
Effect of Familial Longevity on Frailty and Sarcopenia: A Case–Control Study
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
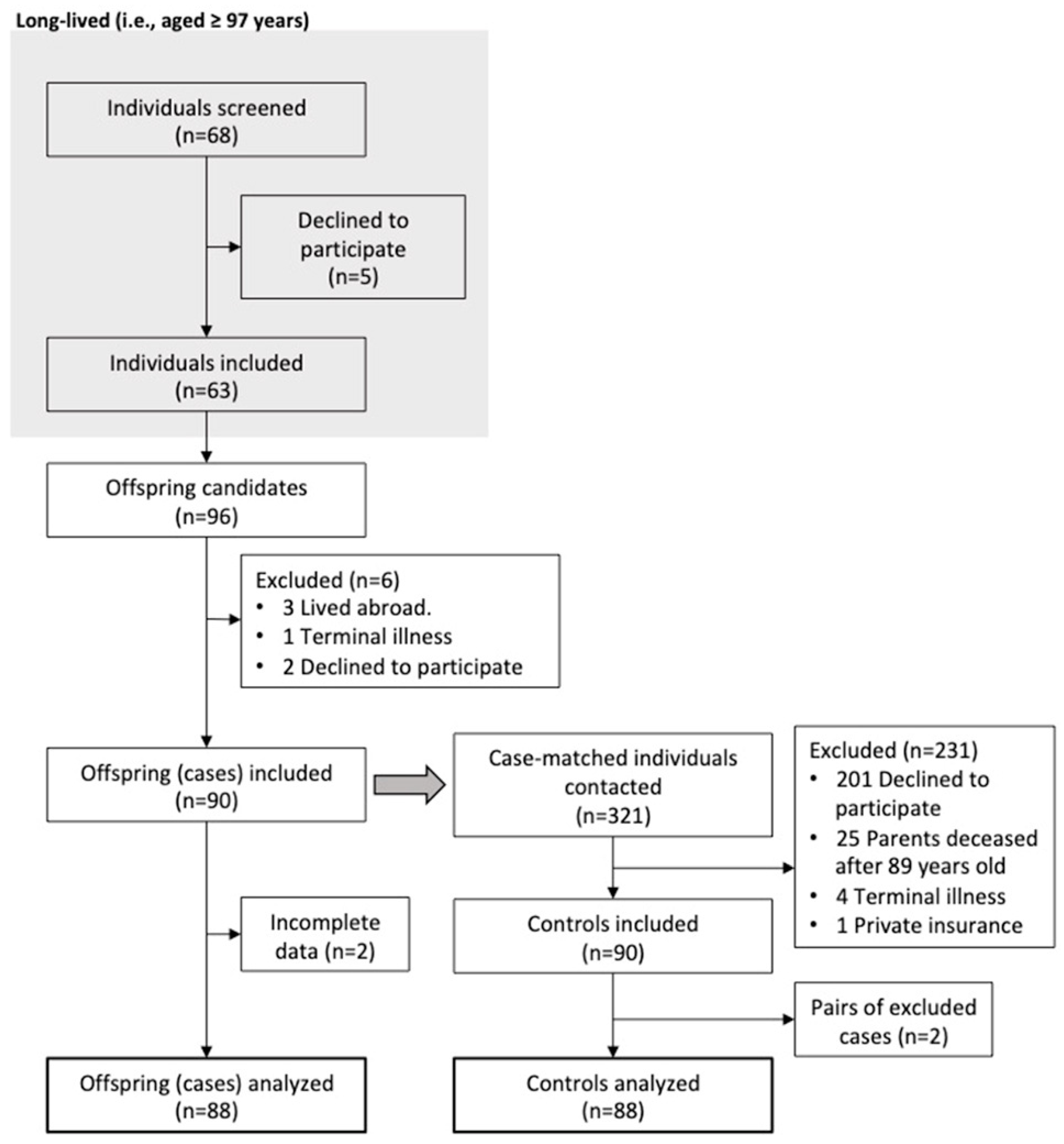
2.1. Study Design and Participants
2.2. Procedures
2.3. Primary Outcomes
2.4. Secondary Variables
2.5. Statistical Analysis
3. Results
3.1. Participant Disposition and Characteristics
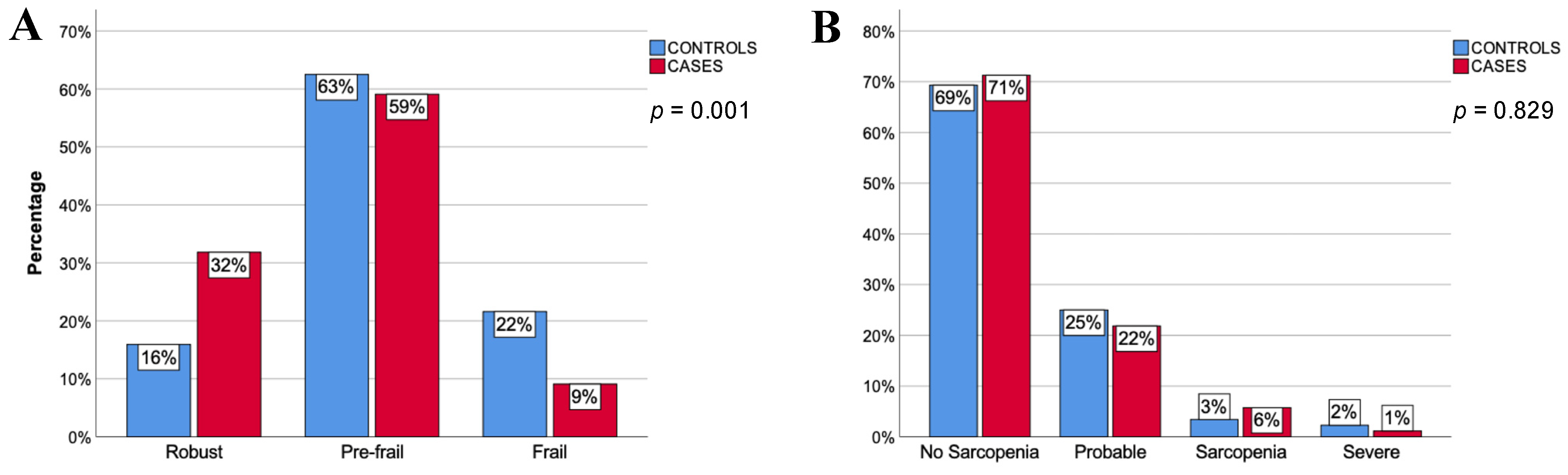
3.2. Frailty and Sarcopenia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Instituto Nacional de Estadística. Población Residente Por Fecha, Sexo y Grupo de Edad. Available online: https://www.ine.es/jaxiT3/Tabla.htm?t=9689 (accessed on 24 September 2022).
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.W.; et al. Forecasting Life Expectancy, Years of Life Lost, and All-Cause and Cause-Specific Mortality for 250 Causes of Death: Reference and Alternative Scenarios for 2016–40 for 195 Countries and Territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeiren, S.; Vella-Azzopardi, R.; Beckwée, D.; Habbig, A.K.; Scafoglieri, A.; Jansen, B.; Bautmans, I.; Bautmans, I.; Vert, D.; Beyer, I.; et al. Frailty and the Prediction of Negative Health Outcomes: A Meta-Analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1163.e1–1163.e17. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Hao, Q.; Ge, M.; Dong, B. Association of Sarcopenia and Fractures in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis of Cohort Studies. Osteoporos. Int. 2018, 29, 1253–1262. [Google Scholar] [CrossRef]
- Shimada, H.; Tsutsumimoto, K.; Doi, T.; Lee, S.; Bae, S.; Nakakubo, S.; Makino, K.; Arai, H. Effect of Sarcopenia Status on Disability Incidence Among Japanese Older Adults. J. Am. Med. Dir. Assoc. 2020, 22, 846–852. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Bustos, A.; Rodríguez-Sánchez, B.; Carnicero-Carreño, J.A.; Sepúlveda-Loyola, W.; Garcia-Garcia, F.J.; Rodríguez-Mañas, L. Healthcare Cost Expenditures Associated to Frailty and Sarcopenia. BMC Geriatr. 2022, 22, 747. [Google Scholar] [CrossRef]
- Landi, F.; Cruz-Jentoft, A.J.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia and Mortality Risk in Frail Older Persons Aged 80 Years and Older: Results from IlSIRENTE Study. Age Ageing 2013, 42, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Santos-Eggimann, B.; Cuénoud, P.; Spagnoli, J.; Junod, J. Prevalence of Frailty in Middle-Aged and Older Community-Dwelling Europeans Living in 10 Countries. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2009, 64, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.; et al. Prevalence of and Interventions for Sarcopenia in Ageing Adults: A Systematic Review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 48–759. [Google Scholar] [CrossRef]
- Wilson, D.; Jackson, T.; Sapey, E.; Lord, J.M. Frailty and Sarcopenia: The Potential Role of an Aged Immune System. Ageing Res. Rev. 2017, 36, 1–10. [Google Scholar] [CrossRef]
- Liu, Z.Y.; Wei, Y.Z.; Wei, L.Q.; Jiang, X.Y.; Wang, X.F.; Shi, Y.; Hai, H. Frailty Transitions and Types of Death in Chinese Older Adults: A Population-Based Cohort Study. Clin. Interv. Aging 2018, 13, 947–956. [Google Scholar] [CrossRef]
- Trevisan, C.; Vetrano, D.L.; Calvani, R.; Picca, A.; Welmer, A.K. Twelve-Year Sarcopenia Trajectories in Older Adults: Results from a Population-Based Study. J. Cachexia. Sarcopenia Muscle 2022, 13, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Bustos, A.; Carnicero-Carreño, J.A.; Davies, B.; Garcia-Garcia, F.J.; Rodríguez-Artalejo, F.; Rodríguez-Mañas, L.; Alonso-Bouzón, C. Role of Sarcopenia in the Frailty Transitions in Older Adults: A Population-Based Cohort Study. J. Cachexia. Sarcopenia Muscle 2022, 13, 2352–2360. [Google Scholar] [CrossRef] [PubMed]
- Dato, S.; Montesanto, A.; Lagani, V.; Jeune, B.; Christensen, K.; Passarino, G. Frailty Phenotypes in the Elderly Based on Cluster Analysis: A Longitudinal Study of Two Danish Cohorts. Evidence for a Genetic Influence on Frailty. Age 2012, 34, 571–582. [Google Scholar] [CrossRef] [Green Version]
- Cournil, A.; Jeune, B.; Skytthe, A.; Gampe, J.; Passarino, G.; Robine, J.M. Handgrip Strength: Indications of Paternal Inheritance in Three European Regions. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65A, 1101–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garatachea, N.; Lucia, A. Genes, Physical Fitness and Ageing. Ageing Res. Rev. 2013, 12, 90–102. [Google Scholar] [CrossRef]
- Andersen, S.L.; Sebastiani, P.; Dworkis, D.A.; Feldman, L.; Perls, T.T. Health Span Approximates Life Span among Many Supercentenarians: Compression of Morbidity at the Approximate Limit of Life Span. J. Gerontol. A. Biol. Sci. Med. Sci. 2012, 67, 395–405. [Google Scholar] [CrossRef]
- Engberg, H.; Oksuzyan, A.; Jeune, B.; Vaupel, J.W.; Christensen, K. Centenarians—A Useful Model for Healthy Aging? A 29-Year Follow-up of Hospitalizations among 40000 Danes Born in 1905. Aging Cell 2009, 8, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Gentilini, D.; Mari, D.; Castaldi, D.; Remondini, D.; Ogliari, G.; Ostan, R.; Bucci, L.; Sirchia, S.M.; Tabano, S.; Cavagnini, F.; et al. Role of Epigenetics in Human Aging and Longevity: Genome-Wide DNA Methylation Profile in Centenarians and Centenarians’ Offspring. Age 2013, 35, 1961–1973. [Google Scholar] [CrossRef] [Green Version]
- Serna, E.; Gambini, J.; Borras, C.; Abdelaziz, K.M.; Mohammed, K.; Belenguer, A.; Sanchis, P.; Avellana, J.A.; Rodriguez-Mañas, L.; Viña, J. Centenarians, but Not Octogenarians, up-Regulate the Expression of MicroRNAs. Sci. Rep. 2012, 2, 961. [Google Scholar] [CrossRef] [Green Version]
- Terry, D.F.; Wilcox, M.; McCormick, M.A.; Lawler, E.; Perls, T.T. Cardiovascular Advantages Among the Offspring of Centenarians. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2003, 58, M425–M431. [Google Scholar] [CrossRef]
- Atzmon, G.; Schechter, C.; Greiner, W.; Davidson, D.; Rennert, G.; Barzilai, N. Clinical Phenotype of Families with Longevity. J. Am. Geriatr. Soc. 2004, 52, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Terry, D.F.; Wilcox, M.A.; McCormick, M.A.; Pennington, J.M.Y.; Schoenhofen, E.A.; Andersen, S.L.; Perls, T.T. Lower All-Cause, Cardiovascular, and Cancer Mortality in Centenarians’ Offspring. J. Am. Geriatr. Soc. 2004, 52, 2074–2076. [Google Scholar] [CrossRef] [PubMed]
- Schoenmaker, M.; de Craen, A.J.M.; de Meijer, P.H.E.M.; Beekman, M.; Blauw, G.J.; Slagboom, P.E.; Westendorp, R.G.J. Evidence of Genetic Enrichment for Exceptional Survival Using a Family Approach: The Leiden Longevity Study. Eur. J. Hum. Genet. 2006, 14, 79–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, E.R.; Nolan, V.G.; Andersen, S.L.; Perls, T.T.; Terry, D.F. Centenarian Offspring: Start Healthier and Stay Healthier. J. Am. Geriatr. Soc. 2008, 56, 2089–2092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westendorp, R.G.J.; Van Heemst, D.; Rozing, M.P.; Frölich, M.; Mooijaart, S.P.; Blauw, G.J.; Beekman, M.; Heijmans, B.T.; De Craen, A.J.M.; Slagboom, P.E. Nonagenarian Siblings and Their Offspring Display Lower Risk of Mortality and Morbidity than Sporadic Nonagenarians: The Leiden Longevity Study. J. Am. Geriatr. Soc. 2009, 57, 1634–1637. [Google Scholar] [CrossRef]
- Stijntjes, M.; de Craen, A.J.M.; van Heemst, D.; Meskers, C.G.M.; van Buchem, M.A.; Westendorp, R.G.J.; Slagboom, P.E.; Maier, A.B. Familial Longevity Is Marked by Better Cognitive Performance at Middle Age: The Leiden Longevity Study. PLoS ONE 2013, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Bucci, L.; Ostan, R.; Cevenini, E.; Pini, E.; Scurti, M.; Vitale, G.; Caruso, C.; Sansoni, P.; Fanelli, F.; Pasquali, R.; et al. Centenarians’ Offspring as a Model of Healthy Aging: A Reappraisal of the Data on Italian Subjects and a Comprehensive Overview. Aging 2016, 8, 510–519. [Google Scholar] [CrossRef] [Green Version]
- Barral, S.; Singh, J.; Fagan, E.; Cosentino, S.; Andersen-Toomey, S.L.; Wojczynski, M.K.; Feitosa, M.; Kammerer, C.M.; Schupf, N. Age-Related Biomarkers in LLFS Families with Exceptional Cognitive Abilities. J. Gerontol.—Ser. A Biol. Sci. Med. Sci. 2017, 72, 1683–1688. [Google Scholar] [CrossRef] [Green Version]
- Shadyab, A.H.; Manson, J.E.; Wenjun, L.I.; Gass, M.; Brunner, R.L.; Naughton, M.J.; Cannell, B.; Howard, B.V.; Lacroix, A.Z. Parental Longevity Predicts Healthy Ageing among Women. Age Ageing 2018, 47, 853–860. [Google Scholar] [CrossRef] [Green Version]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4, 1628–1654. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. Biological Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Mañas, L.; Bayer, A.J.; Kelly, M.; Zeyfang, A.; Izquierdo, M.; Laosa, O.; Hardman, T.C.; Sinclair, A.J. An Evaluation of the Effectiveness of a Multi-Modal Intervention in Frail and Pre-Frail Older People with Type 2 Diabetes—the MID-Frail Study: Study Protocol for a Randomised Controlled Trial. Trials 2014, 15, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European Consensus on Definition and Diagnosis. Age Ageing 2018, 39, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Tudor, G.; Koch, G.G. Review of Nonparametric Methods for the Analysis of Crossover Studies. Stat. Methods Med. Res. 1994, 3, 345–381. [Google Scholar] [CrossRef] [PubMed]
- Scheff, S.W. Chapter 8—Nonparametric Statistics. In Fundamental Statistical Principles for the Neurobiologist; Scheff, S.W., Ed.; Academic Press: Cambridge, MA, USA, 2016; pp. 157–182. ISBN 978-0-12-804753-8. [Google Scholar]
- Maldonado, G.; Greenland, S. Simulation Study of Confounder-Selection Strategies. Am. J. Epidemiol. 1993, 138, 923–936. [Google Scholar] [CrossRef] [Green Version]
- Amblàs-Novellas, J.; Espaulella-Panicot, J.; Inzitari, M.; Rexach, L.; Fontecha, B.; Romero-Ortuno, R. The Challenge of Clinical Complexity in the 21st Century: Could Frailty Indexes Be the Answer? Rev. Esp. Geriatr. Gerontol. 2017, 52, 159–166. [Google Scholar] [CrossRef]
- Kulminski, A.M.; Ukraintseva, S.V.; Kulminskaya, I.V.; Arbeev, K.G.; Land, K.; Yashin, A.I. Cumulative Deficits Better Characterize Susceptibility to Death in Elderly People than Phenotypic Frailty: Lessons from the Cardiovascular Health Study. J. Am. Geriatr. Soc. 2008, 56, 898–903. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Welsh, D.A.; Cherry, K.E.; Myers, L.; Jazwinski, S.M. Association of Healthy Aging with Parental Longevity. Age 2013, 35, 1975–1982. [Google Scholar] [CrossRef] [Green Version]
- Arosio, B.; Ferri, E.; Casati, M.; Mari, D.; Vitale, G.; Cesari, M. The Frailty Index in Centenarians and Their Offspring. Aging Clin. Exp. Res. 2019, 31, 1685–1688. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.L.; Singh, J.; Minster, R.L.; Walston, J.D.; Matteini, A.M.; Christensen, K.; Mayeux, R.; Borecki, I.B.; Perls, T.; Newman, A.B. Association Between Mortality and Heritability of the Scale of Aging Vigor in Epidemiology. J. Am. Geriatr. Soc. 2016, 64, 1679–1683. [Google Scholar] [CrossRef]
- Ayers, E.; Barzilai, N.; Crandall, J.P.; Milman, S.; Verghese, J. Association of Exceptional Parental Longevity and Physical Function in Aging. Age 2014, 36, 9677. [Google Scholar] [CrossRef] [Green Version]
- Soysal, P.; Stubbs, B.; Lucato, P.; Luchini, C.; Solmi, M.; Peluso, R.; Sergi, G.; Isik, A.T.; Manzato, E.; Maggi, S.; et al. Inflammation and Frailty in the Elderly: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2016, 31, 1–8. [Google Scholar] [CrossRef]
- Franceschi, C.; Garagnani, P.; Parini, P.; Giuliani, C.; Santoro, A. Inflammaging: A New Immune–Metabolic Viewpoint for Age-Related Diseases. Nat. Rev. Endocrinol. 2018, 14, 576–590. [Google Scholar] [CrossRef]
- Mazzotti, D.R.; Guindalini, C.; Moraes, W.A.D.S.; Andersen, M.L.; Cendoroglo, M.S.; Ramos, L.R.; Tufik, S. Human Longevity Is Associated with Regular Sleep Patterns, Maintenance of Slow Wave Sleep, and Favorable Lipid Profile. Front. Aging Neurosci. 2014, 6, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.H.; Kong, D.; Lee, Y.T.H.; Lin, C.H.; Liu, C.T.; Chang, Y.C. Functional Disabilities and Changes in Sleep Quality and Duration among Older Adults: Results from a Longitudinal Study in China, 2005–2014. Eur. Geriatr. Med. 2022, 13, 967–975. [Google Scholar] [CrossRef]
- Kocevska, D.; Barclay, N.L.; Bramer, W.M.; Gehrman, P.R.; Van Someren, E.J.W. Heritability of Sleep Duration and Quality: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2021, 59, 101448. [Google Scholar] [CrossRef]
- Madrid-Valero, J.J.; Rubio-Aparicio, M.; Gregory, A.M.; Sánchez-Meca, J.; Ordoñana, J.R. The Heritability of Insomnia: Systematic Review and Meta-Analysis of Twin Studies. Sleep Med. Rev. 2021, 58, 101437. [Google Scholar] [CrossRef]
- Lovato, N.; Lack, L. Insomnia and Mortality: A Meta-Analysis. Sleep Med. Rev. 2019, 43, 71–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, L.; Gao, T.; Barzilai, N.; Milman, S. Association between Sleep Patterns and Health in Families with Exceptional Longevity. Front. Med. 2017, 4, 214. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Blackwell, T.L.; Redline, S.; Ancoli-Israel, S.; Paudel, M.L.; Cawthon, P.M.; Dam, T.T.L.; Barrett-Connor, E.; Leung, P.C.; Stone, K.L. Sleep Disturbances and Frailty Status in Older Community-Dwelling Men. J. Am. Geriatr. Soc. 2009, 57, 2085–2093. [Google Scholar] [CrossRef] [PubMed]
- Tian, Q.; Pilling, L.C.; Atkins, J.L.; Melzer, D.; Ferrucci, L. The Relationship of Parental Longevity with the Aging Brain—Results from UK Biobank. GeroScience 2020, 42, 1377–1385. [Google Scholar] [CrossRef]
- Collino, S.; Montoliu, I.; Martin, F.-P.J.; Scherer, M.; Mari, D.; Salvioli, S.; Bucci, L.; Ostan, R.; Monti, D.; Biagi, E.; et al. Metabolic Signatures of Extreme Longevity in Northern Italian Centenarians Reveal a Complex Remodeling of Lipids, Amino Acids, and Gut Microbiota Metabolism. PLoS ONE 2013, 8, e56564. [Google Scholar] [CrossRef]
- Pradas, I.; Jové, M.; Huynh, K.; Puig, J.; Ingles, M.; Borras, C.; Viña, J.; Meikle, P.; Pamplona, R. Exceptional Human Longevity Is Associated with a Specific Plasma Phenotype of Ether Lipids. Redox Biol. 2019, 21, 101127. [Google Scholar] [CrossRef] [PubMed]
- Picca, A.; Coelho-Junior, H.J.; Cesari, M.; Marini, F.; Miccheli, A.; Gervasoni, J.; Bossola, M.; Landi, F.; Bernabei, R.; Marzetti, E.; et al. The Metabolomics Side of Frailty: Toward Personalized Medicine for the Aged. Exp. Gerontol. 2019, 126, 110692. [Google Scholar] [CrossRef]
- Li, G.H.; Han, F.; Xiao, F.H.; Gu, K.S.Y.; Shen, Q.; Xu, W.; Li, W.X.; Wang, Y.L.; Liang, B.; Huang, J.F.; et al. System-Level Metabolic Modeling Facilitates Unveiling Metabolic Signature in Exceptional Longevity. Aging Cell 2022, 21, e13595. [Google Scholar] [CrossRef] [PubMed]
- Barzilai, N.; Atzmon, G.; Schechter, C.; Schaefer, E.J.; Cupples, A.L.; Lipton, R.; Cheng, S.; Shuldiner, A.R. Unique Lipoprotein Phenotype and Genotype Associated with Exceptional Longevity. J. Am. Med. Assoc. 2003, 290, 2030–2040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gueresi, P.; Miglio, R.; Monti, D.; Mari, D.; Sansoni, P.; Caruso, C.; Bonafede, E.; Bucci, L.; Cevenini, E.; Ostan, R.; et al. Does the Longevity of One or Both Parents Influence the Health Status of Their Offspring? Exp. Gerontol. 2013, 48, 395–400. [Google Scholar] [CrossRef]
- Liou, L.; Kaptoge, S. Association of Small, Dense LDL-Cholesterol Concentration and Lipoprotein Particle Characteristics with Coronary Heart Disease: A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0241993. [Google Scholar] [CrossRef] [PubMed]
- Hirano, T.; Ito, Y.; Yoshino, G. Measurement of Small Dense Low-Density Lipoprotein Particles. J. Atheroscler. Thromb. 2005, 12, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Andersen, S.L.; Sweigart, B.; Sebastiani, P.; Drury, J.; Sidlowski, S.; Perls, T.T. Reduced Prevalence and Incidence of Cognitive Impairment among Centenarian Offspring. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 108–113. [Google Scholar] [CrossRef]
- Gostynski, M.; Gutzwiller, F.; Kuulasmaa, K.; Döring, A.; Ferrario, M.; Grafnetter, D.; Pajak, A. Analysis of the Relationship between Total Cholesterol, Age, Body Mass Index among Males and Females in the WHO MONICA Project. Int. J. Obes. 2004, 28, 1082–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayers, E.; Barzilai, N.; Crandall, J.P.; Milman, S.; Verghese, J. Association of Family History of Exceptional Longevity with Decline in Physical Function in Aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 1649–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, J.Y.; Kim, Y.J.; Shin, W.Y.; Kim, N.Y.; Cho, S.H.; Kim, J.H. Heritability of Muscle Mass in Korean Parent–Offspring Pairs in the Fifth Korean National Health and Nutrition Examination Survey (KNHANES V). Maturitas 2018, 114, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Masanés, F.; Rojano i Luque, X.; Salvà, A.; Serra-Rexach, J.A.; Artaza, I.; Formiga, F.; Cuesta, F.; López Soto, A.; Ruiz, D.; Cruz-Jentoft, A.J. Cut-off Points for Muscle Mass—Not Grip Strength or Gait Speed—Determine Variations in Sarcopenia Prevalence. J. Nutr. Health Aging 2017, 21, 825–829. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, I.; Tanimoto, Y.; Takahashi, Y.; Kusabiraki, T.; Tamaki, J. Correlation between Muscle Strength and Muscle Mass, and Their Association with Walking Speed, in Community-Dwelling Elderly Japanese Individuals. PLoS ONE 2014, 9, e111810. [Google Scholar] [CrossRef]
- Inglés, M.; Gambini, J.; Carnicero, J.A.; García-García, F.J.; Rodríguez-Mañas, L.; Olaso-González, G.; Dromant, M.; Borrás, C.; Viña, J. Oxidative Stress Is Related to Frailty, Not to Age or Sex, in a Geriatric Population: Lipid and Protein Oxidation as Biomarkers of Frailty. J. Am. Geriatr. Soc. 2014, 62, 1324–1328. [Google Scholar] [CrossRef]
- El Assar, M.; Angulo, J.; Carnicero, J.A.; Walter, S.; García-García, F.J.; López-Hernández, E.; Sánchez-Puelles, J.M.; Rodríguez-Mañas, L. Frailty Is Associated With Lower Expression of Genes Involved in Cellular Response to Stress: Results From the Toledo Study for Healthy Aging. J. Am. Med. Dir. Assoc. 2017, 18, 734.e1–734.e7. [Google Scholar] [CrossRef]
- Rakib, A.; Kiran, S.; Mandal, M.; Singh, U.P. MicroRNAs: A Crossroad That Connects Obesity to Immunity and Aging. Immun. Ageing 2022, 19, 64. [Google Scholar] [CrossRef]
- Terry, D.F.; Wilcox, M.A.; McCormick, M.A.; Perls, T.T. Cardiovascular Disease Delay in Centenarian Offspring. J. Gerontol. A. Biol. Sci. Med. Sci. 2004, 59, 385–389. [Google Scholar] [CrossRef] [Green Version]
- Belenguer-Varea, Á.; Tarazona-Santabalbina, F.J.; Avellana-Zaragoza, J.A.; Martínez-Reig, M.; Mas-Bargues, C.; Inglés, M. Oxidative Stress and Exceptional Human Longevity: Systematic Review. Free Radic. Biol. Med. 2020, 149, 51–63. [Google Scholar] [CrossRef]
- Borras, C.; Abdelaziz, K.M.; Gambini, J.; Serna, E.; Inglés, M.; de la Fuente, M.; Garcia, I.; Matheu, A.; Sanchís, P.; Belenguer, A.; et al. Human Exceptional Longevity: Transcriptome from Centenarians Is Distinct from Septuagenarians and Reveals a Role of Bcl-XL in Successful Aging. Aging 2016, 8, 3185–3208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inglés, M.; Belenguer-Varea, A.; Serna, E.; Mas-Bargues, C.; Tarazona-Santabalbina, F.J.; Borrás, C.; Vina, J. Functional Transcriptomic Analysis of Centenarians’ Offspring Reveals a Specific Genetic Footprint That May Explain That They Are Less Frail than Age-Matched Non-Centenarians’ Offspring. J. Gerontol. Ser. A 2022, 10, 1931–1938. [Google Scholar] [CrossRef]
- Kupper, L.L.; Karon, J.M.; Kleinbaum, D.G.; Morgenstern, H.; Lewis, D.K. Matching in Epidemiologic Studies: Validity and Efficiency Considerations. Biometrics 1981, 37, 271. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.J.; Zoccali, C.; MacLeod, A.; Dekker, F.W. Confounding: What It Is and How to Deal with It. Kidney Int. 2008, 73, 256–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for Clinical Practice and Public Health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, J.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of Physical Activities: An Update of Activity Codes and MET Intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Zhang, J.; Shen, S.; Hong, X.; Zeng, X.; Yang, Y.; Liu, Z.; Chen, L.; Chen, X. Association between Body Composition and Frailty in Elder Inpatients. Clin. Interv. Aging 2020, 15, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Airoldi, C.; Ferrante, D.; Mirabelli, D.; Azzolina, D.; Magnani, C. Evaluation of Nonresponse Bias in a Case–Control Study of Pleural Mesothelioma. Int. J. Environ. Res. Public Health 2020, 17, 6146. [Google Scholar] [CrossRef]
- Mazor, K.M.; Clauser, B.E.; Field, T.; Yood, R.A.; Gurwitz, J.H. A Demonstration of the Impact of Response Bias on the Results of Patient Satisfaction Surveys. Health Serv. Res. 2002, 37, 1403–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gubbi, S.; Schwartz, E.; Crandall, J.; Verghese, J.; Holtzer, R.; Atzmon, G.; Braunstein, R.; Barzilai, N.; Milman, S. Effect of Exceptional Parental Longevity and Lifestyle Factors on Prevalence of Cardiovascular Disease in Offspring. Am. J. Cardiol. 2017, 120, 2170–2175. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall n = 176 | Controls n = 88 | Cases n = 88 | p-Value a | |
|---|---|---|---|---|
| Age, years, median (IQR) | 70 (7) | 69 (7) | 70 (6) | 0.69 |
| Female, n (%) | 106 (60) | 53 (60) | 53 (60) | 1 |
| Weight, kg, mean ± SD | 74.1 ± 14.4 | 76.9 ± 13.6 | 71.2 ± 14.6 | 0.008 * |
| BMI, kg/m2, median (IQR) | 28.1 (5.6) | 29.2 (6.1) | 27.6 (4.5) | 0.007 * |
| Underweight, n (%) | 5 (2.9) | 1 (1.1) | 4 (4.6) | 0.004 * |
| Normal weight, n (%) | 30 (17.1) | 12 (13.6) | 18 (20.7) | |
| Overweight, n (%) | 79 (45.1) | 35 (39.8) | 44 (50.6) | |
| Obese, n (%) | 61 (34.9) | 40 (45.5) | 21 (24.1) | |
| Current smoker, n (%) | 23 (13.1) | 12 (13.6) | 11 (12.5) | 0.424 |
| Alcohol use, n (%) | 46 (26.6) | 26 (29.9) | 20 (23.9) | 0.472 |
| Mild physical activity b, n (%) | 96 (56.1) | 52 (59.1) | 44 (53%) | 0.417 |
| Regular exercise b, n (%) | 123 (69.9) | 64 (72.7) | 59 (67) | 0.372 |
| Nutritional risk c, n (%) | 44 (25) | 23 (26.1) | 21 (23.8) | 0.819 |
| Sleeping hours | ||||
| Hours per day, median (IQR) | 7 (2) | 7 (2) | 7.5 (1) | 0.640 |
| Insomnia, n (%) | 59 (34.9) | 37 (44.6) | 22 (25.6) | 0.030 * |
| Charlson, median (IQR) | 3 (2) | 3 (2) | 3(2) | 0.350 |
| Lawton, median (IQR) | 8 (0) | 8 (0) | 8 (0) | 0.719 |
| Barthel, median (IQR) | 100 (0) | 100 (0) | 100 (0) | 0.305 |
| Rankin ≤1, n (%) | 170 (97.7) | 84 (96.6) | 86 (98.8) | 0.613 |
| FAC ≥4, n (%) | 133 (95.7) | 69 (94.5) | 64 (97) | 0.461 |
| QL Spitzer, median (IQR) | 10 (1) | 10 (0) | 10 (1) | 0.839 |
| Falls ≥1/12 months, n (%) | 34 (21.1) | 18 (22.2) | 16 (19.8) | 0.148 |
| Pain d, n (%) | 61 (34.7) | 38 (43.2) | 23 (26.1) | 0.029 * |
| Goldberg scale | ||||
| Anxiety, n (%) | 33 (18.8) | 21 (23.9) | 12 (13.6) | 0.137 |
| Depression, n (%) | 38 (21.6) | 18 (20.5) | 20 (22.7) | 0.850 |
| MMSE-Lobo, median (IQR) | 32 (4) | 33 (3) | 32 (5) | 0.592 |
| Polypharmacy e, n (%) | 67 (38.1) | 43 (48.9) | 24 (27.3) | 0.003 * |
| Nº of drugs, median (IQR) | 3 (3) | 3 (5) | 2 (3) | 0.001 * |
| OARS good or excellent, n (%) | 172 (98.3) | 85 (96.6) | 88 (100) | 0.554 |
| Lives alone, n (%) | 8 (4.5) | 5 (5.7) | 3 (3.4) | 0.727 |
| Education, n (%) | 0.034 * | |||
| No primary | 24 (13.8) | 16 (18.2) | 8 (9.3) | |
| Primary | 108 (62.1) | 52 (59.1) | 56 (65.1) | |
| Secondary | 28 (16.1) | 17 (19.3) | 11 (12.8) | |
| University | 14 (8) | 3 (3.4) | 11 (12.8) | |
| Healthcare utilization, medical visits/year, median (IQR) | ||||
| Primary care | 2 (3) | 2 (3) | 2 (2) | 0.644 |
| Specialized care | 1 (2) | 1 (2) | 0 (2) | 0.518 |
| Overall n = 176 | Controls n = 88 | Cases n = 88 | p-Value a | |
|---|---|---|---|---|
| Glucose, mg/dL, median (IQR) | 95 (25) | 96 (27) | 93 (21) | 0.113 |
| <100, n (%) | 108 (61.4) | 49 (55.7) | 59 (67) | 0.084 |
| 100–125, n (%) | 40 (22.7) | 22 (25) | 18 (20.5) | |
| ≥126, n (%) | 28 (15.9) | 17 (19.3) | 11 (12.5) | |
| Albumin, g/dL, median (IQR) | 4.4 (0.3) | 4.4 (0.3) | 4.3 (0.3) | 0.301 |
| Transferrin, mg/dL, mean ± SD | 277.3 ± 40.8 | 281.3 ± 46.2 | 273.3 ± 34.4 | 0.506 |
| Ferritin, ng/dL, median (IQR) | 89 (101) | 85 (110.5) | 89 (96) | 0.274 |
| Total cholesterol, mg/dL, mean ± SD | 199.1 ± 39.5 | 191.7 ± 37.3 | 206.4 ± 40.4 | 0.015 * |
| LDL, mg/dL, mean ± SD | 115.7 ± 35.3 | 110.1 ± 32.1 | 121.3 ± 37.5 | 0.043 * |
| HDL, mg/dL, median (IQR) | 56.5 (20) | 55.5 (18) | 58 (22) | 0.213 |
| VLDL, mg/dL, median (IQR) | 23 (14) | 23 (13) | 22.5 (14) | 0.370 |
| Triglycerides, mg/dL, median (IQR) | 113 (70) | 115 (68) | 112 (72) | 0.360 |
| ApoB, mg/dl, mean ± SD | 101.5 ± 20.6 | 98.9 ± 21.3 | 104 ± 19.7 | 0.141 |
| LDL/ApoB Ratio < 1.3, n (%) | 135 (77.1) | 74 (84.1) | 61 (70.1) | 0.038 * |
| Vitamin B12, pg/mL, median (IQR) | 372 (188) | 376 (188) | 371 (191) | 0.549 |
| Folic acid, ng/mL, median (IQR) | 10.5 (6.7) | 11.3 (7.1) | 9.4 (6.7) | 0.360 |
| 25-OHD, ng/mL, mean ± SD | 19.6 ± 6.5 | 20.3 ± 6.5 | 18.8 ± 6.5 | 0.193 |
| TSH, mcU/mL, median (IQR) | 1.59 (1.20) | 1.48 (1.12) | 1.67 (1.07) | 0.562 |
| Total testosterone, ng/mL, median (IQR) | 0.58 (3.47) | 0.60 (3.13) | 0.57 (3.67) | 0.328 |
| Free testosterone, ng/mL, median (IQR) | 0.08 (0.05) | 0.009 (0.05) | 0.008 (0.05) | 0.334 |
| SHBG, nmol/L, median (IQR) | 50.3 (26.2) | 47.6 (23.1) | 56.1 (33.1) | 0.004 * |
| Hemoglobin, g/dL, mean ± SD | 14.4 ± 1.2 | 14.3 ± 1.2 | 14.4 ± 1.3 | 0.502 |
| Leukocytes, ×109/L, mean ± SD | 6.72 ± 1.79 | 6.84 ± 1.89 | 6.60 ± 1.70 | 0.475 |
| Lymphocytes, ×109/L, median (IQR) | 1.80 (0.75) | 1.90 (0.80) | 1.80 (0.78) | 0.733 |
| CRP, mg/L, median (IQR) | 1.49 (2.34) | 1.92 (2.24) | 1.18 (2.14) | 0.155 |
| IL-6, pg/mL, median (IQR) | 1.20 (1.26) | 1.45 (1.38) | 1.03 (0.96) | 0.044 * |
| Controls n = 88 | Cases n = 88 | p-value a n = 88 | |
|---|---|---|---|
| Frailty, n (%) | |||
| Weight Loss | 5 (5.7) | 6 (6.8) | 1 |
| Exhaustion | 15 (17) | 4 (4.5) | 0.013 * |
| Reduced activity | 54 (61.4) | 43 (49.4) | 0.082 |
| Weakness | 50 (56.8) | 38 (43.7) | 0.045 * |
| Slowness | 22 (25) | 9 (10.3) | 0.004 * |
| Sarcopenia, n (%) | |||
| Low muscle mass | 8 (9.4) | 10 (11.8) | 0.815 |
| Weakness | 27 (30.7) | 25 (28.7) | 0.038 * |
| Slowness | 28 (32.6) | 14 (16.3) | 0.018 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belenguer-Varea, A.; Avellana-Zaragoza, J.A.; Inglés, M.; Cunha-Pérez, C.; Cuesta-Peredo, D.; Borrás, C.; Viña, J.; Tarazona-Santabalbina, F.J. Effect of Familial Longevity on Frailty and Sarcopenia: A Case–Control Study. Int. J. Environ. Res. Public Health 2023, 20, 1534. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021534
Belenguer-Varea A, Avellana-Zaragoza JA, Inglés M, Cunha-Pérez C, Cuesta-Peredo D, Borrás C, Viña J, Tarazona-Santabalbina FJ. Effect of Familial Longevity on Frailty and Sarcopenia: A Case–Control Study. International Journal of Environmental Research and Public Health. 2023; 20(2):1534. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021534
Chicago/Turabian StyleBelenguer-Varea, Angel, Juan Antonio Avellana-Zaragoza, Marta Inglés, Cristina Cunha-Pérez, David Cuesta-Peredo, Consuelo Borrás, José Viña, and Francisco José Tarazona-Santabalbina. 2023. "Effect of Familial Longevity on Frailty and Sarcopenia: A Case–Control Study" International Journal of Environmental Research and Public Health 20, no. 2: 1534. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20021534