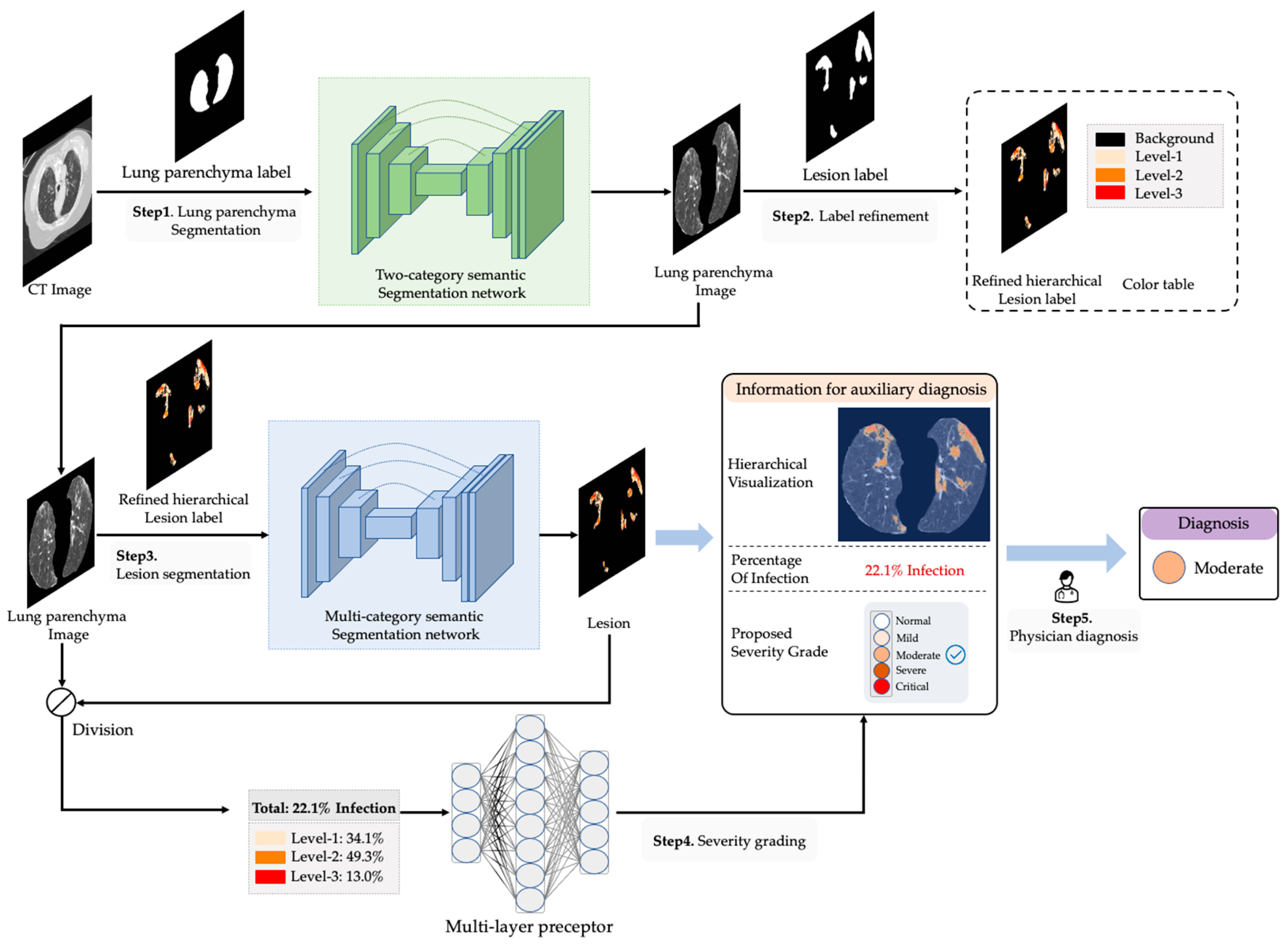
- In order to improve the performance of segmentation on COVID-19 infection, a label refinement method is proposed to refine the existing labels from rough to precise. The refinement reassigns the incorrectly labeled pixels and enables the network to learn the infection degree of each infected pixel.
- Aiming to assist physicians in the efficient diagnosis of COVID-19, a deep learning-aided system (named DLSHELPER) using refined hierarchical labels is proposed. DLSHELPER provides rich auxiliary diagnostic information, including the proposed severity grade, proportion of infected area and infected area visualization.
- We validate the accuracy of our method for COVID-19 lesion segmentation and grading on public COVID-19 CT datasets.
2. Related Work
3. Method
3.1. Overview
3.2. Label Refinement
3.3. Lung and Lesion Segmentation
3.4. Severity Grading
4. Experiments and Analysis
4.1. Implementation and Evaluation
4.2. Evaluation of Lung Segmentation
4.3. Evaluation of COVID-19 Lesion Segmentation Using Refined Hierarchical Labels
4.4. Evaluation of COVID-19 Severity Grading
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Zhang, P.; Zhong, Y.; Deng, Y.; Tang, X.; Li, X. CoSinGAN: Learning COVID-19 Infection Segmentation from a Single Radiological Image. Diagnostics 2020, 10, 901. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, M.; Brambilla, A.; Dallasta, S.; Colombo, G. High-quality chest CT segmentation to assess the impact of COVID-19 disease. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 1737–1747. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of chest CT and RT-PCR testing for coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, H.J.; Kwee, T.C.; Yakar, D.; Hope, M.D.; Kwee, R.M. Chest CT imaging signature of coronavirus disease 2019 infection: In pursuit of the scientific evidence. Chest 2020, 158, 1885–1895. [Google Scholar] [CrossRef] [PubMed]
- Shi, F.; Wang, J.; Shi, J.; Wu, Z.; Wang, Q.; Tang, Z.; He, K.; Shi, Y.; Shen, D. Review of artificial intelligence techniques in imaging data acquisition, segmentation, and diagnosis for COVID-19. IEEE Rev. Biomed. Eng. 2020, 14, 4–15. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Liu, X.; Shen, J.; Li, Z.; Sang, Y.; Wu, X.; Zha, Y.; Liang, W.; Wang, C.; Wang, K.; et al. Clinically applicable AI system for accurate diagnosis, quantitative measurements, and prognosis of COVID-19 pneumonia using computed tomography. Cell 2020, 181, 1423–1433. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.H.; Gao, S.H.; Mei, J.; Xu, J.; Fan, D.P.; Zhang, R.G.; Cheng, M.M. JCS: An Explainable COVID-19 Diagnosis System by Joint Classification and Segmentation. IEEE Trans. Image Process. 2020, 30, 3113–3126. [Google Scholar] [CrossRef]
- Shan, F.; Gao, Y.; Wang, J.; Shi, W.; Shi, N.; Han, M.; Xue, Z.; Shen, D.; Shi, Y. Lung infection quantification of COVID-19 in CT images with deep learning. arXiv 2020, arXiv:2003.04655. [Google Scholar]
- Qiu, Y.; Liu, Y.; Xu, J. MiniSeg: An Extremely Minimum Network for Efficient COVID-19 Segmentation. Proc. Conf. AAAI Artif. Intell. 2020, 35, 4846–4854. [Google Scholar] [CrossRef]
- Çiçek, Ö.; Abdulkadir, A.; Lienkamp, S.S.; Brox, T.; Ronneberger, O. 3D U-Net: Learning dense volumetric segmentation from sparse annotation. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2016; pp. 424–432. [Google Scholar]
- Zhang, L.; Wang, X.; Yang, D.; Sanford, T.; Harmon, S.; Turkbey, B.; Roth, H.; Myronenko, A.; Xu, D.; Xu, Z. When unseen domain generalization is unnecessary? rethinking data augmentation. arXiv 2019, arXiv:1906.03347. [Google Scholar]
- Jin, D.; Xu, Z.; Tang, Y.; Harrison, A.P.; Mollura, D.J. CT-realistic lung nodule simulation from 3D conditional generative adversarial networks for robust lung segmentation. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2018; pp. 732–740. [Google Scholar]
- Shin, H.-C.; Tenenholtz, N.A.; Rogers, J.K.; Schwarz, C.G.; Senjem, M.L.; Gunter, J.L.; Andriole, K.P.; Michalski, M. Medical image synthesis for data augmentation and anonymization using generative adversarial networks. In International Workshop on Simulation and Synthesis in Medical Imaging; Springer: Cham, Switzerland, 2018; pp. 1–11. [Google Scholar]
- Xu, Z.; Niethammer, M. DeepAtlas: Joint semi-supervised learning of image registration and segmentation. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2019; pp. 420–429. [Google Scholar]
- Fan, D.-P.; Zhou, T.; Ji, G.-P.; Zhou, Y.; Chen, G.; Fu, H.; Shen, J.; Shao, L. Inf-Net: Automatic COVID-19 Lung Infection Segmentation from CT Images. IEEE Trans. Med. Imaging 2020, 39, 2626–2637. [Google Scholar] [CrossRef] [PubMed]
- Shan, S.; Yan, W.; Guo, X.; Chang, E.I.; Fan, Y.; Xu, Y. Unsupervised end-to-end learning for deformable medical image registration. arXiv 2017, arXiv:1711.08608. [Google Scholar]
- de Vos, B.D.; Berendsen, F.F.; Viergever, M.A.; Sokooti, H.; Staring, M.; Išgum, I. A deep learning framework for unsupervised affine and deformable image registration. Med. Image Anal. 2019, 52, 128–143. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Liu, X.; Li, C.; Xu, Z.; Ruan, J.; Zhu, H.; Meng, T.; Li, K.; Huang, N.; Zhang, S. A noise-robust framework for automatic segmentation of COVID-19 pneumonia lesions from CT images. IEEE Trans. Med. Imaging 2020, 39, 2653–2663. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, Y.; Guo, L.; Zhou, X.; Zhu, Y.; He, Q.; Han, H.; Feng, Q. Machine learning techniques for CT imaging diagnosis of novel coronavirus pneumonia: A review. Neural Comput. Applications. 2022. [Google Scholar] [CrossRef] [PubMed]
- Santosh, K.; Antani, S. Automated chest X-ray screening: Can lung region symmetry help detect pulmonary abnormalities? IEEE Trans. Med. Imaging 2017, 37, 1168–1177. [Google Scholar] [CrossRef]
- Pratondo, A.; Chui, C.K.; Ong, S.H. Integrating machine learning with region-based active contour models in medical image segmentation. J. Vis. Commun. Image Represent. 2017, 43, 1–9. [Google Scholar] [CrossRef]
- Ahmad, W.; Zaki, W.; Fauzi, M. Lung segmentation on standard and mobile chest radiographs using oriented Gaussian derivatives filter. Biomed. Eng. Online 2015, 14, 20. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, T.; Prince, S.J.; Alexander, D.C. Interactive lesion segmentation with shape priors from offline and online learning. IEEE Trans. Med. Imaging 2012, 31, 1698–1712. [Google Scholar] [CrossRef]
- Xu, W.; He, G.; Pan, C.; Shen, D.; Zhang, N.; Jiang, P.; Liu, F.; Chen, J. A Forced Cough Sound based Pulmonary Function Assessment by Using Machine Learning. Front. Public Health. 2022, 10, 1015876. [Google Scholar] [CrossRef]
- Shaukat, F.; Raja, G.; Gooya, A.; Frangi, A. Fully automatic detection of lung nodules in CT images using a hybrid feature set. Med. Phys. 2017, 44, 3615–3629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza, J.C.; Diniz, J.O.B.; Ferreira, J.L.; da Silva, G.L.F.; Silva, A.C.; de Paiva, A.C. An automatic method for lung segmentation and reconstruction in chest X-ray using deep neural networks. Comput. Methods Programs Biomed. 2019, 177, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Park, B.; Park, H.; Lee, S.M.; Seo, J.B.; Kim, N. Lung Segmentation on HRCT and Volumetric CT for Diffuse Interstitial Lung Disease Using Deep Convolutional Neural Networks. J. Digit. Imaging 2019, 32, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Medical Image Computing and Computer-Assisted Intervention—MICCAI 2015; Navab, N., Hornegger, J., Wells, W., Frangi, A., Eds.; MICCAI 2015, Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2015; Volume 9351. [Google Scholar] [CrossRef] [Green Version]
- Jun, M.; Cheng, G.; Yixin, W.; Xingle, A.; Jiantao, G.; Ziqi, Y.; Jian, H. COVID-19 CT Lung and Infection Segmentation Dataset (Verson 1.0) [Data set]; Zenodo: Geneva, Switzerland, 2020. [Google Scholar]
- Oktay, O.; Schlemper, J.; Le Folgoc, L.; Lee, M.; Heinrich, M.; Misawa, K.; Rueckert, D. Attention U-Net: Learning Where to Look for the Pancreas. arXiv 2018, arXiv:1804.03999. [Google Scholar]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef]
- Firdaus-Nawi, M.; Noraini, O.; Sabri, M.Y.; Siti-Zahrah, A.; Zamri-Saad, M.; Latifah, H. DeepLabv3+ _encoder-decoder with Atrous separable convolution for semantic image segmentation. Pertanika J. Trop. Agric. Sci. 2011, 34, 137–143. [Google Scholar]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metric | IoU | DSC | SEN | SPE |
|---|---|---|---|---|
| Value | 0.94 | 0.96 | 0.97 | 1.00 |
| Network | Labels | IoU (%) | DSC (%) | SEN (%) | SPE (%) | |
|---|---|---|---|---|---|---|
| Original | Refined | |||||
| UNet [28] | √ | 68.02 | 78.36 | 82.31 | 99.74 | |
| √ | 73.54 | 83.47 | 87.75 | 99.83 | ||
| Attention-UNet [30] | √ | 71.89 | 82.13 | 85.51 | 99.78 | |
| √ | 71.82 | 82.35 | 82.37 | 99.87 | ||
| SegNet [31] | √ | 68.98 | 79.57 | 83.38 | 99.74 | |
| √ | 68.49 | 79.54 | 78.85 | 99.87 | ||
| DeepLabV3+ [32] | √ | 72.43 | 82.94 | 85.08 | 99.79 | |
| √ | 68.71 | 80.48 | 79.89 | 99.84 | ||
| Network | g | CPA (%) | IoU (%) | DSC (%) | SEN (%) | SPE (%) | MIoU (%) | MPA (%) |
|---|---|---|---|---|---|---|---|---|
| UNet | 1 | 77.30 | 56.52 | 70.71 | 77.30 | 99.87 | 61.04 | 75.73 |
| 2 | 81.31 | 65.47 | 77.20 | 81.31 | 99.92 | |||
| 3 | 75.33 | 61.13 | 72.93 | 75.33 | 99.95 | |||
| Attention-UNet | 1 | 70.30 | 53.24 | 67.80 | 70.30 | 99.88 | 58.27 | 71.56 |
| 2 | 73.95 | 62.82 | 75.17 | 73.95 | 99.94 | |||
| 3 | 70.41 | 58.75 | 70.81 | 70.41 | 99.96 | |||
| SegNet | 1 | 55.58 | 41.31 | 56.20 | 55.58 | 99.84 | 51.96 | 67.74 |
| 2 | 71.21 | 52.55 | 66.77 | 72.22 | 99.86 | |||
| 3 | 66.59 | 49.40 | 63.18 | 66.59 | 99.92 | |||
| DeepLabV3+ | 1 | 55.21 | 40.62 | 56.20 | 55.21 | 99.85 | 41.69 | 57.05 |
| 2 | 61.62 | 44.43 | 60.37 | 61.62 | 99.86 | |||
| 3 | 54.34 | 40.03 | 55.11 | 54.34 | 99.91 |
| Severity | Precision (%) | Precision (%) (With Operation of Oversampling) |
|---|---|---|
| Normal | 1 | 1 |
| Mild | 0 | 1 |
| Moderate | 99.37% | 99.38% |
| Severe | 62.69% | 82.50% |
| Critical | 79.49% | 89.74% |
| Total | 96.49 | 98.82 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, T.; Liu, H.; Zhang, Z.; Li, C.; Zhou, Y. Research on the Application of Artificial Intelligence in Public Health Management: Leveraging Artificial Intelligence to Improve COVID-19 CT Image Diagnosis. Int. J. Environ. Res. Public Health 2023, 20, 1158. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021158
He T, Liu H, Zhang Z, Li C, Zhou Y. Research on the Application of Artificial Intelligence in Public Health Management: Leveraging Artificial Intelligence to Improve COVID-19 CT Image Diagnosis. International Journal of Environmental Research and Public Health. 2023; 20(2):1158. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021158
Chicago/Turabian StyleHe, Tiancheng, Hong Liu, Zhihao Zhang, Chao Li, and Youmei Zhou. 2023. "Research on the Application of Artificial Intelligence in Public Health Management: Leveraging Artificial Intelligence to Improve COVID-19 CT Image Diagnosis" International Journal of Environmental Research and Public Health 20, no. 2: 1158. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021158